
Abstract
Scrub typhus is a re-emerging and endemic disease in the Asia Pacific region caused by Orientia tsutsugamushi. We present a 65-year-old male from Sri Lanka who presented with fever, bilateral acute sensorineural hearing loss, and confusion. On examination, he was dehydrated. Significant orthostatic hypotension and an eschar were noted. Investigations revealed hyponatraemia with elevated urine sodium, reduced serum osmolality, and normal urine osmolality suggestive of cerebral salt wasting. After initial hydration with 0.9% NaCl, hyponatraemia was corrected with 3% NaCl. Oral doxycycline was prescribed, and he showed dramatic clinical improvement. A diagnosis of typhus must be considered in a patient presenting with a febrile illness and acute hearing loss. Cerebral salt-wasting disease should be considered in a patient with typhus who develops hyponatraemia with dehydration. Furthermore, acute sensorineural hearing loss in both ears is an important manifestation of the disease.
Introduction
Scrub typhus is caused by Orientia tsutsugamushi and is introduced through the bite of an infected trombiculid mite. The disease is re-emerging and is endemic in the Asia Pacific region.1,2 The most common clinical presentations include intermittent fever, headache, lymphadenopathy, and conjunctival injection. An eschar is seen in around 48–82% of patients. 3 Deafness develops in around one-third of patients. The cerebral salt-wasting disease has been rarely reported with scrub typhus infection. 4 We present such a case.
Case Report
A 65-year old man from suburban Colombo in Sri Lanka presented with fever, chills, and rigors of 12 days’ duration. He had generalized myalgia, headache, increased urinary frequency, and acute onset hearing impairment, which had developed on the second day of the illness. He developed confusion and drowsiness on the day before admission.
On examination, he was febrile at 38.5°C. He was drowsy with a GCS of 13/15. There was no neck stiffness. He was dehydrated with dry mucous membranes, prolonged capillary refill time, and reduced skin turgor. Mild orthostatic hypotension was observed with 128/80 mmHg supine and 106/76 mmHg erect at 3 min. There was no lymphadenopathy or hepatosplenomegaly. His respiratory system examination was normal and there were no significant murmurs or peripheral stigmata of infective endocarditis. The neurological examination was normal except for a reduced whisper test and impaired Rinne's and Weber's tests bilaterally. An eschar was noted over his right arm (Fig. 1).
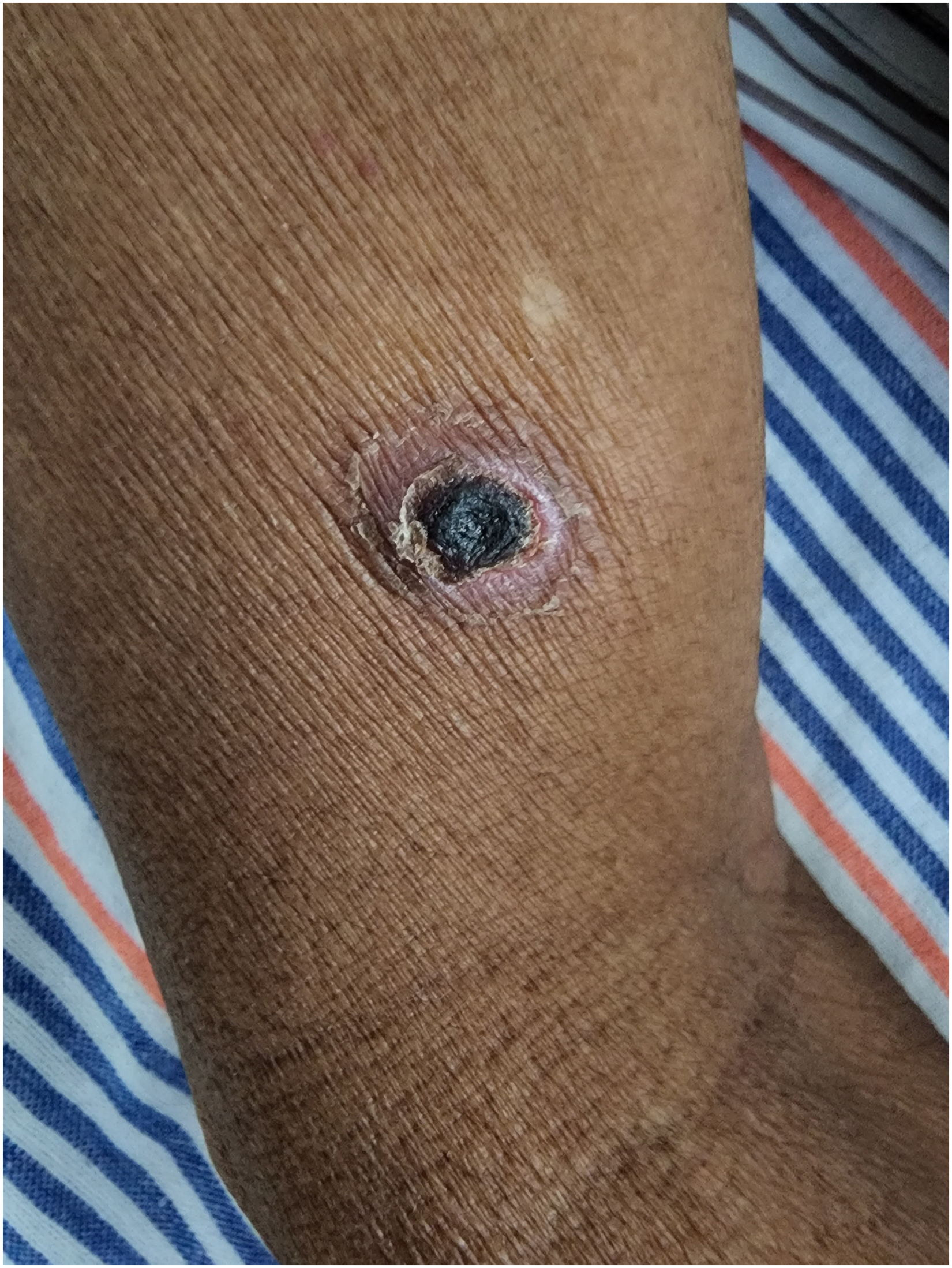
Eschar over the right arm of the patient.
There was a leucocytosis (10.9 × 109/L with 78.7% neutrophils and 16.6% lymphocytes). He was mildly anemic (Hb 122g/L) with normal thrombocythaemia (239 × 109/L). C-reactive protein was elevated at 1310 mg/L. Erythrocyte sedimentation rate was 35 mm/1st h. Aspartate aminotransferase was marginally elevated (58.4 U/L). Alanine transaminase (36.8 U/L), total bilirubin (16.6 μmol/L), serum creatinine (70.5 μmol/L), urea (3.0 mmol/L), serum calcium (2.4 mmol/L), and serum potassium (4.0 mmol/L) were all normal. Serum sodium was low (116.8 mmol/L) but urine sodium was high (60 mmol/L). Serum osmolality was 271 mOsm/kg while urine osmolality was 350 mOsm/kg. He had a urine output of 4300 mL for 24 h with a total intake of 2400 mL. Non-contrast computerized tomography scan of the brain was normal. A diagnosis of cerebral salt wasting was made based on the presence of hyponatremia with dehydration, reduced serum osmolality, normal urine osmolality, and high urine sodium. Weil Felix test for rickettsial infection was positive. Pure-tone audiometry revealed bilateral profound sensorineural hearing loss (Fig. 2).
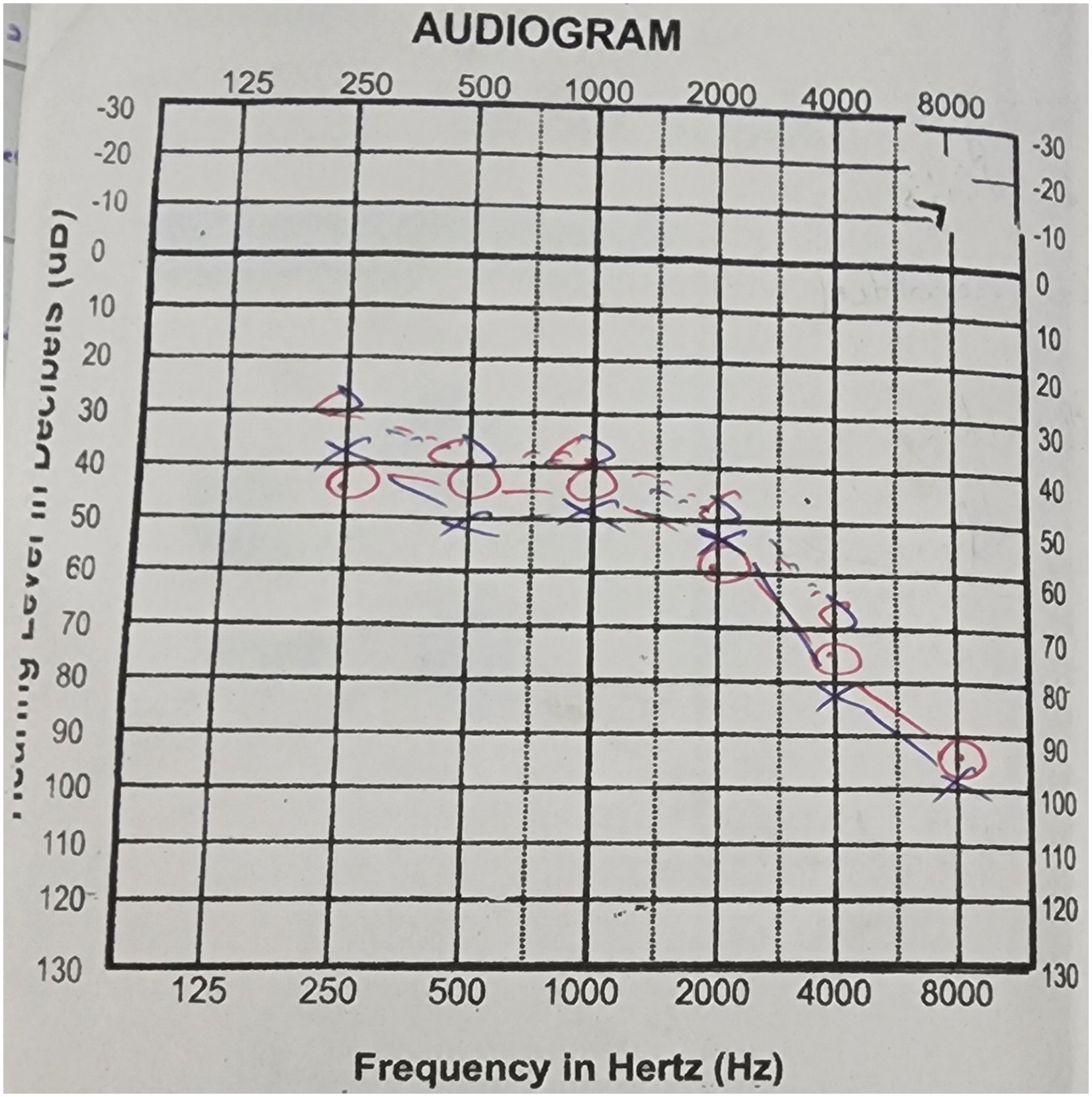
Audiogram of the patient.
The patient was hydrated with 0.9% saline and then 3% NaCl was administered since he had symptomatic hyponatremia. Oral doxycycline 100 mg bd was commenced and continued for 7 days.
Confusion and drowsiness improved with the correction of hyponatremia. The fever settled 24 h after the initiation of doxycycline. After 3 days, he could be discharged. After 3 months, partial deafness was still noted. His serum electrolytes had returned to normal.
Discussion
Hearing impairment is rarely seen in scrub typhus. 3 It usually manifests in the second week of the illness. 5 Muli-organ involvement is sometimes seen. 5 Sensorineural hearing loss has been reported in patients with Rickettsia rickettsii, R. typhi, and R.coronii. 6 Otalgia and tinnitus have also been documented. 5 The pathophysiology of hearing loss is not fully understood, but two mechanisms have been proposed. The first involves direct invasion of the central nervous system, causing vasculitis in the cochlear division of the 8th cranial nerve. The second involves a secondary immune-mediated vasculitis of the vasa nervorum of the cochlear nerve. 6 Improvement in hearing is noted with treatment with antibiotics, but may take up to 6 months. 3 Permanent hearing loss has also been reported, as in our patient. 7
Cerebral salt wasting (CSW) is rarely encountered with scrub typhus.4,8 The presence of hypovolaemic hypo-osmolar hyponatremia favors cerebral salt wasting as opposed to a syndrome of inappropriate antidiuretic hormone secretion where patients are euvolemic. 8 The treatment of CSW involves volume repletion and sodium replacement. 4
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient consent
The patient provided written informed consent for patient information and images to be published.