
Abstract
Refugees, or humanitarian migrants, often experience profound health disadvantages stemming from disrupted healthcare access, interrupted education, and systemic barriers to integration. For the Yazidi community resettled in Toowoomba, Queensland, these challenges are compounded by trauma and limited support systems. This study, part of a broader community-based project, explores the multi-layered factors shaping their health and wellbeing, with the aim of informing culturally responsive and sustainable support strategies. Utilising a qualitative design, we conducted semi-structured interviews (n = 23) and focus groups (n = 24) with service stakeholders and Yazidi community members. Hybrid inductive-deductive thematic analysis of transcripts was informed by the PRECEDE-PROCEED model, enabling the categorisation of health determinants into predisposing, enabling, and reinforcing factors relevant to health planning and evaluation. Five interrelated themes emerged: mental health and trauma, social integration, health literacy, language proficiency, and access to sustained funding and resources. This study illuminates the lived experiences and health needs of a high-burden refugee community in regional Australia. Findings underscore the importance of trauma-informed care, culturally tailored health education, language services, and gender-sensitive psychosocial support. The resilience demonstrated by the Yazidi community offers a foundation for designing inclusive, community-driven health interventions. These insights are critical for professionals seeking to address health disparities and promote equity.
Keywords
Introduction
Due to the escalating effects of climate change, protracted conflicts, and armed warfare, global resettlement needs are projected to reach 2.5 million in 2026, with an increasing number of international refugee populations.1,2 In recent years, Australia has responded with a substantial increase in humanitarian resettlement, particularly in regional areas.3 -5 How to effectively resettle refugees while ensuring their health and wellbeing has become an urgent public health challenge and humanitarian concern. Toowoomba, a regional city in Southeast Queensland, designated as a Refugee Welcome Zone, 6 has become a primary site for Yazidi resettlement, which now represents the largest refugee group in the region. 7
Yazidi, also spelt as Yezidi or Ezidi, is an ethnic and religious minority geographically native to the Kurdistan region. 8 They have faced repeated systemic persecutions, culminating in the 2014 genocide in Northern Iraq. This tragic event led to thousands of people being killed and thousands of women and children being enslaved, driving 350,000 Yazidis into refugee camps.9,10 The experience of trauma and displacement, combined with disrupted access to education and healthcare,11 -16 has resulted in elevated risks for mental illness, chronic disease, and social marginalisation.17 -25 These risks are further exacerbated by post-resettlement challenges, including language barriers, limited health system knowledge, and difficult social integration.26 -31 However, limited studies explicitly assess the specific needs, health factors and determinants, and overall wellbeing of this community, with few studies focusing on social determinants relevant to effective health planning.32 -34
Refugee communities resettled in rural and regional areas often face more complex health needs due to the unique sociocultural backgrounds and the resource limitations. Yet, Toowoomba lacks studies understanding the social determinants and structural constraints—including the regional setting—that shaped the Yazidi community’s health and wellbeing to inform health planning. Additionally, this community is far from homogeneous, adding further complexity to health management. Subtle differences in language, culture and religious belief between members from Iraq and members from Syria have created challenges in establishing unified community leadership and representation.
Guided by the PRECEDE-PROCEED model (PPM model),35 -38 this study aims to assess health determinants and identify key predisposing, enabling, and reinforcing factors that are most likely lead to behavior changes, essential for effective program planning. The PPM model was selected as a sensitising framework for its proven utility in diagnosing multi-layered health determinants of the disadvantaged population. 33 It enables the interpretation of complex health determinants into actionable factors of program design, which aligns with constructivist paradigms of qualitative refugee studies.39,40
This study provides detailed insight into how interacting social determinants shape the health and wellbeing of refugee-background people following resettlement in a regional Australian city. The findings reveal interactions of individual experiences with broader institutional and systemic dynamics. It offers insights into the behavioral and structural dimensions of refugee health, and informs the development of equitable, community-informed health interventions.
Method
Study Design
This exploratory study employed a constructivist qualitative inquiry approach, which asserts that realities are co-constructed between participants and researchers.41,42 Incorporating participatory methods,43 -45 that ensure active community participation, the method emphasised researcher reflexivity and community empowerment, while capturing the nuanced perspectives of both community members and service stakeholders. Semi-structured in-depth interviews and focus group discussions were conducted. Interview and focus group questions were designed in consultation with Yazidi bicultural support workers. Two bicultural support workers were invited to pilot test the interview and focus group questions.
Participants Recruitment
The study sample included Yazidi refugees and stakeholders working directly with the Yazidi community. Kurdish Kurmanji is the primary language spoken among Yazidis, with many community members experiencing limited English proficiency and low literacy. To accommodate these linguistic and cultural considerations, stakeholders were engaged through one-on-one interviews, while Yazidi participants were primarily involved via focus groups facilitated by bicultural support workers. This arrangement is confirmed in considerations of the cultural appropriateness, as the Yazidi participants tend to feel more comfortable in a group setting.
Interview participants were recruited using purposive sampling followed by snowball sampling to deliberately select information-rich participants and leveraged their networks to access members of this hard-to-reach population.46,47 Initial participants—identified by the authors based on direct experience working with the Yazidi community, English fluency, relevant health and wellbeing expertise, and audio-recorded interview willingness—were invited to refer others meeting these criteria. The purposive sampling ensured relevance and depth while snowballing expanded reach and scope, suitable for recruiting multidisciplinary information-rich participants. Participants are encouraged to refer workers and community members from multiple disciplines to maximise representation. Potential participants without direct working experience with the Yazidi community and those unable to communicate independently in English were excluded from interviews. Recruitment ceased at information saturation.
A total of 23 participants were recruited for interviews, including psychologists, health and social services workers, bicultural workers, schoolteachers, and volunteers—4 of whom had refugee lived experience. Data saturation was achieved for interviews.
Focus group participants were recruited using convenience sampling, with support from bicultural community workers. Convenience sampling was employed to prioritise practicality within in time and resource constraints and the absence of population frame for this community. Participants were selected through established networks of trusted community workers, specifically those already engaged with community services and networks with high levels of participation comfort. Sample size was pre-determined for focus groups (4-8 members for each group) to allow an approximate even contribution across sub-populations.
Four focus groups were conducted, structured by gender and age to reflect cultural norms and ensure participant comfort:
(1) Adult male group (18+ years).
(2) Adult female group (18+ years).
(3) Youth male group (15-24 years).
(4) Youth female group (15-24 years).
Each participant joined only 1 group. Individuals whose cognitive conditions could significantly affect communication with the researcher, and those who did not identify as having a Yazidi refugee background, were not invited to participate in the focus groups. Bicultural workers provided language interpretation and cultural support, with a female facilitator assisting the adult female group and a male facilitator supporting the remaining groups, upholding cultural appropriateness. A total of 24 Yazidi participants were recruited for the focus groups. Data saturation was achieved for the focus groups.
Demographic details of the participants can be found in the Supplemental Appendix.
Data Collection Procedure
All interviews and focus groups were conducted by the first author. Interview participants were provided with discussion prompts covering:
(1) Cultural and professional background.
(2) Health needs of the Yazidi community.
(3) Barriers and facilitators to health.
(4) Challenges in service provision.
(5) Resources and support needed.
Focus group discussions explored:
(1) Common health concerns.
(2) Resettlement challenges.
(3) Likes and dislikes about local services and the area.
(4) Recommendations for new arrivals.
A vignette approach was used in focus groups to present hypothetical scenarios and encourage discussion. Participants responded in a round-robin format, with experienced bicultural workers translating responses. The researcher then repeated the responses, and bicultural workers interpreted them back to the participants to confirm their meaning. When encountering culturally specific concepts and idioms, bicultural support workers explained these terms in plain language to ensure clear understanding by both participants and the researcher. Participants were fully informed about the research and data collection procedure.
Data Management and Analysis
All sessions were audio recorded using dual devices to ensure quality and accuracy. During focus groups, speech was captured both in the original language and the interpreted English. Transcripts were generated using Microsoft Teams and manually reviewed and edited by the first author to ensure completeness and validity.
Hybrid inductive-deductive thematic analysis was conducted following Braun and Clarke’s (2006) established steps. 48 Data were initially coded inductively, after health factor themes emerged, they were mapped to predisposing, enabling, and reinforcing factors, as guided by the PPM model. 37 NVivo 14 was used to support data management and coding.
Throughout the analysis, the research team engaged in reflexive practice to consider assumptions, positionality, and potential influences on interpretation. To enhance trustworthiness of the results, community members and frontline workers were invited to review the analytic approach and preliminary findings, providing feedback that strengthened the coherence and credibility of the analysis. 49 The impact of social integration was further highlighted after community review of the findings and emerged as a key theme.
Positionality Statement
All authors do not have lived experience of being a Yazidi refugee or of Yazidi ethnicity. The first author and 2 of the co-authors are Public Health researchers external to Toowoomba community, while the remaining 2 co-authors are frontline resettlement workers who have daily engagement with the community.
To manage inherent power dynamics, the research team prioritised prolonged relationship-building with trusted bicultural support workers and community members before data collection, and co-designed research process with community input to promote equitable dialogue and participant comfort. Regular consultation with the community members, bicultural workers, and frontline workers enabled ongoing reflection on researcher influence and methodological adjustments to mitigate power imbalances and research bias. 50
Ethical Considerations
The ethical conduct of this study was evaluated and approved by Griffith Human Research Ethics Committee (No. 2024/481). Decisions were guided by the UNHCR Ethical Communication Guidelines, including principles of doing no harm, ensuring dignified representation, challenging stereotypes, amplifying refugee voices, and upholding informed consent and accountability. 51
Written informed consent was obtained from all interview participants prior to the commencement of the sessions. Informed oral consent was obtained from all focus group participants due to linguistic barriers, and to avoid participant fatigue on documentations. For participants under 18-year-old, parental or guardian consent was secured. These practices complied with ethical requirements.
Trauma-informed practice was incorporated through providing support pathway, managing distress, maximising participants comfort, and sensitivity consultation with community advisors. Confidentiality may be limited within in a small community, but rigorous ethical practice was maintained through de-identified data and quotations, aggregated reporting, and secure storage compliant with ethical approvals.
Overlapping Work
An additional paper may be developed from the same dataset, as the research identified critical health concerns that require separate discussion. However, this potential work has not yet been submitted or published.
Results
Stakeholders consistently emphasised that the Yazidi community presents more complex and intensive needs than other refugee groups in the region. As one social worker noted:
There is definitely heightened need, really much more significant needs in a lot of cases within the Yazidi community. —Social Worker
Participants reported widespread mental health concerns, alongside diabetes, hypertension, chronic pain, and additional challenges about limited formal education experience, dental health, domestic violence support, and transportation access. Multiple intercorrelated factors collectively affect the health management behavior and wellbeing of the Yazidi community.
Five interrelated themes were constructed through thematic analysis. These themes are organised into the health factors defined in Phase 3 of the PPM model—predisposing, enabling, and reinforcing factors—reflecting to multi-layered determinants of effective health program planning. These themes are illustrated in Table 1 and Figure 1.
Summary of Main Themes.
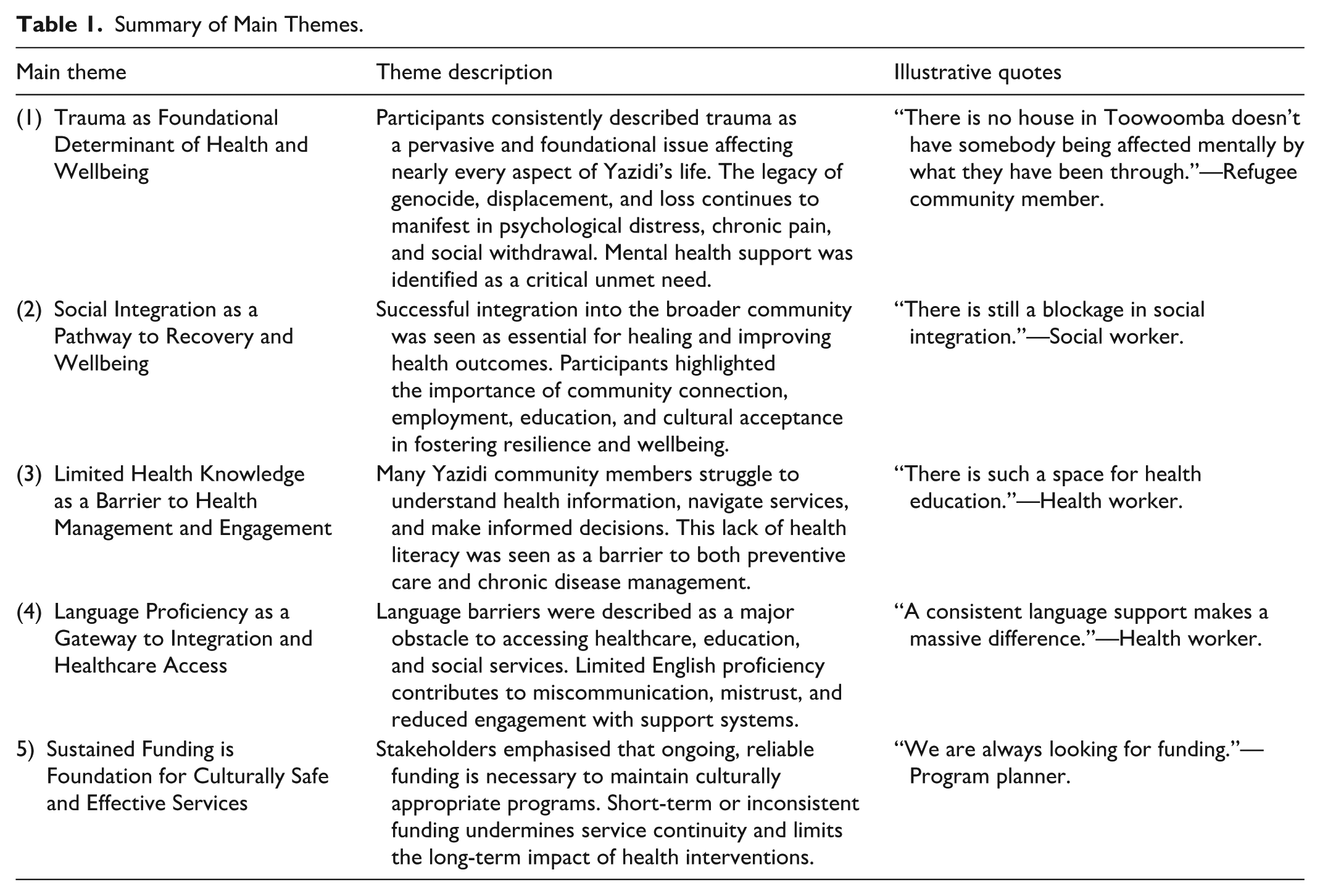
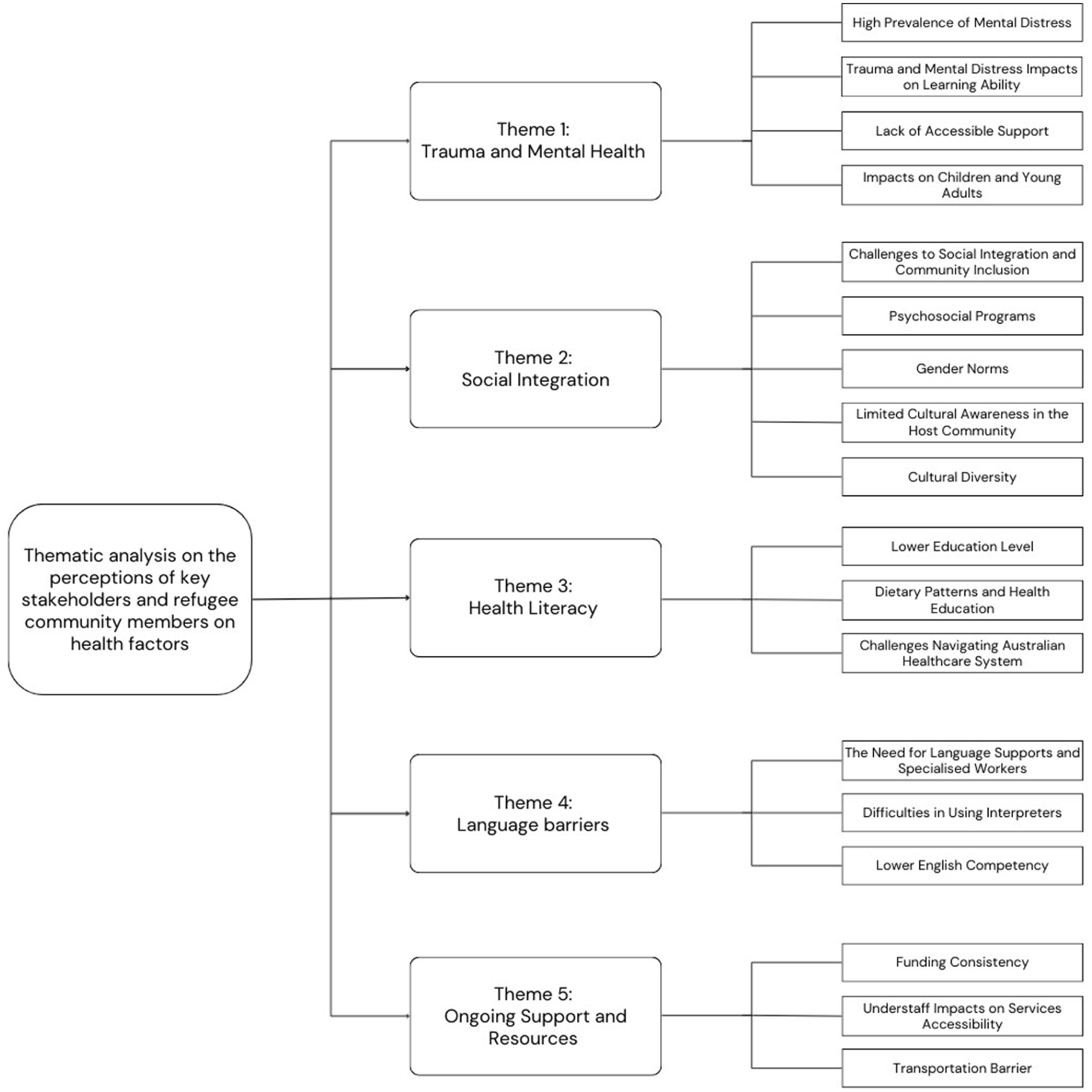
Key themes and subthemes on the factors impacting health and wellbeing of the local Yazidi refugee community.
THEME 1: Trauma as Foundational Determinant of Health and Wellbeing
Trauma, or mental health, was identified as the most prioritised health determinant for the Yazidi community. It is classified as a predisposing factor, internal characteristics that motivate behavior changes, forms the cornerstone of successful behavior changes and program planning.
Enduring Pervasive Mental Distress
Enduring mental distress and trauma from the legacy of the genocide, pervasive PTSD, depression, anxiety, and somatic symptoms are common across the Yazidi community. Participants emphasised that mental health is foundational in health management.
We all need mental health support in the beginning to be continued correctly with healthier body, or you can’t do any change in your life. —Refugee community member.
This underscores trauma as the key predisposing factor. Pervasive mental distress further highlights the pressing need for accessible mental health support, yet the long waiting list of affordable consultation services revealed significant service gaps. This finding suggests the need for sustained trauma-informed program planning.
Cognitive and Emotional Impacts on Learning and Adaptation
Trauma-related distress impairs memory, concentration, and learning capacity, leading to overwhelming feelings for the new arrivals toward the complex health system information. The stress of adapting to a new environment further compounded these difficulties.
Imagine the amount of information you received when you first come here, it is overwhelming, and scary even! —Refugee community member.
Some stakeholders emphasised the need for repeated reinforcement of key information and consistent messaging across service providers and consultation appointments to reduce confusion and improve engagement. However, providing translated written information remains a major challenge, as illiteracy is common within this group.
This finding implies the difficulty in processing information for the new arrivals and further emphasised the gaps that remain in trauma-informed programs in response to this predisposing factor.
Barriers to Accessing Mental Health Support
Despite the high demand, access to mental health care remains limited and is often unaffordable. The Queensland Program of Assistance to Survivors of Torture and Trauma (QPASTT) was identified as the most accessible provider, yet long waitlists and resource constraints mean that only those with acute needs are prioritized, despite specialists working at their maximum capacity. Others are left with few options—either to wait, pay out-of-pocket, or seek care overseas:
She was quite unwell, in a lot of pain. But the waitlist to see a psychologist here is too long. We have to pay a lot for a private psychologist and extra for interpreter, after a couple of sessions, we can’t afford it. Then we have to send her back to Iraq to get some treatments there. —Refugee community member.
The financial barriers also reflect systemic constraints in resources and affordable services, revealing policy and service gaps in the regional setting that fail to match the sustained mental health needs of the Yazidi community.
Stakeholders believe that early-stage supplementary community-based psychosocial programs can mitigate the service access barriers and often yield better outcomes:
Those not involved in any early psychosocial programs become more isolated, anxious and fall into a deep slope of depression, and the climb back up is a steep one. —Stakeholders.
Local low-cost psychosocial programs, including Pilates for women, art therapy, weekly sewing groups, sports programs, and social groups, aim to foster mental wellbeing through positive social connection and provide effective coping strategies for cultural shock and associated depression.
The programs have higher participant engagement compared to conventional one-to-one consultation therapy. While some show promising outcomes, their sustainability remains a challenge due to inconsistent funding.
Intergenerational Impacts on Children and Youth
Trauma affects children and young adults through either direct experience of violence or indirect absorption from family members. These effects have manifested as challenges in trust-building, emotional dysregulation, learning difficulties, and premature caregiving roles among school-aged children and young adults.
. . . they’ve experienced a lot of traumas in their house, and you see the adverse reaction they have in school, and they don’t know how to trust people. —School teacher. They take way more responsibility than what the average young adults at their age will take for their family. —Community worker.
This finding underscores the current gap in timely and inclusive specialised mental health and development support in school settings. Participants advocated for universal access to mental health care, regardless of diagnosis severity, as a foundational step toward enabling refugees to manage their health and rebuild their lives.
THEME 2: Social Integration as a Pathway to Recovery and Wellbeing
Social integration emerged as the next priority determinant, which is classified as a key enabling factor that provides access and capacity for practical help-seeking. It closely interacts with mental health, affecting access to essential supports and other social determinants such as employment. However, determinants relating to social integration, such as community supports, cultural norms, and social connection rewards, also act as reinforcing factors that sustain health management and program engagement.
Challenges to Social Integration and Community Inclusion
Social integration was widely recognised as a critical determinant of health and wellbeing among the participants. Multiple factors exacerbate challenges in the integration process, resulting in social isolation. These factors are commonly experienced as the limited and confusing public transportation, greater cultural and linguistic differences, and the lack of accessible services in regional areas. The ongoing housing crisis in Toowoomba further compounded these challenges, making it difficult to secure stable accommodation while matching expectations, hindering integration.
Social engagement in Toowoomba is hard. —Yazidi community member.
This difficulty in social engagement is commonly felt among Yazidi community members, which also revealed gaps in regional infrastructure to match the needs of the resettled community.
Psychosocial Programs as Bridges to Belonging
The traditional Yazidi community are close-knit and socially conservative. Some community members feel unmotivated or even scared to integrate with other communities without necessarily realising the health benefits associated with social integration. In response, program planners developed culturally relevant psychosocial programs to foster integration and wellbeing.
For example, the Hockey Program brings together refugees and migrants from diverse backgrounds through sport. Participants reported improvements in self-esteem, English language skills, and social confidence, which facilitate integration and employment by enhancing teamwork and interpersonal skills.
The aim for the sport program is to provide a safe space for people to get involved, raise self-esteem and peer-respect, improve language and attitude, increase integration, and introduce positive role models, as well as an active healthy lifestyle. —Stakeholder.
Despite its success, stakeholders noted that sustaining and upscaling such programs to reach more Yazidi refugees remains a challenge due to limited resources and funding.
Gender Norms and Unequal Access to Integration
Women were identified as the most marginalized subgroup within the Yazidi community, facing significant barriers to social integration through traditional gender roles emphasising domestic responsibilities and discouraging women from engaging in public life. Many women were reported as having limited opportunities to leave the house, learn English, or drive. As a result, they often rely on male family members for transportation and communication. This isolation may exacerbate trauma, hinder recovery, and limit access to health and social resources.
I can see the men are moving on, which is good. But the women are still living in the past. —Stakeholder.
The rising concerns of domestic violence reveal structural gender inequities and gaps in legal awareness among men and support awareness among women. Gender norms also influence attitudes of some younger males, reflected in their disrespect toward female supervisors, teachers, and peers.
Sometimes I think that the women can be very isolated, very easily. That’s what worries me the most . . . —Local resident.
Stakeholders emphasised the need for early education on gender equality and legal rights, particularly among youth and younger generations, to prevent further entrenchment of harmful gender norms. Program planners trialled the introduction of strong female role models in sports programs, which have shown early signs of shifting attitudes among male participants.
Cultural Awareness in the Host Community
Limited cultural awareness among the broader host community may hinder integration. While describing the city as amazingly welcoming and a group of people being very interested in providing support, some participants believed that many lack understanding of the Yazidi people’s history and their displacement experience, leading to xenophobia, ignorance, and feelings of exclusion among refugees.
I would say the majority of people do not even know that they are here. —Health worker.
This represents a reinforcing factor that limits the delivery of culturally appropriate practice across all sectors, which is vital for fostering connection and trust. For example, the community hubs embedded in local schools provide culturally safe spaces and opportunities for informal engagement, language learning, and cross-cultural understanding. Community members also expressed appreciation for the community hubs:
We like the community hubs. —Refugee community members.
Sustained program and policy efforts to promote culturally appropriate practices remain essential.
Valuing Cultural Diversity
Participants emphasised that successful integration is not only beneficial for refugees but also enriches the broader community. Cultural diversity was described as essential to a healthy and vibrant society:
Multiculture makes things better. —Stakeholder. In the garden, you want diversity to keep plants healthy, and the garden looks good, and human society is the same as a garden - diversity is needed. —Stakeholder.
THEME 3: Limited Health Knowledge as a Barrier to Health Management and Engagement
Besides trauma and mental health, another key predisposing factor identified is health knowledge, which is the internal readiness for effective health communication and health decision-making that directly impacts health program engagement.
Limited Educational Background and Foundational Health Knowledge
Having limited experience of formal education, because of previous rural isolation and disrupted education, is common among the Yazidi community members. The resulting lack of basic biological and health knowledge impedes both self-care and effective communication with healthcare providers, leading to frequent misunderstanding of symptoms:
What you and I would consider basic health knowledge, they don’t have that. We must really start (health education) from the beginning. —Health worker.
One frequently mentioned example was clients misinterpreting abdominal discomfort as kidney stones, but only to discover that it was constipation. This broader gap in foundational health education reflects a critical predisposing factor, meaning program design must prioritise health education. Some suggested education areas include anatomy, diet and nutrition, lifestyle changes, disease prevention, the healthcare system and roles, and appropriate use of emergency services.
Dietary Habits and Lifestyle-Related Health Risks
Unhealthy dietary patterns were common within the community, with an observed preference toward sugary beverages and processed foods. Some community members were unaware of the health benefits of drinking water and viewed sweetened drinks as more desirable. Shisha smoking was described as a normalised social activity, with limited awareness of its health risks.
There’s such a space for dietetics education. —Health workers.
These behaviors contribute to higher rates of diabetes, hypertension, and elevated blood lipid levels. The community’s restricted access to health education further undermines informed dietary decision making.
Navigating the Australian Healthcare System
Many Yazidi community members struggle to understand the structure and function of the Australian healthcare system. Participants reported confusion on help accessing pathways, the roles of health professionals, and when to use emergency services. Emergency departments were more frequently attended for non-urgent issues, resulting in longer waiting times and more frustration.
The presentations to emergency seem quite high for GP type issues. —Health worker.
Cultural expectations shaped clinical interactions as many Yazidi patients view doctors as authoritative figures, often expect clear instructions and medication at each visit. Some expressed anxiety or questioned the doctor’s expertise when given options or informed of the risks—an unfamiliar concept for them—affecting trust and compliance.
They believed the doctor is authority . . . the doctors should tell them what to do rather than giving them options. —Social worker. It is very scary when the doctors are talking about the risks of the treatments. Like, why are you telling me that? —Community member.
This finding suggests that different perceptions may heighten anxiety and mistrust toward health workers, which hinders effective health management and service engagement.
Limited health knowledge also fosters other health misconceptions—such as the excessive care for vulnerable individuals with disabilities, which hinders their independence—and the over-reliance on health professionals. Many individuals lacked motivation for healthier lifestyles or preventative health management. Instead, they relied on medical interventions to address discomfort, reinforcing a cycle of dependency.
They’ve become the passive participants of their own health. —Social Worker
Participants agreed that improving health literacy is essential for fostering autonomy and enabling healthy behavior changes that promote long-term wellbeing. Health education is critical for health program planning and a necessary step toward community empowerment.
THEME 4: Language Proficiency as a Gateway to Integration and Healthcare Access
Language proficiency also presents as a key enabling factor, which is a critical skill that makes services more accessible and facilitates positive health management through addressing other factors, like social integration.
The Central Role of Language Support and Specialized Workers
Kurdish Kurmanji, the primary language spoken by the Yazidi community, is the second most spoken language in Toowoomba after English. 7 However, many Yazidi individuals speak Kurdish Kurmanji orally but lack literacy in both Kurdish Kurmanji and English, creating significant communication barriers.
The daily need for interpreters and specialised language support staff in clinics, schools, and community services is evident, highlighting the importance of sustained language support:
A consistent language support makes a massive difference. —Health worker.
Difficulties with Interpreter Services
Phone interpreters, commonly used in healthcare settings, were described as inflexible and difficult to rebook when appointments were delayed. Concerns were also raised about their inability to convey non-verbal cues and body language.
Phone interpreters are just difficult to use. —Health worker.
Additionally, some health terms—such as “anxiety” and many organs —lack direct equivalents in Kurdish Kurmanji, complicating accurate translation. Confidentiality was another concern, as interpreters often came from within the Yazidi community, raising fears about the potential spread of sensitive information. These challenges underline the need for trusted in-person interpreters and sustained language proficiency programs.
Nevertheless, the community’s strong internal communication networks act as an enabling factor. Once a program or service is perceived as beneficial, word-of-mouth advocacy often leads to increased participation, upscaling program engagement.
Lower English Proficiency and Social Mobility
Community members viewed English proficiency as essential for integration, education, employment, and independence.
When I came to Toowoomba, I didn’t know English language, so that was hard for me. I used to get learning and now it’s better. —Refugee community member.
While free language programs were offered, pre-arrival language training and alternative learning formats—such as conversational English and activity-based learning—were considered better suited than traditional classroom-style learning, particularly for those with limited formal education experience or constrained learning capacity, like the older individuals.
Low English competency was a barrier to program participation, where safe and effective program delivery became impossible.
Some volunteer instructors have to withdraw from the driving program as they cannot give instructions safely because of the language barriers. —Program manager.
This finding again highlighted the importance of improving community language proficiency and recruiting trusted bilingual community workers for program sustainability.
THEME 5: Sustained Funding is Foundation for Culturally Safe and Effective Services
Sustained funding and resources are critical for health program planning. It can act as both an enabling factor, which makes programs and services possible, and a strong reinforcing factor, which sustains positive health management behavior through continuous engagement.
Funding Instability and Program Disruption
Participants expressed concern over the lack of sustained funding for refugee support programs. Many initiatives addressing the complex needs of the Yazidi community have been paused or discontinued due to resource constraints.
The funding we have is not continuous, we don’t know what to do for the next period if no more fundings. —Program manager.
This instability undermines long-term program planning and the continuity of care.
Staffing Shortage and Service Accessibility
Funding limitations created staffing shortages in essential language support, health education, employment services, and cultural liaison roles. For healthcare services, the lack of bulk-billing allied health providers has made some services more unaffordable, exacerbating access barriers. Sufficient funding could however resolve healthcare gaps and improve accessibility. For example, securing funding from Primary Health Network, Toowoomba community benefited from a dedicated Refugee Health Officer role that ensured sufficient local GP access for refugee-background patients, a success many resettlement cities have failed to achieve.
. . . to solve lack of staff, we need more funding. We’ll need more funding throughout these very essential programs. —Program manager.
The policy gaps in sustainable funding and services directly contributed to environmental barriers to health management and confirmed the need for systemic interventions to strengthen health equity.
Transportation as a Structural Barrier
Transportation was a major barrier to program participation, reflected by infrequent public transport in the regional setting and limited access to private vehicles. Marginalised individuals, like women and the elderly, rely on family or friends for transportation. Language barriers and unfamiliarity with traffic rules further limit the number of licensed drivers within the community.
Participants emphasised that transportation support, which requires ongoing funding inputs on organisation vehicles and support, must be embedded into program design to ensure safety and accessibility:
You need transportation for them to come. —Program Planner.
Sustained funding is required for service delivery, adequate staffing, and culturally safe infrastructure, essential to support program implementation and behavior changes toward better health and wellbeing. Without these resources, programs risk becoming fragmented and ineffective.
Discussion
The findings revealed a constellation of challenges, including high rates of mental distress, chronic disease, smoking behaviors, language and transportation barriers, cultural dissonance, and limited employment opportunities. These issues are shaped by intersecting determinants—trauma, social integration, health knowledge, language proficiency, and resource availability—which can be examined using the PPM framework, organising them into predisposing, enabling, and reinforcing factors. 37 These factors are identified in Phase 3 of the PPM framework, education and ecological diagnosis, which normally take place after social problems have been identified and interventions have been selected.35,37,38 Due to the complexity of the social and health issues of this community, various interventions are required to address them comprehensively. The early application of education and ecological diagnosis could move the focus beyond designing a single intervention and translate community voices into structural and modifiable elements that can inform future health planning and program evaluation.
Predisposing Factors
The first modifiable factor is the Predisposing Factor, which are individual-level or internal characteristics that could influence health behavior and decision-making. 38 For the Yazidi community, these characteristics are multi-layered and interrelated. Several determinants, like cultural norms, cognitive functioning, literacy, and interpersonal experience, all shaped their beliefs, values, and attitudes toward healthy behaviors and health management. The key determinants that form the foundation of these characteristics are trauma and health knowledge.
Trauma significantly impairs cognitive function, learning capacity, and emotional regulation, which also affects social interaction.52 -54 Regarding the Yazidi community, participants described the impact of trauma on memory and the ability to process new information. Trust-building challenges caused by interpersonal trauma also hinder service delivery and sustained engagement. This pattern is also found in other trauma-affected refugee and asylum seeker communities, where prevalent cognitive impairments predict higher rates of disability and interpersonal trust continues to erode following resettlement, further complicating health needs and service delivery.55,56 Previous trauma treatment attempts trialled diverse evidence- based approaches, including Cognitive Behavior Therapy, Stabilisation Interventions, Narrative Exposure Therapy (NET), and Eye-Movement Desensitisation and Reprocessing (EMDR).57,58 But the effectiveness of these Western approaches for the refugee communities is controversial.57,58 Gentler approaches, adopting trauma-informed practices and emphasising positive social connection, may better address the community’s trauma and mental health needs, as evidenced by the improved mental health outcomes among community-based program participants.
The other key modifiable predisposing factor is health knowledge, shaping how community members perceive health symptoms and professional advice, and has emerged as a foundational barrier to effective health management.59 -61 The limited health knowledge commonly observed within the Yazidi community is contributed to by community cultural norms, disrupted education trajectories, and systemic barriers to access higher education.62,63 Post-resettlement challenges, including school disparities and social discrimination, further undermine education access. The marginalised subgroups with limited autonomy, such as women,64,65 are disproportionally affected.
Refugee-focused health literacy interventions have shown overall positive outcomes, but their efficacy and outcome sustainability remain uncertain. 27 Additionally, most studies were in metropolitan settings, adding further uncertainty about their feasibility in regional settings with additional constraints in education resources. 27 Addressing the health knowledge needs of the Yazidi community, and thereby improving service accessibility, would require tailored approaches. As health workers reported better engagement with short, integrated health information rather than lengthy, dedicated education sessions, embedding brief health messages across community-based programs would be more feasible and acceptable. Messaging featuring diverse media formats, bilingual health navigators and community health advisors can be considered, given their evident effectiveness among refugee populations. 66 These messages should include basic biological knowledge and practical advice grounded in daily activities, such as drinking water and healthy snacking.
Enabling Factors
The Enabling Factors come from the environment, which are related to the skills and resources required to motivate and attain health behaviors. 35 The help-seeking ability of the Yazidi community is largely affected by their English proficiency and social integration level. Resources available for local programs also determine whether systemic barriers, like the transportation barriers, can be overcome.
Language barriers impede service access and health communication, sometimes causing greater challenges than health literacy. 67 This can be addressed by upscaling refugee language training programs or enhancing access to trained interpreters and bicultural support workers. Nevertheless, language training outcomes vary by age and learning capacity, which also requires substantial time commitment. Therefore, prioritising bicultural and interpretation supports may be more feasible to resolve the pressing communication barriers of health planning and delivery. While they do not fully replace interpreters, the integration of bilingual and bicultural support workers into community-based services evidently better improves the feasibility to overcome language barriers. 68 They provide cultural supports and facilitate positive social connections with the community, benefits beyond language interpretation. 69 This suggests the importance of incorporating bicultural support workers, ideally both male and female, to ensure gender-appropriate cultural alignment, into all health planning. The positive social connections facilitated by bicultural workers are also beneficial for social integration.
Social integration is a critical yet difficult-to-address enabling factor that influences health management and quality of life. Challenges associated with social integration are common among refugee communities,70 -74 yet are intensified in regional settings by significant transportation barriers and limited employment opportunities.63,73,75 Addressing social integration in the regional setting requires multi-level actions, including sustained resettlement services, strong community networks, and targeted integration policies, alongside investments to improve public transport infrastructure and safe transportation provided by community-based health programs.76 -78 The importance of cultural competency is further highlighted in addressing social integration difficulties and loneliness. 77
Patients and consumers feel safer in a culturally appropriate environment and are more likely to engage.79,80 This was evident among the Yazidi community members, who appreciated the culturally competent community hubs, providing informal support and fostering trust. This finding highlights the importance of cultural competency training for all health services and community-based program staff. Organisational level competency is also essential, encompassing facilitating policies, training protocols, and collective attitudes across the healthcare system. 81 Program planners should co-design staff training protocols in consultation with bicultural workers and community members, incorporating training in cultural awareness and trauma-informed practice.82,83
Reinforcing Factors
Reinforcing Factors are the mechanisms that influence the continuation or modification of health behaviors. 38 While social integration often acts as a reinforcing factor across refugee communities, 77 the sustained resources and funding are the stronger reinforcing factors to the Yazidi community, affecting the continuation of programs and therefore community engagement.
Participants identified multiple community-based programs that were chronically underfunded with only short-term grants. Consequently, program planners continuously sought funding to ensure program continuity. Some initiatives, such as the art therapy workshops, had to be paused if no suitable funding was available. Unlike major cities, regional areas often faced amplified resource shortages due to less stable support and greater needs. 73 For example, longer distances to services and community centres, combined with less frequent public transport in regional cities, have increased the need for dedicated program transportation. Yet, there are no matching funds for vehicles accessible to program staff, nor are there resources to upscale community driving programs. Moreover, primary health workers have previously reported workforce and resource shortages in regional resettlement areas,31,84 further challenging the delivery of culturally competent practices. These findings highlight the existing deficits in reinforcing factors, where inconsistent funding and resources fail to ensure the continuity of essential health services and programs. Thus, ensuring stable funding and facilitating policies is critical for competent health planning and program design.
Although funding and resource allocation decisions are affected by multiple determinants, there are strategies to enhance sustainability. One potential strategy is to enable community capacity building. It focuses on strengthening community autonomy through facilitating refugee-led organisations and knowledge sharing. 85 Such initiatives can foster a positive support cycle for health co-design, planning, and implementation. However, they may encounter substantial challenges during initial phases, especially in communities where identifying universal community leaders is difficult. Strong organisational capacity and leadership to ensure the investment in both the infrastructure and value-building—supports the creation of administrative structures and the engagement of the local community 86 —aligning with the needs of culturally competent refugee health planning.
Theoretical Lens
This study identified significant health and social issues for the Yazidi community, spanning mental health burdens, chronic physical conditions, and barriers to social wellbeing. These issues are prevalent, arise from intercorrelated determinants that conventional single intervention cannot adequately address. The application of PPM model mapped the thematic findings into modifiable factors critical to successful program planning and enhanced its transferability to practice and policy: from the predisposing trauma and health literacy influencing the community’s health management decisions, to enabling barriers of language proficiency and social integration, and culminating in the funding shortages as the reinforcing gaps. Successful health planning for the Yazidi community needs to prioritise modifying these factors alongside proper cultural competency and trauma-informed practice.
Practice and Policy Implications
The findings provide critical implications for practice, policy, and planning targeting refugee populations with heightened needs:
Trauma and Mental Health concerns are common among the refugee communities. These concerns can be better addressed by trauma-informed practices. To action such practices, proactive consultation with the bicultural support workers on service delivery and program implementation are recommended. Trauma Informed Care (TIC) training across all service providers and program staff is recommended to foster understanding of the refugees’ trauma and displacement experiences and healthcare equity. 87
Social Integration is critical for enabling the community’s healthy behaviors. Investing in community resources, such as the community hubs and refugee-led programs, can foster social connections and reduce isolation. Policies supporting transportation infrastructure to reduce geographic isolation in regional areas are also recommended as transportation barriers significantly hinder employment and social connections. Initiatives that promote refugee employability through skill development and fast-track credential recognition can further strengthen social integration. 88
Health Knowledge shapes community members’ interpretation of health symptoms and services, which affects their ability to manage health. Incorporating health message alongside culturally responsive care plans that acknowledges its influences should be organizational prioritise. 89 Co-designing with the community on brief health message materials using various media formats, such as video, chats, and illustrations, is recommended.
Language Proficiency affects the community members’ ability to engage in healthy behaviors. The linguistic barriers can be better mitigated through incorporating bicultural support workers across services. To increase accessibility, policies and organizations could facilitate trainings of competent bicultural workers from the community to provide trusted language support in addition to the trained interpreter services.
Sustained Funding is critical for the long-term impacts of community-based health planning. Addressing this requires strong governance and political level leadership that enables appropriate resource allocation to regional resettlement cities. Local organizations and grants can trial demand-driven funding models with the focus to foster community autonomy.85,86
Cultural Competency training should be prioritized across all sectors. It should be co-designed with community members and implemented to all program workers to better address the abovementioned factors.
Network Support on resources and information sharing is beneficial for competent health planning and service delivery. Health services could establish communication boards and resource folders with regularly updated referral information in regional settings.
Additionally, social prescribing approach was recommended by community stakeholders as a relatively lower-cost initiative that could address health determinants identified in this study. It prescribes nonclinical services, such as social activities or community programs, to improve health and wellbeing through addressing underlying emotional and social needs. 90 This approach provides positive social engagement in less confronting ways, and targets social determinants and the complex social needs, 91 improving mental health, loneliness, and noncommunicable diseases. 92 The focus of this approach aligns with the complex needs of the Yazidi community. Although evidence on its effectiveness remains tentative, requiring further investigation, community members confirmed its potential benefits and acceptability as they enjoyed the community hubs, workshops, and social activities. Thus, social prescribing consultation and problem-solving assistance may facilitate health planning success.
Limitations and Research Directions
A key strength of this study lies in its inclusion of diverse stakeholders across sectors—refugees, social work, allied health, mental health, education, and community support— providing a comprehensive assessment of the social determinants of health for the refugee communities. Through the lens of the PRECEDE-PROCEED model, this study translated the voices of community members and stakeholders into modifiable factors that influence health planning.
However, several limitations should be acknowledged. Due to language barriers and time constraints, the study included a limited number of vulnerable community members into the one-to-one interview. The interview and focus group guides also lack structural validation but were only pilot tested with two biocultural support workers. Additionally, convenience sampling employed for focus group introduces a risk of selection bias by potentially under-representing isolated individuals. Although efforts were made to minimise bias, data from interviews and focus groups may be affected by subjectivity and influenced by the interpretations of both bicultural workers and researchers. Future research would benefit from the involvement of trained researchers from Yazidi backgrounds to safeguard the meanings of participants’ response and to improve access to hard-to-reach subgroups, particularly women and individuals with low English proficiency. Engaging researchers with cultural and linguistic expertise will enhance the depth and validity of findings.
Future research could examine the lived realities and service access barriers among hard-to-reach subgroups, such as women and older adults. Additionally, this study had limited scope to explore the identified barriers to higher education access for refugee-background students. Subsequent investigations could further explore these barriers and evaluate expanded access pathways for refugee-background students, such as bridging programs and tailored academic support, to enhance educational equity.
Conclusion
This study offered novel insights into the key determinants shaping the health and wellbeing of the Australia’s largest Yazidi refugee community resettled in the regional city. By applying PRECEDE-PROCEED model as an innovative analytic framework to map the lived experiences of community members and service stakeholders, this study provides a structured yet flexible lens to identify the intersecting barriers and modifiable health factors.
This study highlights its practical significance through the direct implication to health planning and intervention design. Trauma was found to impair cognitive function, emotional regulation, and trust-building, underscoring the urgent need for trauma-informed care across all sectors. Social integration enables recovery, access to resources, and improves overall quality of life, while health literacy and language barriers shaped health management behaviors, communication, and service navigation. Finally, sustained funding is essential to ensure the continuity and cultural safety of health programs and reinforce health outcomes.
Future healthcare and planning should address these interacting factors through culturally responsive, trauma-informed, and community-driven approaches—supported by consistent investment — to enhance health equity for refugee populations, particularly those in regional and high-need settings where structural constraints amplify vulnerability.
Supplemental Material
sj-docx-1-inq-10.1177_00469580261438078 – Supplemental material for Intersecting Factors Impacting the Health and Wellbeing of a Resettled Yazidi Refugee Community: A Qualitative Study
Supplemental material, sj-docx-1-inq-10.1177_00469580261438078 for Intersecting Factors Impacting the Health and Wellbeing of a Resettled Yazidi Refugee Community: A Qualitative Study by Shujie Chen, Nicola Wiseman, Kelly Hogan-Buckingham, Elizabeth Laverty and Hai Phung in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580261438078 – Supplemental material for Intersecting Factors Impacting the Health and Wellbeing of a Resettled Yazidi Refugee Community: A Qualitative Study
Supplemental material, sj-docx-2-inq-10.1177_00469580261438078 for Intersecting Factors Impacting the Health and Wellbeing of a Resettled Yazidi Refugee Community: A Qualitative Study by Shujie Chen, Nicola Wiseman, Kelly Hogan-Buckingham, Elizabeth Laverty and Hai Phung in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors would like to acknowledge the bicultural support workers for being advocators and interpreters. The authors also acknowledge the support from Multicultural Australia, local gatekeepers, other organizations and individuals.
Ethical Considerations
The ethical conduct of this study was evaluated and approved by the Griffith Human Research Ethics Committee (No. 2024/481).
Consent to Participate
Informed consent to participate was obtained from all participants and their legal guardians (if under 18).
Consent for Publication
Consent for publication was obtained from all participants and their legal guardians (if under 18).
Authors Contributions
All authors contributed to the writing of this manuscript. The first draft of the manuscript was written by Shujie Chen. Study conception and design were performed by Shujie Chen, Nicola Wiseman, and Hai Phung. Participant identification and recruitment were performed by Shujie Chen, Elizabeth Laverty, and Kelly Hogan-Buckingham. Data collection and analysis were performed by Shujie Chen. All authors agreed and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by Griffith University Higher Degrees by Research Funds and Griffith University Postgraduate Research Scholarship.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.