
Abstract
While adoption of the Ponseti method has continued gradually, its use to manage patients with congenital talipes equinovarus (CTEV) has been limited in low- and middle-income countries (LMICs) for a number of reasons including a lack of clinical training on technique and lack of appropriate clinical equipment. There are a frequent number of emerging studies that report on the role of clubfoot training programmes; however, little is known in regard to cumulative benefits.
A systematic review was undertaken through Medline, the Cochrane Library and Web of Science for studies analysing clubfoot training programmes. There were no limitations on time, up until the review was commenced on January 2020. The systematic review was registered with PROSPERO as 165657. Ten articles complied with the inclusion criteria and were deemed fit for analysis. Training programmes lasted an average of 2–3 days. There was a reported increase in knowledge of applying the Ponseti method in managing clubfoot by participants (four studies P < 0.05). Skill retention was examined by multiple choice (MCQ) examination style questions before and after the training programme in two studies; both showed an improvement (MCQ answers improved from 59% to 73%). All studies showed an improvement in participants' self-reported understanding of the Ponseti method and confidence in its use in future practice (P < 0.05). There were improved benefits of knowledge and clinical application of the Ponseti method by participants in the programmes in all studies examined. However, there was a significant lack of follow-up and exploration of long-term effects of these programmes. Implementing training programmes based on perceived benefits rather than actual long-term benefits may have a negative impact on healthcare delivery and patient management in LMICs.
Keywords
Introduction
Congenital talipes equinovarus (CTEV) is one of the most prevalent congenital deformities, estimated to occur in 0.6–1.5 per 1000 live births, with 80% born in low- and middle-income countries (LMICs). 1 It is defined as fixation of the foot in adduction, varus and in supination, rotated outwards and downwards. 2
The advent of the Ponseti method to manage CTEV has dramatically improved patient outcomes when compared to the invasive surgical approach.3–7 The method consists of two key elements: first, correction of the deformity by manipulation and serial casting; and second, the use of abduction braces to maintain achieved correction.8,9 While adoption has continued gradually, the use of the Ponseti method to manage patients with CTEV has been limited in LMICs for a number of reasons: a lack of clinical training on the technique and a lack of appropriate clinical equipment. 10 Reasons for this may include limited training in the Ponseti method, limited personnel and competing priorities, particularly in sub-Saharan Africa.10,11 Further, the major challenge for the availability of surgical services for children in LMICs worldwide is low-skilled workforce and infrastructure.12–14 A recent Zambian study, using the World Health Organization (WHO) SAT tool, also demonstrated that lack of surgical skill and relevant equipment was the leading factor in limiting availability of 93% of paediatric procedures. 15
Training programmes and short-term courses appear beneficial in terms of addressing the issue of lack of clinical skills. 16 These typically consist of ‘hands-on workshops’ and theoretical lectures on the Ponseti method that span over 1–7 days.
Given the expenditure and burden of running potentially expensive courses in LMICs which might have otherwise prioritised their available funds/time, training programmes have an ethical responsibility to clarify benefit against costs. As such, the importance of an evidence-based approach is vital to consider. Costs of running the programmes and long-term retention/application of skills are factors that should be monitored closely with such programmes.
The aim of the present article is to systematically review the literature to determine the role and long-term effectiveness of clubfoot training programmes in LMICs and categorise these reported benefits. In the event that statistical reported benefits differ, we shall use a narrative analysis to identify common themes and discuss in depth the reported benefits and significance of them.
Methods
A systematic review was undertaken through Medline, the Cochrane Library and Web of Science. There were no limitations on time, up until the review was commenced in January 2020. The systematic review was registered with PROSPERO as 165657.
A literature search was conducted electronically with no time constraints using ‘(“Congenital equinovarus” or “CTEV” or “Clubfoot”)’ AND ‘(Programme)’, including MeSH terms (training programmes, teaching) with no language restrictions. Included were the introduction of training programmes specific to management of clubfoot in LMICs; excluded were training programmes not related to clubfoot and where no clear description of training programme implemented was given.
Following the recommended PRISMA guidance, three authors (SS, SN and EK) examined the selected studies against an inclusion criterion (Figure 1). Inclusions were specific to clubfoot or congenital equinovarus management training programmes. We did not exclude articles based on chosen technique (e.g. Ponseti or other manipulative methods). A secondary search was undertaken, which involved screening references from selected texts for further studies. Duplicates were removed and any disputes noted between the two authors on eligibility of studies were discussed with the third author.
PRISMA flow diagram.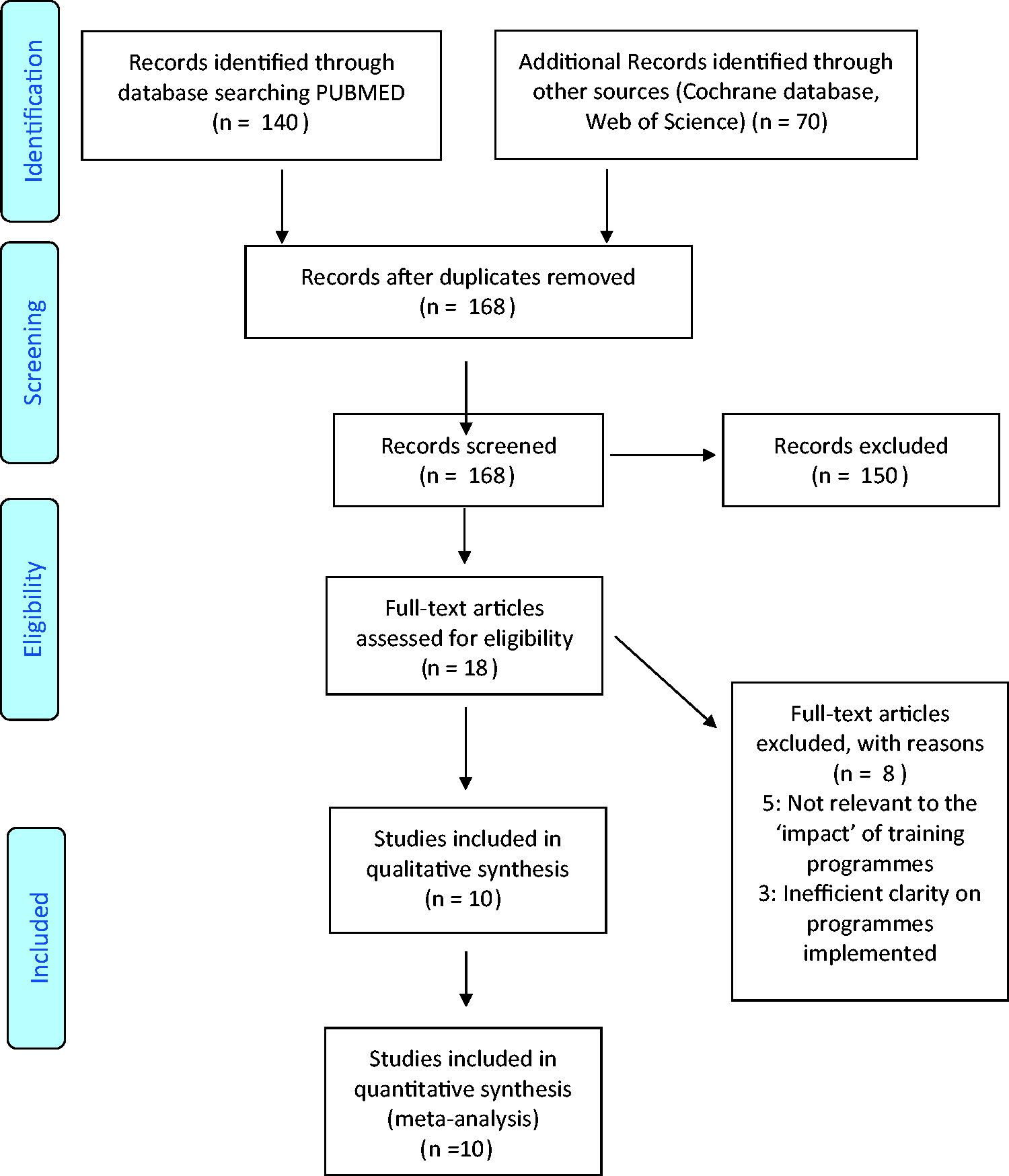
Key data including author names, date of publication, study design, location, number of participants, duration of follow-up and results were extracted and formulated. We included a quality analysis for quantitative studies for further evaluation, including risk of bias assessment.
Where possible, a data analytical analysis was performed for improvement in skills, confidence after training and retention of skills gained. If different statistical methods were used, a narrative analysis on common themes was opted for.
The Cochrane tool for assessing risk of bias was used to assess the quality of included studies, adapted from Higgins and Altman. 17
Results
Ten articles complied with the inclusion criteria and were deemed fit for analysis. All papers reviewed were published in 2007–2018.
There was a reported increase in the knowledge of the Ponseti method in managing clubfoot in participants in all studies. Two studies opted for multiple choice (MCQ) examination style questions before and after the training programme; both showed an improvement (MCQ answers improved from 59% to 73%). All other studies opted for the use of questionnaires that were given after the training programmes were completed (range = 1–5 days), focusing on confidence and perceived improvement in understanding of the Ponseti method after the training session. All studies showed an improvement in participants' self-reported understanding of the Ponseti method and confidence in its use in future practice (P < 0.05).
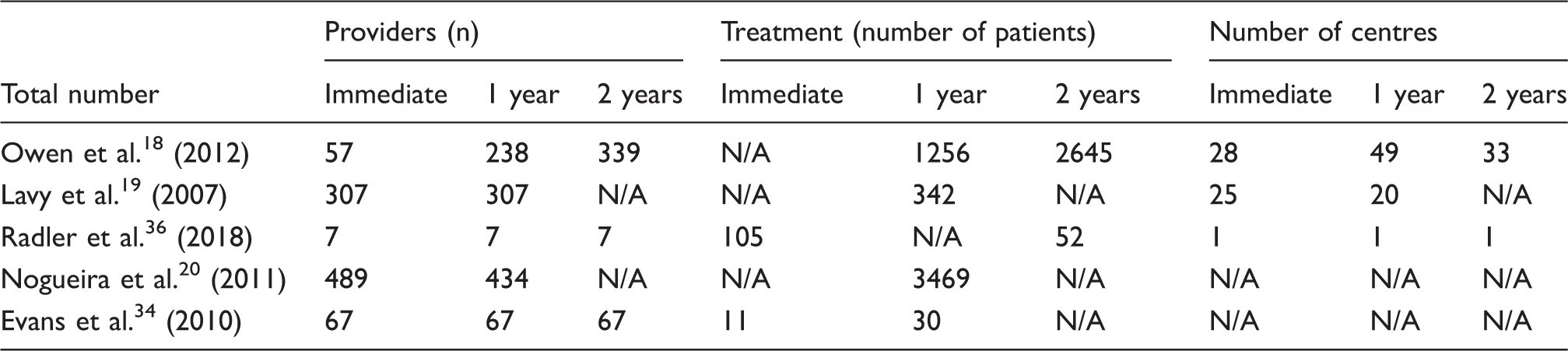
Reported results of number of trained providers, patients treated and treatment centres established resulted from providers completing CTEV training courses.
Nogueira et al. 20 showed the most significance in knowledge gained by participants after the training programme/symposium, going from 17% to 88% self-reporting that they were able to treat children with the Ponseti technique (P < 0.05). Of them, 94% attributed this to the training programme.
Training programmes lasted an average of 2–3 days in the studies examined. The content of the training programmes varied between hands-on casting, lectures/workshops and directly observing qualified Ponseti clinicians manage patients.
To analyse gained benefits, the majority of studies utilised questionnaires before and after the programme. The rate of completion for the questionnaires was in the range of 50%–70%. The duration for completion was in the range of 1–5 days after the programme. Few studies examined the benefits of programmes in relation to skill retention after seven days.
The majority of participants in the programmes were orthopaedic surgeons, physiotherapists and nurse practitioners. No study examined the differences between skills retained and practised between non-physicians and physicians.
There were no randomised control trials/comparative studies found.
Quality analysis
Most studies reviewed were observational. Overall, the majority of studies were reported as fair, with lack of reporting on withdrawals/drop-outs reducing a large proportion of the quality of the studies. Further, only few studies reported yearly assessments. Most studies scored 2–3 for methods of data collection, reflecting on the frequent use of self-reported questionnaires and rarely any objective assessment of retained skill.
Discussion
Description of the studies included in the present review.
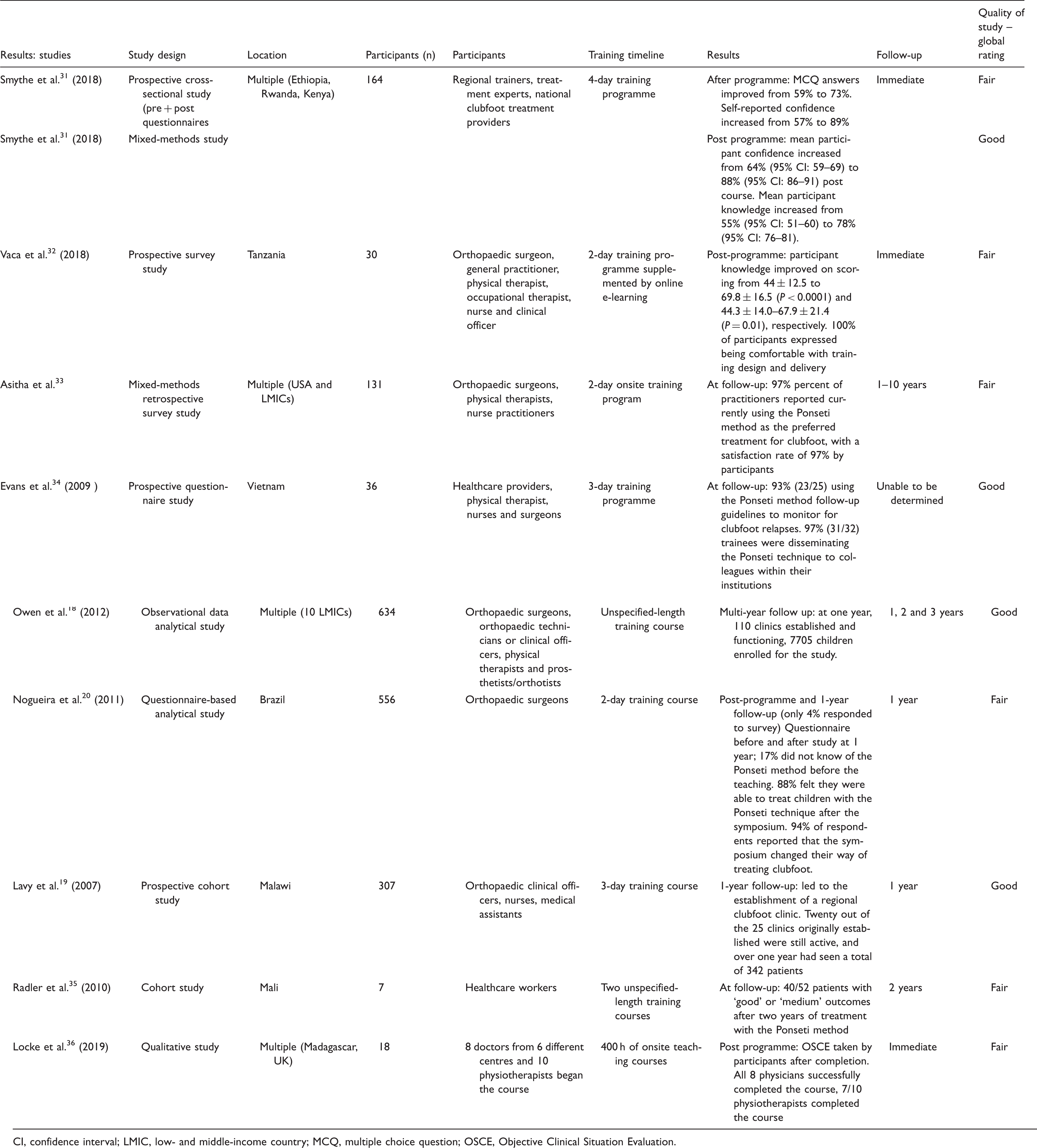
CI, confidence interval; LMIC, low- and middle-income country; MCQ, multiple choice question; OSCE, Objective Clinical Situation Evaluation.
Cochrane's tool for assessing risk of bias (adapted from Higgins and Altman 18 ).
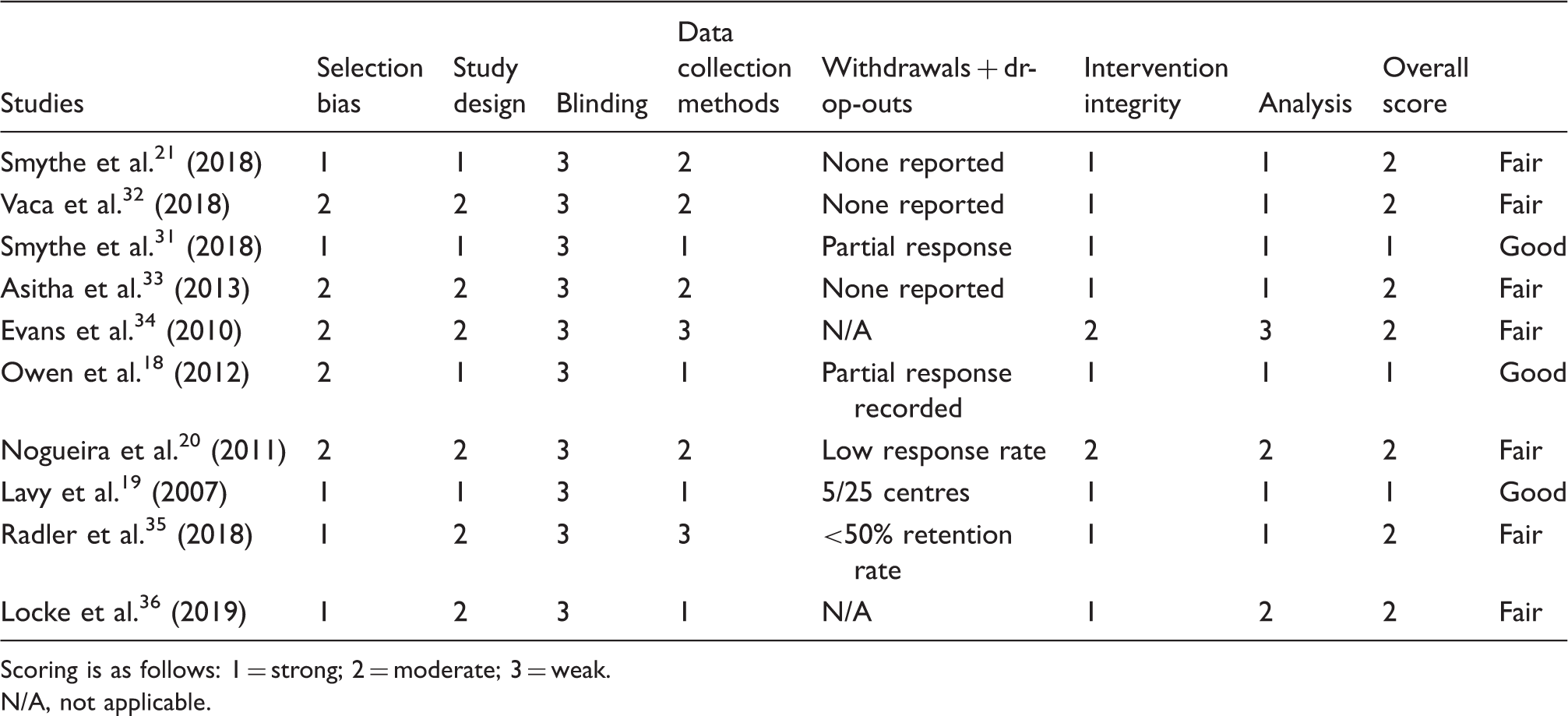
Scoring is as follows: 1 = strong; 2 = moderate; 3 = weak.
N/A, not applicable.
Given the prevalence of CTEV, particularly in LMICs, 1 non-invasive methods of managing the condition are a significant cost-efficient technique in comparison to invasive intervention. Thus, short training programmes to teach LMIC participants the Ponseti method as well as other non-invasive methods to implement in their own practice are well warranted.
Furthermore, on quantifying the economic burden of clubfoot in LMICs, we note a reported average of 7.42 disability-adjusted life years (DALY) averted with a cost-effectiveness ratio of US $22.46 per DALY averted in sub-Saharan African countries as a result of contribution to society due to CTEV. 22 Other studies have reported similar findings. 23 Considering the low costs of training programmes in relation to DALY, it would make financial sense for LMICs to continue invest in training methods of non-invasive techniques for its healthcare delivery personnel.
However, training programmes reported in the literature do not provide a reliable measure of long-term impact given the short duration of follow-up. Previous studies have alluded to loss of knowledge gained unless continually used or reassessed in a given capacity. 24 The authors' suspicions are that although training programmes may be beneficial in the short term, it would be wise to reassess gained skills to cement the notion that clubfoot training programmes benefit LMICs, as well as ensure the correct level of quality of care provided by the trained participants.
Reasons for the lack of follow-up may include the relatively new introduction of CTEV programmes in LMICs, difficulties in following up a programme due to change of personnel/loss of contact, and lack of sufficient programme funding to allow further studies to evaluate outcomes.10,25 Programmes that did record follow-ups demonstrated some coherent structure to evaluate the benefits of implemented programmes over a recorded timescale (Table 3).
Follow-up on implementation of learnt skills would require well-recorded analytical data on patients seen and treated by personnel who attended the training programmes. These data would need to be collected objectively. There is a general lack of quality-assured hospital data and audit in hospitals in LMICs that have been previously explored in prior studies. This could suggest one of a number of possible reasons behind the lack of follow-up. 26
Relapse rates of CTEV have been associated with lack of parental guardians' knowledge on Ponseti casting and the importance of follow-up clinics. 27 It is therefore of some surprise that not all training programmes in the literature fostered the importance of parental education as a skill to their trainees. Inclusion of educative methods for families provided by clinicians should be intertwined in training programmes. 27
Content of training programmes varied, mainly in the personnel taught, ranging from physiotherapists and doctors to non-physician clinical officers. The majority of the programmes included lecture-based study with practical elements. Arguments have been made for a uniformed, established, reproducible training curriculum for manipulative methods on managing clubfoot in LMICs. 21 A good example is the Africa Clubfoot Training Project, part of the Global Clubfoot Initiative, a project that reinforced a standardised curriculum of clubfoot training in Ethiopia and aligned with local priorities through joint planning and coordination. However, data on follow-up and the impact of said training are yet to be made available.
A well-managed training programme must take into consideration the materials that are sourced in LMICs, the number of cases of clubfoot seen by each practitioner, and follow-up on the effectiveness of the programme to monitor the following:
Are skills still being practised and retained? Knowledge still present. Clinics still functioning. Issues identified as a result of the training and managed appropriately (audit and quality improvement).
The importance of the evidence base for medical/surgical training has been well explored.28,29 Implementing training programmes based on perceived benefits rather than actual benefits may have a negative impact on healthcare delivery and management of patients in LMICs. It is thus incredibly important that alongside clear rationale, which the majority of CTEV training programme studies provide, there must be a structured, robust follow-up scheme in place to employ good sustainability of reported benefits. Neglecting the long-term effects of training programmes can cause under-reporting of complications and overestimation of perceived benefits. 30 Further, important factors that must be objectively explored include the level of skill retention over a longer duration and continuous assessment of participants current/future practice. The bias in self-reported questionnaires may not report the full extent of the impact of training. Rather, we suggest objective assessments such as MCQs or Objective Clinical Situation Evaluations (OSCEs) as a formal assessment of retained skills. These should ideally take place over a yearly time span.
Conclusion
The present study highlights the effects of CTEV training programmes in LMICs. There are improved benefits of knowledge and application in all studies examined. However, there is a significant lack of follow-up and long-term effects of said programmes. As a result, it is difficult to ascertain the long-term benefits of implementing these programmes. The authors agree that this can be ameliorated with objective follow-up measures in place to examine application of knowledge and skill. Given the number of studies that highlight reasons for relapse of CTEV, training programmes would do well to address highlighted reasons such as lack of parental understanding of the condition, as well as foster long-term collaboration and partnership between institutions to ensure long-term follow-up from training programmes. Future studies should focus on the long-term effects of CTEV training programmes on the impact on practice in LMICs.
Strengths and limitations
This is the first systematic review in the literature assessing the impact of CTEV training programmes in LMICs. A robust analysis of the literature revealed a significant lack of important follow-up data on CTEV training programmes.
The limitations of this study include the small sample size and lack of current CTEV training programme studies. This could be due to the recent implementation of such programmes in LMICs.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CL leads the Africa Clubfoot Training (ACT) project which focuses on strengthening and expanding clubfoot training in sub-Saharan Africa.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article.