
Abstract
Amid rapid population aging and the rising prevalence of chronic diseases, healthcare-related financial stress has become a critical risk factor undermining residents’ subjective well-being. Using micro panel data from the China Family Panel Studies (CFPS) for 2018 to 2022, this study examines the impact of healthcare financial stress on subjective well-being and its underlying mechanisms. Two-way fixed-effects models are employed, controlling for individual and time fixed effects and a wide set of demographic and household characteristics. We estimate the association between healthcare financial stress and happiness scores and use mediation analysis to assess the roles of self-rated health status and freely disposable household income in transmitting this effect. The results indicate that, after controlling for individual and time fixed effects as well as a range of demographic and household characteristics, healthcare financial stress is significantly negatively associated with subjective well-being. Mediation analysis shows that healthcare financial stress worsens self-rated health and compresses disposable income, thereby amplifying its adverse effect on well-being. Heterogeneity analysis further reveals that low-income groups, rural residents, and individuals with limited social security coverage bear a disproportionately larger negative impact, suggesting that healthcare financial stress constitutes an important constraint on advancing common prosperity. Accordingly, this study recommends advancing a “quasi-free” reform of basic healthcare, accompanied by optimizing the financing and expenditure structure and strengthening health insurance payment and oversight, to alleviate healthcare financial stress, enhance well-being, and improve the healthcare security system.
Keywords
Introduction
Subjective well-being (SWB) refers to individuals’ overall subjective evaluation of their quality of life, encompassing affective experiences and life satisfaction. It has become an important complementary indicator for assessing the quality of social development and the performance of public governance. 1 In China, with the establishment of the people-centered development philosophy, enhancing residents’ sense of gain, happiness, and security has been placed in a more prominent position. 2 However, the World Happiness Report (2022) shows that, among 146 countries and regions, China ranks only 72nd in overall happiness, and its happiness level has not improved substantially compared with the 1990s, 1 thereby revealing a paradoxical decoupling between economic growth and subjective well-being. The “Easterlin paradox” proposed by Easterlin (1974) points out that income growth does not translate linearly into higher happiness in the long run, 3 which has stimulated extensive academic debate on the roles of income effects, living costs, social comparison, and public service provision.
Among the various explanatory pathways, healthcare expenditures and the associated healthcare financial stress have attracted growing attention. Existing studies indicate that in many countries, healthcare expenditure has been rising persistently faster than economic growth, and in some cases spending on health insurance already accounts for more than 20% of total health expenditure. 4 Rising medical expenditure not only crowds out other categories of household consumption, but also, by heightening financial insecurity and health-related anxiety, reshapes residents’ expectations and affects macroeconomic dynamics.5,6 In China, population aging and the high prevalence of chronic diseases, compounded by the impact of the COVID-19 pandemic, have jointly placed mounting demand pressure on the healthcare system. According to the 2022 Statistical Bulletin on the Development of China’s Health Undertakings, national health expenditure reached 84 846.7 billion yuan, accounting for 7.0% of GDP, with per capita health expenditure of 6010 yuan; the average outpatient expenditure per hospital visit increased by 4.1% year-on-year. 7 At the same time, pronounced regional inequalities and urban–rural gaps in the distribution of medical resources mean that the problems of “difficult access to care” and “expensive medical treatment” remain persistent. 8 Empirical analyses based on CGSS, CFPS and other micro-surveys show that the share of health expenditure in total household consumption continues to rise, and the risks of “falling into poverty due to illness” and “returning to poverty because of illness” have become significantly more severe among low- and middle-income groups. 9 The resulting healthcare financial burden—that is, the healthcare-related financial stress and the associated perceived financial stress arising from medical expenditures—has thus become an important factor eroding family well-being and residents’ subjective happiness.
Stress process theory posits that chronic stressors—such as economic constraints—can affect individual well-being through sustained psychological burden and the depletion of resources. 10 In the healthcare context, healthcare financial stress, as a typical form of financial strain, may reshape household resource allocation and thereby influence residents’ subjective well-being. Healthcare financial stress may affect subjective well-being mainly through 2 pathways: Health status and household disposable income. First, the health status mechanism. As healthcare financial stress increases, households face stronger payment constraints and cost-related barriers, making them more likely to delay or forgo the use of healthcare services and necessary care, which is detrimental to health outcomes. 11 Meanwhile, consistent with established literature, catastrophic health expenditure is defined as household out-of-pocket health payments exceeding 40% of the household’s non-food expenditure (which represents the household’s capacity to pay after covering basic subsistence needs), 12 and such expenditure has been shown to be associated with adverse mental health outcomes such as a higher risk of depression. 13 Since health status is a fundamental basis of subjective well-being, poorer health is typically linked to lower subjective well-being. 14 Second, the household disposable income mechanism. Rising healthcare financial stress implies that medical spending imposes a heavier squeeze on the household budget, potentially reducing household disposable resources and generating a “crowding-out effect” on other consumption, thereby lowering quality of life and life evaluations. Related studies provide evidence that out-of-pocket medical spending crowds out non-medical consumption 15 and show that changes in medical expenditures can significantly alter household consumption structure. 16 Moreover, a contraction in household disposable income weakens households’ capacity for consumption and risk coping, thus reducing individuals’ subjective well-being. 17 The above mechanisms are illustrated in Figure 1. Based on this analysis, we propose the following hypotheses:

Graphical representation of conceptual framework.
Literature Review
Connotation and Structural Drivers of Healthcare Financial Stress
The Chinese literature often conceptualizes “medical stress” as a multidimensional condition shaped by economic, psychological, and institutional forces. In this study, we define healthcare financial stress as the compounded burdens individuals or households face when confronting disease risks, medical expenditures, and the care-seeking process. 18 Beyond the narrower notion of “expensive medical treatment,” it captures not only a rising medical share in the household budget but also perceived anxiety, helplessness, and insecurity induced by information asymmetry, therapeutic uncertainty, and institutional complexity. 19 From a sociological perspective, healthcare financial stress is produced through interactions among individuals, families, healthcare providers, and wider social structures, implying that mitigation requires coordinated improvements in institutional fairness, resource allocation, and public trust. Consistent with an institutional-choice view, systems lacking universal free or quasi-free basic coverage leave residents insufficiently protected against health shocks, thereby generating a structural form of healthcare burden. 20 Accordingly, we treat healthcare financial stress as both healthcare-related objective financial strain and the associated perceived financial stress arising from medical spending. For the objective financial strain dimension in this study, we use the internationally recognized 40% threshold of catastrophic health expenditure as the core classification standard, which ensures the objectivity and comparability of our core explanatory variable setting.
In China, escalating healthcare financial stress reflects several structural conditions. First, deteriorating population health and widening health inequalities heighten vulnerability to disease risks. As a core component of human capital, health capital affects individuals’ capacity for labor and non-labor activities. 21 Rising health inequality implies that health-disadvantaged groups face larger income losses and weaker long-run wealth accumulation when shocks occur. 22 Inequality is also experienced subjectively via relative deprivation and the “tunnel effect,” whereby comparisons with advantaged groups intensify negative emotions and amplify perceived healthcare financial stress. 23 Second, cost pressures have been reinforced by marketization and institutional incentives, including legacy reliance on drug mark-ups and diagnostics that encouraged overtreatment and unnecessary examinations. 24 Despite reforms, insurance design—reimbursement rates, deductibles, and ceilings—still leaves sizable out-of-pocket spending for major and chronic conditions, pushing disadvantaged households into a “high bills–depleted savings–borrowing” trajectory.25,26 Third, population aging increases chronic disease and long-term care needs, 27 while spatially uneven medical resources raise travel, time, and opportunity costs for grassroots residents.28,29 Taken together, existing evidence suggests that healthcare financial stress is jointly shaped by health inequality, rising costs, institutional arrangements, and demographic change. 30
Prior Research on Residents’ Subjective Well-Being and Healthcare-Related Financial Stress
The idea of happiness originates in classical Greek reflections on the “good life,” but contemporary research on subjective well-being (SWB) has mainly evolved within 20th-century psychology and sociology. Psychology emphasizes affective well-being (emotional experiences), whereas sociology focuses more on cognitive well-being, such as life satisfaction and self-evaluation. The emergence of happiness economics—especially after the Easterlin paradox—made the complex, non-linear relationship between income and happiness a core concern. 3 Subsequent interdisciplinary, quantitative research has mapped diverse determinants of SWB and generated evidence relevant to public policy optimization. 31
At the micro level, SWB is consistently linked to socio-demographic traits and household conditions, notably gender, age, marital status, health, and income. For example, unequal division of household labor imposes a disproportionate burden of unpaid work on women and significantly depresses their happiness. 32 Health is similarly central: longitudinal evidence shows that better physical health predicts higher happiness, whereas chronic illness and long-term pain lower SWB. 33 Income effects are also robust; both absolute and relative income positively shape happiness, with relative income accounting for an important share of SWB differences. 34
At the macro level, research incorporates income inequality, perceived social fairness, employment and social security, political trust, environmental quality, and government size. Easterlin (1974) argues that higher-income individuals report greater happiness at a given time, yet long-run national economic growth does not necessarily raise average happiness proportionally. 3 Evidence from Chinese social surveys likewise suggests that economic, social, and political factors jointly shape SWB, with absolute and relative income remaining key channels. 35 Labor-market status matters strongly: unemployment substantially reduces SWB, while re-employment partially repairs the loss (Clark, 2003). Social support further bridges macro–micro mechanisms; individuals embedded in strong support networks report significantly higher happiness. 36
As health expenditure occupies a growing share of household budgets, healthcare financial stress has become an emerging lens in SWB research. However, relatively few studies systematically incorporate healthcare-related financial stress and the perceived financial stress arising from medical spending into standard SWB frameworks, and dynamic panel evidence remains particularly scarce. Existing work on healthcare-related factors and SWB broadly follows 3 strands: (i) health economics emphasizes health as a mediator linking healthcare utilization to SWB 37 ; (ii) studies on access and care-seeking experiences highlight how resource shortages, access barriers, information asymmetry, and poor service can trigger anxiety and institutional distrust, undermining life satisfaction; and (iii) research on catastrophic health expenditure shows that medical spending raises poverty risk and lowers SWB by crowding out other consumption and reinforcing economic insecurity. 38 Policy responses—including expanded insurance, catastrophic coverage, medical assistance, chronic disease management, and health-promotion programs—aim to reduce burdens and improve SWB.39 -42
Three gaps remain: conceptually, many studies equate healthcare financial stress with single objective indicators; methodologically, cross-sectional designs dominate; and contextually, nationally representative panel research jointly linking healthcare financial stress and SWB in China is limited. Related domestic work has begun to model broader household strain; for example, housing stress increases medical spending via income and health status using CFPS 2016-2020, 30 but it still treats expenditure as the outcome rather than comprehensive healthcare financial burden including perceived stress.
Compared with the above studies, this paper makes 3 main marginal contributions. First, at the conceptual level, it reconceptualizes healthcare financial stress from a “comprehensive stress” perspective, linking healthcare-related economic burdens with risk expectations, health status and institutional protection, and operationalizes this construct using indicators that capture households’ relative healthcare burden. This approach partly overcomes the predominant reliance on single expenditure-based measures in previous research. Second, at the methodological level, the paper employs CFPS micro panel data for 2018 to 2022 to construct a mediation model that incorporates health status and discretionary household income, thereby systematically testing the transmission chain from healthcare financial stress to income/health and, in turn, to subjective well-being, and enhancing the identification of causal pathways and dynamic effects. Third, at the contextual level, the analysis is embedded in China’s urban–rural structure and social protection system, with particular attention to heterogeneous effects across income groups, between urban and rural residents, and among groups with different levels of social security coverage. In doing so, the study provides more contextually grounded empirical evidence on the mechanisms linking healthcare financial stress and subjective well-being under China’s medical security arrangements.
Methods
Data Source
This study is an empirical study based on nationally representative longitudinal survey data from China. We use micro-level data from the China Family Panel Studies (CFPS), a nationwide panel survey implemented by the Institute of Social Science Survey (ISSS), Peking University since 2010 and covering 31provinces (municipalities/autonomous regions) in China. The CFPS adopts a community–household–individual design and tracks Chinese residents’ socio-economic conditions, health status, and subjective well-being over time. The CFPS questionnaire covers multiple dimensions, including household income and expenditure structure, health status and medical costs, housing ownership and housing expenditure, marital and educational background, as well as labor and employment conditions. 43 These rich micro-level data provide a high-quality empirical foundation for examining the impact of healthcare financial stress on residents’ subjective well-being.
Given the research focus and data availability, this study uses the 2018, 2020 and 2022 waves of the CFPS as the analytical sample and constructs a panel dataset of Chinese residents for the period 2018 to 2022. The data processing follows standard procedures for data cleaning. First, observations with missing information on core variables—namely healthcare financial stress, subjective well-being and key control variables—are removed. Second, observations with clearly implausible values or internally inconsistent responses on critical variables are excluded. Third, only those cases for which household and individual information can be consistently matched and identification codes are aligned across waves are retained, so as to enhance the reliability and robustness of the estimation results. After these steps, the final sample consists of 30 900 households. The sample selection process and the distribution of the final sample size are illustrated in Figure 2.

Flowchart of data processing and analysis.
Description of Variables
Dependent Variable
This study uses residents’ subjective well-being (SWB) as the dependent variable. Compared with objective indicators of welfare, subjective well-being provides a more comprehensive assessment of individuals’ overall evaluation of their life circumstances, as it encompasses both cognitive judgments about living conditions and affective states and emotional experiences. 44 Such self-reported evaluations capture psychological and emotional dimensions that are difficult to observe with conventional objective metrics and, being unconstrained by predetermined objective indicator dimensions, more closely reflect individuals’ genuine sense of well-being.
Accordingly, this study measures subjective well-being (SWB) using the core happiness question in the China Family Panel Studies (CFPS) questionnaire: “How happy do you feel?” Respondents are asked to rate their happiness on an integer scale from 0 to 10, with higher values indicating higher levels of subjective well-being. This score is directly used as the quantitative indicator of residents’ subjective well-being and is denoted as the variable Happy in the empirical analysis.
Explanatory Variable
We measure healthcare financial stress using a catastrophic-spending–based threshold approach. Specifically, we first compute the ratio of a household’s out-of-pocket medical expenditure to its non-food expenditure, where non-food expenditure proxies the household’s resources available after meeting basic subsistence needs. Following the canonical definition proposed by Xu et al, 12 which identifies catastrophic health spending when health payments exceed 40% of the household’s capacity to pay, we classify households with a ratio ≥0.40 as experiencing high healthcare financial stress (coded as 1), and those with a ratio <0.40 as low stress (coded as 0).
Mediating Variables
This study introduces 2 mediating variables—health status and household disposable income—into the empirical model in order to identify the indirect effects through which healthcare financial burden influences residents’ subjective well-being via a “health channel” and an “economic channel.” The selection and specification of these mediators are informed, to a considerable extent, by the analytical framework proposed by Liu et al. 30
Health Status
Health status captures both individuals’ physical and psychological conditions and constitutes a key mediating link between healthcare financial stress and subjective well-being. This study measures health status using the self-rated health indicator in the CFPS. Higher values of this indicator correspond to better self-assessed health.
Household Disposable Income
Household disposable income, as defined in this study, reflects the remaining income that a household can allocate at its own discretion after covering basic living and necessary expenditures. It is used to capture the extent of household economic slack and the realized standard of living. Based on the CFPS variable documentation, this indicator is constructed by deducting expenditures on food, clothing and footwear, daily necessities and household equipment, housing, culture and education, healthcare, and transportation and communication from household net income. Formally:

Where
Control Variables
To mitigate potential omitted variable bias in the empirical model, this study includes a set of sociodemographic and socioeconomic characteristics as control variables. These variables comprise age, gender, educational attainment, marital status, employment status, and the dependency ratio. Their definitions and coding schemes are reported in Table 1.
Descriptive Statistics of the Variables.
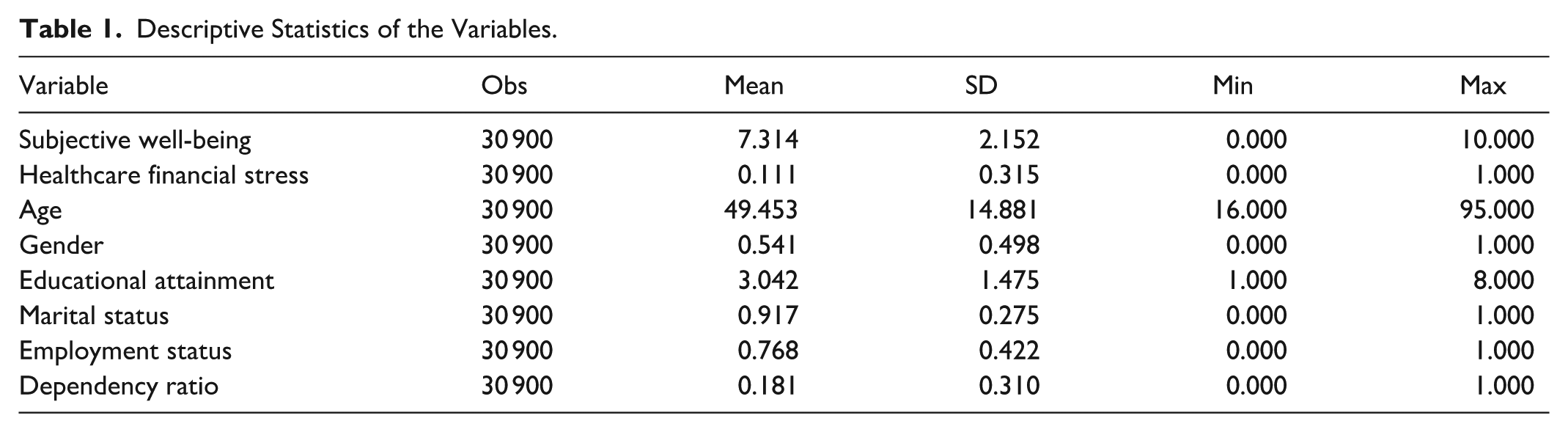
Specifically, age is treated as a continuous variable based on the actual age of the household head. Gender is coded as a dummy variable, taking the value 1 for males and 0 for females. Marital status is also specified as a dummy variable, where currently married respondents are coded as 1, and all other marital states—including never married, divorced, and widowed—are coded as 0. Educational attainment is measured by years of schooling, converted from the CFPS education categories, with higher values indicating higher levels of education. Employment status is defined as a dummy variable that equals 1 if the respondent is currently employed (including both wage employment and self-employment) and 0 if the respondent is unemployed or not in employment.
At the household level, dependency ratio is defined as the share of non–working-age household members in total household size and is used to capture the intensity of household caregiving and support obligations. All of the above control variables are included in the regression models alongside the core explanatory variable and the dependent variable. Their detailed definitions, coding rules, and descriptive statistics are summarized in Table 1.
Model Specification
To identify the impact of healthcare financial stress on residents’ subjective well-being, this study first estimates a 2-way fixed effects panel model. This specification simultaneously controls for unobserved time-invariant individual characteristics and time-specific macro shocks, thereby mitigating, to some extent, endogeneity concerns arising from omitted variables. The baseline model is specified as follows:

In equation (1),
Building on this baseline specification, and in order to examine the indirect mechanisms through which healthcare financial stress affects subjective well-being via health status and household disposable income, this study further employs a panel mediation framework. Given the inherent limitations of the conventional 3-step procedure for testing mediation effects 46 , a more appropriate strategy is to directly estimate the impact of the core explanatory variable on the mediating variables. This study adopts the latter approach, specifying the following model:

where
Statistical Analysis
Using a household-panel dataset, we estimate the effect of healthcare financial burden on subjective well-being with a 2-way fixed-effects OLS model, including household and year fixed effects to account for time-invariant household heterogeneity and common time shocks. We also employ propensity score matching (PSM) as an endogeneity check to mitigate potential self-selection based on observable covariates. We report robust standard errors, and all analyses are performed in Stata Version 18.0.
The reporting of this study follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for cohort studies. 47 The completed STROBE checklist is provided as a Supplemental file to ensure the transparency and completeness of the study findings.
Results
Baseline Regressions
Using the 2-way fixed effects specification constructed in equations (1) and (2), Table 2 presents the baseline estimates of the effect of healthcare financial stress on residents’ subjective well-being. Model (1) includes only the core explanatory variable together with individual and year fixed effects. Building on this, Model (2) additionally incorporates a series of control variables, including age, educational attainment, marital status, employment status, household size, and the dependency ratio.
Fixed Effects Estimates of the Impact of Healthcare Financial Stress on Residents’ Subjective Well-Being.

Note. Robust standard errors in parentheses
P < .10. **P < .05. ***P < .01.
As shown in Table 2, the estimated coefficients on healthcare financial stress are both −0.133 in Models (1) and (2), and both are statistically significant at the 5% level. The signs and magnitudes of the coefficients remain highly consistent across specifications. This pattern indicates a stable negative association between healthcare financial stress and residents’ subjective well-being, regardless of whether rich demographic and household characteristics are controlled for.
In terms of economic significance, and holding other factors constant, a 1%-point increase in the relative level of healthcare financial stress is associated with an average decline of approximately 0.13 points in residents’ subjective well-being score on the 0 to 10 scale. While this magnitude is modest on a 10-point scale, it is statistically significant and non-negligible when considered against the overall variation in subjective well-being. This suggests that an increase in healthcare-related financial stress exerts a statistically and substantively significant dampening effect on individuals’ perceived well-being, thereby providing strong empirical support for Hypothesis 1.
Endogeneity Analysis
Although healthcare financial stress is largely shaped by external institutional arrangements and health shocks and thus reflects an objectively imposed burden, individuals’ exposure to, and perception of, such burden exhibits pronounced heterogeneity. Characteristics such as income level, educational attainment, and region of residence may simultaneously affect both the likelihood and intensity of incurring medical expenditures and individuals’ subjective well-being, thereby giving rise to sample self-selection and biased estimates.
To address this potential endogeneity concern, this study treats the occurrence of high healthcare financial stress as a quasi-natural experiment, constructs a treatment group (treated = 1) and a control group (treated = 0), and employs the Propensity Score Matching (PSM) method. Specifically, the analysis uses 3 matching algorithms—K-nearest neighbor matching with caliper, radius matching, and kernel matching—to estimate each individual’s propensity score of experiencing high healthcare financial stress, based on a set of covariates including age, gender, educational attainment, marital status, employment status, household size, and the dependency ratio.
When applying propensity score matching to correct for potential sample selection bias, it is first necessary to verify the presence of common support in the distribution of propensity scores between the treatment and control groups, so as to ensure the validity and credibility of the PSM estimates. In addition, balance tests are required to assess whether differences in covariates between the 2 groups are substantially reduced after matching.
Appendix Figure A1 plots the kernel density distributions of the propensity scores for the treatment and control groups before and after matching. As shown, the propensity scores of most observations fall within a common support region, and the 2 density curves become much more closely aligned following matching. The differences between the treatment and control groups are markedly attenuated, indicating a high quality of matching and suggesting that the common support assumption is largely satisfied.
Appendix Table A1 reports the results of the covariate balance tests. Relative to the pre-matching sample, the Pseudo R2 and LR chi-square statistics under all 3 matching algorithms decline substantially; the mean and median standardized biases (MeanBias and MedBias) are markedly reduced, and the standardized bias measure B is below 25% in all cases. These patterns indicate that PSM effectively attenuates systematic differences in covariates between the treated and control groups and largely controls for endogeneity arising from observable characteristics. Overall, the use of PSM can be regarded as consistent with the conditional independence assumption, and the resulting estimates are therefore reliable.
Building on the previous analysis, Table A2 reports the PSM-based estimates of the average treatment effect on the treated (ATT). Regardless of whether K-nearest neighbor matching with caliper, radius matching, or kernel matching is employed, the estimated average treatment effect of high healthcare financial stress on residents’ subjective well-being is significantly negative, and the magnitudes are highly similar across the 3 matching algorithms. Taking the kernel matching results as an illustration, after controlling for covariates and implementing sample matching, the mean happiness score of residents who do not experience high healthcare financial stress is approximately 7.470, whereas the average score for those exposed to high healthcare financial stress falls to 7.145, implying a decline of about 0.325 points. This difference is statistically significant at the 1% level.
Overall, the PSM estimates indicate that, even after fully accounting for observable characteristics, healthcare financial stress continues to exert a pronounced and robust suppressing effect on residents’ subjective well-being. From a theoretical standpoint, healthcare financial stress not only heightens the household’s economic strain, but may also intensify health-related anxiety, crowd out other forms of consumption, and disrupt intra-household relationships through multiple channels. These mechanisms jointly weaken individuals’ emotional states and life satisfaction over time, thereby lowering their overall level of subjective well-being.
Robustness Checks
To assess the robustness of the estimated impact of healthcare financial stress on residents’ subjective well-being, a series of sensitivity analyses are conducted by (i) replacing the dependent variable, (ii) excluding observations from municipalities directly under the central government, and (iii) changing the regression specification. The results are reported in Table 3.
Robustness Test of Healthcare Financial Stress and Residents’ Subjective Well-Being.
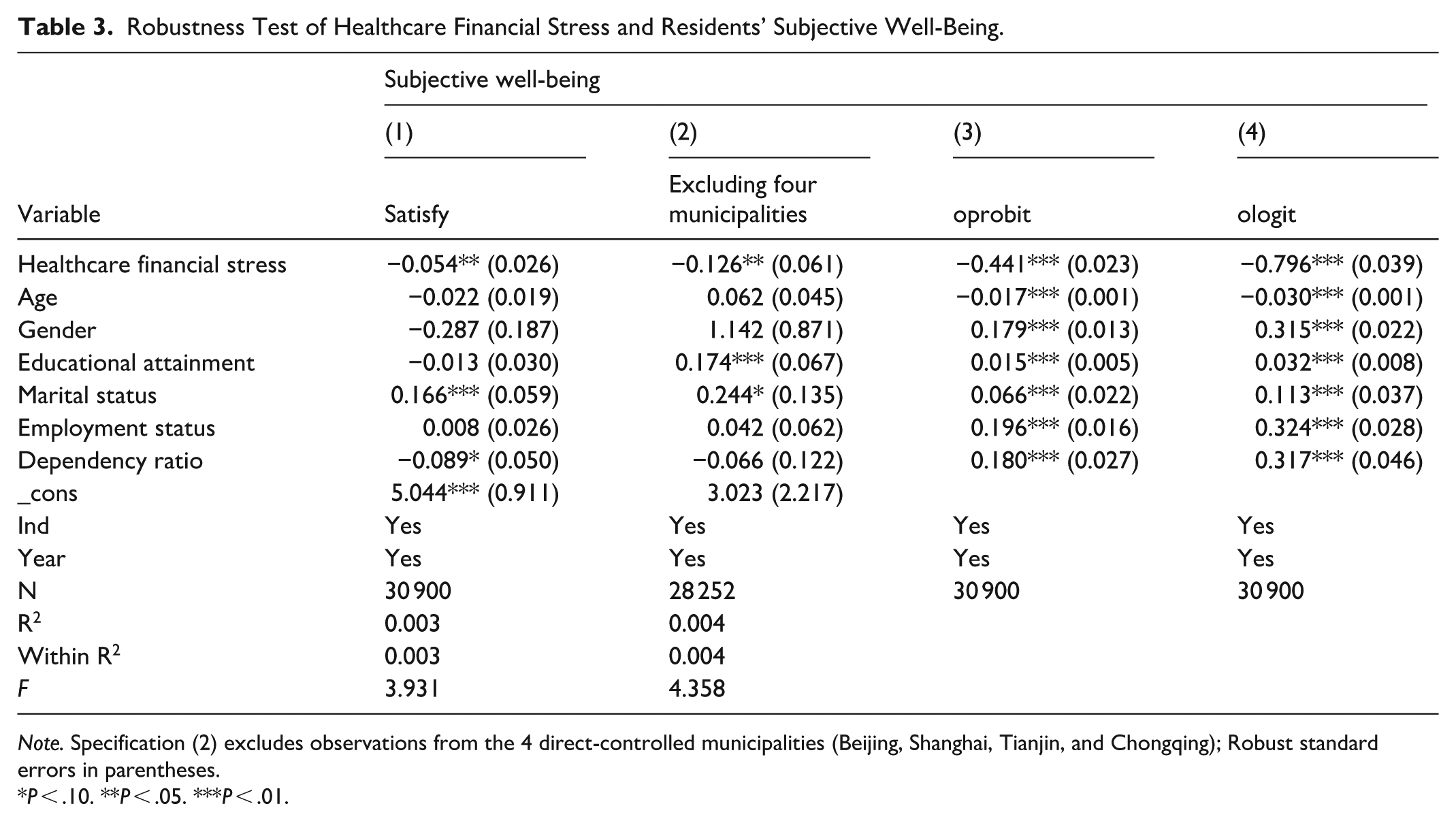
Note. Specification (2) excludes observations from the 4 direct-controlled municipalities (Beijing, Shanghai, Tianjin, and Chongqing); Robust standard errors in parentheses.
P < .10. **P < .05. ***P < .01.
First, in view of the multidimensional nature of subjective well-being, the original dependent variable “happiness” is replaced with “life satisfaction” (Satisfy), and the 2-way fixed effects model is re-estimated. The coefficient on healthcare financial stress is −0.054 and remains statistically significant at the 5% level, indicating that the main finding is robust to using an alternative subjective well-being measure.
Second, to rule out potential heterogeneity arising from the distinctive allocation of public healthcare resources in municipalities, the sample is re-estimated after excluding Beijing, Shanghai, Tianjin, and Chongqing. The estimated coefficient of healthcare financial stress is −0.126 and continues to be significantly negative, which further strengthens the credibility of the baseline result.
Finally, given that the happiness variable is inherently ordered categorical, ordered Probit (oprobit) and ordered Logit (ologit) models are additionally employed to estimate the effect of healthcare financial stress. The regression results show that the coefficients on healthcare financial stress are −0.441 and −0.796 in the ordered Probit and ordered Logit models, respectively, and both are statistically significant at the 1% level. These findings confirm that the negative association between healthcare financial stress and subjective well-being is robust to alternative modeling strategies.
Taken together, the results based on variable substitution, sample adjustment, and model re-specification consistently point to a significant adverse effect of healthcare financial stress on residents’ subjective well-being. Overall, these robustness checks provide strong support for Hypothesis
Mechanism Analysis
Drawing on relevant literature and theoretical considerations, this study further investigates the specific mechanisms through which healthcare financial stress affects residents’ subjective well-being. Conceptually, healthcare financial stress can influence well-being through at least 2 pathways. First, via a health channel, heightened financial pressure related to healthcare may delay or reduce timely healthcare utilization, increase stress exposure, and ultimately worsen perceived or actual health status. Second, via an economic channel, healthcare-related payments and financial pressure may crowd out other household expenditures, tighten the household budget, and reduce the resources available for daily consumption and future planning, thereby lowering subjective well-being.
To examine these channels empirically, we specify a mediation model in which health status and household disposable income are sequentially treated as dependent variables, and healthcare financial stress is used as the key explanatory variable. This approach allows us to test whether healthcare financial stress is significantly associated with (i) worse health status and (ii) reduced disposable resources—2 conditions consistent with the proposed transmission mechanisms. The regression results are reported in Table 4.
Mediation Effects of Healthcare Financial Stress on Residents’ Subjective Well-Being.

Note. Robust standard errors in parentheses.
P < .10. **P < .05. ***P < .01.
Along the health-related channel, Model (1) shows that the coefficient of healthcare financial stress on health status is −0.137 and statistically significant at the 1% level. This finding indicates that, conditional on other factors, an increase in healthcare financial stress significantly worsens residents’ health status, providing empirical support for an indirect effect operating through the pathway of “health deterioration → lower subjective well-being.”
Along the economic channel, Model (2) shows that the coefficient of healthcare financial stress on household disposable income is −0.284, which is likewise negative and significant at the 1% level. This result suggests that healthcare financial stress substantially compresses households’ discretionary budget space, heightens economic strain and financial constraints, and thereby reduces individuals’ subjective well-being.
Taken together, the evidence indicates that healthcare financial stress not only directly depresses residents’ subjective well-being in the baseline regressions, but also indirectly amplifies its adverse impact through 2 mediating channels—deteriorating health status and shrinking disposable resources. The direction of these mediation effects is highly consistent with everyday experience and provides strong overall support for Hypothesis 2.
Heterogeneity Analysis
To further examine whether the impact of healthcare financial stress on residents’ subjective well-being varies across groups, this study conducts a heterogeneity analysis along 2 dimensions: region and urban–rural residence. Specifically, separate regressions are estimated for the eastern, central, and western regions, as well as for rural and urban subsamples. The results are reported in Table 5.
Heterogeneous Effects of Healthcare Financial Stress on Residents’ Subjective Well-Being.

Note. Robust standard errors in parentheses.
P < .10. **P < .05. ***P < .01.
From the regional perspective, healthcare financial stress exerts a significantly negative effect on subjective well-being in both the eastern and central regions. The estimated coefficient for the eastern region is −0.191 and is statistically significant at the 5% level, while the coefficient for the central region is −0.185 and significant at the 10% level. These findings suggest that even in eastern and central China—where healthcare resources are relatively concentrated and service capacity is comparatively strong—residents still face a substantial healthcare-related financial stress. On the one hand, the ongoing processes of urbanization and population aging have heightened health-related anxiety, making medical expenditures more likely to translate into noticeable pressure on subjective well-being. On the other hand, the central region as a whole remains in a “climbing over the hump” stage of economic development, with relatively limited risk-pooling capacity in the health insurance system and narrower financial buffers at the household level; as a result, the adverse impact of healthcare financial stress on subjective well-being is particularly pronounced.
By contrast, the estimated coefficient for the western region is 0.017, which is positive but statistically insignificant, indicating that healthcare financial stress does not exert a clear effect on subjective well-being in this region. A plausible explanation is that, first, the overall level of economic development in western China is relatively low, and residents’ expectations regarding public healthcare services are more modest, which may strengthen their perceived gain from simply “having access to care.” Second, the state has long implemented targeted health poverty alleviation and pro-poor health insurance policies—such as “treatment before payment” and “one-stop reimbursement”—which have effectively cushioned the medical stress and anxiety of low-income groups, thereby attenuating the negative effect of healthcare financial stress on subjective well-being.
From the urban–rural perspective, the coefficient of healthcare financial stress for the rural subsample is −0.127 and statistically significant at the 10% level, which is broadly consistent with prior expectations. Rural residents generally have lower income levels, face gaps in health insurance protection and healthcare accessibility, and are more likely to delay treatment for minor illnesses or forgo timely care for serious conditions. Under such circumstances, medical expenditures are more readily transformed into direct economic pressure on the household, thus significantly undermining individual subjective well-being.
In contrast, for the urban subsample, the coefficient on healthcare financial burden is −0.144 and thus also negative in sign, but it does not reach conventional levels of statistical significance. This pattern may indicate that urban residents, by virtue of higher income levels and more comprehensive social security systems, possess stronger capacity to cope with risks and share healthcare costs. In addition, supplementary mechanisms such as commercial health insurance help buffer the financial impact of medical spending, so that such expenditures are more likely to be perceived as routine investments rather than salient sources of psychological stress.
Overall, the regional and urban–rural heterogeneity analysis jointly indicates that the adverse effect of healthcare financial stress on subjective well-being is more pronounced among groups with weaker economic foundations and less adequate protection capacity. These findings further corroborate that the transmission pathways and impact intensity of healthcare-related financial stress differ across social groups.
Discussion
Discussion and Implications of the Findings
This study focuses on how healthcare financial stress affects residents’ subjective well-being and generates several important implications at both the theoretical and empirical levels.
First, using 2018 to 2022 CFPS micro panel data, we estimate an individual fixed-effects model that largely controls for time-invariant unobserved heterogeneity. Compared with cross-sectional studies, this design more robustly identifies the relationship between healthcare financial stress and well-being, adding evidence on the “healthcare burden–well-being” nexus in China. Related work also shows that household health-related expenditures do not necessarily increase happiness or life satisfaction and may even be negatively associated with them. 48
Second, mechanism analyses indicate that healthcare financial stress not only directly reduces subjective well-being but also amplifies its adverse impact through 2 mediating pathways—worsening health status and compressed household disposable income—supporting both a “health channel” and an “economic channel.” Health shocks significantly lower subjective well-being among middle-aged and older adults, with stronger negative effects in rural and other vulnerable groups. 49 Catastrophic health expenditure can undermine household living standards and is associated with poorer mental health. 50 These findings imply a multi-pronged policy response—strengthening health insurance protection, improving cost-sharing arrangements, and enhancing income-support policies—to alleviate healthcare financial stress and raise overall well-being.
Third, heterogeneity results show that the negative effect is more pronounced among groups with weaker economic foundations and limited protection capacity, concentrated in rural areas and China’s central/eastern regions, while being relatively weaker for urban and western populations. This pattern echoes evidence that health shocks and healthcare burdens impose larger well-being losses on rural and disadvantaged groups, 51 implying the need for more targeted burden relief and institutional support across regions and the urban–rural divide.
Overall, by systematically incorporating healthcare-related economic factors into the study of subjective well-being, this paper represents an attempt at interdisciplinary integration across healthcare, psychological stress, and welfare outcomes. The findings indicate that reducing the healthcare financial burden is not only a core agenda of health policy, but also a critical pathway for improving residents’ happiness and advancing the goal of “common prosperity.” In this sense, the evidence provided here offers an empirical foundation for subsequent institutional debates on the feasibility of free healthcare or quasi-free basic medical care.
Feasibility of Quasi-Free Basic Healthcare: An Institutional Pathway to Reducing Healthcare Financial Stress
Our panel evidence indicates that healthcare financial burden—captured by both objective out-of-pocket expenditure and subjective perceptions of “difficulty in seeking medical care”—significantly undermines residents’ subjective well-being, with disproportionately larger effects among low-income households and families with sick members. This pattern suggests that, within the current institutional configuration, marginal adjustments (eg, slightly higher reimbursement rates or broader benefit lists) are unlikely to eliminate the structural anxiety of “falling into poverty due to illness” or “returning to poverty because of illness.” A quasi-free basic healthcare model, primarily delivered through public providers, therefore emerges as a controversial yet normatively defensible and practically relevant policy option.
Macro fiscal Capacity: From Nominal GDP to “Welfare-Related GDP.”
In 2023, China’s total health expenditure reached about 9.06 trillion yuan (7.2% of nominal GDP). However, nominal-GDP comparisons may understate fiscal room for welfare-enhancing reforms because a sizable share of growth has been investment-driven, especially through real estate and infrastructure. Estimates show that the real estate sector and its induced upstream–downstream value added accounted for roughly 24.5% of GDP in 2021, 52 and recent evidence points to high “multiplier-like” contributions from broad real estate and infrastructure relative to manufacturing. 53 Further, as Rogoff and Yang’s analysis, summarized in the Stanford SCCEI China Brief, shows, real estate and infrastructure combined accounted for roughly 31.7% of China’s GDP in 2021 and approached 34% in 2015, with declining marginal returns over time. 54 Drawing on “welfare-adjusted GDP,” 55 we adopt a conservative scenario that discounts one-third of nominal GDP as low-welfare, bubble-like increments, yielding a “welfare-related GDP” of about 84 trillion yuan in 2023 and implying a health spending share near 10.8%. 56 Under this perspective, the binding constraint is less the absolute scarcity of resources than the allocation efficiency and priority structure of public spending.
Reclaiming Eroded Fiscal Space via Institutional Reform
Supplier-induced demand and rent-seeking are reinforced by revenue structures tied to drug mark-ups, diagnostics, and equipment, as well as soft budget constraints and weak insurance-fund oversight. 57 Empirical work documents excessive testing, redundant medication, inflated billing, and fraud, 58 implying a non-trivial share of wasteful spending. 59 Payment reform (DRG/DIP prospective payment and global budgeting) and strengthened supervision, alongside anti-corruption, can reclaim fiscal space and redirect it toward burden reduction without necessarily raising aggregate spending. 60
Pharmaceutical Reform and a “Medicine Price Dividend.”
India’s experience highlights the policy leverage embedded in TRIPS flexibilities—higher patentability thresholds, limits on evergreening, selective compulsory licensing, and strong support for quality-assured generics. For China, stricter criteria for “substantive innovation,” price negotiation or limited compulsory licensing for essential high-priced drugs, deeper generic consistency evaluation, and institutionalized volume-based procurement could convert pharmaceutical “price bubbles” into a stable “medicine price dividend” financing essential medicines.
Quasi-Free Basic Healthcare: From Normative Vision to Policy Design
Japan shows that near-free care can be achieved through universal enrollment, a unified benefits package, and centrally negotiated fees, keeping OOP around 10% of total health expenditure. 61 Yet China’s comparatively high household OOP reflects a financing structure tilted toward families and fiscal priorities favoring infrastructure and real estate. 62
Given governance and incentive risks, universal zero co-payment is premature. A feasible pathway is a public-sector-led, quasi-free basic package focusing on essential services and high-risk populations: primary facilities providing registration-free/low co-payment care supported by capitation and global budgets, 63 higher protection for catastrophic illness with strict annual OOP caps and targeted assistance, 64 tiered co-payments for high-cost diagnostics and special-demand services, and improved transparency and counseling to reduce information asymmetry and anxiety, 65 complemented by disease-specific subsidies for high-prevalence chronic conditions. 66 Overall, quasi-free basic healthcare should be operationalized as a reform agenda that restructures spending, reclaims waste, and ring-fences resources to explicitly reduce healthcare financial burden.
Limitations and Directions for Future Research
Drawing on nationally representative CFPS panel data from 2018 to 2022 and employing 2-way fixed-effects and mediation models, this study identifies how healthcare financial stress affects subjective well-being through both economic and psychological pathways. The findings remain robust across multiple sensitivity checks and exhibit a reasonable degree of reliability and explanatory power. Nonetheless, several limitations should be acknowledged.
First, healthcare financial stress is primarily measured by the ratio of annual household medical expenditure to annual total household consumption, which captures mainly the economic burden dimension. Due to the constraints of the CFPS questionnaire, the analysis does not incorporate information on healthcare accessibility, service quality, disease severity, or the time costs of caregiving. As a result, it is difficult to fully reflect the multidimensional structure of healthcare financial stress. Second, because this study is based on existing survey data, no formal sample size or power analysis was conducted at the research design stage, and the discussion of institutional scenarios such as quasi-free basic healthcare largely remains at the level of theoretical reasoning and experience-based extrapolation. Future work should therefore combine policy pilots with richer data sources to subject these institutional proposals to more rigorous empirical testing.
Overall, these limitations do not overturn the core conclusions of the study; rather, they highlight promising avenues for further research. Subsequent work could refine measurement scales for healthcare financial stress, improve the identification of heterogeneity among vulnerable groups, and strengthen policy simulations and institutional evaluations. Such efforts would provide more solid empirical support for alleviating healthcare financial burden and enhancing residents’ subjective well-being.
Conclusion
Drawing on CFPS panel data from 2018 to 2022, this study systematically examines how healthcare financial stress affects residents’ subjective well-being and through which mechanisms. Baseline regressions, controlling for individual and time fixed effects as well as a series of demographic and household characteristics, reveal a significant and robust negative association: a 1%-point increase in healthcare financial stress is associated with an average decline of about 0.13 points in self-reported happiness. Descriptively, the mean happiness score falls from 7.470 to 7.145 among those facing healthcare financial stress, a drop of 0.325 points, indicating that the economic stress of healthcare has become an important source of erosion of subjective well-being.
Mechanism analysis further shows that healthcare financial stress amplifies its adverse impact through 2 indirect channels—worsened health status and a reduction in freely disposable household income. Heterogeneity tests suggest that low-income groups, rural residents, and individuals with relatively weak social security coverage are disproportionately affected, implying that healthcare financial stress has become a key constraint on the pursuit of common prosperity.
Fiscal Feasibility Analysis of the Transformation: Short-term (3-5 years): This transformation primarily relies on adjusting the existing structural framework rather than large-scale incremental investments. First, the adoption of DRG/DIP payment reforms will change the provider incentive mechanism, curb over-treatment, and save healthcare funds. Second, centralized bulk procurement of pharmaceuticals and medical supplies can save over 100 billion yuan in healthcare funds annually, and these “system dividends” can be directed to compensate for the technical service income of public hospitals. Third, optimizing the revenue and expenditure structure of public hospitals can help reduce management costs.
Long-term (5+ years): The necessary incremental investments mainly include: (1) explicit government responsibility for medical care (infrastructure, equipment, key disciplines); (2) costs related to the reform of medical staff compensation systems; and (3) investments to strengthen primary healthcare capacity. However, compared to the “market-driven” model, this approach can avoid waste of healthcare funds and the continuous rise of patient out-of-pocket expenses, potentially leading to a lower net fiscal cost. The experience of the Sanming healthcare reform shows that after strengthening the public healthcare system, the share of fiscal health expenditure only increased by 0.3% to 0.5% points, while the efficiency of healthcare fund utilization improved by over 15%, serving as a model for others.
Policy Recommendations: Accelerate the Expansion of DRG/DIP Payment Reform: By the end of 2024, DRG/DIP payments will cover over 70% of the pooled areas. It is recommended to add a “public welfare-oriented” adjustment factor based on the current disease group weights, to provide reasonable compensation for the public health tasks and critical care provided by public hospitals, thereby avoiding the weakening of public welfare due to cost orientation.
Deepen the Application of AI-based Medical Insurance Supervision Systems: The coverage of AI-based medical insurance supervision has exceeded 90% nationwide. The focus of supervision should shift from cost compliance to medical quality and appropriateness. AI should be used to identify over-testing and unreasonable medication, guiding public hospitals to standardize diagnosis and treatment behaviors, and providing technical support for the public-led model.
Clarify the Fiscal Support Mechanism for Centralized Bulk Procurement: The savings from centralized procurement should not simply be transferred to medical insurance pooling but should establish a “medical insurance-finance-hospital” tripartite sharing mechanism. A portion of the savings should be directed toward increasing medical staff salaries to stabilize the public healthcare workforce.
Supplemental Material
sj-docx-1-inq-10.1177_00469580261440165 – Supplemental material for Impact of Healthcare Financial Stress on Residents’ Subjective Well-Being: Health Status and Household Disposable Income as Mediators
Supplemental material, sj-docx-1-inq-10.1177_00469580261440165 for Impact of Healthcare Financial Stress on Residents’ Subjective Well-Being: Health Status and Household Disposable Income as Mediators by Juanjuan Su, Gai Liu and Guanglin Cheng in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Appendix
PSM Estimation Results.

| Matching method | Treated group | Control group | ATT | Std. error |
|---|---|---|---|---|
| K-nearest neighbor matching with caliper | 7.146 | 7.527 | −0.382*** | 0.053 |
| Radius matching | 7.145 | 7.442 | −0.296*** | 0.045 |
| Kernel matching | 7.145 | 7.441 | −0.296*** | 0.045 |
| Average | 7.145 | 7.470 | −0.325*** | — |
Note. ATT denotes the average treatment effect on the treated.
P < .10. **P < .05. ***P < .01.
Acknowledgements
The guidance and assistance provided by the esteemed elder individuals, Tang Ke, Wang Yuxiang from Zhengzhou University School of Management, as well as Professor Zhou Janchao from Yangzhou University College of Marxism are sincerely appreciated.
Ethical Considerations
The CFPS project received ethics approval from the Biomedical Ethics Review Committee of Peking University under the unified IRB approval number IRB00001052-14010, which applies across survey waves. The present study used de-identified public data and was conducted in accordance with relevant ethical standards.
Consent to Participate
Informed consent was obtained from all participants by the CFPS project. The present study analyzed de-identified, publicly available CFPS 2018-2022 data; therefore, additional informed consent from participants was not required.
Consent for Publication
All the authors listed in this paper read the manuscript and agreed to submit it for publication.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the key project of the 2025 Basic Scientific Research Funds Special Program of the Ministry of Education Vocational Education Development Center, “Research and Practice on Vocational Education Serving an Aging Society” (Project No. ZG202508).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
CFPS 2018-2022 public-use data are publicly available from the China Family Panel Studies (CFPS) data repository. The datasets analyzed during the current study are available from the corresponding author upon reasonable request.*
Grant Number
ZG202508.
Supplemental Material
Supplemental material for this article is available online.