
Abstract

Introduction
Actinomycosis is a rare infective disease caused by anaerobic gram-positive commensal bacteria Actinomyces. Although typical anatomical sites remain uncertain, these commensal bacteria are mostly found in cervicofacial, pelvic, and foot regions. Actinomycosis occurs following a breach in the continuity of epithelium and immune suppression. The lesions are usually superficial nodulo-ulcerative containing characteristic ‘sulphur’ granules. However, sometimes they may be very large, fleshy and involving a deeper plane which may clinically and radiologically be confused as malignancy. Treatment includes long-term antibiotics with or without surgical debridement; hence early diagnosis is crucial in the management.
Case report
A 73-year old female presented with a 6-year history of a painless, ulcerating multi-nodular lesion in the left suprascapular region which bled on touch. Initially, the lesion had begun as a single nodule measuring 1cm, and gradually increased in size to 18 × 17 cm with multiple satellite lesions (Fig. 1a). Ulceration, yellowish granular discharge and peripheral crusting were noted. There was no history of trauma, past illness, or diabetes.

Clinical images (a) Pre-treatment showing multinodular ulcerated lesion showing multiple satellite nodules with peripheral brownish crusting and yellowish discharging sinuses containing sulphur granules, (b) Post-treatment image showing near complete healing with fibrotic scar of the lesion.
On examination, no significant lymphadenopathy was found. A CT thoracic scan showed an extensive lesion involving subcutaneous and deeper soft tissue, suggestive of malignant pathology (Fig. 2). A biopsy was taken which showed skin covered with surface ulceration, multiple colonies of actinomyces, and dense mixed inflammatory cell infiltrate in the dermis. A Spledore-Hoeppli reaction was also noted (Fig. 3a). Actinomyces colonies were Gomori methanamine silver (Fig. 3b), periodic acid Schiff (Fig. 3c), and Gram stain (Fig. 3d) positive. Ziehl Neelsen stain for acid fast bacilli was negative.
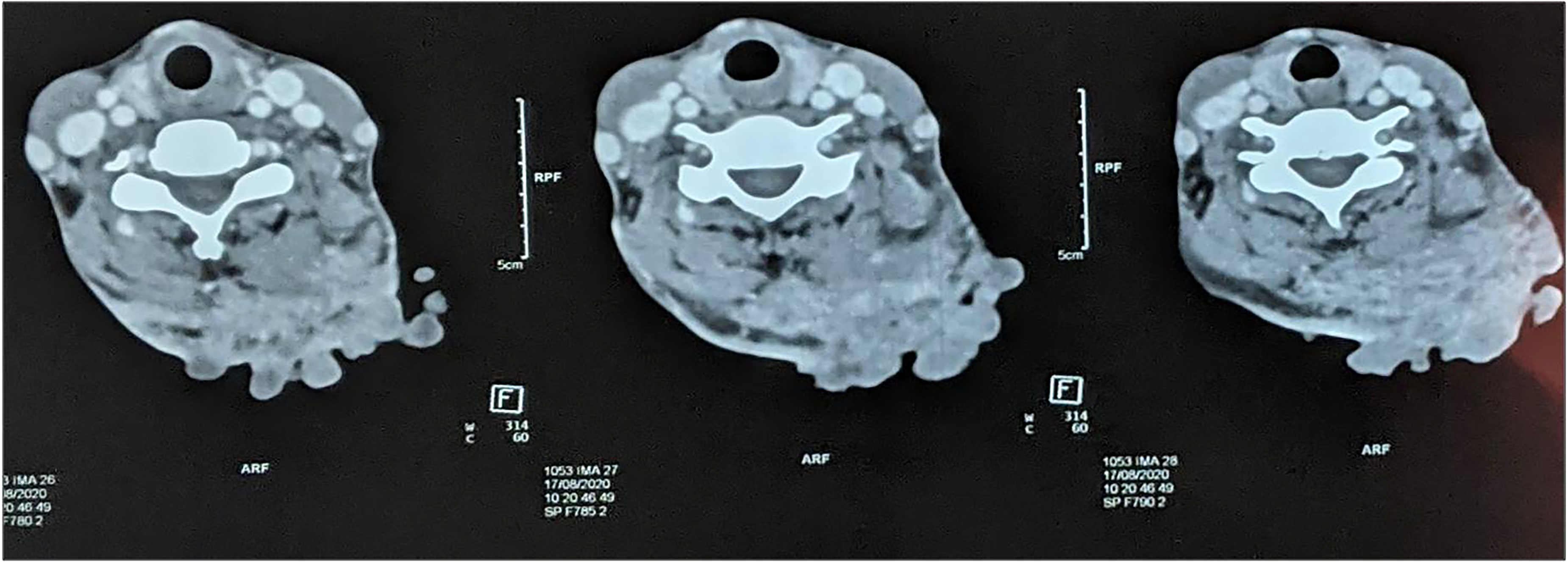
CT scan axial section showing an irregularly marginated heterogeneously enhancing soft tissue density lesion in left upper back abutting the left trapezius and rhomboid muscles with loss of fat plane. The lesion is involving subcutaneous tissue with overlying skin, causing irregular bulging.
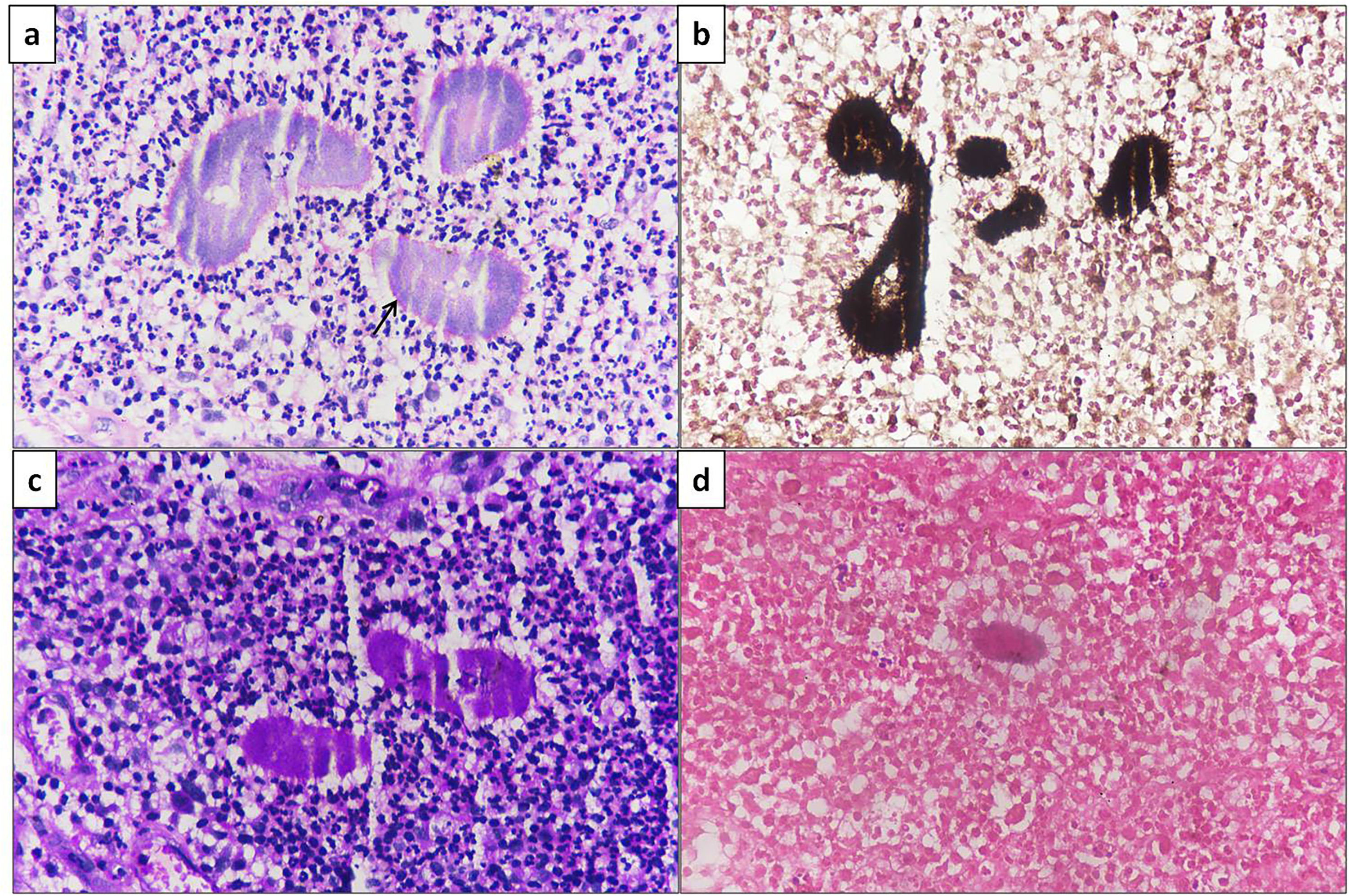
Histopathological examination showing (a) colonies of actinomyces with Splendore–Hoeppli reaction (Arrow) surrounded dense mixed inflammatory cell infiltrate and granulation tissue (HE ×400), (b) Gomori methanamine silver, (c) periodic acid Schiff and (d) Gram stains highlighting and showing positivity in Actinomyces colonies [×400 each].
Ampicillin-clavulanic acid was given for 12 weeks and at nine months of follow-up there was significant improvement with near total healing (Fig. 1b).
Discussion
Actinomyces is a gram positive anaerobic filamentous commensal bacteria belonging to the family Actinomycetaceae. There are six species responsible for human disease among which Actinomyces israelii is the most common. Based on site, actinomycosis is broadly classified into four types as cervicofacial, thoracic, abdominal, and pelvic.1,2 Primary cutaneous actinomycosis is a rare form usually preceded by a history of trauma, as epithelial disruption is required for infestation and spread to deeper tissue. 3 However, such trauma may be minor and not recalled. Actinomycosis is recognized by the WHO as a neglected disease; most of the literature reports late presentations. Though Actinomycosis has a very slow progression, the toxins released lead to suppression of the local immune response.
The differential diagnosis includes cutaneous tuberculosis, Nocardia and malignancy. Lupus valgaris also produces sinuses which are not yellowish. ‘Sulphur’ granules are septic foci (<1 mm in size) in the ulcerated skin surface sinuses comprising filamentous Actinomyces colonies, acute inflammatory granulation tissue, and cell débris. Other superadded bacteria may also be present giving a mixed growth pattern on culture and create confusion in accurate typing of the infection. Moreover, ‘sulphur’ granules may also be seen in Nocardia, Streptomyces and some species of staphylococci. Thus the mere presence of ‘sulphur’ granules is not sufficiently diagnostic. However, the characteristic morphology on biopsy and peculiar molar tooth appearance of colonies in culture over chocolate agar are important diagnostic features. Actinomyces is acid fast negative which differentiates it from tuberculosis and Nocardia. Another valuable clue is that Nocardia is an aerobic organism, whereas Actinomyces grow under anaerobic conditions. 4 Bacterial colonies are surrounded by inflammatory micro-abscess comprised predominantly of neutrophils, plasma cells and lymphocytes - signs of suppurative inflammation.
Actinomyces spread across the tissue planes and invade deeper tissue. Soft tissue involvement may give a false impression of malignancy, particularly on CT scan, especially when there is deep tissue involvement in long-standing neglected cases. There is often a long time interval between the appearance of a skin lesion and its subsequent diagnosis.
The effective treatment protocol includes high dose intravenous antibiotics for 4–6 weeks followed by oral antibiotics for 6–12 months. A patient who receives only a short course of prophylactic antibiotic therapy often later requires surgical excision owing to incomplete response. Beta-lactams including penicillin G are the treatment of choice. In penicillin-allergic patients, tetracycline, clindamycin, erythromycin, and chloramphenicol may be used.5,6 Amoxicillin/clavulanate can be used for cutaneous actinomycosis as suitable oral agents for a maximum of 12 weeks with considerable efficacy. 7
Footnotes
Authors’ contributions
Rakesh Kumar Gupta, MD: Concept of work, Intellectual content and finer editing
Kartavya Kumar Verma, MD: Collection of data and drafting the manuscript
Radhakrishna Ramchandani, MS: Clinical work-up and literature review
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Availability of data and material
Yes
Ethics approval
Not applicable
Patient consent for publication
Taken