
Abstract
Standard urine culture is the gold standard for diagnosing urinary tract infections (UTIs) but fails to differentiate true UTI from asymptomatic bacteriuria, which is important to prevent the overuse of antibiotics. Correlation with the presence or absence of pyuria can be helpful in giving a hint of the true situation. With the help of Laboratory Information System (LIS), patients’ urinalysis reports can be conveniently accessed and compared simultaneously with appropriate reports. In our study, a quality improvement initiative was planned for appropriate reporting of urine culture and antimicrobial susceptibility testing using information obtained through LIS.
Materials and methods
All urine samples showing significant bacteriuria (SB), that is, growth of ≥105 colony-forming units [CFU]/mL over a period of three months were included. Urine samples received without clinical information were further identified by Laboratory Information System (LIS) or telephone conversation. Where provisional diagnosis or signs and symptoms could not be established, the urinalysis report was checked to record the leucocyte (WBC) count before a decision to proceed with antimicrobial susceptibility testing (AST) reporting. Pyuria was defined as the presence of ≥10 WBC/mm3 in a urine specimen, ≥3 WBC per high-power field of unspun urine, a positive result on Gram's staining of an unspun urine specimen, or a urinary dipstick test that was positive for leucocyte esterase. 1 Samples with pyuria were processed for AST. Samples with WBC <10/mm3 were also processed for AST but reported with a comment, ‘kindly correlate clinically’. These cases were followed up to monitor the outcome.
Results
A total of 250 suspected urinary tract infection (UTI) cases where the standard urine culture (SUC) yielded significant bacterial growth were analysed (Fig. 1). Out of these, 44% (110) mentioned relevant signs and symptoms on the requisition form and fitted true UTI cases. The remaining 140 had no history or provisional diagnosis. Signs and symptoms were confirmed in 80 of these. The two combined groups of 190 were processed for AST. For those 60 cases where no history was obtained, the urinalysis report was checked by LIS. Pyuria was present in 38 (63.3%), which were also processed for AST. The remaining 22 (8.8% of the total of 250) did not have pyuria, and a comment was sent, ‘kindly correlate clinically’. Follow-up of these cases revealed 13 were in-patients and had been discharged after recovery. The other nine were out-patients and had, apart from two who could not be contacted, no symptoms.
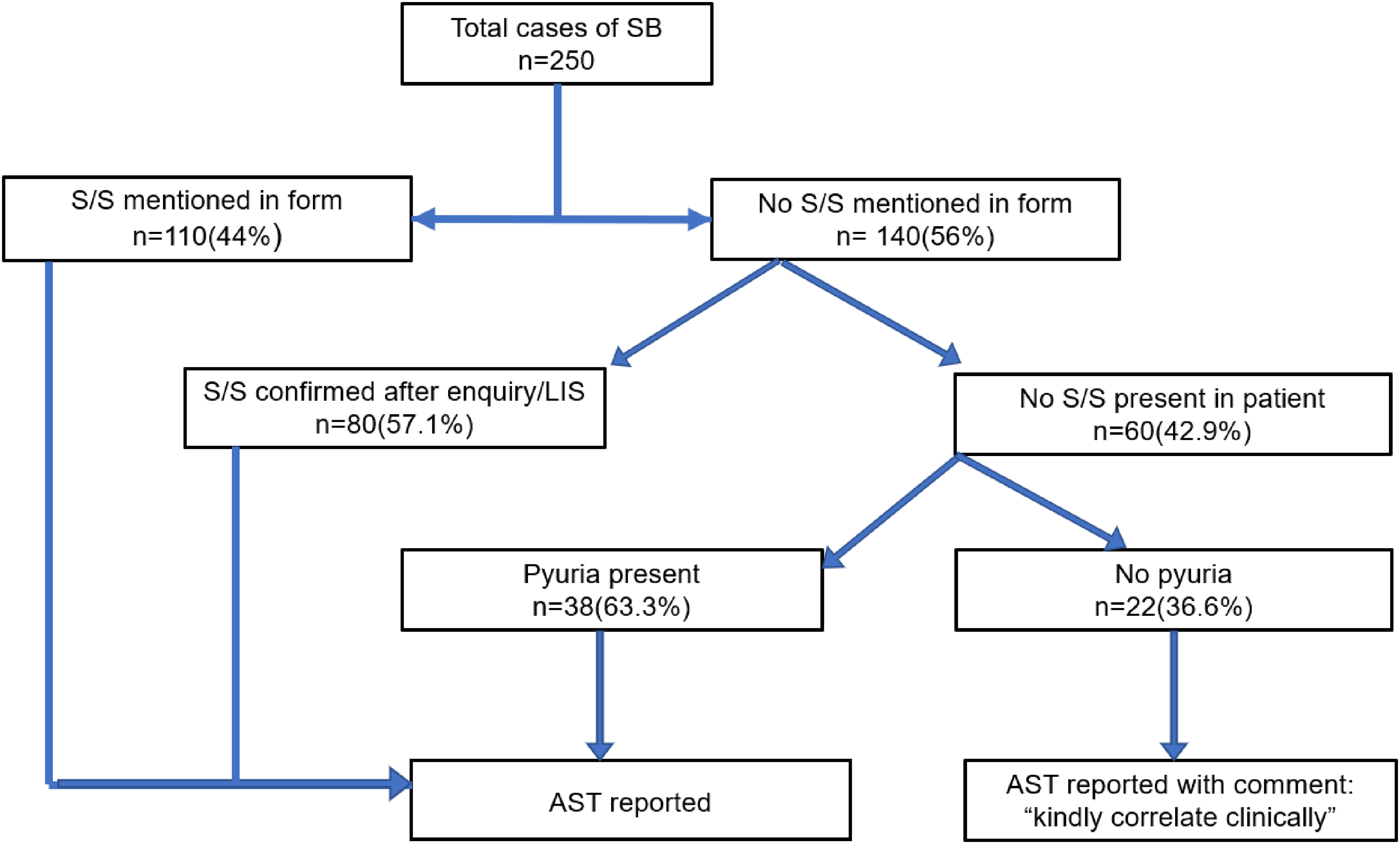
Workflow of the study. SB: Significant Bacteriuria, LIS: Laboratory Information System, S/S: Signs and symptoms.
Discussion
Clinical correlation with a SUC result is essential. Over-reporting and over-treatment of supposed infection prevails. One study 2 showed that restricting urine culture reporting to true UTIs was associated with lower antimicrobial consumption, with no effect on patient mortality. Correlation with pyuria aids in differentiating asymptomatic bacteriuria from true infections, and this has been recommended as a criterion. 3 Using LIS, all cases of SB could be checked before AST processing commenced; this obviously reduces unnecessary treatment. Right diagnosis, along with the right drug, dose, duration and de-escalation are indeed the 5 Ds of antimicrobial stewardship. 4
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.