
Abstract
The most common site of the congenital duodenal web is the second part. Web distal to the second part of the duodenum is rare. It mimics the windsock deformity. Diagnosis may be missed if accompanying malrotation is present. We hereby report two cases of distal duodenal webs associated with malrotation and challenges in their diagnosis and management.
Introduction
Type I defect with a mucosal web is the most common type of duodenal atresia. 1 The origin of the web is usually in the second part of the duodenum. It may be stretched, leading to windsock deformity and dilatation of the distal duodenum. Duodenal web with its origin in the distal duodenum is rare. 2 Before enterotomy, the surgeon should be careful regarding the origin of the web, which can be visualised as a transition zone. A change in the calibre of the intestine and visualisation of indentation at the base of the web and the feel of the ring extraluminally give an important clue. The presence of malrotation can mask the duodenal web in the distal duodenum as both have similar clinical presentation and findings on radiological investigations. We report two cases of the duodenal web at unusual locations, viz. in the third part of the duodenum (D3) and at its junction with the fourth part (D4). Their association with malrotation made the diagnosis and treatment even more challenging.
Case series
Case 1
A 10-day female infant presented with bilious vomiting, epigastric fullness and no passage of stool for five days. On examination, she was mildly dehydrated. Mild epigastric distention was present. Routine blood investigations were normal. The erect abdominal radiograph showed a double bubble (Fig. 1(A)). No gas was seen distally. An upper gastrointestinal contrast study showed gastric and proximal duodenal dilation (Fig. 1(B)). There was a narrowing in D3 with a minimal passage of contrast beyond the narrowed portion. After fluid resuscitation, an exploratory laparotomy showed evidence of a malrotation with volvulus. Ladd's procedure was done. A bowel run-through was performed. Dilated stomach and proximal duodenum were seen. A ring-like transition zone was noted in D3. A membranous structure was felt intraluminally corresponding to an external ring-like transition zone. On introducing saline intraluminally, saline passed slowly across this transition. However, on trying to pass a Ch6 nasogastric tube by the mouth across the transition zone, it coiled up. An enterotomy was therefore performed in the duodenum proximal to the transition, and the web visualised. Initially, no passage was seen, but on retrograde milking of the small bowel, a small aperture could be identified in the web across which a Ch6 Foley catheter was passed (Fig. 1(C)). The web was then excised, and the enterotomy closed (Fig. 1(D)). Post-operatively, the child passed stool on the second day. Oral feeding was commenced on the fifth post-operative day and she could be discharged three days later. At 2 years’ follow-up, the child is accepting feeds well and has gained weight.
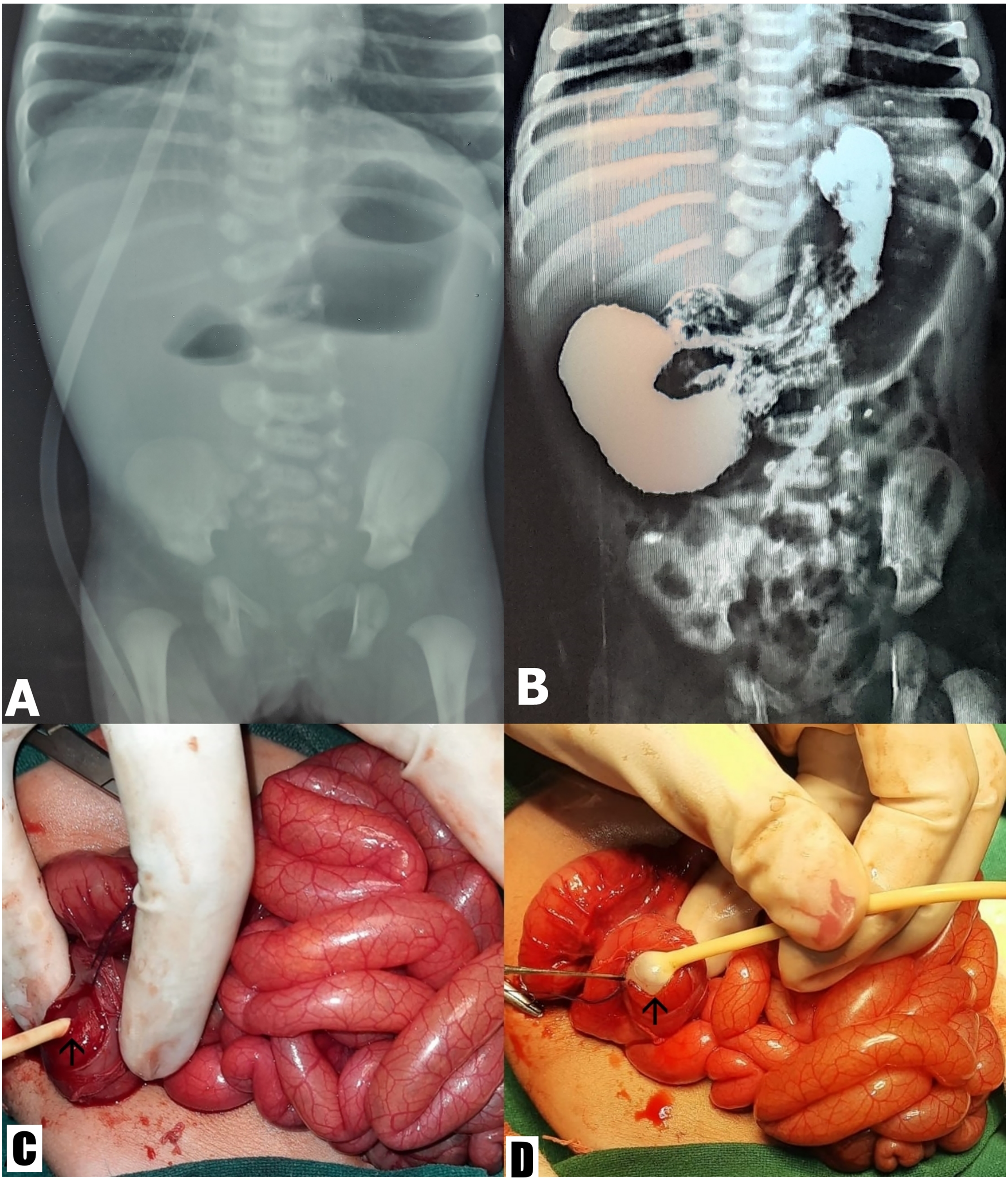
(A) Abdominal radiograph showing multiple air-fluid levels with absent distal gas; (B) upper gastro-intestinal contrast study showing obstruction in the third part of the duodenum; (C) web (arrow) exposed through enterotomy; (D) web (arrow) excision performed.
Case 2
A 3-year old girl presented with a six-month history of episodes of bilious vomiting and epigastric fullness after feeds. On examination, she was malnourished and had epigastric fullness. Routine blood investigations revealed anaemia (Hb 79 g/l). A barium meal was suggestive of dilation of the stomach and first, second and third parts of the duodenum, with minimal passage of contrast in the distal segment (Fig. 2(A) and (B)). An abdominal CT scan was suggestive of abrupt narrowing at the junction of D3 and D4, with a small fluid-filled beak-like luminal projection into D4 with resultant gross gastric and duodenal dilation (Fig. 2(C)).
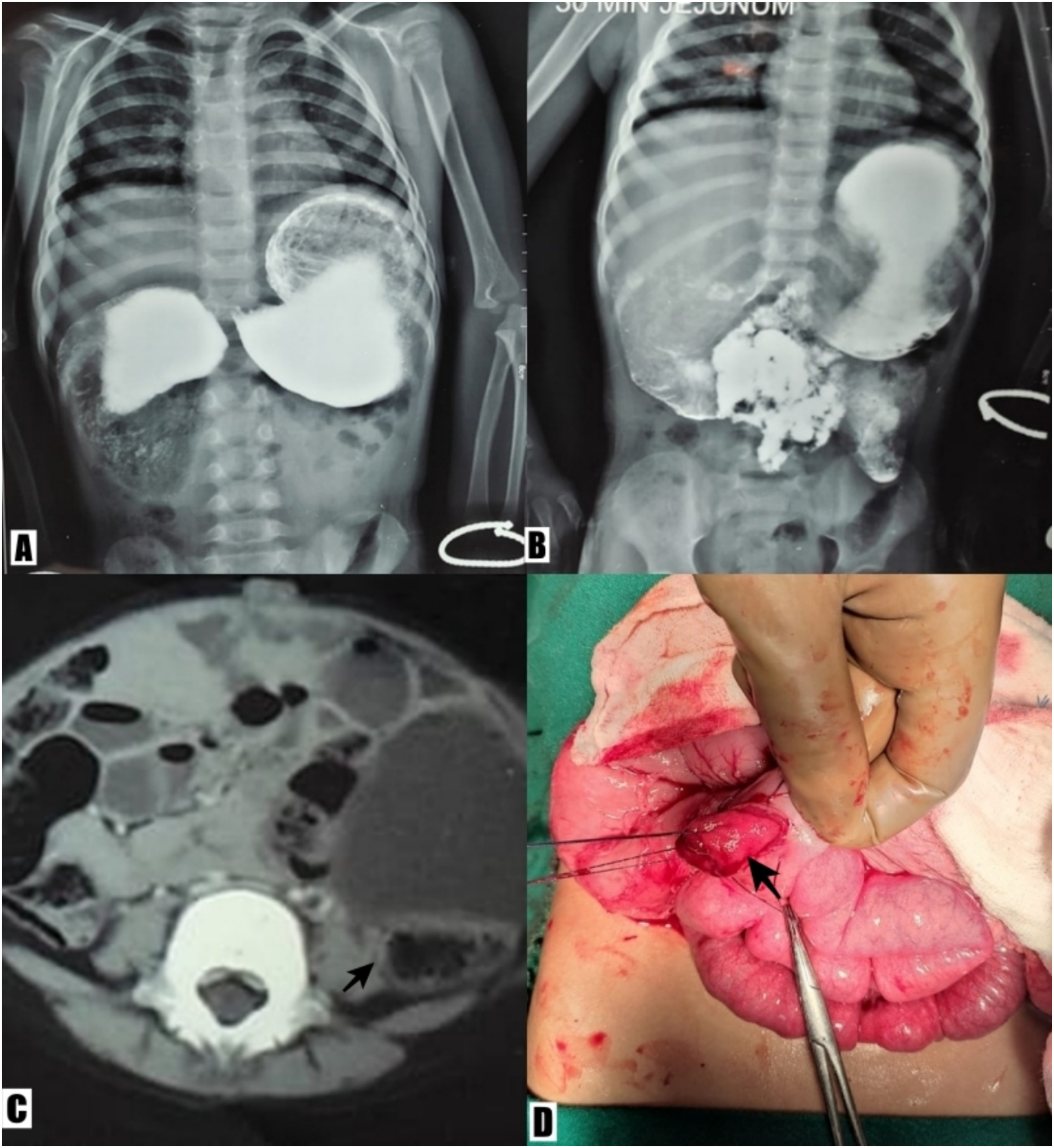
(A, B) Barium meal showing stomach and the first, second and third part of the duodenum dilated, with minimal passage of contrast in the distal segment; (C) abdominal CT scan showing abrupt narrowing at the junction of D3 and D4, with a small fluid-filled beak-like luminal projection (arrow) into the D4; (D) web (arrow) exposed through enterotomy.
On laparotomy, malrotation was present, for which Ladd's procedure was performed. The aforementioned dilation was found, with an abrupt transition at the junction of D3 and D4. Keeping in mind the possibility of a wind-sock deformity, we looked for the base of the web. However, no indentation indicating the base of the web visualised in D2 and D3 was found. The ring was felt at the junction of D3 and D4. A Fogarty catheter was passed orally which coiled up in D3 and could not be negotiated into D4. An enterotomy was opened in D3, and a mucosal web was noted at the junction of D3 and D4. A Ch8 Foley catheter was passed across the web defect and the web was pulled out through the enterotomy and excised (Fig. 2(D)). The enterotomy was subsequently closed. Post-operatively, the child was started on feeds orally on the fifth day and discharged on the ninth. Follow-up at 1 year showed normal development.
Discussion
Type I duodenal atresia is the most common type constituting c.92% of cases in which an obstructing web is seen. 1 The base of the web is usually located in D2. 3 In these two patients, the base of the web was located in D3. Congenital webs in the distal duodenum are rare. 2
During the sixth week of foetal development, the duodenal epithelium proliferates, thus obliterating its lumen and converting it into a solid cord. 4 It forms vacuoles that fuse to form a lumen. The hepato-pancreatic duct and accessory pancreatic duct open in D2 which form the area of traffic jam. Recanalisation of both ducts can interfere with normal recanalisation of the duodenum. So, most of the atresias occur in D2. 4 The direction of recanalisation of the duodenum is cranio-caudal. The probable aetiology that can lead to atresia in the distal duodenum is the failure of progress of the recanalisation process to the distal duodenum. 2
The duodenal web may or may not have a fenestration. 5 Webs with larger fenestration can remain asymptomatic and therefore have a delayed presentation. If the web has a small fenestration or none at all, distention by intestinal contents may lead to ballooning of the web distally into D3 or D4, producing a windsock effect. Duodenal dilation distal to the web can make it difficult to localise the web. Before enterotomy, the level of the base of the web should be anticipated. In cases with a wind-sock deformity, the change in the calibre of the intestine may give a false impression regarding the level of its base. Indentation visualised there and the feel of the ring can help in localising its origin.
Malrotation with small bowel volvulus also has a similar clinical and radiological presentation. After correction of the malrotation, a change in the duodenal calibre should be looked for. Malrotation may be associated with a duodenal web, which might be missed if a surgeon is not forewarned. An upper gastrointestinal contrast study is useful in making a pre-operative diagnosis. However, differentiating it from malrotation may still be challenging.
Thin webs, as in our patient, can be excised. 5 The most common location of the duodenal web is D2. If the ampulla of Vater is on the medial side of the web or not visualised, only the lateral side of the web is excised. If adequate web excision cannot be performed, a bypass should be done. In the distal duodenal web, there is no chance of damage to the ampulla, and therefore no danger exists.
With advances in laparoscopy, even children with a weight <3 kg are successfully treated laparoscopically. 6 There is difficulty in identifying the extent of the web from the mucosa of the duodenal wall laparoscopically, because of the lack of tactile sensation. There is also a risk of damaging the Ampulla of Vater. Consequently, some surgeons prefer duodeno-duodenostomy over web excision during laparoscopic surgery. 7 A recent study has proved the usefulness of intraduodenal indocyanine green injection for localisation of the duodenal web during laparoscopic surgery. 8
Some cases are reported to have been successfully managed endoscopically. 9 Dilation with the balloon is preferred as incising the web can damage the ampulla. 9 However, the major limitation is the non-availability of the facility, as well as inexperience of the endoscopist.
To conclude, congenital web in distal duodenum is rare but should be anticipated. It may mimic the wind-sock deformity and should be carefully differentiated from it. It may be accompanied by malrotation which can mask the duodenal web. The non-passage of contrast may not be solely attributable to malrotation. The duodenal web itself may be missed if the surgeon is not diligent.
Footnotes
Author contributions
Concept: RN, VP. Design: RN, GS, VP, SK. Definition of intellectual content: RN, VP. Literature search: RN, SK, GS. Manuscript preparation: RN, SK, GS. Manuscript editing: RN, VP. Manuscript review: RN, VP. All authors have read and approved the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.