
Abstract
In order to synthesise the existing evidence of Traditional Bone Setters' (TBS) treatment and its associated complications in Low and Middle Income Countries (LMICs), we conducted a literature search following PRISMA guidelines. The keywords “traditional bone setter”, “traditional bone healer”, “traditional bone setting”, “fracture”, “complication”, “low income country”,” low to middle income country”, “poor outcome” and “death” were searched in PubMed. Articles included in the review demonstrated complications associated with treatment by TBS for Musculoskeletal injury in LMICs. Out of 878 papers screened, twelve studies were finally included for review. Seven were prospective, and five retrospective studies. All were observational studies with all but one hospital based, the remaining being community based, and investigated the outcomes of treatment of fractures by traditional bonesetters published between 1999 and 2020 in LMICs. In total, this review covers 833 participants with 691 complications of TBS treatment. We identify a significant number of limb and life-threatening complications including mortality associated with the treatment by TBS. However, recent studies have shown that TBS are willing and keen to engage with local orthodox services and training courses. As shown in many countries, this can lead to a reduction in complications including mortality and can form a favourable environment where TBS and orthodox services can work side by side.
Introduction
Bone setting is the practice of joint manipulation and treatment of fractures, and TBS practice has been and still is an important part of health care delivery in many LMICs long before orthodox medicine was introduced. 1 TBS is a speciality within Traditional Medicine that is usually passed from father to child whilst some non-family members might receive training via an apprenticeship. There would be no formal teaching as in modern day medical practice. 2
Despite advances in modern day healthcare through technology and medical research,TBS has continued as an alternative health care service. It is practised in many communities of the world, especially LMICs in the continents of Asia, South America and Africa where there are less developed healthcare resources and TBS play an important role in the healthcare delivery system. According to one estimate, between 10 to 40% of patients with fractures and dislocations in the world are managed by an unorthodox TBS. 2 Despite the complications that arise from this cultural practice, TBS services are still in high demand by a significant number of people. 3
In most low-income countries where traditional bone setting is practised, many failures of bone setting procedures have been reported to be due to the use of unscientific methods adopted by TBS. These methods of treatment lack the knowledge of anatomy, physiology, radiology and basic principles of infection prevention and control and soft tissue care. Thus limb and life threatening complications, 4 which range from acute compartment syndrome, tetanus, deformities, chronic osteomyelitis, gangrene, amputation and death, 5 have become a major concern with regard to morbidity and mortality.
Material and methods
This systematic review was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 6
An attempt was made to register the study with PROSPERO, but this tool was not accepting registrations for scoping, literature, or mapping reviews and thus a registration number code was not provided. 7
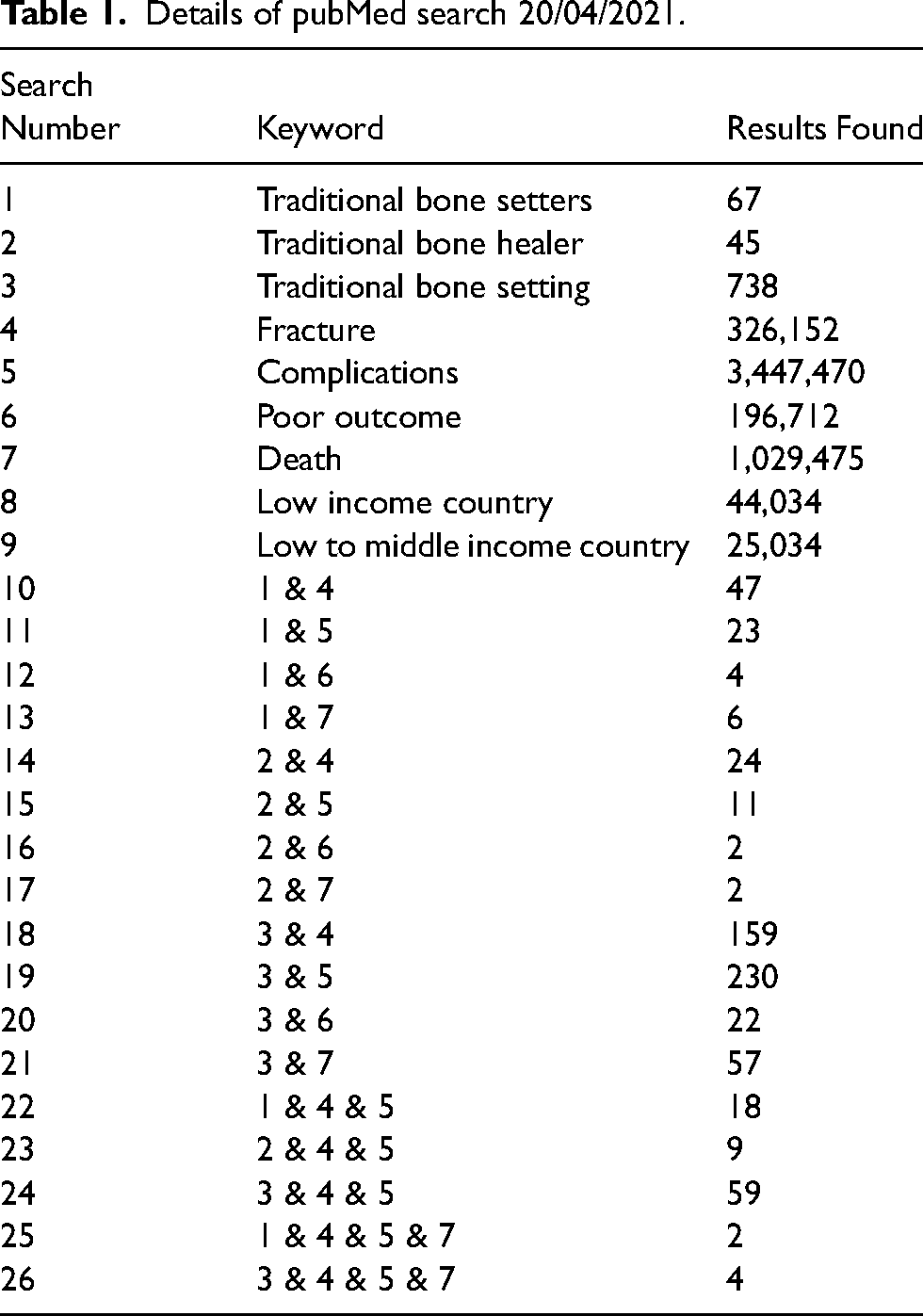
The PUBMED electronic database was searched from its inception in January 1996 to 20th April 2021 to identify relevant studies and articles. Within the database, the following keywords were used: Traditional bone setter, traditional bone healer, traditional bone setting, fracture, complication, poor outcome, death, low income country, low to middle income country.
Relevant articles were also searched for by hand search of reference lists.
Table 1 shows the combination of keywords during literature search from PubMed.
Details of pubMed search 20/04/2021.
Eligibility criteria were informed using the SPIDER guidelines
8
:
(S) Sample: Any patients who have experienced treatment by TBS and had complications due to this treatment (PI) Phenomenon of Interest: TBS and associated complications (D) Design: All types of observational study; cohort, case control, single case studies (E) Evaluation: The use of TBS in various countries and the complications reported were evaluated (R) Research type: qualitative, quantitative and mixed-methods research were searched.
Papers not written in English and studies describing patients outside of LMICs, as defined by the World Bank 2021 list,
9
were excluded.
One author (VG) searched information sources independently and assessed identified studies for inclusion, facilitated by grading each eligibility criterion as eligible, not eligible, or might be eligible. 10 The full text of a study was reviewed and was considered potentially relevant when it could not be clearly excluded on the basis of its Title and Abstract (CRD, 2009). The full text was then obtained for abstracts if there was insufficient information. A study was included when it satisfied the inclusion criteria from the full text. Any indecision to include or dismiss a paper was decided upon by following a discussion with four other authors (DKY, MGM, KM, WJH).
One author (VG) extracted the data independently. A review meeting was held between all five authors following article selection to check the data for consistency and clarity. Data extracted included study design, date of study, country of study, sample size, sample characteristics including ages and gender, aetiology of injury, presenting injury (including whether the injury was an open or closed injury), treatment by TBS, types and frequency of associated complications (limb and life threatening) and subsequent corrective treatments required and outcomes.
Results
Figure 1 shows the flow of the search strategy criteria.
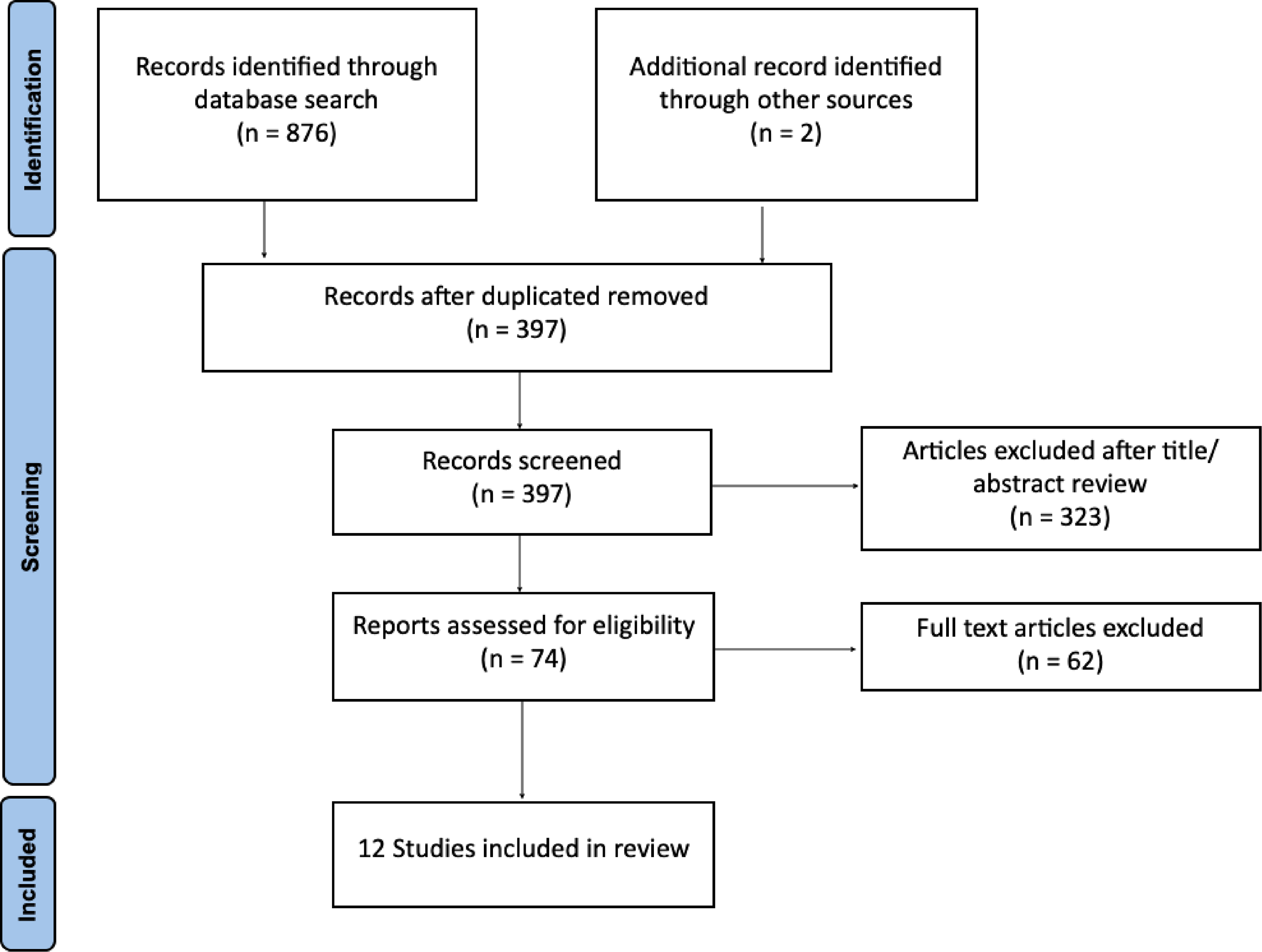
PRISMA flow diagram of article selection process.
The electronic database search yielded 876 potential articles and an additional two articles were found by hand search of the reference lists. Once duplicates were excluded, there were 397 articles eligible for further screening, which excluded 323 articles. Review screening of the remaining 72 full-text articles resulted in exclusion of 60 further articles, leaving twelve articles that have been included in this systematic review.
The main characteristics of the twelve articles are shown in Table 2
Characteristics of articles included in review.
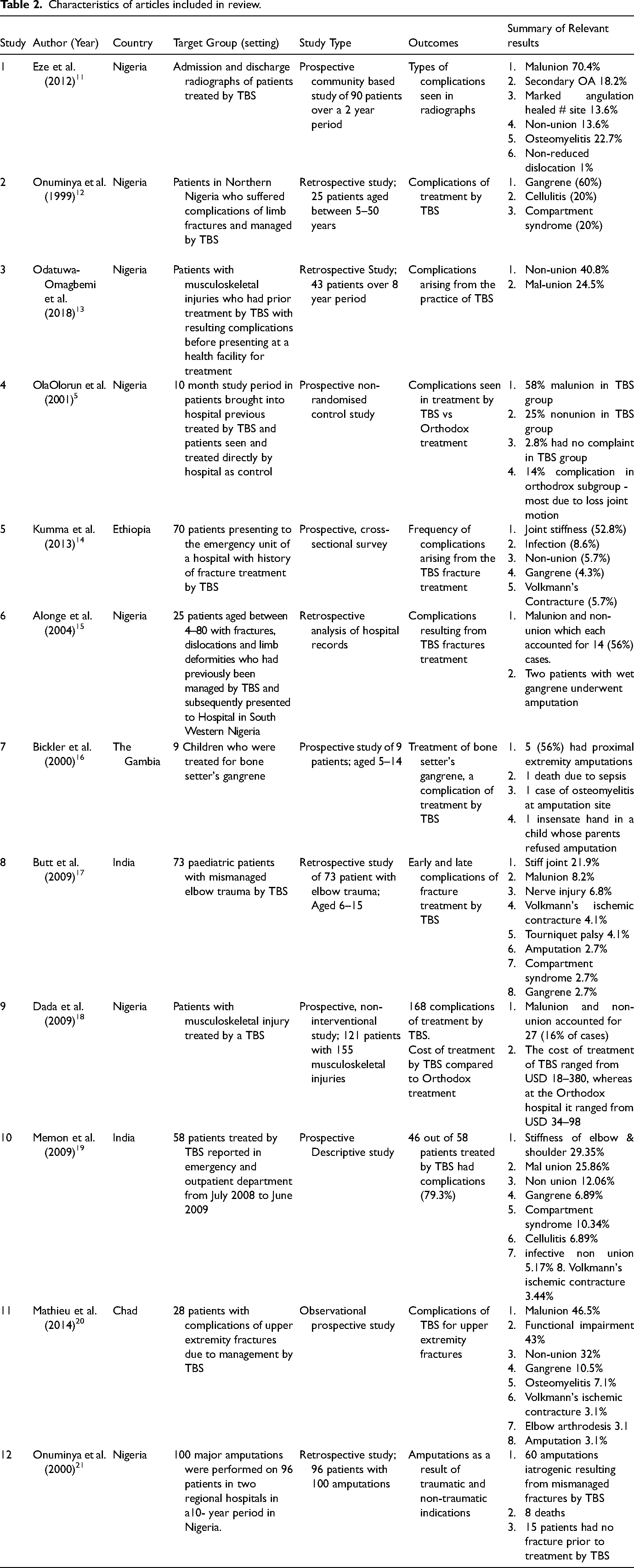
All but one article are hospital based with the one a community based study. Five were retrospective and seven prospective. Ten focus on countries within Africa including Nigeria, Ethiopia, The Gambia and Chad with the two others on an Indian population.
Many complications resulting from TBS treatment were cited, nine articles describing causative techniques used by TBS. Six articles described whether the injury concerned was open or closed. Three articles described upper limb injuries and the rest demonstrate upper and lower limb injuries. Nine articles described treatment methods utilised by TBS. All twelve articles discussed limb threatening injuries but only two discussed life threatening injuries resulting in death. The most common complications included malunion, non-union, gangrene, amputations and stiff joints.
A total of 833 patients were reported in whom there were 691 complications noted. Patient ages ranged from 6 weeks to 87 years. Two of the articles observed a specifically paediatric population. Only 7/12 articles specified the age of patients or categorised their ages, thus only 354/833 had their age documented. Of these, 180 were aged <18, 99 between 19–39 years, 56 between 40–59 years and 19 >60 years.
Observed patients comprised 64.7% males with a total duration of observation from recruitment to follow up ranging from 4 months to 10 years with a mean of 2.3 years.
Complications noted were 9 (1.3%) deaths, 139 (20.1%) amputations, 112 (16.2%) cases of gangrene, 16 (2.3%) compartment syndrome, 144 (20.8%) malunion, 92 (13.3%) non-union, 48 (6.9%) joint stiffness, 30 (4.3%) other infections, 22 (3.1%) Volkmann ischaemic contracture, 14 (2.0%) non-reducible dislocations and 62 (9.0%) other complications including nerve injury amongst others. Of the 112 cases of gangrene, 103 (92%) went on to have amputations.
Ten out of the 12 articles described corrective surgery of which there were 231 operations ranging from amputation to correction of malunion and soft tissue intervention. Three articles stated the length of treatment by TBS and this ranged from 3 days to 46.24 weeks prior to treatment by orthodox methods, but the length of stay in orthodox hospitals following TBS treatment was not explicitly stated.
Some comparisons between management by TBS and Orthodox services was made in two articles; one noted a 14% complication rate with orthodox services over their study period. The other paper reviewed cost differences in treating complications, those from TBS costing $18–$380 whilst those from orthodox services costing $34–$98.
Discussion
The database search showed the topic is well researched and reviewed, revealing most articles were set in Africa and Asia where there is a rich historical background of TBS.
Several articles demonstrate the economic and educational background of those seeking treatment from TBS in an attempt to explain the high level of patronage towards TBS within many LMICs.11,14,15,17,18 The main reasons for utilisation of TBS included cheap fees, cultural beliefs, quick service, easy accessibility and pressure from family and friends. 22 Amongst the reasons given not to seek orthodox treatment included a fear of amputation, apathetic attitude of health workers and delays in care at hospitals due to bureaucracy. The study demonstrated that those seeking treatment by TBS came from a spectrum of society and a wide range of educational backgrounds and professions. It was noted that those in a rural community sought the help of TBS more than those from an urban conurbation.11,14
Nine of the articles described methods used by TBS to treat musculoskeletal injury, which included the use of bamboo stick splinting and bandaging as well as herb application and massage to the injured site.5,12,15–21 The use of incantations during the TBS process is also described in the literature and is attributed to the belief that healing power arises from their ancestors and God. 23
The complications due to treatment by TBS have a huge health and socioeconomic impact on LMICs as they predominantly involve children or young adults of reproductive age (the average age was 23.1 years). Orthodox care was often sought following failed treatment by TBS indicating that the complications may also pose a management challenge to orthoodox care providers and a further burden on the health system.
Eleven articles called for strategies to help prevent and alleviate these complications that arise.5,11–14,16–21 Discouraging the use of TBS, suggested by one, has been found difficult to achieve their goal owing to high levels of TBS patronage.22,23 Educating TBS, by providing training to recognise their limitations and link with the orthox health care system was another strategy. Another 23 sought to explore the knowledge and practice among TBS and to assess the opportunities for engagement with the formal health sector. It was noted that whilst most TBS felt that the care that they provided had advantages over orthodox care, all agreed that the latter also has some advantages over TBS care. Moreover most TBS expressed an interest in such an engagement, especially with exchange of referral contacts, regular meetings and training courses.
The approach to educating TBS has been shown to be successful in various countries globally. A one day course in Ethiopia on safe fracture care resulted in a decrease in TBS-induced amputations from 49 in the two years prior to the course, to 25 in the two years following the course. 24 Similar improvements in Nigeria where a TBS centre was provided a one day course showed a statistically significant difference between the rate of gangrenous limbs, infection, non-union and mal-union in tibial shaft fractures. 25 In Turkey, traditional practitioners have been trained to refer difficult cases to orthodox health care providers. 26 In Nepal, training programmes for rural village health workers increased knowledge base and working skills and continued for six years after the training. 27
Recommendations for TBS to be regulated, certified and licensed prior to providing care to the general population5,13 have also been made with varying success.
Some limitations to our review exist in that it was limited to an established scientific database and by hand search of the reference lists. The conclusions drawn in the present paper may not be generalisable. A noted limitation of our review is the heterogeneity of the studies included, and the limitation to publications in English which may suggest cultural bias.
The prevalence rate of complications from TBS care is difficult to ascertain as the number of people seen by TBS is quite unknown.
Conclusion
TBS provides a service to a vast population of varying education backgrounds and professions and will continue to do so due to large patronage within LMICs. This review identifies that there are a significant number of limb and life threatening complications as well as high mortality associated with the treatment by TBS.
However, recent studies have shown that TBS are willing and keen to engage with local orthodox services and training courses. As shown in many countries, this can lead to a reduction in complications and mortality and can form a set up where TBS and Orthodox services can work side by side.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article