
Abstract
Caesarean scar ectopic pregnancy (CSEP) is a uncommon presentation of pregnancy with incidence of nearly 1 in 2000 pregnancies. We present this case series of scar pregnancy with a objective to help obstetricians in early diagnosis and appropriate management to prevent its catastrophic complications.
Introduction
Caesarean scar ectopic pregnancy (CSEP) is a uncommon presentation of pregnancy and its incidence is rising in parallel with the increase in incidence of Caesarean sections (CS).1–3 Hysterotomy scar ectopic pregnancy has also been reported in women with previous history of myomectomy, hysteroscopy, previous abnormally adherent placentation, hysteroscopy, introduction of intra-uterine devices, in vitro fertilisation, uterine evacuation and manual removal of the placenta.1,4
CSEP may be of two types: Type 1 (endophytic) develops in the myometrium and grows inwards within the uterine cavity, and Type 2 (exophytic) which progresses outwards toward the uterine serosa. 4 The latter has a higher risk on account of spontaneous uterine rupture, as well as uterine haemorrhage. Symptoms may however be absent or with mild pelvic pain in the first trimester. Pervaginal ultrasound is the investigation of choice, and can be combined with a trans-abdominal view for other details. MRI may be needed for confirmation or to rule out other diagnoses. 2
Possible treatment is varied ranging from radical to conservative surgery depending upon physician choice, availability of facilities, the gravity of signs and symptoms, gestational age, and the patient's desire for future fertility. 5
We present a series of five cases to illustrate specific points and individual management.
Case 1
A 26-year old female (gravida 2, para 1) presented as an emergency with painless vaginal bleeding following two months of amenorrhoea. She had had a previous CS two years previously for foetal distress. Her pulse was 88/min and blood pressure 128/74 mmHg. On speculum examination, slight bleeding was present. Bimanual examination revealed a uterus of ten weeks’ size, retroverted with the cervix downward and both fornices free. Her haematological and biochemical investigations were within normal limits. A pervaginal ultrasound showed an irregular single intra-uterine gestational sac with yolk sac and foetal node in the lower uterine segment adjacent to her previous scar. On colour Doppler, excessive vascularity at the previous scar was noted. These findings were confirmed on MRI imaging, which showed a lesion measuring 2.3 × 3.5 cm in the lower anterior uterine wall with altered signal, multiple hypo-intense foci and multiple tortuous vascular channels in the parametrium with an empty cervical canal suggestive of scar pregnancy. Her β-HCG level was 6673 IU/L (normal < 5 IU/L in non-pregnant women) and after 48 h, it was 5576 IU/L. Considering her desire for future fertility, the decreasing β-HCG level and her stable haemodynamic condition, medical management seemed appropriate. Four doses of 50 mg methrotraxate were given IM with alternate day folinic acid over eight days. On the ninth day of follow up, her β-HCG was 1330 IU/L and the ultrasound showed reduction in size of the uterine lesion to 1.1 × 2.1 cm with no colour Doppler flow nor gestational sac noted, and an endometrium of 5 mm thickness. Our patient was monitored on a weekly basis as an out-patient till her β-HCG normalised five weeks later.
Case 2
A 36-year old female (gravida 3, para 2) presented as an emergency with vaginal bleeding and abdominal pain. An ultrasound scan done elsewhere had suggested a scar pregnancy. She had a history of two previous CS, the last ten years prior for foetal distress. She was tachycardic (pulse 128/min) and hypotensive (90/54 mmHg). She had become severely anaemic (Hb 70 g/l). On abdominal examination, the uterus was just palpable and on vaginal examination, the os admitted one finger with a suggestion of scar dehiscence with products of conception attached and also protruding anteriorly towards the urinary bladder.
Her β-HCG was 1824 IU/L, her ultrasound showed a large irregular heterogeneously hypoechoic lesion measuring 6.3 × 5.6 cm with multicystic areas in the lower endometrial cavity, with anterior myometrial thinning to < 1 mm and profuse vascularity reaching the anterior myometrium on colour Doppler. Her MRI findings showed an irregular thickened endometrial cavity with multiple irregular cystic areas and disruption of the junctional zone with myometrial invasion, likely to be a scar pregnancy or invasive mole.
As the patient was continuously bleeding, an emergency laparotomy was carried out. An ectopic pregnancy of 6 × 6 cm at the scar site circumferentially involving both left lateral and anterior uterine walls with ectopic tissue was excised. Further bleeding however required inotropic support, and transfusion of three units of packed red blood cells; in view of this, an emergency hysterectomy was carried out. Her recovery was uneventful and she was discharged on the tenth post-operative in a stable condition.
Case 3
A 27-year old female (gravida 2, para 1) was referred to our hospital with painless vaginal bleeding for two days and a diagnosis of scar ectopic pregnancy of five weeks’ gestation. She had a history of previous CS seven years before due to foetal distress. Her urine pregnancy test was positive and an ultrasound showed a gravid uterus with an irregular gestational sac with its foetal pole in the lower uterine segment measuring 5.6 × 3.4 cm at the previous scar site with relevant vascularity (Fig. 1). Her MRI findings showed a gestational sac within the endometrial canal in the lower uterine segment with thinning of the overlying anterior myometrium measuring 2.1 mm, likely due to post Caesarean scarring suggestive of Caesarean scar pregnancy (Fig. 2). Her ß-HCG was 1205 IU/L on admission. On speculum examination, slight bleeding was seen and on bimanual examination the uterus was retroverted, bulky, but both fornices were free. She remained haemodynamically stable, and so was given medical management with four doses of injectable methotrexate given with alternate folinic acid injections. On the eighth day, her β-HCG reduced to 400 IU/L and her ultrasound showed a 3 × 2 cm lesion in lower uterine cavity with no flow on colour Doppler. She was discharged in a stable condition and thereafter followed up on a weekly basis till her β-HCG normalised after 4 weeks.
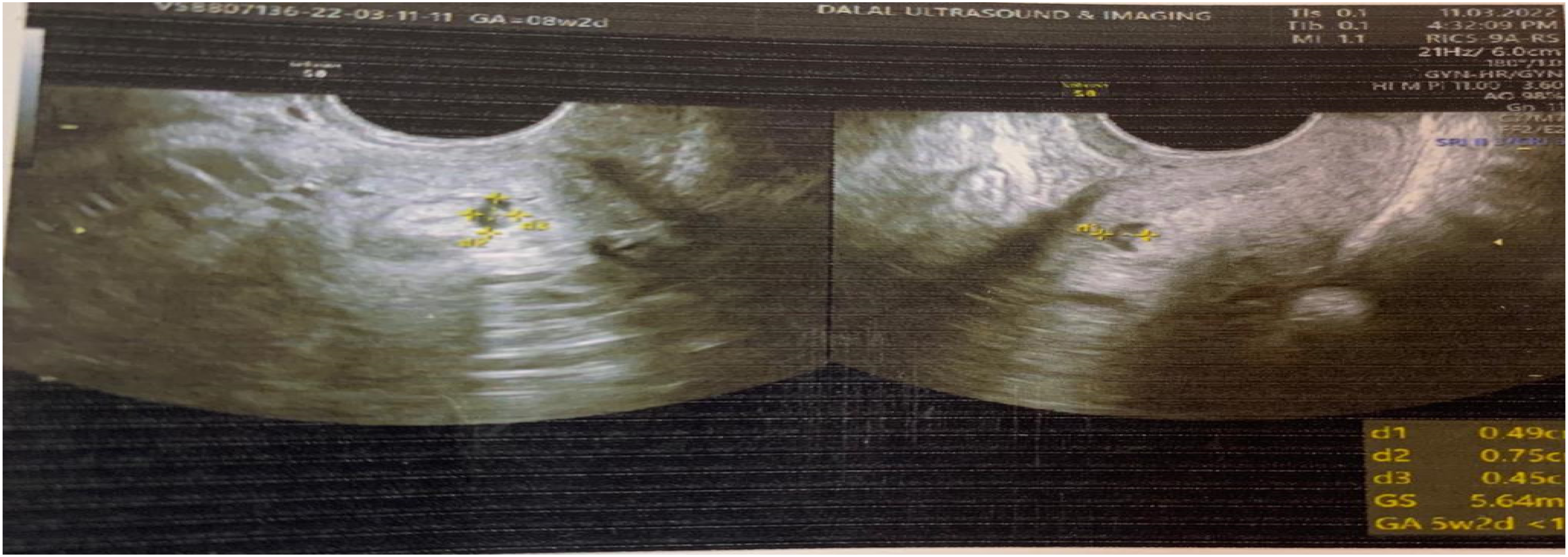
Ultrasound image showing irregular gestational sac with foetal pole in lower uterine segment with high vascularity.
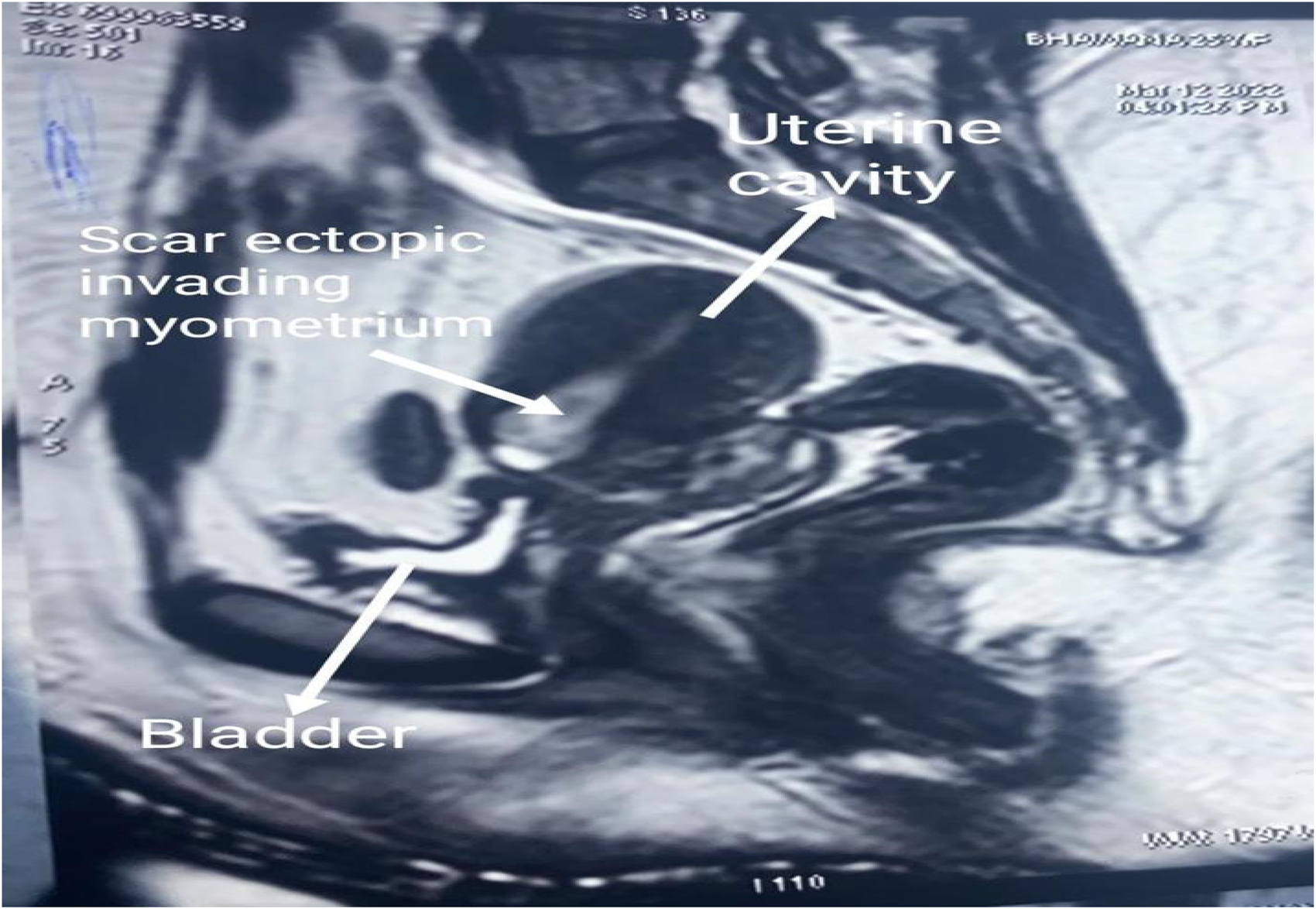
MRI image showing scar ectopic invading the myometrium.
Case 4
A 26-year old female (gravida 2 and para 1) presented for medical termination of pregnancy. She had two months of amenorrhoea and a history of a previous CS 15 months before on account of a contracted pelvis. Her pulse was 83/min and blood pressure 118/68 mmHg. There was no bleeding on speculum examination and on bimanual examination, the uterus was bulky with no other palpable abnormality detected.
Ultrasound showed a single intra-uterine gestational sac with the yolk sac with foetal pole in the lower uterine segment and normal flow on colour Doppler. Her MRI showed likewise with a thick T2 hyperintense rim of signal intensity around the gestational sac suggestive of a decidual reaction abutting the anterior myometrium and its thinning. Her β-HCG level was 75760 IU/L on admission.
An ultrasound-guided intra-lesional injection of 50 mg methotrexate was given and on the next day, a Foley catheter balloon was inserted into the uterus and inflated with 50 ml saline (Fig. 3) to compress the scar gestation; it was, however, spontaneously expelled the next day.

Ultrasound image showing intrauterine inflated Foley balloon compressing the scar gestation.
A second dose of 50 mg methotrexate was injected IM. However, on the fourth day, her β-HCG had risen to 54000 IU/L. Another balloon was inserted, the patient remaining stable for the next three days, but thereafter a high grade fever ensued. Consequently a suction evacuation was decided upon. Three days later, the β-HCG level had dropped to 1516 IU/L but an ultrasound showed a 2 × 1.4 cm hypoechoic lesion in the anterior myometrium with increased vascularity, suggestive of retained products of conception. Misoprostone 400 μg tds was administered orally for two days; this produced a vaginal discharge of the conceptus over three subsequent days, after which a repeat ultrasound showed minimal volume of retained products of conception with no flow on Doppler; the β-HCG had further fallen to 1212 IU/L. Our patient was discharged in a stable condition and followed up weekly till β-HCG levels normalised after seven weeks.
Case 5
A 25-year old female (gravida 2, para 1) presented as an emergency with painless vaginal bleeding for one day. She had a history of previous CS eight months before. Her pulse was 95/min and blood pressure 104/62 mmHg. She had become severely anaemic (Hb 62 g/L), and was transfused two units of packed red blood cells. Abdominal examination revealed a well-healed transverse scar. Speculum examination revealed slight vaginal bleeding. On bimanual examination, the uterus of 12 weeks’ size was anteverted, with os closed and both fornices normal. Her β-HCG was 3018 IU/L, and her ultrasound showed a 5.4 × 5.2 cm heterogeneously hyperechoic gestation at the scar site with vascularity. An injection of 50 mg methotrexate was administered IM but bleeding persisted, and suction evacuation was decided upon. This was unsuccessful, with unchanged ultrasound findings. An MRI now showed a large hetero-intense lesion measuring 6 × 7 × 8.4 cm predominantly in the lower uterine segment at the previous scar site causing myometrial thinning and focal bulging of the anterior myometrium suggestive of scar ectopic pregnancy (Fig. 4). Her β-HCG level was 1192 IU/L. On account of persistent haemorrhage, a laparotomy was performed, where an 8 × 3 cm scar ectopic pregnancy, bleeding with areas of necrosis and bluish discoloration, was excised (Fig. 5). The patient was discharged on the tenth post-operative day in a healthy condition.
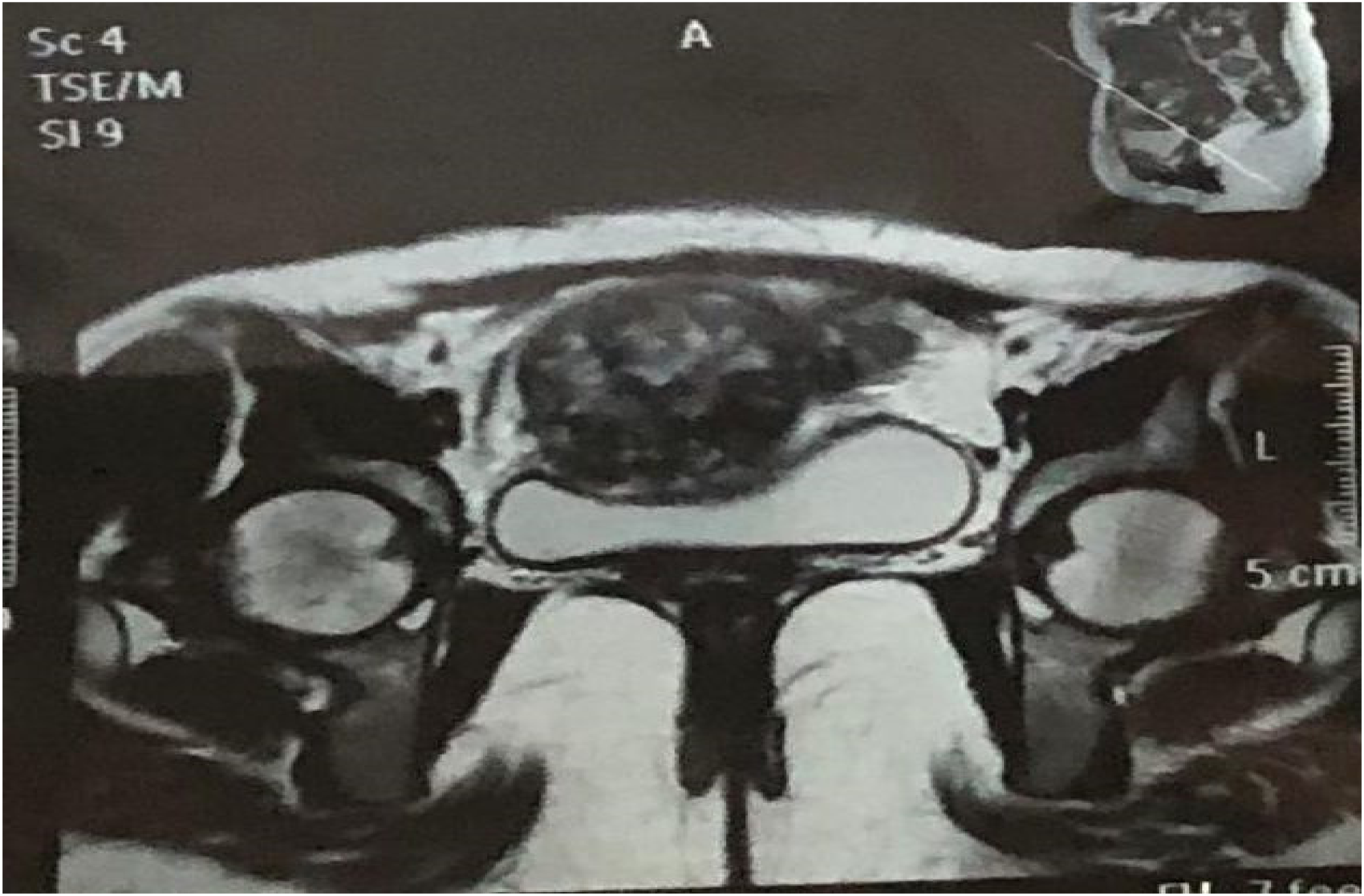
MRI with coronal view of scar ectopic invading the myometrium.
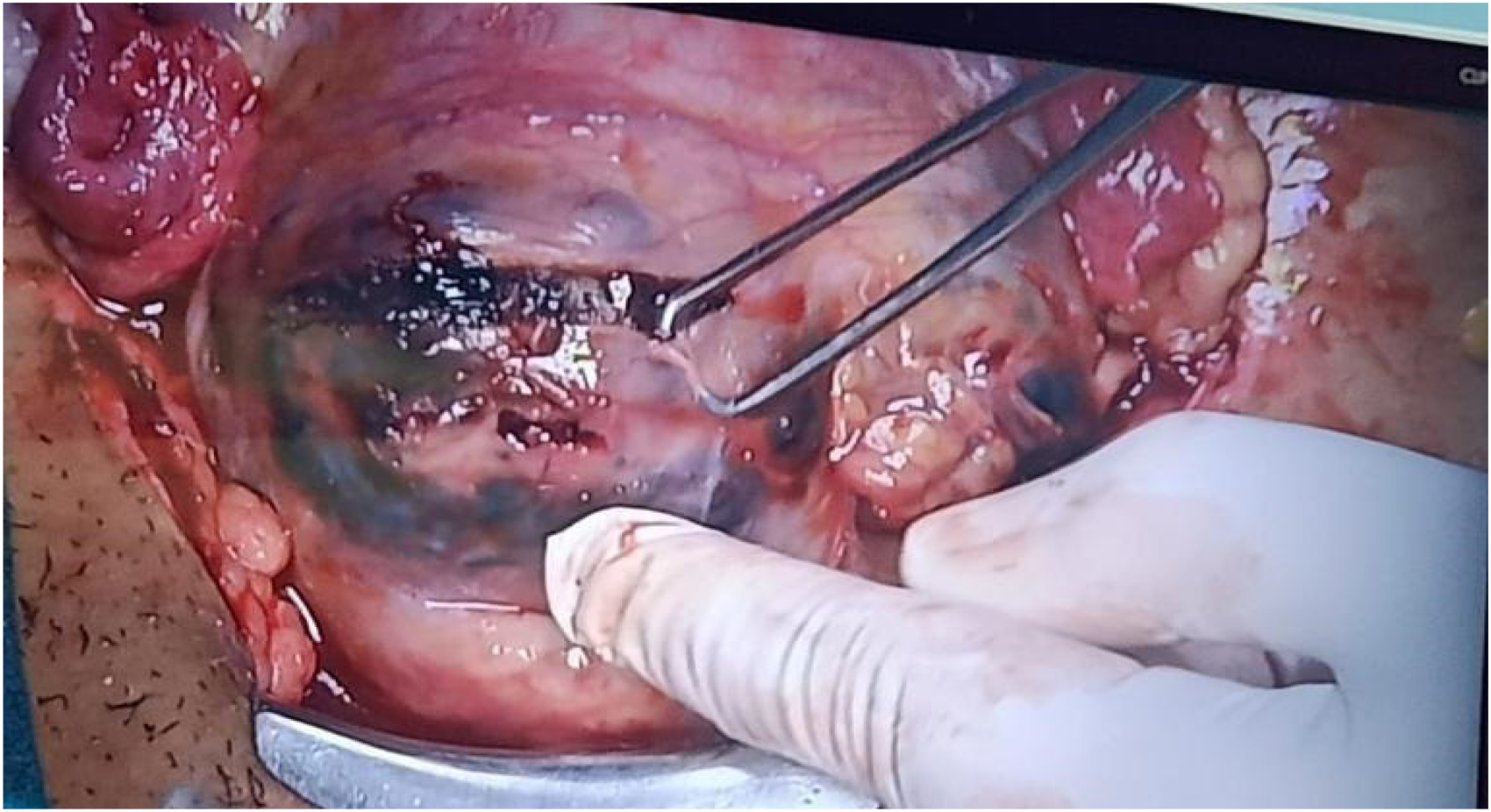
Intra-operative image showing CSEP.
Discussion
CSEP is uncommon. 6 It may be life-threatening, and may be very difficult to diagnose. A false negative diagnosis may be disastrous. Ectopic gestation is thought to be caused by blastocyst invasion into the myometrium through a microscopic tract formed because of previous uterine injury, however caused.7–9 The diagnosis rests on pervaginal ultrasound findings (preferably with colour Doppler) and raised β-HCG levels, supported, if possible, by MRI findings, which can more accurately define location and uterine attenuation.
Painless vaginal bleeding in the first trimester is the most common presentation. Abdominal pain may signify more sinister progression. There is no common consensus on treatment. Although management must be individualised depending upon haemodynamic stability, desire for future fertility, gestational age and size of the pregnancy, a plethora of options exist, including: methotrexate injection systemically or intra-lesion, balloon compression, gestational sac needle aspiration, uterine curettage, pervaginal or open resection, uterine artery embolisation, repeated high-intensity focused ultrasound ablation, or most radically, a hysterectomy.10,11
Conservative medical treatment is suitable for a haemodynamically stable patient with < 8 weeks’ of gestation, β-HCG levels <5000 IU/L, without cardiac activity and myometrial thickness < 2 mm between the bladder and scar gestation. 12 Although medical treatment has the advantage of being preserving fertility and is non-invasive, it may take 4–16 weeks till β-HCG levels settle to normal; the risk of uterine rupture and haemorrhage, however, remains. 13
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.