
Abstract

Introduction
Hyperreactio luteinalis (HL) refers to the enlargement of bilateral ovaries by multiple theca lutein cysts due to the influence of the placental hormone beta-human chorionic gonadotropin (β-hCG). 1 Its primary function in pregnancy is to promote progesterone release from the corpus luteum. 2 HL is a rare condition 3 which usually occurs in women with high β-hCG levels such as pregnancies with multifetal gestation, molar pregnancy and choriocarcinoma. 4 It is also seen in women with polycystic ovarian syndrome (PCOS) owing to the increased sensitivity of the ovarian stroma to β hCG. 4
We present a case of HL incidentally discovered during caesarean delivery of a spontaneously conceived singleton pregnancy. It is worth noting that to date, the literature on HL in term pregnancies is only limited to a few case reports.
Case report
An unbooked 24-year-old primigravida at 37 completed weeks of gestation with chronic hypertension was referred to our institute in view of oligohydramnios. She complained of decreased perception of fetal movements over the last 2 days. The pregnancy was spontaneously conceived. She had no significant past medical or surgical history. Her antenatal period was uneventful. Her antenatal blood pressure (BP) recordings on tablet labetalol 100 mg twice daily were within normal range. Her pre-pregnancy weight was 62 kg and height 167 cm, giving a BMI of 22.2 kg/m2 (within normal range). A review of her antenatal scans revealed a normal anomaly scan, which had been performed at 20 weeks of gestation. She did not have any previous transvaginal ultrasounds. Her antenatal investigations were within the normal range including a normal glucose tolerance test. At the time of presentation, she had a pulse rate of 74/minute and BP 126/88 mm Hg. General physical examination revealed no abnormality. She had a fundal height corresponding to 34 weeks’ gestation and the abdomen appeared full of fetus. Transabdominal ultrasonography (TAS) was performed on arrival, revealing a single live intra-uterine fetus in cephalic presentation with an estimated fetal weight of 2560 g which corresponds to the 12th centile for gestational age, and an amniotic fluid index of 4.8 cm.
In view of term pregnancy with chronic hypertension and oligohydramnios, the decision was taken to induce labour. However, a non-stress test performed prior to induction showed prolonged fetal bradycardia (Fig. 1). Emergency caesarean delivery was therefore decided upon. A term healthy male baby weighing 2600 g was delivered. Intra-operatively, after the delivery of the baby, when the uterus was exteriorized for closure, both ovaries were found to be enlarged with multicystic lobules with increased vascularity measuring 10 × 6cm on the right side and 6 × 5cm on the left (Fig. 2). Close follow up in the postnatal period was programmed. Biopsy from an ovary was not taken in view of their increased vascularity.
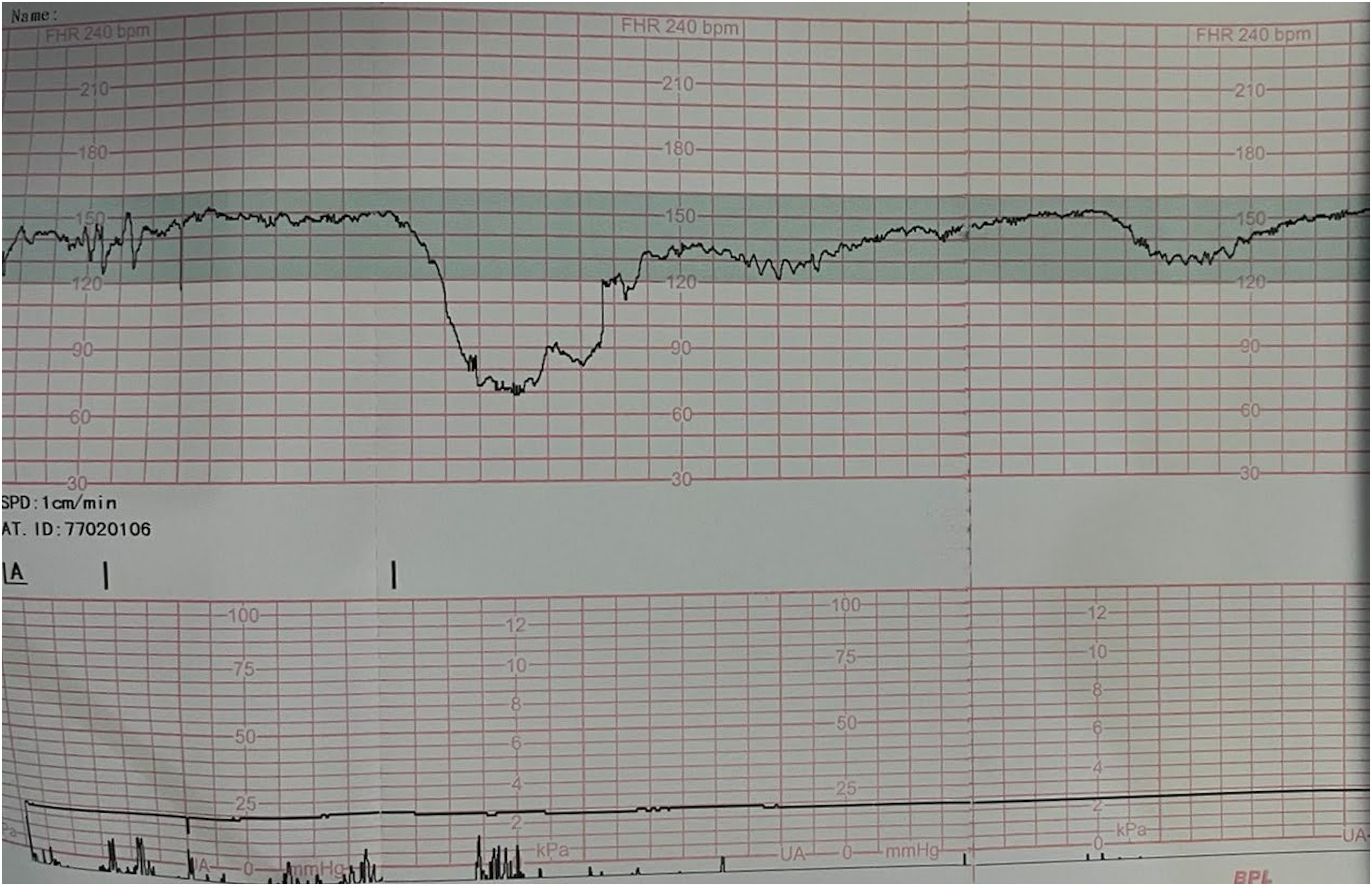
Non-stress test showing prolonged fetal bradycardia.
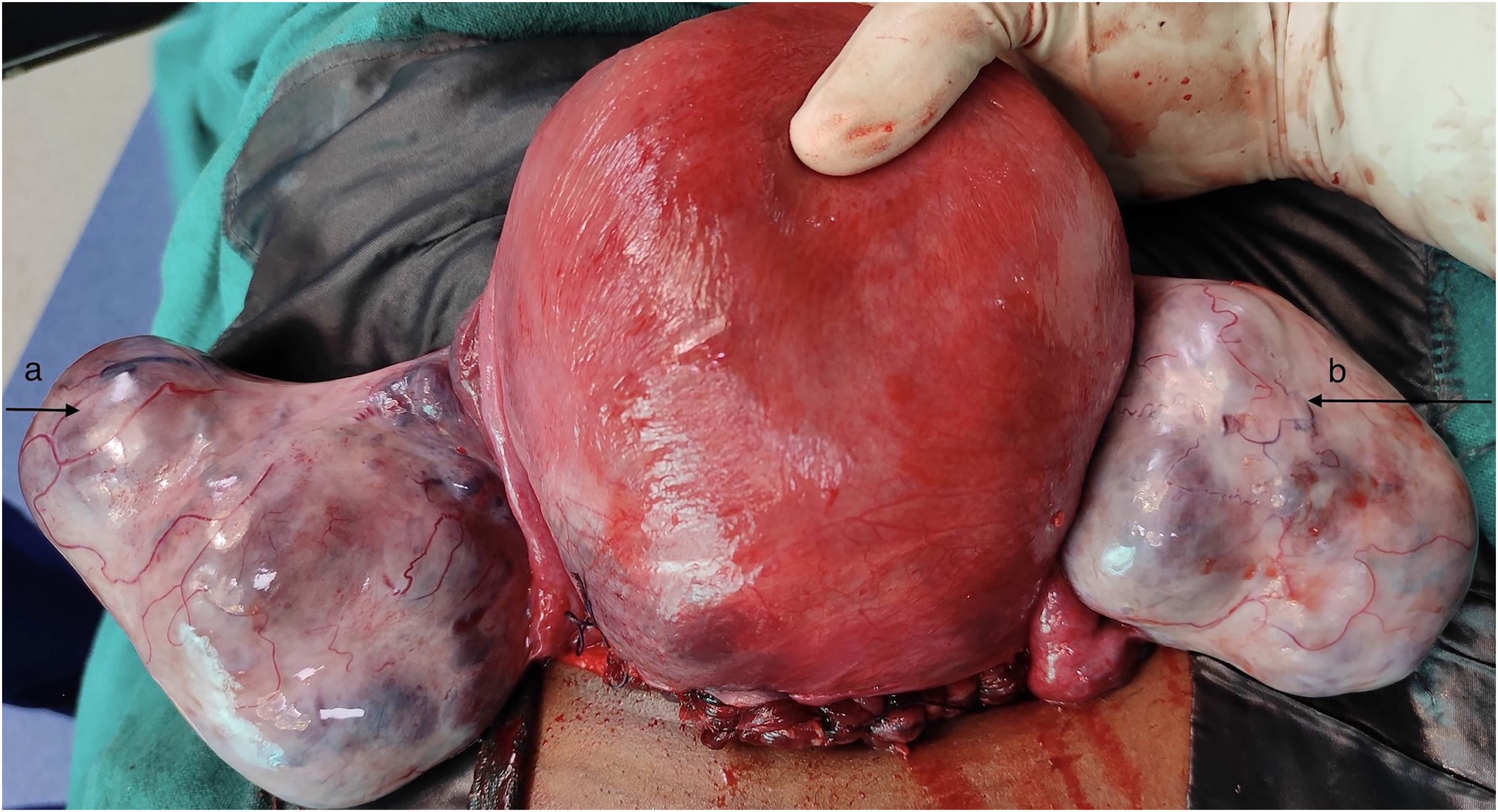
Hyperreactio luteinalis (right and left hyperstimulated ovaries marked by ‘a’ and ‘b’, respectively) in term pregnancy encountered during caesarean delivery.
Retrospectively, she told a history of hyperemesis gravidarum in the first trimester. After caesarean delivery, β-hCG levels were 2850 IU/mL. Other tumour markers of ovarian malignancy and thyroid function tests were within the normal range. Serum androgen levels were not tested in view of absence of any clinical features of hyperandrogenism. Transvaginal ultrasound was suggestive of bilateral enlarged ovaries with a spoke-and-wheel pattern (Fig. 3). A provisional diagnosis of HL was made. Six weeks postdelivery a urine pregnancy test was negative and a transvaginal ultrasound showed complete regression of the ovarian cysts (Figs. 4 and 5), thus confirming the diagnosis of HL.
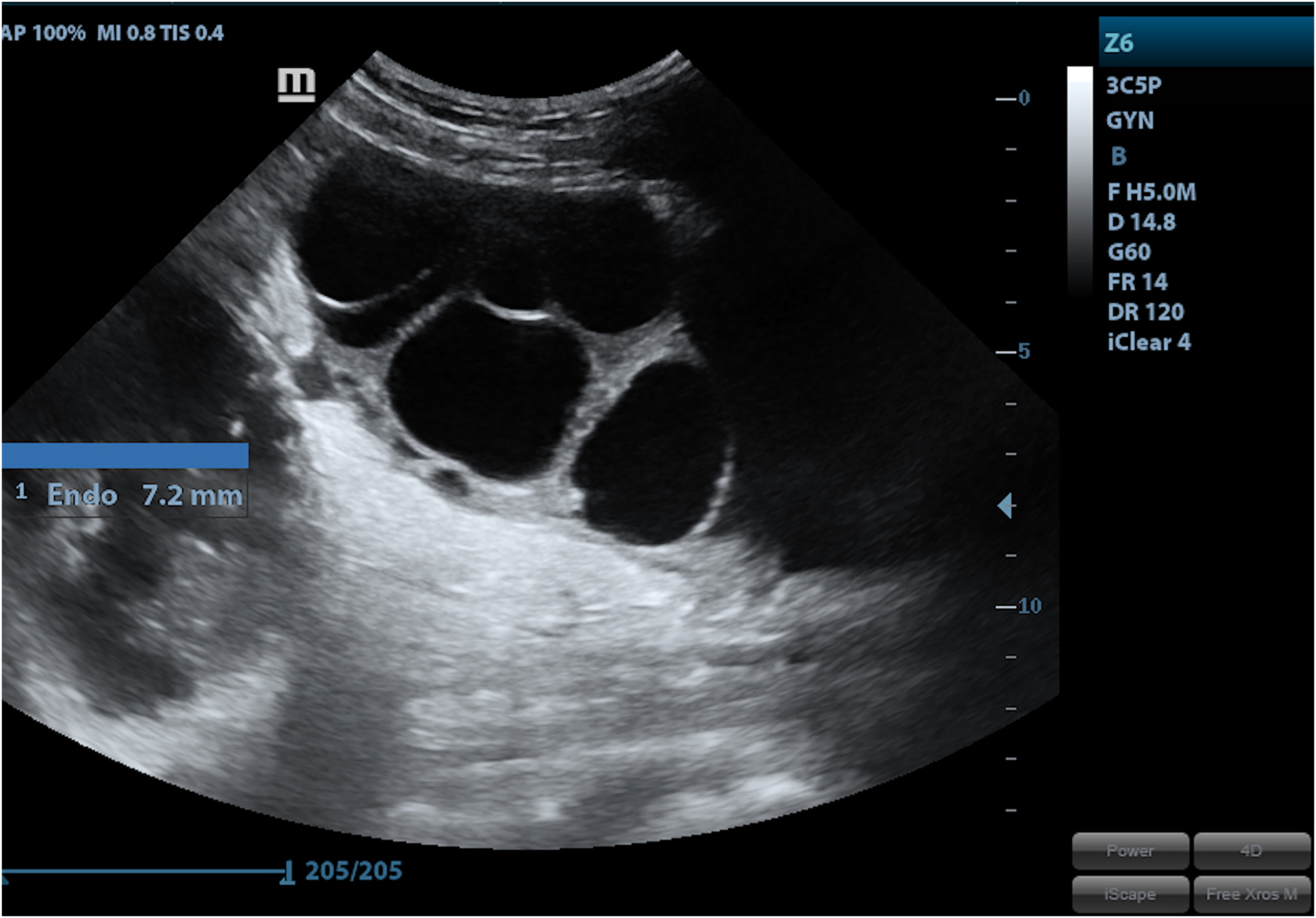
Transvaginal ultrasound showing bilateral enlarged ovaries with a spoke-and-wheel pattern.
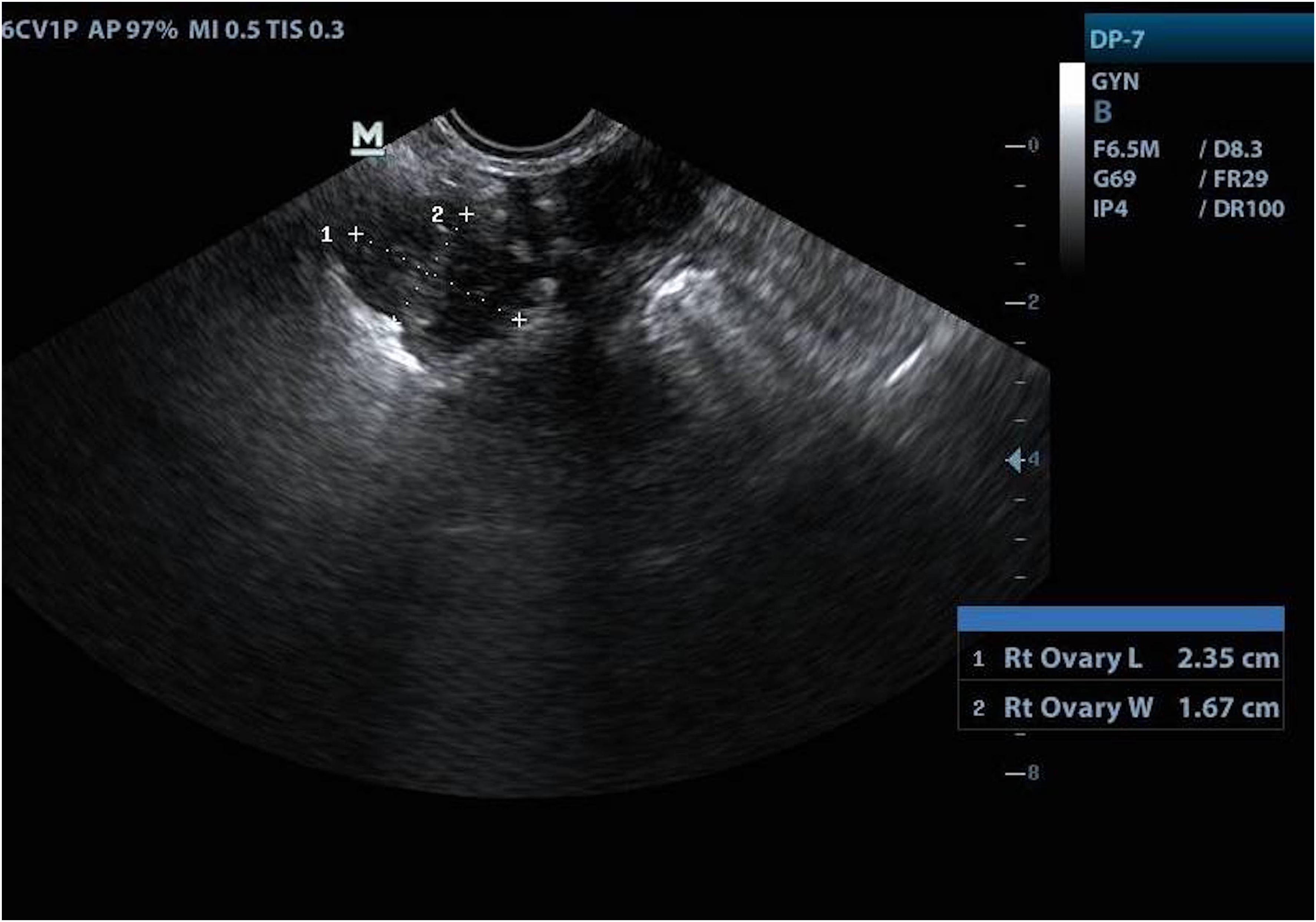
Transvaginal ultrasound performed 6 weeks postdelivery showing a normal right ovary with complete regression of the cysts.
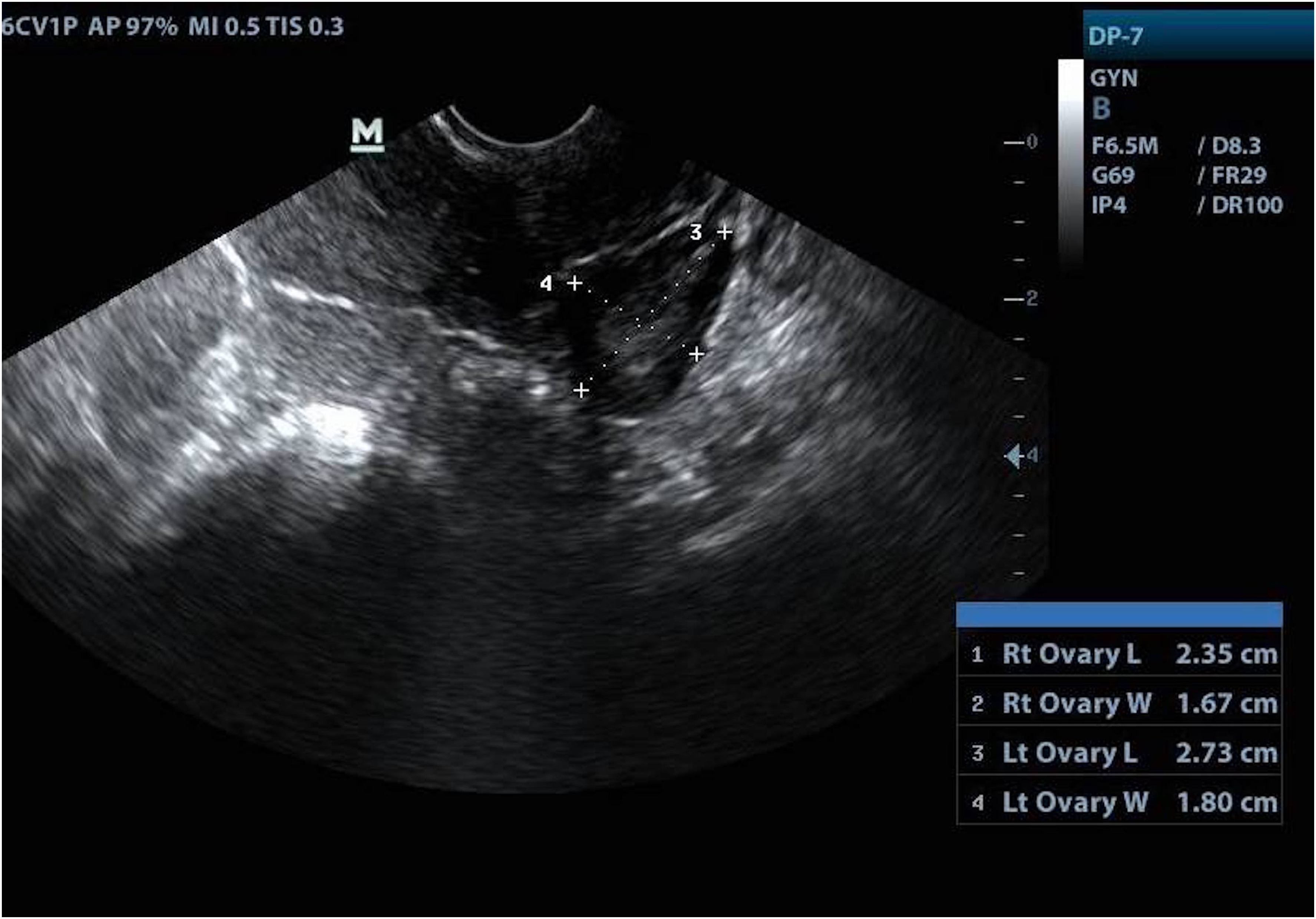
Transvaginal ultrasound showing a normal left ovary at 6 weeks postdelivery.
Discussion
HL is usually an incidentally diagnosed condition, which is typically seen in the second and third trimesters of pregnancy in women at risk.5–7 It is mostly asymptomatic unless complicated by torsion or rupture when it can present with acute abdomen.6,8 It can also be associated with symptoms of maternal hirsutism or virilization, especially in females with PCOS. 9 However, virilization has been reported in only 25–30% pregnant women,5,6 usually due to the increased levels of sex hormone binding globulin in pregnancy, which result in lower amounts of circulating free testosterone. 5 Foetal virilization has also been reported, albeit extremely rare 4 as foetal labioscrotal fusion occurs in the first trimester and HL is seen later in gestation. 5
Our case has the limitation in terms of an absent report of levels of serum androgen of the patient.
HL is a rare condition, the prevalence of which is unknown. 3 The literature on this rare condition primarily consists of case series and isolated case reports. 3 The condition has been reported in association with the intake of ovulation induction agents, gestational trophoblastic disease, 10 multifetal gestation, and PCOS. The reported incidence ranges from 10% in cases of choriocarcinoma and 25% in patients with molar pregnancy. 1 It can also occur due to increased β-hCG released from a large placenta in women with non-immune fetal hydrops and gestational diabetes. 8 However, in 60% cases, no predisposing factors or associated abnormalities are found.11,12 There is also the possibility that HL is due to an aggravated maternal response to physiological levels of β-hCG, or an abnormally rapid increase in β-hCG levels in early gestation. 12
It is of paramount importance to distinguish HL from its mimics. An important differential is ovarian hyperstimulation syndrome (OHSS). However, this is mostly iatrogenic, presents in the first trimester usually and is associated with signs of fluid and electrolyte imbalance while HL is usually asymptomatic and presents at a later gestation. Another differential is luteoma of pregnancy, which is mostly seen in the first trimester. 8 Also, malignant mimics such as mucinous tumours and germ cell tumours such as juvenile granulosa cell tumours (GCTs) need to be kept in mind. While juvenile GCTs are usually unilateral, 8 HL is almost always bilateral. Mucinous tumours can be differentiated by their specific tumour markers and ultrasound appearance. 1
As β-hCG promotes angiogenesis of the uterine vasculature, causes differentiation of the cytotrophoblasts to syncitiotrophoblasts, and promotes immunotolerance in pregnancy, 2 dysregulation of β-hCG levels are associated with pregnancy complications such as pre-eclampsia, fetal growth restriction (FGR) and hemolysis, elevated liver enzymes and low platelets (HELLP) syndrome.2,3 Our case had none of these, though she developed oligohydramnios, which is also an indicator of placental insufficiency, hence worth noting. These patients may also have associated difficulty in lactation in the postpartum period owing to pituitary dysregulation. 5
HL can be diagnosed in pregnancy by its classical ultrasound appearance of a ‘spoke-and-wheel’ or ‘bunch-of-grapes’ pattern, 6 bilateral thin-walled cysts, normal flow on colour Doppler and absent solid components. 4 If diagnosed antenatally, care must be taken to exclude thyroid dysregulation, diabetes mellitus and gestational trophoblastic disease, which are commonly associated with HL. 5 Also, tumour markers should be tested to rule out ovarian malignancy.
With increasing numbers of ultrasound scans being performed in pregnancy, it is likely that the incidental diagnosis of HL will become more common. Hence, it is imperative that obstetricians are aware of this condition so that unnecessary oophorectomy can be avoided in these young females. There are various reports where bilateral oophorectomy was performed when HL was misdiagnosed as malignancy.3,5 In one case report, biopsy was attempted from the enlarged ovaries but because of uncontrolled hemorrhage, the ovary had to be sacrificed. 4 Our case is a typical example of the self-resolving nature of this condition.
The association of HL with placental insufficiency warrants further research as to whether timely prophylaxis of anti-platelet agents such as aspirin should be advocated. Also, there exists a potential risk for fetal malpresentations and obstruction to fetal descent during labour because of the large ovaries. There is also a likelihood of recurrence in future pregnancy. 13 Hence, the routine habit of examining the ovaries in the antenatal period at ultrasound is advised, so that an antenatal diagnosis may be made, and steps can be taken to avoid the above-mentioned complications in the antepartum, intrapartum and postpartum periods.
Footnotes
Authorship and contributorship
Dr Ishita Agarwal collected the data, designed the case report and played a central role in writing the manuscript. Dr Sweta Singh defined the concepts, conceived the idea, and managed the case. Dr K Amirtha helped in collecting the data and in manuscript writing. Dr Jasmina Begum helped in patient management and data collection. All authors have read the manuscript and agree to its final version being published.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All India Institute of Medical Sciences, Bhubaneswar does not require ethical approval for reporting individual cases or case series.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Guarantor
On behalf of all authors, Dr. Sweta Singh will act as the guarantor and will guarantee the manuscript's accuracy and contributorship of all co-authors.
Informed consent
Written informed consent was obtained from the patient for her anonymous information including the images to be published in this article.