
Abstract
Retained needle fragments can occur in intravenous drug user (IVDU), which can lead to significant morbidity and mortality. The aim of present study is to give an overview of our institutional experience and treatment protocol followed for such patients. IVDU with retained fragment of fractured needle were taken from the patient presenting in Emergency, Medicine and CTVS departments with history of IVDU, from January 2019 to December 2020. Six patients were found with retained broken needles. Detailed history, examination and investigations were done. The needle was removed under local anaesthesia successfully in all patients. IVDU with retained broken needle poses risk for catastrophic complications along with possibility of local complications. A systematic approach in managing such patients is required. These broken needles can be successfully retrieved as day care procedure. Lastly, IVDUs with fractured needles pose threat to the caregivers who should take caution to avoid iatrogenic injury.
Introduction
The incidence of broken needle remaining in situ is common (20%) among intravenous drug users (IVDUs). 1 Sites of retention vary.2–4 Descriptions of embolic complications of needle fragments are plentiful,5,6 but no protocol or guideline exists for the safe management of symptomatic chronically retained needle parts.
Materials and methods
From January 2019 to December 2020, patients with a history of broken hypodermic syringe needle in their forearms after injecting themselves with narcotics were recorded.
Details of substance used and years of IV drug abuse were recorded. Routine blood investigations, liver function tests, including viral markers (HIV, Hepatitis B and C) were done. A radiogram (Figs. 1 and 2) of the needle site was taken; ultrasound guided location and marking of the needles completed the investigation (Fig. 3).
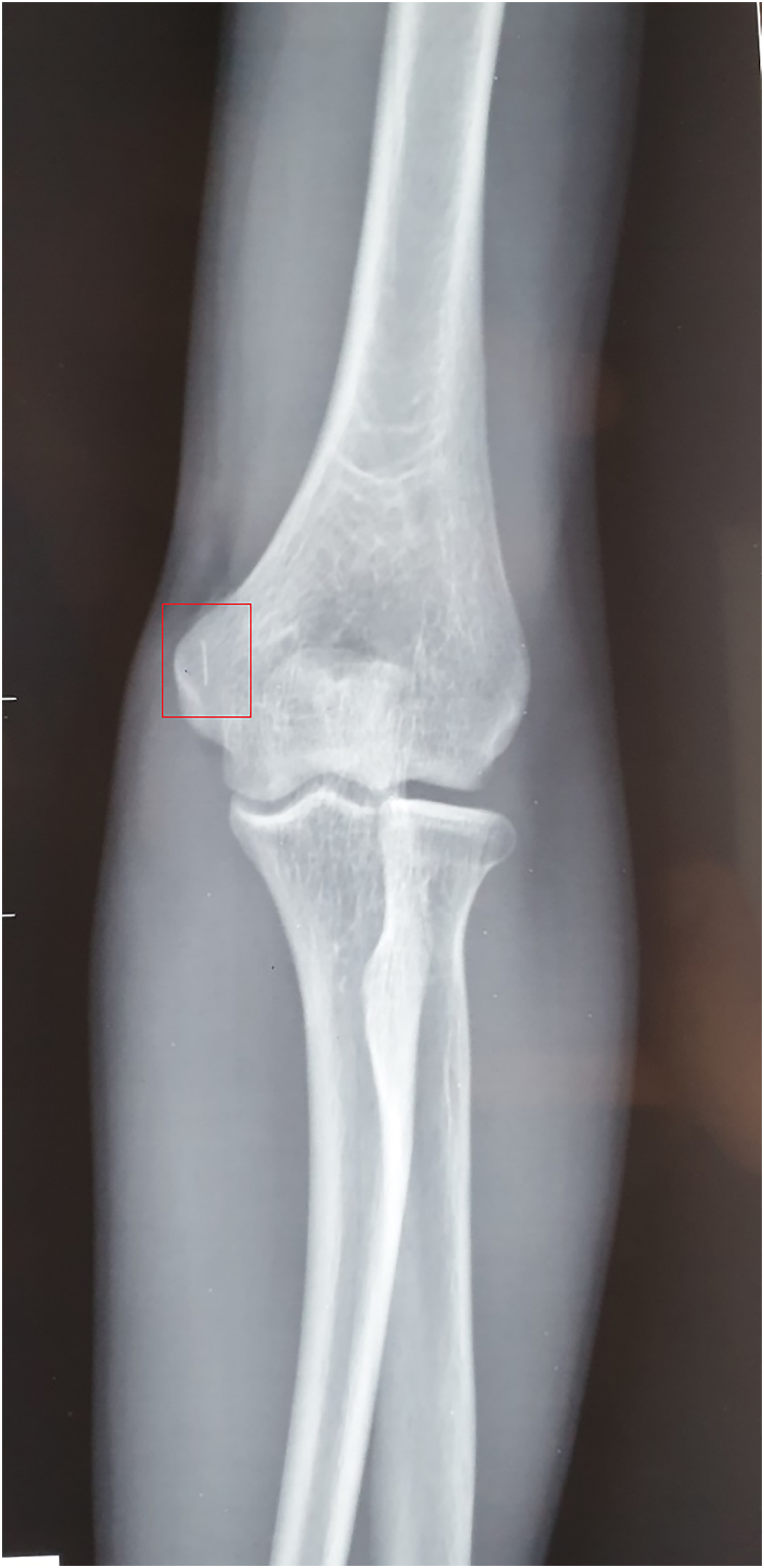
Anterior posterior radiograph of elbow joint of patient showing metallic foreign body (box).

Lateral view radiograph of elbow joint of patient showing metallic foreign body (box).
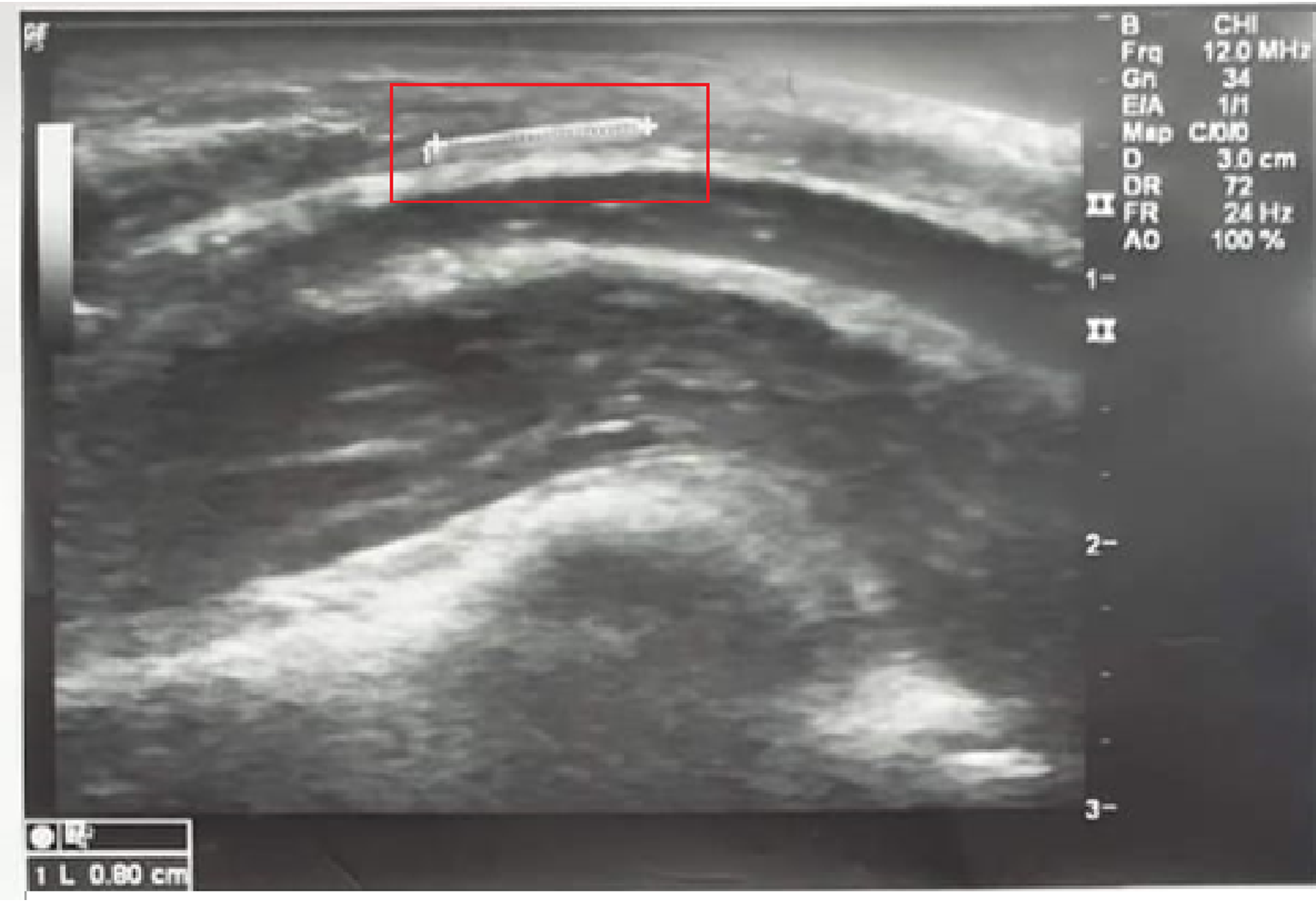
Ultrasound of elbow joint of patient showing metallic foreign body of 0.8 cm length (box).
Counselling and psychological addiction help was provided.
Operative procedure
Removal of the retained needle was carried out under local anaesthesia and C-arm guidance. With the patients supine and the arm extended on a side-table (Fig. 4), an arterial tourniquet was fixed proximally, the area was prepared with betadine from mid-arm to wrist and draped exposing the marked region. 10 mL of 1% lignocaine was introduced around the needle fragment site and a 3 cm oblique incision was made over the marked area.
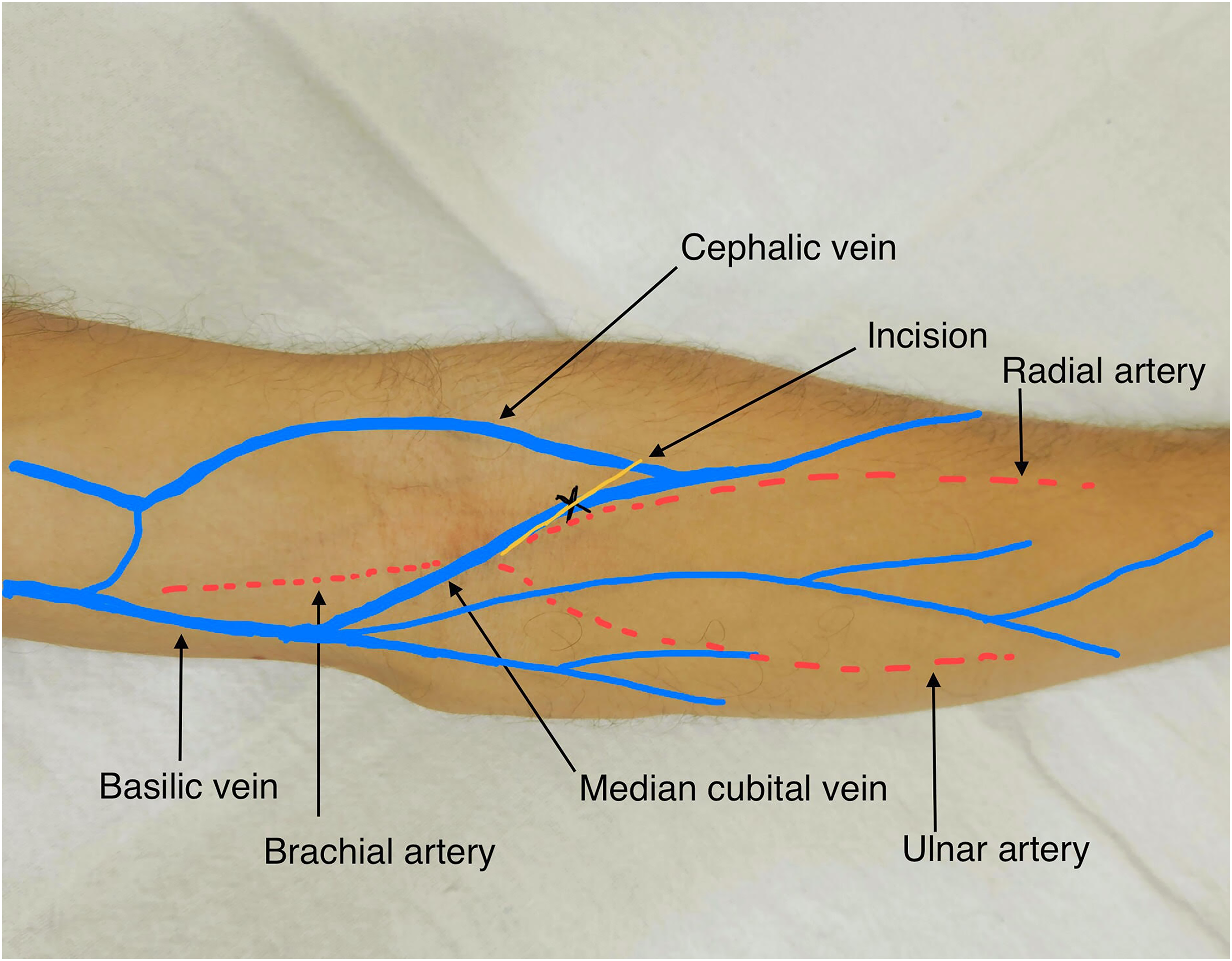
Outline of venous anatomy and incision site (X – ultrasound guided pre-operative mark).
Tissues were separated by blunt and sharp dissection under C-arm guidance. Digital dissection was avoided. An additional 5 ml of diluted lignocaine was used in deeper tissues. Once the foreign body was located, the vein was controlled both proximally and distally, and the vein incised longitudinally to remove the needle. The vein was then ligated at both ends with 2/0 silk, the tourniquet released and haemostasis checked. The area was washed with saline and the wound was then closed in two layers. A dressing was applied and patient discharged with oral antibiotics and analgesics.
Patients were followed in the outpatient department after seven days and telephonic follow up checking on addiction rehabilitation was done up to six months.
The study was approved by the Institutional Ethics Committee. Informed written consent was taken from all the participants of the study group.
Results
Over a period of two years, out of 66 IVDU patients, six were included with a retained needle fragment. Only two were sero-negative (no detectable HIV, Hepatitis B or C markers). All were young adult males between the ages of 18 and 28 years. One patient absconded during work up. The narcotic used for injection was heroin in all cases, with dependence ranges from 2 to 4 years. All used insulin hypodermic syringes and injected themselves in the left arm. They reported breaking of the hypodermic needle during repeated flushing and aspiration of remaining drug substance in the syringe barrel. They all noted fear of the broken needle fragment migrating to the heart and mentioned a pricking sensation during elbow movements.
No retained fragments were left in situ; intra-operatively, soft tissues were scarred and the needle found in a vein already fibrosed, with an obliterated lumen and cord-like firmness (Figs. 5 and 6). All wounds were healthy on removal of sutures on the 7th postoperative day. One patient complained of tingling and numbness of the ipsilateral little and ring finger postoperatively. He was managed conservatively with pregabalin 75 mg once daily.

Intraoperative view of broken needle (arrow) lodged in scarred vein.

Extracted broken needle (box) compared to a No. 24 surgical blade.
On telephonic follow up till six months, three patients reported full rehabilitation, two were still undergoing treatment and one could not be contacted.
Discussion
Fracture and dislodgment of hypodermic syringe needle fragments occur in IVDUs due to attempts to gain IV access in heavily scarred tissue. This causes the needle to bend and ultimately to break. An incidence of 20% broken needles has been reported in IVDUs with 4 out of 70 participants requiring surgical intervention for their removal. 1 Pulmonary embolisation may occur, or embolisation to the right atrium or right ventricle may give rise to endocarditis, pericarditis, pericardial effusion and cardiac tamponade.7,8
Though needle fragments are found inside fibrosed veins, the chances of life-threatening embolic complications are minimal but some such cases have been reported. 9
Being foreign bodies, fragments may produce abscesses or cellulitis at injection sites.10–12 Successful retrieval without major complications is possible with the help of a radiographic C-arm and ultrasound guidance. Nonetheless, with high risk of viral transmission, the procedure is not without hazard. Digital dissection is contra-indicated, even at autopsy. 13
Footnotes
Acknowledgements
We are thankful to the Department of Psychiatry, NEIGRIHMS, Shillong, India.
Data availability statement
Data, materials and hospital records are available. The datasets generated and/or analysed during the current study are available in the Medical Records Department of the NEIGRIHMS Hospital, Shillong repository, electronically on request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.