
Abstract
Mycetoma is a suppurative chronic bacterial or fungal disease inoculated into the body by minor trauma which may penetrate from subcutaneous tissue to bone. Although the lower extremities are most commonly affected, rare forms can also be seen from time to time. The diagnostic triad of swelling in the affected area, multiple sinus formation, and purulent discharge with grains are typical. Definitive diagnosis is made by isolation of the causative pathogen, radiologic imaging, and histopathologic examination. Antifungal and antibacterial options are applied together with surgery. Our aim in this case series is to report and analyze 10 rare cases of mycetoma.
Introduction
Mycetoma is usually found in tropical and sub-tropical climatic zones, the regions known as the “Mycetoma Belt” (latitude 30 N to 15 S). 1 The disease is chronic and characterized by swelling, fistulae, and extrusion of grains; suppurative lesions affecting the skin and subcutaneous tissues and may reach bone. Bacterial and fungal pathogens cause similar clinical manifestations.2,3 The most common causative agent of eumycetoma in Africa is Madurella mycetomatis and of actinomycetoma are Actinomadura madurae and Streptomyces somaliensis. 4 Entry is via minor trauma.5,6 Incubation ranges from three months to many years. The causative trauma is often forgotten on presentation. 1 Surgical treatment and long-term antimicrobial therapy are advised, but the treatment response is poor, and the duration of treatment must not be shorter than one year. 7
Material and methods
All patients previously diagnosed with mycetoma and those newly diagnosed in our outpatient clinic were included in the study. Since fungal culture could not be performed in our centre, we relied on diagnosis by biopsy. A detailed history was taken from all patients. Gender, age, physical examination findings, region of residence, diagnosis, treatment, and duration were recorded. Recurrence status and whether previous treatment had been given was noted.
Results
Ten cases were analyzed. The lower extremities were usually affected (Fig. 2). Two cases had thoracolumbar (TL) region involvement. The case with extensive TL lesions underwent a surgical procedure. After surgery, the lesions spread to the whole TL region.
All wounds were chronic. All lived in rural areas and generally were engaged in the care of livestock or farming. One was a porter and another a bus driver. Diagnosis was made by biopsy (Fig. 1). As no fungal cultures were available, treatment was planned empirically or according to the biopsy results. Itraconazole 100 mg with amoxicillin-clavulanic acid 1G bd or Monocycline 100 mg bd or trimethroprim-sulfamethoxazole bd combinations were prescribed for at least one year. Surgical treatment was performed on one knee because of suspicion of malignancy. Recurrence was seen one year after treatment had been stopped in two patients (Table 1).
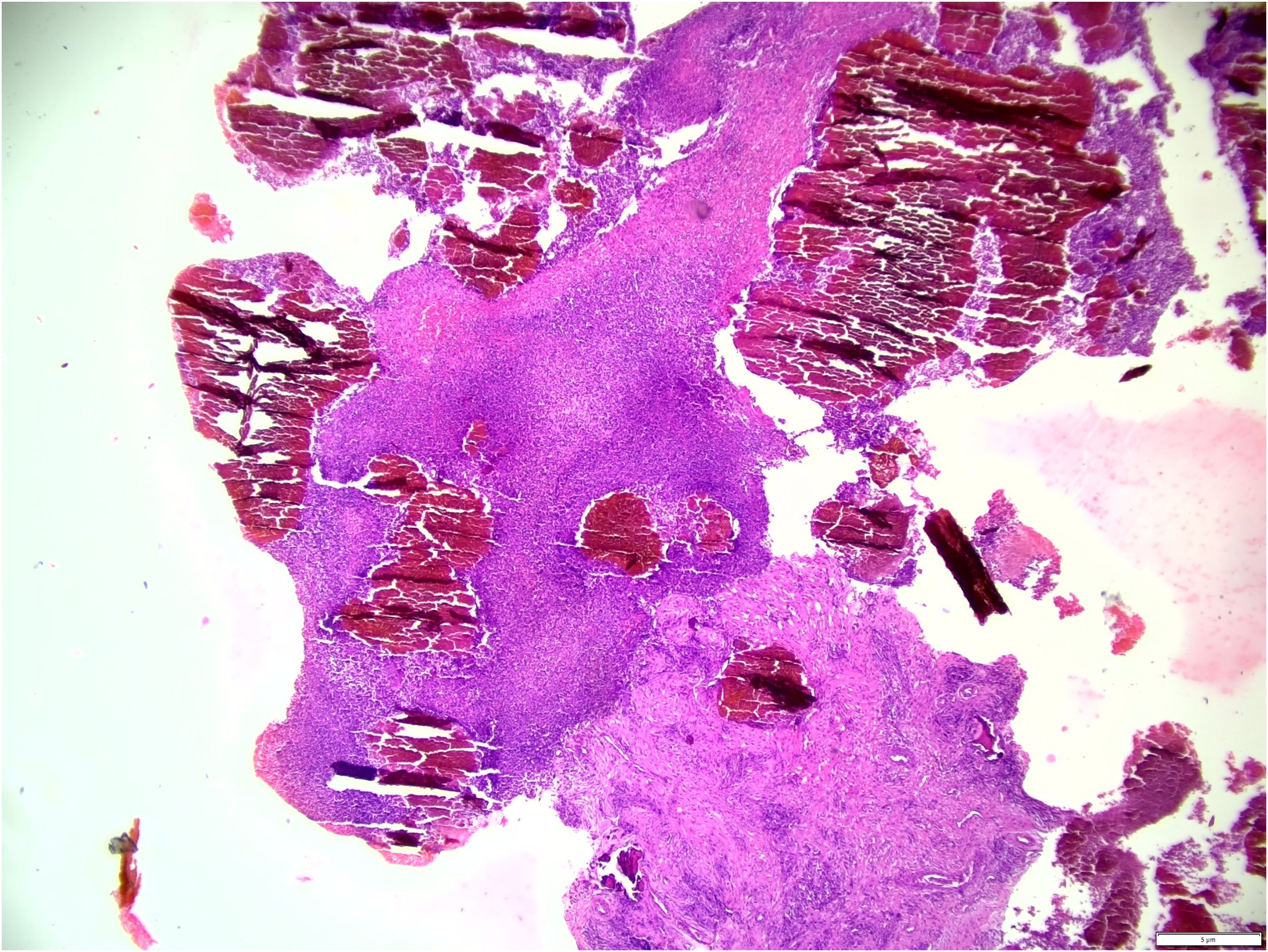
Microscopic view of mycetoma biopsy.

Upper right foot.
Mycetoma cases.
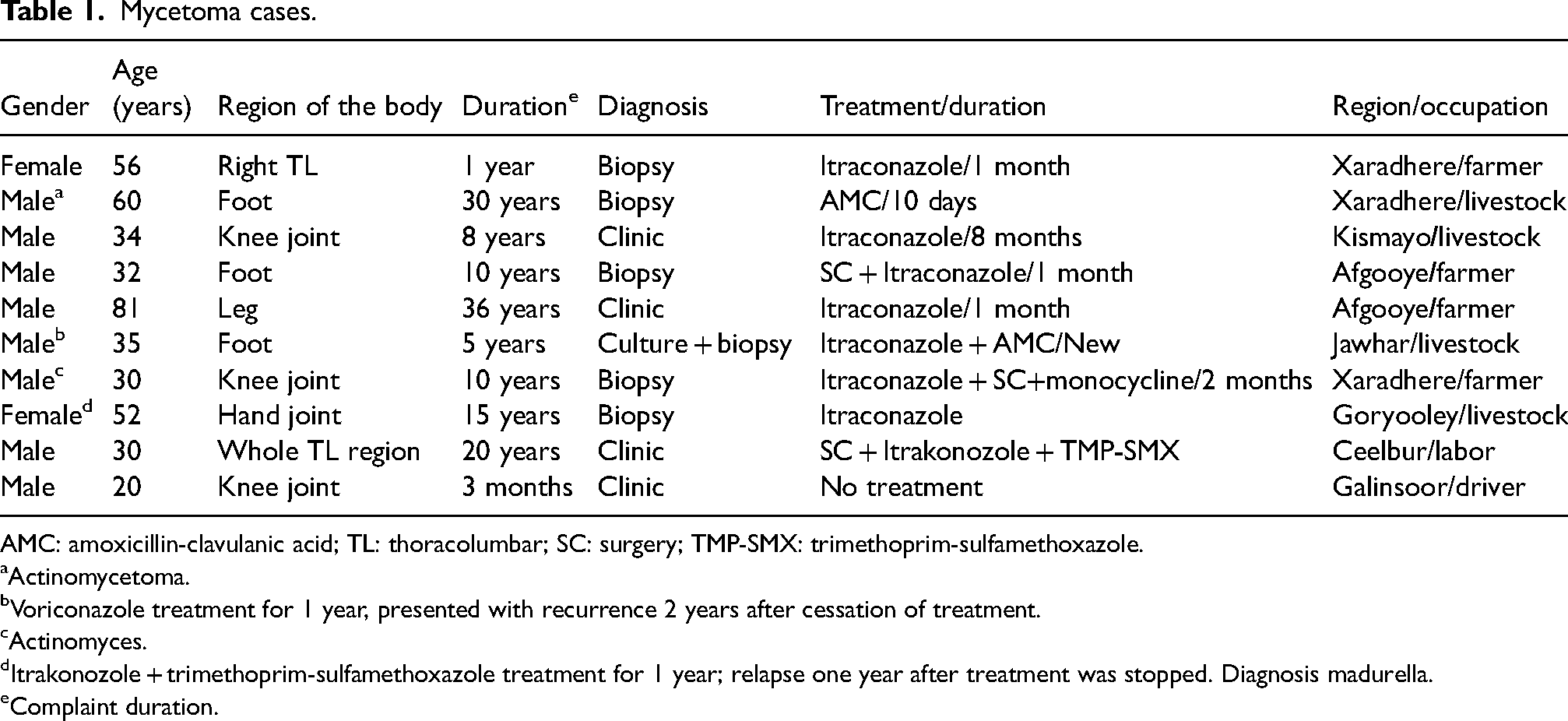
AMC: amoxicillin-clavulanic acid; TL: thoracolumbar; SC: surgery; TMP-SMX: trimethoprim-sulfamethoxazole.
Actinomycetoma.
Voriconazole treatment for 1 year, presented with recurrence 2 years after cessation of treatment.
Actinomyces.
Itrakonozole + trimethoprim-sulfamethoxazole treatment for 1 year; relapse one year after treatment was stopped. Diagnosis madurella.
Complaint duration.
Discussion
Since mycetoma occurs as a result of minor trauma, lesions are usually seen in the lower extremities, especially in barefoot workers. The feet are most commonly affected.
Lesions on the hands are seen second in frequency. The head and neck region, chest, back, and fingers are less commonly affected. For eumycetoma and actinomycetoma, the common areas of lesions are similar, but the locations of rare areas differ.8,9 While mycetoma is three times more common in men than in women, this may be due to more men working in farming, care of livestock, and construction. Higher levels of progesterone and oestradiol in women may be protective.10,11
Actinomycetoma responds more rapidly to antibiotic treatment than eumycetoma. Trimethoprim-sulfamethoxazole (TMP-SMX) is still the gold standard of treatment, but combination regimens with Amikacin, carbapenem, or amoxicillin-clavulanic acid (AMC) are also available.10,12 In the treatment of eumycetoma, the benefits of surgical treatment have been shown. Antifungal treatment with ketoconazole or itraconazole needs long periods of time to be effective. 1 Relapse was nonetheless observed in some cases. Surgical extirpation may, however, reduce the frequency of relapse.
Conclusion
The risk of mycetoma is high in the central regions of Somalia amongst middle-aged farmers or livestock breeders. There are difficulties in obtaining a definitive diagnosis. Effective prolonged treatment is usually successful.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.