
Abstract
Health care-related tasks (e.g., making appointments, talking to providers) performed by informal caregivers caring for older adults with dementia have become increasingly common, yet the evidence on caregiving task profiles remains fragmented and has not been comprehensively synthesized. This is a systematic review with narrative synthesis of the patterns of health care-related tasks and the characteristics of caregivers who performed them. We searched PubMed, Embase, PsychInfo, Web of Science, and CINAHL databases. The identified tasks were grouped into health and medical care, advocacy and care coordination, and surrogate tasks. We also reported caregiver characteristics. We included 12 studies. Only 5 studies reported on racial and ethnic minority caregivers. Medication management was the most common health and medical care task. Only 1 study reported surrogate tasks, and 2 studies reported caregivers performing advocacy and care coordination tasks. This study is particularly timely given the recent implementation of the Centers for Medicare and Medicaid Services (CMS) Guiding an Improved Dementia Experience (GUIDE) Model, which includes caregiver support and education as core components of dementia care delivery. Systematically characterizing the health care-related tasks performed by dementia caregivers can inform the design, targeting, and evaluation of the GUIDE Model.
Introduction
As of 2024, approximately 6.7 million people in the United States (US) have Alzheimer’s disease and related dementias, and the number is predicted to rise to 14 million people by 2060. 1 People living with dementia (PLWDs) require assistance with activities of daily living (ADLs), such as bathing, feeding, and dressing, as well as instrumental activities of daily living (IADLs), such as preparing meals and shopping. 2 Informal caregivers are individuals who provide unpaid assistance with ADLs or IADLs to a person with a chronic disease or disability, including family members, friends, and relatives. 3
In addition to ADLs and IADLs, informal caregivers also assist with health care-related tasks, such as making appointments, coordinating care, and managing medications. According to the Home Alone Revisited report, 50.1% of family caregivers perform health care-related tasks. 4 Although medication management was categorized as one of the IADLs, more recent research has separated medication management and other health care-related tasks from ADLs and IADLs because these tasks have become increasingly complex over the years and require medical knowledge and skills.5-7 Caregivers are expected to handle complex medication regimens, give injections, manage intravenous lines, provide wound care, and other sophisticated medical tasks, often without the necessary training.8-11 Family caregivers are generally responsible for educating themselves on how to perform health care-related tasks. 4 Performing these tasks can be stressful, difficult, and time-consuming.7,12-15 While performing health care-related tasks, 27.5% of informal caregivers feared making mistakes. 4
In addition, the complex and fragmented health care system in the US contributes to challenges for caregivers. From 2000 to 2019, the proportion of Medicare beneficiaries seeing 5 or more physicians annually in the outpatient setting has increased from 17.5% to 30.1%. 16 In a national survey conducted by the Commonwealth Fund, 77% of caregivers would like health care advocates to help them navigate the health system, and 68% would like care coordination by social workers or trained professionals. 17
The Home Alone Revisited report recommended assessing the prevalence of medical/nursing tasks to provide a comprehensive overview of the caregiver’s experience. This has been done by Lee and colleagues, focusing on the prevalence, types, and impact of medical/nursing tasks performed by informal caregivers of PLWDs. 18 The National Academies of Sciences, Engineering, and Medicine’s Families Caring for an Aging America report indicated that caregiving activities range widely, encompassing not only medical and nursing tasks, but also advocacy, care coordination, and surrogate tasks. 19 The detailed description is shown in Supplemental Table S1.
Our review builds upon Lee et al’s work and incorporates other health care-related tasks outlined in the Family Caregiving for Aging America report. 18 This narrative synthesis review examines the patterns and characteristics of health care-related tasks, and the characteristics of informal dementia caregivers. This study is timely, following the Food and Drug Administration approval of disease-modifying therapies for Alzheimer’s disease, which require frequent infusion and regular imaging monitoring, necessitating caregiver involvement in health care-related tasks. 20 This study is also timely, following the Centers for Medicare and Medicaid Services’ (CMS) announcement in July 2024 of the nationwide initiation of the Guiding an Improved Dementia Experience (GUIDE) Model. 21 The GUIDE Model aims to support PLWDs and their caregivers through a comprehensive package of care coordination, caregiver support and education, and respite services. 21 Implementation involves assigning PLWDs and their caregivers to care navigators, who deliver standardized dementia care through an interdisciplinary team. 21 Caregivers are offered supportive services after their caregiving strain is assessed using validated tools. 22 Starting in the second year, evaluation will include performance-based payments to participating organizations, with the CMS planning to incorporate reductions in caregiver strain as a performance metric. However, the specific measurement approach has not yet been finalized. 22 Moreover, the GUIDE Model does not yet provide a detailed, evidence-based specification of the types and complexity of health-care related tasks performed by informal dementia caregivers. This review helps address that gap by consolidating evidence on caregivers’ task profiles and characteristics of caregivers performing them. Findings from this study help inform policy directions by identifying the types and complexity of caregivers’ tasks, which can guide task-specific training and support, risk and role-based targeting of services, and the development of meaningful process and outcome measures to evaluate the GUIDE Model’s effectiveness.
Despite growing recognition of the caregiver’s role in managing complex healthcare-related tasks, evidence describing the range and patterns of these responsibilities among informal dementia caregivers remains fragmented. A clearer synthesis of caregivers’ task profiles is needed to understand the scope of caregiver involvement and demands placed on families. Therefore, this systematic review with narrative synthesis aims to examine the types and patterns of healthcare related task performed by informal caregivers of PLWD and to characterize the caregivers who perform them. By consolidating this evidence, this review seeks to inform caregiver support strategies and policy initiatives, particularly in the context of emerging dementia care models such as the CMS GUIDE Model, where understanding caregiver task complexity can support implementation, service targeting, and evaluation.
Methods
This systematic review with narrative synthesis was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement. 23 The completed PRISMA checklist is available in Supplemental Table S2. As this review was based on previously published studies and did not involve human subjects, ethical approval and informed consent were not applicable in this study.
Data Sources and Search Strategy
A comprehensive search was performed in MEDLINE/PubMed, Embase, CINAHL, PsychINFO, and Web of Science databases from inception to October 1, 2023. During manuscript revision, 1 additional eligible study published in February 2026 was identified through the author’s knowledge and incorporated into the review. The search strategy was developed using the terms “Dementia” AND “Caregivers” AND “Tasks.” All possible synonyms, MeSH terms, and key terms were considered. The detailed search syntax is given in Supplemental Table S3. The bibliography of the included studies was also searched for additional studies.
Study Selection
The inclusion criteria are as follows: (a) studies including informal dementia caregivers, (b) studies reporting patterns of health care-related tasks, (c) original research including cross-sectional studies, randomized controlled trials, secondary analyses of observational studies, and qualitative studies, (d) studies conducted in the US and published in English, and (e) studies reported more broadly on tasks performed by caregivers were eligible for inclusion, as long as results for health care-related tasks were reported separately for informal dementia caregivers. The exclusion criteria are as follows: (a) studies focusing on caregivers of people living with conditions other than dementia or paid caregivers, (b) studies including caregivers of older adults with multiple conditions (including dementia) were excluded unless dementia-specific caregiver results were reported separately, (c) studies that did not report health care-related tasks, (d) studies that were non-English and conducted outside of the US, and (e) qualitative studies that did not specify the number of caregivers reporting such tasks were excluded from our study. There was no restriction on the year of publication. Health care-related tasks were not commonly considered in the literature; therefore, citations that dealt with any kind of task, duty, or responsibility performed by informal dementia caregivers were included in the search. The screening was performed in a 2-step process. Initially, the titles and abstracts of the retrieved articles were screened for inclusion, followed by a full-text screening. Two independent reviewers (MZ, SB) conducted the screening process, and discrepancies were resolved through discussion within the research group.
Data Extraction and Synthesis
The extracted data variables included study characteristics, caregiver characteristics (age, sex, relationship to the care recipient, race and ethnicity, receipt of support service and training), and characteristics of older adults with dementia (types and severity). We extracted quantitative data on caregivers’ involvement in health care-related tasks, and qualitative data such as types, and definitions of health care-related tasks following the approach of Lee et al. 18 If a study did not report these findings, they were stated as not reported. Based on the aforementioned report Families Caring for an Aging America, we grouped health care-related tasks into 3 categories: health and medical care, advocacy and care coordination, and surrogate tasks. 19 Two independent reviewers (MZ, SB) performed the data extraction, and any discrepancies were resolved by discussion within the research group with the third and fourth reviewers (NL, CJT). While extracting data from the qualitative studies, we considered the number of caregivers performing health care-related tasks as indicative of caregivers’ involvement in these tasks.
Due to the heterogeneity in task definitions across studies, a meta-analysis was not feasible. Therefore, we adopted a narrative synthesis and presented the findings in descriptive tables to summarize and compare the results across the studies.
We followed the 4 steps of narrative synthesis outlined by Popay et al, 24 in which the first step is to develop a theoretical framework. As mentioned above, our theoretical framework is based on the classification of healthcare-related tasks described in the Families Caring for an Aging America report (Supplemental Table S1). 19 The second step is developing a preliminary synthesis by presenting the study designs and populations and identifying patterns. We presented the study characteristics, characteristics of informal dementia caregivers, and informal dementia caregivers’ involvement in health care-related tasks. The third step is exploring relationships in data. We summarize the characteristics of caregivers who perform these tasks and compare caregivers’ involvement in health care-related tasks with the theoretical framework. The last step is to assess the robustness of the synthesis. We assessed the quality of the included studies using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist and reported the results.
Quality Assessment
The JBI critical appraisal tool for prevalence studies was used to assess the quality of the included studies. 25 The JBI tool has 9 criteria assessing various aspects of study design and execution, described elsewhere. 25 We presented the results of critical appraisal for all criteria. The JBI expert group advised against using a cut-off score from the 9 criteria in quality appraisal. 26 In the quality assessment, we described the total number of criteria met for each study. Given our research question, Criterion No. 4, “Were the study subjects and the setting described in detail?” and Criterion No. 7, “Was the condition measured in a standard, reliable way for all participants?” were most critical, because Criterion No. 4 guided the extraction of information on caregiver characteristics and health care-related tasks, which aligns with the objective of this review. Criterion No. 7 was highlighted due to the inconsistency in how health care-related tasks are defined in the literature. Therefore, whether the included studies clearly defined and measured these tasks was also an important consideration. We also described the percentage of studies that met these 2 criteria. Two independent reviewers (MZ, SB) performed the quality assessment, and any discrepancies were resolved by discussion within the research group. Although the JBI Critical Appraisal Checklist for Prevalence Studies is typically used for quantitative studies, we applied it to a subset of qualitative studies that reported caregiver counts for specific health care-related tasks. This approach aligns with our objective of examining patterns in health care-related caregiving tasks.
Results
The findings of this narrative synthesis are presented according to study selection, study characteristics, caregiver characteristics, and caregivers’ involvement in health care-related tasks. Findings from both quantitative and qualitative studies are integrated to provide a comprehensive description of caregiving patterns and caregiver characteristics.
Study Selection
A total of 8772 records were identified from database searches, and 1 study was identified through other sources. The removal of duplicates (n = 2498) resulted in 6275 unique articles. After the study selection process, 12 articles were included. The PRISMA flow diagram illustrating the study selection process is presented in Figure 1.

PRISMA flow diagram.
Study Characteristics
Of the 12 articles, 8 were quantitative studies that used observational data, and 4 were qualitative studies.5,27-37 All the quantitative studies used nationally representative surveys such as the National Health and Aging Trends Study (NHATS) and National Study of Caregiving (NSOC) databases of 2011 (n = 2), 2017 (n = 1), and 2023 (n = 1), the 1999 and 2004 National Long-Term Care Survey (NLTCS) and NHATS data from 2011 and 2015, linked with caregiver surveys and Medicare claims, the National Health and Wellness Survey, the Home Alone study, and the Caregiving in the US 2020 study.5,28,31-35,37 The 4 qualitative studies took place in Oregon, Illinois, New York, and 2 large metropolitan cities in the Southwestern United States.27,29,30,36 Sample sizes of the caregivers ranged from 13 to 1887. Six studies using nationally representative survey data did not report the weighted population estimates.28,31-35 Ten studies included care recipients with dementia,5,27-29,31-34,36,37 one study included care recipients with memory problems, including dementia and Alzheimer’s disease, 35 and 1 study included only care recipients with Alzheimer’s disease. 30 The study characteristics are reported in Table 1.
Study Characteristics.
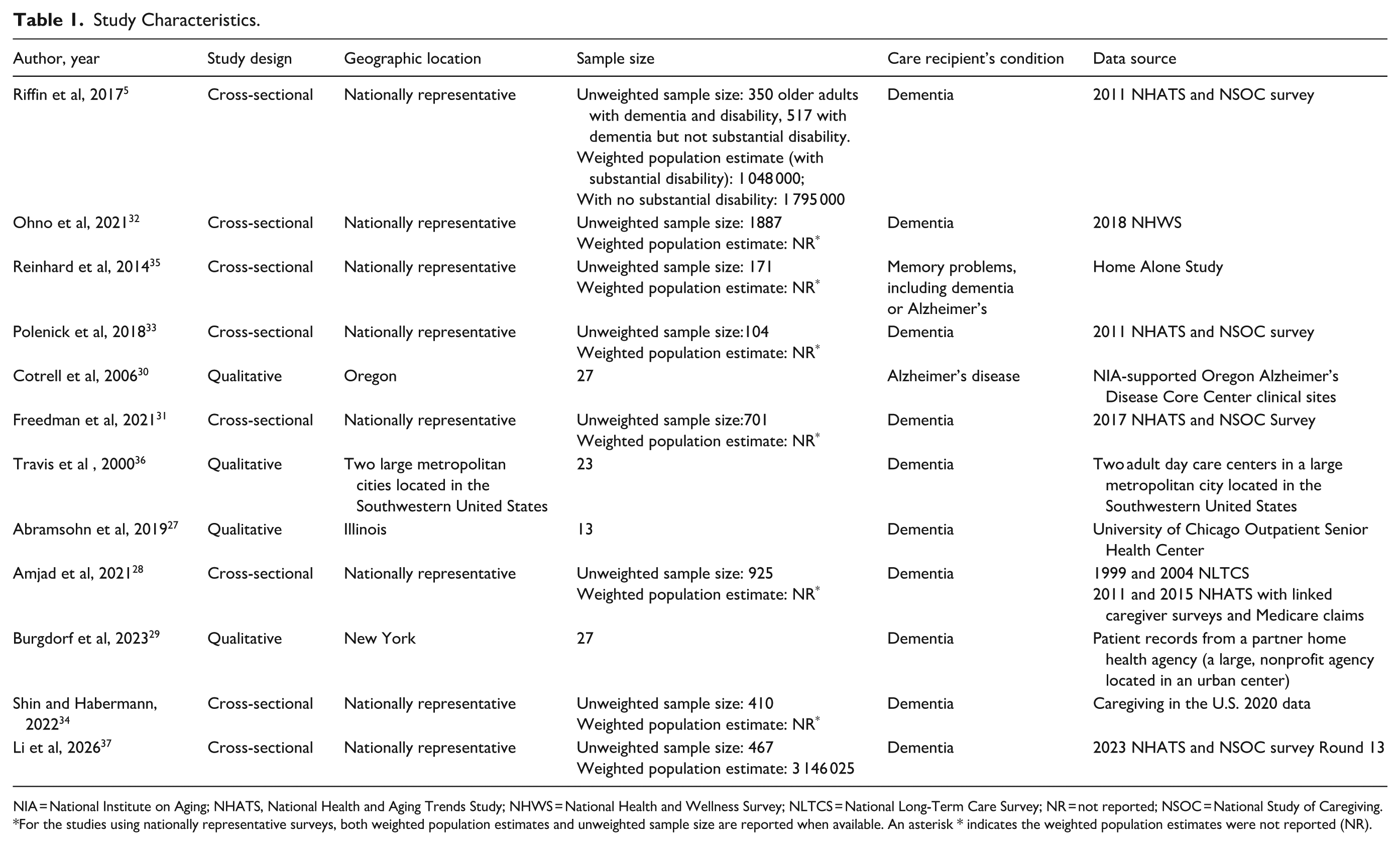
NIA = National Institute on Aging; NHATS, National Health and Aging Trends Study; NHWS = National Health and Wellness Survey; NLTCS = National Long-Term Care Survey; NR = not reported; NSOC = National Study of Caregiving.
For the studies using nationally representative surveys, both weighted population estimates and unweighted sample size are reported when available. An asterisk * indicates the weighted population estimates were not reported (NR).
Caregiver Characteristics
The characteristics of caregivers are given in Table 2. The average age of caregivers ranged from 58 to 76 years, as reported in 6 studies.5,29-31,33,34 All studies reported a higher percentage of female caregivers ranging from 56% to 85% and male caregivers ranging from 19% to 44%.5,27-36 The 2 major groups of caregivers were spousal caregivers (11%-93%),5,27-31,34,36 and care recipients’ children (1%-78%).5,27,29,30,34,36 The remaining studies reported other relationships between care recipients and caregivers, such as relatives, siblings, and friends. Reporting of race and ethnicity was inconsistent across the included literature. Seven of the 12 studies did not report the racial or ethnic composition of participants,27,29-31,34,36,37 of which only 3 had diverse samples, including White (37%-60.7%), Black (10%-30%), Hispanic (10.7%-26%), and Asian (7%-12.7%).29,34,37 Only 1 study reported the caregivers’ employment status, where 33% of them were employed. 28 Three studies reported the duration of caregiving in years.29,34,37 Burgdorf et al reported that 46% of the caregivers have cared for care recipients for 1 to 5 years, 42% have cared for 5 or more years, and 12% have cared for less than a year. 29 Shin and Habermann reported the average duration of caregiving as 4.6 years, and 31.7% of caregivers provided care for more than 5 years. 34 Li et al reported that 74.9% of caregivers provided over 4 years of caregiving. 37
Characteristics of Informal Dementia Caregivers.

NR = not reported.
Riffin et al (2017) reported results separately for PLWDs with substantial disability, and PLWDs without substantial disability. The results with a represent PLWDs without substantial disability. The results without a represent PLWDs with substantial disability.
Ohno et al (2021) and Amjad et al (2021) reported age categories and frequency distribution in each category.
Reinhard et al (2014) did not provide caregiver demographic characteristics. Therefore, these are indicated as “NR”.
Travis et al (2000) reported the age range in years.
Abramsohn et al (2019) reported median age.
Li et al (2026) reported age category and percentage distribution in each category.
For the studies using nationally representative surveys, both weighted population estimates and unweighted sample size are reported when available. An asterisk * indicates the weighted population estimates were not reported (NR).
Few caregivers used support services (including support groups, respite services, and financial support) and received training from health professionals. Only 2 studies reported caregivers’ use of support services.5,28 Riffin et al reported that 9% of caregivers caring for PLWDs with substantial disabilities joined support groups, as opposed to 4% of those without substantial disability. This study also highlighted a higher percentage (23%) of caregivers caring for PLWDs with substantial disability using respite care services compared to 10% of those without substantial disability. 5 Amjad et al reported that 6% and 24% of caregivers used support groups and respite care services, respectively. 28 No study reported caregivers receiving financial support, and only 2 studies reported the percentages of caregivers who had received training from health care providers.5,37 A higher percentage of caregivers (14%) caring for PLWDs with substantial disability reported being trained by health care providers compared to 6% of caregivers caring for PLWDs without substantial disability. 5 Li et al reported that around 58% of the caregivers received training from health care providers after helping with overnight hospital stay. 37 Regarding the distribution of caregivers across rural and urban areas, none of the 8 quantitative studies reported information on the rural or urban status, despite using nationally representative data. In the 4 qualitative studies, only Abramsohn et al reported that the caregivers were from an urban area. 27
Health Care-Related Tasks
We grouped the health care-related tasks into 3 groups: Health and medical care, advocacy and care coordination, and surrogate tasks (Table 3). 19
Informal Dementia Caregivers’ Involvement in Health Care-Related Tasks.

NR = not reported.
Riffin et al (2017) reported results separately for PLWDs with substantial disability, and PLWDs without substantial disability. The results with a represent PLWDs without substantial disability. The results without a represent PLWDs with substantial disability.
Freedman et al reported the mean minutes of care over the prior day provided by family caregivers. 31
For the studies using nationally representative surveys, both weighted population estimates and unweighted sample size are reported when available. An asterisk * indicates the weighted population estimates were not reported (NR).
Health and Medical Care Tasks
Out of the 12 included studies, 10 reported caregivers’ involvement in health and medical care tasks.5,27-29,31-36 Medication management (including keeping track of medicines and giving shots/injections) was the most common health and medical care task. In 7 of the 12 included studies, medication management was performed by approximately 52% to 86% of caregivers.5,27,28,30,34-36 Qualitative evidence from Travis et al highlighted the clinical complexity of medication management, including logistical, procedural, and safety-related challenges experienced by caregivers. 36 Skin and wound care was the second most common task performed by informal dementia caregivers, as reported in 4 studies performed by 18% to 47% of caregivers.5,28,33,35 Amjad et al reported that about 82% of caregivers were involved in medication management or assistance, skin/wound/dressing care, and administration of injections. 28 Caregivers also helped manage medical devices and equipment. Reinhard et al reported about 44% of caregivers helped PLWDs with assistive devices for mobility (canes or walkers), about 32% of caregivers used medical equipment such as meters or monitors, and about 31% of caregivers used incontinence equipment, supplies, and administering enemas. 35 Furthermore, about 10% to 21% of caregivers also operated durable medical equipment (hospital beds, wheelchairs, etc.) and other medical equipment (mechanical ventilators, home dialysis equipment, etc.). 35 Two studies reported ostomy care as 1 of the tasks performed by caregivers.33,35 One study using the 2017 NSOC time diary data reported that caregivers spent about 34 min a day providing physical and medical care to PLWDs on average. 31
Advocacy and Care Coordination
Two studies reported caregivers’ involvement in advocacy and care coordination tasks.5,37 One study reported an approximately equivalent percentage of caregivers involved in various advocacy and care coordination tasks for PLWDs with substantial disability compared to those without. 5 The tasks involved in both the studies were making appointments (73.3%-79%), managing, changing or handling other insurance matters (20.4%-26.9%), and speaking with medical providers (67.5%-82.2%).5,37 Other tasks reported by Li et al were getting online for telehealth visits (8.5%), sitting in on doctor appointments (68.4%), helping with an overnight hospital stay (44.2%), checking online medical accounts (42.9%), and coordinating care (63.0%). 37 Caregivers in one of the qualitative studies described certain system navigation challenges such as managing insurance and service coverage, coordinating care, and overcoming communication barriers within the health care system. 29
Surrogate Tasks
Ohno et al reported that 32% of caregivers were mainly responsible for their care recipient’s treatment decisions and nursing home placement. 32 We did not find any study with caregivers involved in advance care planning.
Quality Assessment
Of the 9 criteria listed in the JBI quality assessment tool, the number of criteria met in the included studies ranged from 7 to 9, indicating overall high quality, which enhances confidence in the reliability of this review’s findings.5,27-37 All the studies (100%) fulfilled Criterion No. 4, “Were the study subjects and the setting described in detail?,” and 91.6% fulfilled Criterion No. 7, “Was the condition measured in a standard, reliable way for all participants?.”5,27-37 The detailed scoring of each study using the JBI appraisal tool can be found in Supplemental Table S4.
Discussion
This study reviewed and summarized research examining informal dementia caregivers’ involvement with health care-related tasks other than ADLs and IADLs. Among health and medical care tasks, medication management was the most commonly reported. This finding is consistent with prior literature.5,18 We also found that skin/wound care was informal caregivers’ second most commonly reported health and medical care task. However, the literature on the challenges faced by family caregivers providing wound care is rather scarce, 38 and warrants future research. 5
Only 2 studies reported informal dementia caregivers’ assistance in advocacy and care coordination tasks, including making and sitting on doctor appointments, talking with the health care providers, managing health insurance, helping with overnight stays in the hospital, navigating online medical accounts of the care recipients, and managing telehealth visits.5,37 The US health care system is fragmented and difficult to navigate for patients and their families. 39 These difficulties arise as dementia care requires interacting with multiple providers from various disciplines, including primary care physicians, geriatricians, neurologists, psychologists, and occupational therapists. 2 A recent Alzheimer’s Association survey reported that 53% of caregivers found it difficult to navigate the health care system, 70% found it stressful to coordinate care, and more than two-thirds found it challenging to find resources related to providing care. 2 A study included in our review also reported that caregivers found it most difficult to transition after hospital stay, followed by coordinating care, and handling insurance. 37 Another study noted that 32% of caregivers would like assistance navigating various insurance options. 2
Caregivers are often responsible for surrogate decision-making (including financial and legal matters and treatment decisions).40-42 A qualitative study reported various legal and financial challenges faced by dementia caregivers who performed surrogate tasks. Caregivers reported difficulty paying for dementia care, understanding multiple financial procedures, and finding reliable professionals to seek guidance in the financial aspects of dementia. 43 Caregivers also faced challenges in legal matters, such as setting up a medical and financial power of attorney and difficulties in finding elder law attorneys. 43 Surrogate decision-makers often face confusion, lack of confidence, uncertainty, and a substantial burden when making decisions for PLWDs.44-47 Moreover, ethical and emotional considerations are introduced in surrogate decision-making tasks if the preferences of PLWDs are not known. 48
A critical gap in the literature is that only 5 studies in our review reported on racial and ethnic minority caregivers. Previous research has highlighted the importance of including racially and ethnically diverse groups of dementia caregivers to better understand the distinctive requirements, challenges, and capabilities of racial and ethnic minority family caregivers in the US. 49 Lack of understanding of the unmet needs of various racially and ethnically diverse subgroups may also lead to underutilization of various support services (such as respite care and support groups) in marginalized populations.49,50 This underrepresentation also limits the generalizability of findings and poses risks of overlooking culturally specific caregiving practices, health beliefs, and access barriers. Strategies to ensure a racially and ethnically diverse population in caregiving research could be incorporated in the future, such as using the National Institute on Aging Health Disparities Research Framework as the guide. 51
Our review indicated that some health care-related tasks were more commonly performed than other tasks, corroborating the shifting of care responsibility from health systems to family caregivers described in the Home Alone Revisited report. 4 Given the challenges caregivers face and their need for training in performing these tasks,2,18 health systems and community-based organizations should recognize the complexity of caregiving and should provide caregiver training. In fact, dementia caregivers would like to receive training. 18 However, only 1 study in this review mentioned receiving training from health professionals. Recently, the CMS added 3 new Current Procedural Terminology (CPT®) codes (97550-97552) for health care professionals to train caregivers in behavioral management and ADLs. 52 Moreover, the Alzheimer’s Association formed the Dementia Care Navigation Roundtable to share best practices and resources in dementia care navigation programs. 53 In summary, there have been increasing efforts to support informal dementia caregivers in the care continuum. Still, more future work is needed, such as ensuring minoritized populations have access to support services and programs and identifying barriers to providing them.
This review has several strengths beyond summarizing literature. First, it highlights that informal caregivers are commonly involved in performing complex health care-related tasks that extend beyond ADLs and IADLs, which reflects their expanded role in dementia care. Second, the substantial variability in how these health care-related tasks are defined and measured reveals a critical need for a standardized measurement framework to enable a streamlined approach and to provide resources and training to caregivers. Third, the limited reporting of caregiver characteristics, particularly employment status, rural or urban status, race and ethnicity information, training needs, and caregiving intensity, highlights gaps that limit the understanding of what types of caregivers are most affected and what support they need. Qualitative evidence from our included studies further suggests that caregiver experiences are shaped by factors not consistently captured in quantitative studies, including the clinical complexity of tasks, the system-navigation burden, and caregiver capacity.29,36 To contextualize these findings, a conceptual framework can be useful, which includes the caregiver profile (eg, demographics, clinical profile, and resources available), the task profile (eg, caregiving intensity and clinical complexity of health care-related tasks), and components of the GUIDE model. This framework will highlight that caregiver burden and outcomes are influenced not only by who the caregivers are, but also by the demands and complexity of the tasks they perform. Moreover, our findings are particularly important for the GUIDE model as it aims to reduce caregiver burden. Caregiver workload, preparedness, and access to resources cannot be fully understood without adequate definitions and incomplete measurement approaches, which can limit the effectiveness of policy interventions. Future studies should more comprehensively incorporate measures of caregiver intensity, clinical complexity, system navigation burden, and caregiver capacity to inform tailored support strategies to caregivers. Collectively, this synthesis clarifies the key knowledge gaps and emphasizes the importance of developing robust, standardized measures that capture the scope, complexity, and diversity of health care-related caregiving activities.
This study has several limitations. First, conducting a formal meta-analysis of results was not feasible because health care-related tasks were not defined consistently in the literature. Second, we adopted our classification of health care-related tasks from the Families Caring for an Aging America report. There is no comprehensive measure to capture the multidimensional nature of caregiving or the burden or effort involved with each task. Future research should also include the complexity of the caregiving tasks and caregiving trajectory. 4 Future studies should consider using a mixed-methods design to capture both quantitative and qualitative aspects of diverse caregivers’ experiences and develop a comprehensive list of health care-related caregiving tasks. Third, due to the heterogeneity in study design, populations, and definitions of health and medical care tasks across the included studies, formal comparisons of prevalence were not possible. Thus, these findings should be interpreted as descriptive patterns rather than definitive prevalence estimates. Fourth, although we used the Families Caring for an Aging America report to classify health care-related tasks, some tasks, such as sitting in on doctor’s appointments, do not fit neatly into a single category. For example, sitting in on doctor’s appointments could be both, an advocacy and care coordination task and a surrogate task, as caregivers often participate in shared decision making. 37 To prevent duplication, we assigned each task to 1 primary category. This issue reflects challenges in operationalizing and measuring caregivers’ involvement in health care-related tasks and warrants future research. Finally, we used the JBI Critical Appraisal Checklist for Prevalence Studies to assess the qualitative studies included in this review, as several of the included studies reported caregiver counts or proportions relevant to our objective of describing caregiving patterns. As this checklist is primarily for quantitative prevalence studies, it may not fully capture methodological rigor specific to qualitative research. Using this checklist may have limited our ability to comprehensively assess the risk of bias across all study designs.
Conclusion
This review highlights the critical role of informal dementia caregivers in performing health care-related tasks for PLWDs. We found that medication management was the most prevalent health and medical care task, followed by skin and wound care. Overall, informal caregivers’ assistance with medication management dominates the literature, and we call for more research on other health care-related tasks such as skin and wound care, advocacy and care coordination, and surrogate tasks. Particularly since the GUIDE Model aims to support care coordination. Moreover, as few studies have reported on more clinically complex health care-related tasks such as managing medical devices and equipment, using monitors or meters, and providing ostomy care, further exploration of these tasks is needed. Last but not least, our study revealed a lack of racially and ethnically diverse caregivers in the included studies. It is critical to include minoritized informal caregivers in research to provide a more complete picture of caregiving and ensure their voices are included in intervention and policy development.
Supplemental Material
sj-docx-1-inq-10.1177_00469580261438330 – Supplemental material for Health Care-Related Tasks of Informal Dementia Caregivers in the U.S.: A Systematic Review with Narrative Synthesis
Supplemental material, sj-docx-1-inq-10.1177_00469580261438330 for Health Care-Related Tasks of Informal Dementia Caregivers in the U.S.: A Systematic Review with Narrative Synthesis by Mohammed Zuber, Samruddhi Nandkumar Borate, Chia Jie Tan and Niying Li in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Author Note
An earlier version of the abstract has been presented at the Gerontological Society of America Annual Scientific Meeting in November 2024.
Author Contributions
Niying Li: Conceptualization, Methodology, Validation, Writing – Review & Editing, Supervision, Project administration. Mohammed Zuber: Investigation, Data curation, Visualization, Writing – Original Draft. Samruddhi Nandkumar Borate: Investigation, Data curation, Visualization, Writing – Original Draft. Chia Jie Tan: Methodology, Validation, Writing – Review & Editing, Supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data generated and analyzed in this study are part of the publication and Supplemental Materials.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.