
Abstract
Digital mental health interventions are increasingly used to address gaps in access to psychological services in Saudi Arabia. However, cultural, technological, and usability factors may shape public acceptance of these tools. This study examines the willingness of Saudis to use the Labayh mental health application, guided by the Unified Theory of Acceptance and Use of Technology (UTAUT), focusing on the roles of performance expectancy, effort expectancy, social influence, and facilitating conditions. A cross-sectional online survey was administered to adult participants (n = 307). Validated UTAUT measures were used, and multiple regression analyses tested the effects of the 4 constructs on behavioral intention to use the application. The findings supported 3 of the 4 UTAUT constructs. Performance expectancy was the strongest predictor of behavioral intention. Effort expectancy also had a significant effect, indicating that ease of use increased adoption. Social influence significantly predicted intention, particularly among younger respondents, underscoring the role of peers, family, and clinicians. By contrast, facilitating conditions were not significant, likely reflecting a ceiling effect whereby most participants already possessed sufficient access and technical readiness, making this factor less relevant. These results indicate that acceptance of digital mental health applications in Saudi Arabia is primarily driven by perceived usefulness, ease of use, and social endorsement, whereas infrastructure plays a limited role. Efforts to increase adoption should prioritize culturally sensitive communication, usability-centered design, and engagement with trusted social and clinical influencers to encourage sustained uptake across diverse groups of users nationwide. No clinical trial registration applies.
Keywords
Introduction
Psychological health is an aspect of health that relates to how people think, feel, and behave in their day-to-day lives. In many cultures, including Saudi Arabia, psychological health problems were not spoken of, and people did not go for help, as it was taboo. However, there has been a trend over time to acknowledge the need for psychological health, primarily because of awakened awareness and some drive to deploy psychological disorders as something shameful.1-3 Despite the Saudi government initiating several programs to enhance the accessibility of psychological health care, many individuals still face barriers to seeking help due to cultural conservatism and the social stigma associated with mental illness. In this context, the preference for maintaining anonymity and confidentiality reflects cultural sensitivities rather than concerns about data security, which are global in nature.
Psychological health is one of the most vital aspects of human life since it influences physical health and productivity, interpersonal relationships, and overall well-being. Speaking of the possible adverse outcomes of psychological health disorders, if not diagnosed and treated, these can lead to chronic illnesses, disability, development of further mental disorders, and even suicide. 4 Studies show that there are various mental health illnesses such as depression, anxiety, and stress, among others, with these rates being influenced by the COVID-19 pandemic that imposed measures such as lockdowns to prove fatal to these ailments. 5 Hence, attending to psychological health is essential to prevent and treat diseases not only within people but also in society at large.
As the application of technology advances in human society, new ways of combating psychological health disorders are introduced, and these are solutions that are sufficiently free from the constraints that exist when a person decides to seek physical help. With the use of applications and telehealth services in delivering psychological health services, there is anonymity, ease, and access, which is quite essential in cultures that do not support psychological health. 6 These technologies may resonate with more people as they enable someone to receive support and guidance through information and services available from the comfort of their home. The Labayh app is one such example; it is an application that offers psychological support, especially in the Kingdom of Saudi Arabia, where the presence of professional psychologists is still limited and accepting help in this regard is not culturally feasible. 7
Despite the growing literature on digital mental health, few studies have examined how cultural stigma and social norms shape technology adoption in non-Western contexts, particularly in Arab societies. Most prior research has focused on Western populations or generalized global samples, overlooking localized determinants of willingness to use psychological health applications.8-10 Within Saudi Arabia, existing studies have primarily described awareness levels or general attitudes without applying comprehensive theoretical frameworks to explain behavioral intention. Furthermore, while several digital mental health tools exist, empirical investigations of culturally grounded platforms such as Labayh remain limited. As a locally developed and widely used application, Labayh offers a unique opportunity to explore how cultural sensitivity, perceived trust, and usability interact to influence adoption intentions. Addressing these gaps not only extends the UTAUT model’s applicability but also contributes to the global understanding of mental health technology acceptance across diverse cultural settings.
This study aims to assess the acceptance of psychological health online interventions among Saudis, using the Labayh app as a case study. By employing the Unified Theory of Acceptance and Use of Technology (UTAUT), the study seeks to understand the factors that influence the behavioral intention of individuals to use the Labayh app for psychological health. The Unified Theory of Acceptance and Use of Technology (UTAUT) was selected as the guiding framework for this study because it provides a more comprehensive and integrative model of technology adoption compared with earlier theories such as the Technology Acceptance Model (TAM 11 ), the Theory of Planned Behavior (TPB 12 ), and the Theory of Reasoned Action (TRA 13 ). UTAUT consolidates the main determinants of user intention and behavior—performance expectancy, effort expectancy, social influence, and facilitating conditions—offering superior explanatory power across diverse contexts. 14 This model has been widely validated in digital health research,15,16 particularly in studies examining health app adoption, which makes it well suited for assessing psychological health technologies in a culturally conservative and rapidly digitizing society such as Saudi Arabia.
The primary objective of this study is to evaluate the impact of social influence, performance expectancy, effort expectancy, and facilitating conditions on users’ behavioral intentions. Through this study, the study aims to provide insights that can help enhance the effectiveness and acceptance of digital psychological health solutions, ultimately contributing to better psychological health outcomes in Saudi Arabia.
Psychological Health Talk in Saudi Arabia
The focus in Saudi Arabia on psychological health as a topic has evolved over a few years, changing from a state which could be regarded as stigmatized into one that is being increasingly discussed and matters. Traditionally, psychological health problems and illnesses were not discussed much; people did not admit when they were dealing with any of these problems. This prejudice stemmed from the culture and society, whereby the symptoms of psychological health problems were considered shameful. 17 Nevertheless, the Saudi government and its various organizations have begun the process of changing these perceptions. Programs like the new Saudi National Mental Health Survey have substantially contributed to raising awareness of the situation with mental health disorders and the demand for affordable and quality mental health care. 18 Besides the government support, other factors played roles in raising awareness concerning psychological disorders and their treatment, namely, the attempts to launch the campaigns and media coverage of the mentioned issue. Such campaigns can divest mental illnesses and promote seeking help for those who need it among the population. For instance, through social media platforms, mental health awareness and support have become effective since they help demystify psychological health discussions. Furthermore, global challenges like the COVID-19 pandemic have come to expose psychological health even more by receiving attention and calls for focus on how to improve the health of people’s minds. 5
However, current research indicates that there are still prevalent issues that are still rampant in Saudi Arabia concerning psychological health. Persons continue to experience restricted access to psychological health care, especially in rural settings, while the need for more qualified psychological health care workers rises. Therefore, cultural and societal issues remain barriers to the improvement of mental health services, with many people not willing to come forward to seek help from a psychological health practitioner because of stigma or lack of knowledge of psychological health conditions. 19 Also, even though digital psychological health interventions can provide the desired solutions, their adoption and efficacy are contingent upon surmounting these cultural barriers and ensuring that the solutions introduced align with the Saudi population’s needs and technological convenience. 20 These problems must be solved using additional methods such as enhancing awareness about psychological health, providing more facilities, and using culturally appropriate strategies.
Psychological Health and Applications
Digital technology has significantly impacted almost every area of health, including psychological health. Psychological health online interventions, also known as psychological health applications, are novel in how they provide psychological health assistance. These applications’ services contain self-help, counselling, and psychoeducation, which is comfortable and anonymous. 6 The accessibility is profound in areas where psychological health prejudice is still present, enabling persons to seek assistance without the possibility of experiencing such prejudice and discrimination.6,19 Further, the possibility of a change and its applicability to a large number of people with psychological health issues also makes digital solutions a suitable means for dealing with the problem.
In Saudi Arabia, particularly, the uptake of psychological health applications is being embraced due to the opening up of the country, which is availed by the increasing number of smartphones and internet access. Due to the COVID-19 pandemic, such technologies have gained more popularity because face-to-face services have become limited due to the social distancing measures observed. 21 It has revealed that psychological health online interventions can enrich healthcare service delivery by fulfilling the existing voids. Research has further indicated that the availability and usage of digital psychological health interventions help reduce the symptoms of depression, anxiety, and stress, hence enhancing psychological wellness. 6 These interventions work best for the identified target population because they are culturally neutral and easy to use. However, extensive use and efficacy of psychological health applications are contingent on certain factors. It is crucial to guarantee the protection of users’ data since such considerations contribute to the non-usage of such services. 21 Moreover, there is a further need to provide scientific evidence of the effectiveness of the mentioned interventions, which should be systematically investigated and assessed. Therefore, technology developers, healthcare practitioners, and policymakers need to work together to make suggestions to develop a sustainable context to integrate digital psychological health solutions, as Alqifari et al 22 suggested. If such challenges are addressed, then apps in psychological health will significantly facilitate the improvement of mental health care and its availability in Saudi Arabia as well as other parts of the world.
Labayh App as a Psychological Health App in Saudi Arabia
The Labayh app is an excellent example of how digital technologies tackle concerns about psychological well-being in Saudi Arabia. Labayh provides live sessions with professional counsellors, self-help tools, guides, and access to materials and articles to address the individual’s psychological needs. The app is meant to de-sensitize people seeking support and assistance regarding mental health, as the application promises to keep it confidential and, at the same time, easily accessible. 7 This app’s success indicates that any intervention implemented in modern society must develop solutions that are particular to a society’s cultural and social context.
The creation of the Labayh app is a step forward for the therapy sector in digital mental health in Saudi Arabia while considering the cultural context. Labayh provides live sessions with professional counsellors, self-help tools, guides, and educational materials that enhance the mental health of its users. According to Labayh app, the best psychologists and psychotherapists providing sessions, webinars, and support groups easily through the app with more than 1000 Licensed therapists by the Saudi Commission for Health Specialties, available 24/7, in total, 47.5 million minutes of therapy so far. Moreover, people can find out their level using assessments such as depression, anxiety, self-esteem test, shyness, obsessive compulsive scale, burnout, and narcissistic personality.
A significant aspect is the need to maintain confidentiality and users’ privacy when using Labayh because culture is a significant barrier to seeking mental health support, even in the current context. In this way, as these concerns are addressed with the help of the app, more people will turn to the mentioned services, and consequently, the stigma for people with psychological disorders will be reduced, and more open discussions about mental health problems in the country will be initiated.
Furthermore, Labayh’s structural design and performance are optimal for Saudi users only. This app was developed with an Arabic user interface, making it usable for Arabic people. Moreover, the services offered are culturally sensitive regarding the social and cultural setting of Saudi Arabia, as presented by Habachi. 7 Through the widespread use of the app and positive user reviews, it is possible to conclude about the efficiency of the method adopted by the app in addressing the clients ’ mental health issues as Saudis. 23 Additionally, the Labayh app shows the usefulness of technology-supported interventions that can be secondary yet supportive for professional mental health care interventions in enhancing the psychological quality of life. 22 Nevertheless, Labayh can be instrumental in filling the gap in mental health services and stimulating Saudi Arabia’s population’s interest in balanced psychological well-being.
The Unified Theory of Acceptance and Use of Technology (UTAUT)
One of the most reliable models for studying technology acceptance and use is the Unified Theory of Acceptance and Use of Technology (UTAUT). Proposed by Venkatesh et al in 2003, UTAUT is a model that incorporates parts from the other models to make a new and wholesome view of technology acceptance. The constructs of UTAUT include performance expectancy, effort expectancy, social influence, and facilitating conditions, which are influential in predicting users’ behavioral intentions and actual technological use. 24 This model has also been used in various fields, such as the healthcare domain, to explain the usage of new technologies and how to increase user engagement and satisfaction. The first component is performance expectancy is the perceived benefit of using a specific technology to improve a job’s performance. 14 In an innovation such as Labayh, a psychological health technological application, performance expectancy could be defined as the user’s belief in the application’s capability to enhance their psychological well-being. It has been ascertained that when the users’ perceived usefulness is high, the likelihood of the user continuing to use the developed technology will also be high. 25 For example, if the users assume that they can be hurriedly relieved of anxieties or depressive disorders by using digital psychological health interventions, their behavioral intention will be inclined positively toward it. 6 The second component is effort expectancy, which is the extent to which one believes using technology is easy. 14 In the case of the Labayh app, these are the application’s facility and navigation, where many new users may require some guidance, especially when utilizing the app. The studies provided in the current article point out that users’ general perception of technologies is that when technologies are easy to use, customers are more likely to adopt them to the extent that the ease of use reduces the perceived and actual usage costs. 24 In the case of Labayh, the app must be easy to use and friendly enough, especially for those without excellent advanced technological knowledge, so that people can fully accept the application and continue to use it. 7
The third component is social influence which is the level of pressure that individuals feel they are expected to use the new technology by other people who matter in their lives. 14 In the context of Labayh, social pressure might be from people who use and suggest that this application is helpful in the management of psychological health problems. In nations where collective opinion is decisive in changing one’s actions, such as Saudi Arabia, social influence is vital to the enlightenment of new technology. As suggested by Labayh, when key influencers recommend this application, it raises the potential users’ behavioral intentions regarding the app’s adoption and improves its reception and utilization. 19 The fourth component is facilitating conditions. Enablers relate to the user’s experience of the resources and support that can be made available to attain technology by the organization. 14 These are technical infrastructure, which refers to the availability of devices that go hand in hand with user support. In the case of Labayh, using the mentioned features as potential facilitation factors could include internet connection, technical support concerning applications, and linking with other health systems. According to Tamilmani et al, 24 when users are supported and have all they need to use a specific technology, they have a high chance of continuing to use it. Accordingly, by maintaining strong facilitating conditions, Labayh can increase user satisfaction and extend the frequency of application usage.
A synthesis of the reviewed literature reveals both convergence and tension across studies on digital mental health adoption in Saudi Arabia. While earlier works consistently identify stigma, privacy concerns, and limited access as enduring barriers to psychological help-seeking,17,19 more recent findings suggest gradual normalization of mental health discourse driven by governmental campaigns and social media visibility.18,21 This contrast underscores an urban–rural divide: digital interventions appear more acceptable among young, digitally literate Saudis, yet remain underused in rural or conservative regions.26-28 Integrating these insights through the UTAUT model allows a deeper understanding of how cultural values—particularly collectivism, gender norms, and trust in authority—mediate constructs such as social influence and facilitating conditions. Existing studies have rarely examined these interactions empirically, creating a gap this study addresses by situating UTAUT within a culturally grounded context. In doing so, it contributes to refining technology acceptance theory for non-Western populations and extends the evidence base for culturally responsive digital mental health interventions in Saudi Arabia (Figure 1).
Based on the above discussion, the following hypotheses were proposed:
H1: Social influence positively influences the behavioral intention of people to use the Labayh app for Psychological health.
H2: Performance expectancy positively influences the behavioral intention of people to use the Labayh app for Psychological health
H3: Effort expectancy positively influences the behavioral intention of people to use the Labayh app for Psychological health.
H4: Facilitating conditions positively influence the behavioral intention of people to use the Labayh app for Psychological health.

The Proposed UTAUT model for the willingness to utilize psychological health applications.
Methods
On August 20, 2024, the author submitted the initial report to the Research Ethics Committee (IRB), which included the basic information about this research, and the informed consent form for the respondents. The ethical approval consent was received on September 8, 2024, and the ethics approval number ID is KSU-HE-24-714. The procedures used in this study adhere to the tenets of the Declaration of Helsinki. The scope of approval included the design and distribution of an online survey, voluntary participation of adult respondents in Saudi Arabia, data anonymization, and statistical analysis of the collected responses.
Informed consent was obtained from all participants involved in this study. Participants were provided with a written consent form at the beginning of the online survey, which clearly outlined the purpose of the research, the voluntary nature of participation, the assurance of anonymity and confidentiality, and the intended use of the data for academic publication. Participants were informed that there were no anticipated risks to their participation and that they could withdraw from the survey at any time prior to submission. Data were collected between October 10 and 31, 2024.
This study adheres to the relevant EQUATOR reporting guideline, and the corresponding checklist has been completed and included as a Supplemental File.
Study Design and Participants
This study employed a quantitative, cross-sectional research design to explore the psychological and demographic factors influencing the acceptance of the use of Labayh psychological online intervention app using the Unified Theory of Acceptance and Use of Technology (UTAUT) framework. Participants were recruited online via a non-probabilistic sampling approach. The inclusion criteria required participants to be aged 18 or above and to have a basic familiarity with mobile health applications, particularly Labayh. To ensure that only actual users of the Labayh application were included, a screening question was placed at the beginning of the questionnaire: “Do you currently use the Labayh application?” Respondents who answered “Yes” were automatically directed to the subsequent sections of the survey, while those who selected “No” were redirected to a thank-you page indicating that they were not part of the target sample. This procedure ensured that all analyzed responses represented active users of the application. The initial sample consisted of 417 participants. However, 110 responses were excluded due to none response at all (60 participants) or indication of unfamiliarity with the Labayh app (50 participants), resulting in a final sample size of 307. Participants were informed about the study objectives and provided consent electronically before accessing the survey. The survey was hosted on Qualtrics which was optimized for both desktop and mobile device access. Completion of the survey took approximately 10–15 minutes, and participation was entirely voluntary and anonymous.
A formal power analysis was not conducted for this study because it was designed as an exploratory cross-sectional investigation aimed at understanding behavioral trends rather than testing a specific hypothesis. The final sample (N = 307) was considered adequate based on comparable studies employing the Unified Theory of Acceptance and Use of Technology (UTAUT) framework in similar contexts.29,30 This sample size ensured sufficient variability and representation across demographic groups to support meaningful statistical interpretation.
Measures
All study variables were measured using an adapted version of the UTAUT. The original instrument was modified for contextual relevance to the mental health field and the Labayh app. The questionnaire consisted of 5 primary constructs from the UTAUT model; Behavioral intention (acceptance) was assessed using 3 items (eg, “I would use a psychological online intervention if offered to me”). Performance expectancy included 3 items focusing on perceived improvements in psychological health (eg, “The Labayh app could improve my general well-being”). Effort expectancy assessed ease of use through 2 items (eg, “The Labayh app would be easy to operate and comprehend”). Social influence was measured using 3 items evaluating approval from peers, friends, and health professionals (eg, “My general practitioner would approve of a psychological online intervention”). Facilitating conditions consisted of 3 items including the availability of resources, knowledge, and support (eg, “I have the knowledge necessary to use Labayh”).
Each item was rated on a 5-point Likert scale ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). Higher scores suggested stronger agreement with the statement and greater acceptance or belief in the app’s usefulness or accessibility. The exact questionnaire is presented in Table 1.
Descriptive Statistics Showing Mean, SD and Mode for all Study Items.

Scale is on a 5 point rating.
To ensure the cultural appropriateness and clarity of the adapted UTAUT items, a 2-stage validation process was undertaken. First, 2 academic experts in communication and behavioral research reviewed all items for content relevance, linguistic equivalence, and contextual suitability within the Saudi cultural setting. Minor adjustments were made to wording to improve clarity and maintain conceptual consistency. Second, a pilot test involving 30 participants was conducted to evaluate comprehension and item reliability. Based on the pilot results, all items demonstrated satisfactory internal consistency, with Cronbach’s alpha values ranging between .81 and .89. Exploratory factor analysis further confirmed the expected factor structure, supporting the validity of the adapted measures (Table 2).
Exploratory Factor Analysis and Reliability of Adapted UTAUT Constructs.
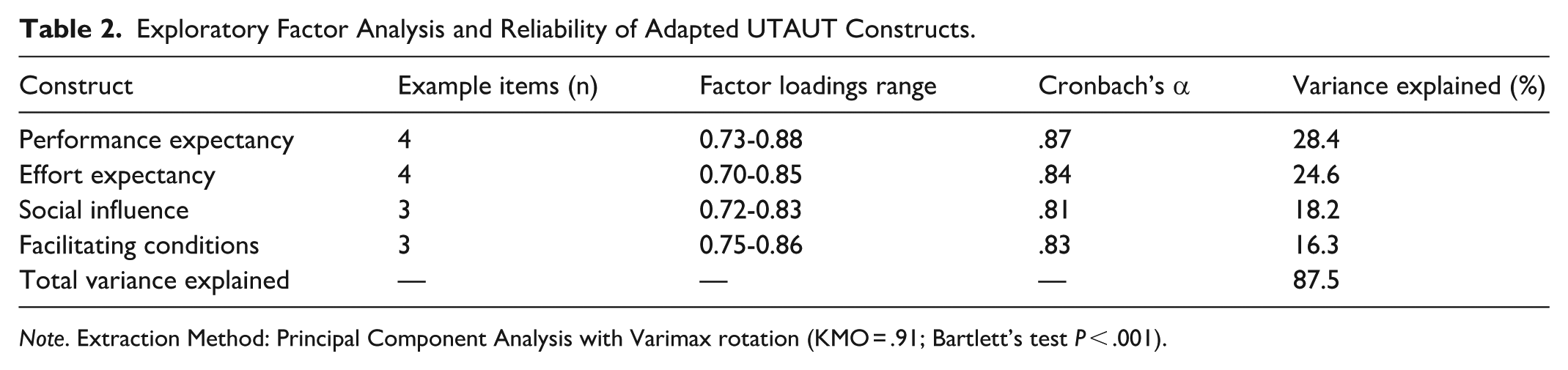
Note. Extraction Method: Principal Component Analysis with Varimax rotation (KMO = .91; Bartlett’s test P < .001).
Exploratory factor analysis (Table 2) confirmed the four-factor structure corresponding to the UTAUT dimensions. All items loaded strongly (≥.70) on their intended factors, and reliability coefficients exceeded .80, indicating robust internal consistency.
Demographic Data
This study collected demographic information focusing on age and gender. Respondents indicated their age in 1 of 4 categories: 18 to 20, 21 to 30, 31 to 40, and 41 years and above. Due to only 2 individuals reporting being over 40, these responses were merged with the 31 to 40 age bracket, resulting in three groups for analysis: 18 to 20 years, 21 to 30 years, and 31 years and older.
The final age distribution showed that the largest proportion of participants (n = 158, 51.5%) were between 21 and 30 years old, followed by 142 participants (46.2%) aged 18 to 20. A small group of seven individuals (2.3%) were 31 years or older. In terms of gender, the sample was predominantly female, with 275 participants (approximately 89.6%) identifying as female and 32 participants (10.4%) as male.
Statistical Methods
Data were analyzed using IBM SPSS Statistics version 30.0. The analytical approach was conducted in 3 sequential stages. First, descriptive statistics (means, standard deviations, and modes) were calculated to summarize participant responses to all UTAUT-related items. This provided insight into general trends in users’ attitudes and levels of agreement across the 5 theoretical constructs. Second, to assess group differences in behavioral intention and UTAUT variables by demographic characteristics, inferential statistics were used. One-way analyses of variance (ANOVA) were applied to compare age groups, while independent samples t-tests were used to examine gender-based differences. For all analyses, a P-value of <.05 was considered statistically significant. Effect sizes were calculated using partial eta-squared (η 2 ) for ANOVA tests to determine the strength of observed relationships. Lastly, hierarchical multiple regression analysis was conducted to identify predictors of behavioral intention to use the Labayh app. In the first block of the model, age and gender were entered to account for demographic variance. In the second block, the 4 UTAUT predictors—performance expectancy, effort expectancy, social influence, and facilitating conditions—were added to determine their individual and combined contribution to explaining behavioral intention. Beta coefficients (β), standard errors (SE), t-values, R2, and ∆R2 were reported to assess model fit and predictor strength.
Result
Scale Description
Descriptive statistics provided some clear insights (see Table 1) of participants’ views about the Labayh psychological intervention app. Of the 3 items measuring behavioral intention, the strongest agreement came from the statement, “I would use a psychological online intervention if offered to me” (M = 4.11, SD = 0.89), suggesting general willingness to use such services. Interestingly, the statement “I would like to try a psychological online intervention” scored the lowest (M = 3.74, SD = 1.02). This could mean that those already familiar with Labayh felt no need to “try” it again, or perhaps new users showed greater hesitation. The wider spread of responses on this item (reflected in the standard deviation) supports this interpretation. Social influences also played a role. Participants tended to agree that people close to them—especially their general practitioners (M = 4.06, SD = 0.84)—would support the use of such interventions. In other would, general practitioner, followed by friends’ approval are strong influence for the use of Labayh app for psychological online intervention. Performance expectations were generally positive as well, with scores clustering between 3.91 and 3.94 and similar standard deviations. These ratings suggest users believe the app could support their stress management, mental and general well-being. Effort expectations were also favorable. Many respondents felt confident in the app’s ease of use (M = 4.00, SD = 0.87) and its fit within daily routines. The highest ratings overall were seen in facilitating conditions. A large number of users felt they had both the technical resources (M = 4.43, SD = 0.73) and the knowledge (M = 3.93, SD = 0.98) to use the app effectively. Most scores across all items shared the same mode of 4, indicating consistent agreement throughout the responses.
Analysis of Variance: Influence of Sociodemographics
The Analysis of variance (ANOVA) in Table 3 looked at how participants’ age and gender related to their views on using the Labayh psychological app. Interestingly, younger participants—especially those between 18 and 20 years old—seemed the most open to trying the app. Their average score for intention to use was higher (M = 4.07) than older groups, and the statistical test showed this difference was meaningful (P = .045). This might reflect greater comfort with digital tools among younger users. They also rated the app’s usefulness more positively than older participants, particularly when it came to improving their mental health (P = .039). While differences in ease of use and access to resources weren’t statistically strong (P > .05), the 18 to 20 age group again gave higher ratings on average. On the other hand, social influence—how much approval they felt from friends or professionals—didn’t vary much with age.
Result of ANOVA for Age and t-Test for Gender.
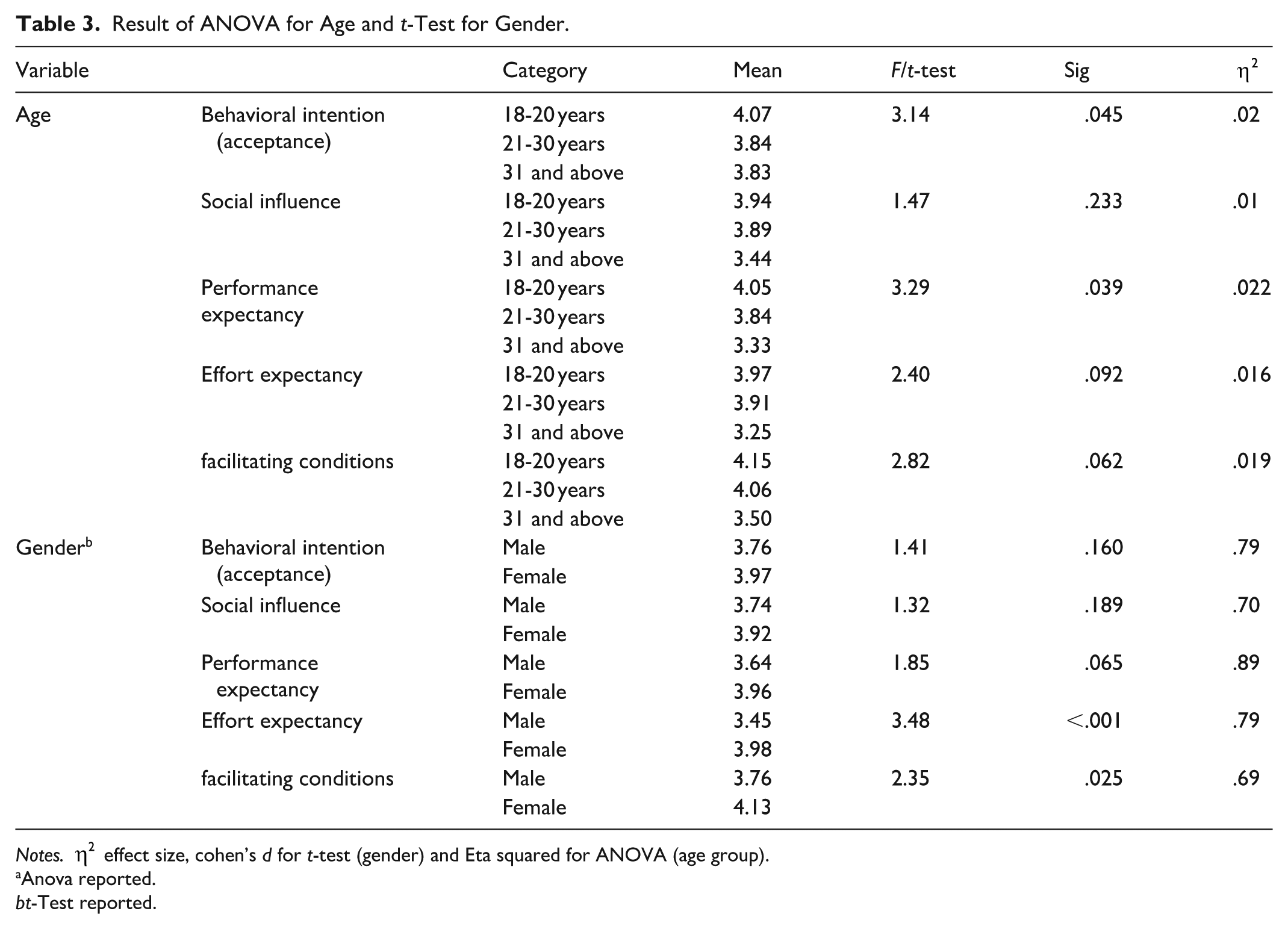
Notes.
Anova reported.
t-Test reported.
Gender differences painted a different picture. While male and female participants did not differ much in whether or not they would use the app (acceptance and social influence) or how helpful they thought it was (performance expectation), females did report feeling more confident (effort expectancy) about actually using it. In fact, women found the app easier to use (M = 3.98 vs 3.45), and this difference was quite significant (P < .001). They also felt more supported and better equipped (facilitating conditions) to access the app compared to their male counterparts (P = .025). This could suggest that women not only feel more comfortable with digital health tools but also have stronger support systems in place.
Hypotheses Testing
Table 4 present the result of the study hypothesis testing. It is presumed that social influence, performance expectancy, effort expectancy and facilitating conditions positively predicts participants behavioral intention (acceptance) to use the Labayh app for online psychological intervention.
To understand factors that might influence people’s willingness to use the Labayh psychological app, a hierarchical regression analysis was performed. The first model included the 2 basic factors: age and gender. The results showed that age had a small but significant effect (B = −.18, P = .041), meaning that older participants were a bit less likely to show interest in the app. Gender didn’t have much of an impact (B = .19, P = .224), so men and women seemed to feel pretty much the same about trying, using or recommending the app. These 2 sociodemographic accounted for only 2% (0.02) of the variations in participants behavioral intentions.
Hierarchical Regression.

B = unstandardized regression coefficient, SE = standard error, β = standardized coefficient, R2 = Percentage explained variation in the model, ∆R2 = Change in percentage explained variation between model 1and 2.
Sig: *P < .05. **P < .01. ***P < .001.
In the next part of the analysis, the conceptual scales were included: what people expected from the app (performance expectancy), how easy they thought it would be to use (effort expectancy), whether people around them would support their use (social influence), and whether they had the tools and help they would need (facilitating conditions). Once these were added, the model got much better at explaining people’s intentions, accounting for about 50% of the differences in how participants responded (R2 = .501).
The strongest predictor was performance expectancy (B = .443, β = .497, P < .001). In plain terms, people were more likely to want to use the app if they believed it would actually help their mental health. Effort expectancy was also statistically significant (B = .165, P = .005); when participants perceived the app as user-friendly, they were more inclined to experiment with it. Followed by Social factors which also achieved statistical significance (B = .158, P = .008). Albeit to a lesser extent, support from friends, family, or healthcare providers positively influenced their willingness to engage. These results support the study first, second and third hypothesis.
Interestingly, facilitating conditions had minimal impact (B = .022, P = .737) on participants intention (acceptance) to use the APP (the fourth hypothesis). This might be due to the fact that most participants already felt they had internet access or were familiar with app usage, rendering it a non-essential element for them. Therefore, there is no sufficient evidence from the study data to conclude that facilitating conditions positively influence behavioral intention (accept) to use Labayh app.
Discussion
This study sought to investigate the factors influencing Saudi individuals’ willingness to utilize psychological health applications, using the Labayh app as a case study and guided by the Unified Theory of Acceptance and Use of Technology (UTAUT). Drawing upon data from 307 participants and examining performance expectancy, effort expectancy, social influence, and facilitating conditions, the findings offer valuable insights into the contextual dynamics shaping digital mental health adoption in a culturally conservative society.
The findings reveal strong support for 3 of the 4 UTAUT constructs. Performance expectancy emerged as the most significant predictor of behavioral intention. This suggests that participants were more likely to use the Labayh app if they believed it would positively impact their psychological well-being. This aligns with previous research indicating that perceived usefulness is a dominant determinant in adopting health technologies.6,24 Effort expectancy also demonstrated a significant influence. This reflects that users were more inclined to adopt Labayh when they perceived it as user-friendly. This is particularly relevant in digital mental health, where ease of use may determine whether individuals with limited digital literacy can benefit from services.21,25 Social influence was another significant predictor, particularly among younger respondents. Approval from general practitioners and peers was found to shape willingness to use digital interventions, reflecting the collectivist and relational nature of Saudi society, where family and social circles hold strong sway over health-related decisions.14,19 Interestingly, facilitating conditions did not significantly predict behavioral intention, despite high ratings for access and technical readiness. This divergence may be due to a ceiling effect—most participants already possessed adequate technical capabilities, rendering facilitation less of a barrier in this specific context. Previous studies in high-tech societies have shown similar diminishing returns when technological infrastructure is abundant. 31
The results partially validate the UTAUT model. The 3 core constructs—performance expectancy, effort expectancy, and social influence—were supported, indicating the robustness of UTAUT in explaining technology adoption in non-Western, collectivist societies. However, the non-significance of facilitating conditions invites theoretical refinement. In the Saudi context, where internet penetration is high 22 and smartphone use is ubiquitous, facilitating conditions may no longer serve as a differentiating factor. This aligns with suggestions to evolve UTAUT constructs for digital-native populations or in contexts where infrastructure is stable. 15 Furthermore, the strong effect of social norms reflects the salience of cultural values, which suggests that UTAUT might benefit from integrating constructs from models like the Theory of Reasoned Action 32 or cultural dimensions theory 33 in future applications.
The findings of this study align with Lattie et al, 6 who emphasized the importance of perceived usefulness and usability in mental health app adoption among college students. Similarly, Alhusseini and Orji 20 identified cultural sensitivity, usability, and peer influence as pivotal to digital intervention success in the Gulf region. Cultural sensitivity in Saudi Arabia involves awareness of religious, social, and moral values that shape attitudes toward mental health. Since help-seeking is influenced by collectivist norms, privacy, and alignment with Islamic principles, digital psychological interventions must respect these cultural frameworks to enhance trust and utilization. 18 My results reinforce these insights, suggesting continuity in the literature regarding the universal importance of performance and effort expectancies. However, the negligible role of facilitating conditions diverges from findings by Al-Kahtani et al, 34 who found infrastructure and access limitations to be barriers to mental health technology adoption in rural Saudi regions. This difference may be attributable to the sample in our study, which predominantly comprised urban, educated, and digitally literate users. It underlines the need for demographic segmentation when studying health tech adoption. The study also complements qualitative findings by Alattar et al, 2 who noted the central role of stigma and social influence in mental health discourse in Saudi Arabia. Labayh’s privacy features may help overcome barriers of stigma, explaining its favorable reception among users and the strong impact of social influence on adoption.
This study has several practical implications. First, it reinforces the need for culturally adapted, Arabic-language digital mental health tools that are not only clinically effective but also perceived as useful and easy to use. Developers should prioritize user-centered design and accessibility, particularly for populations with limited digital fluency. Second, health campaigns aimed at encouraging digital mental health adoption should leverage trusted influencers—especially general practitioners and community leaders—to enhance social endorsement. As our findings suggest, peer and professional approval are pivotal in swaying behavioral intention, particularly among younger users. Third, while infrastructure support (ie, facilitating conditions) may not have shown direct influence in our sample, ensuring digital equity across rural and underserved regions remains critical. Policymakers should continue investing in internet infrastructure and mental health education to bridge the accessibility gap observed in other studies.
Despite the study’s valuable insights, several limitations warrant consideration. First, the sample was not representative of the entire Saudi population. The majority were female (89.6%) and aged between 18 and 30 years, limiting generalizability to older adults or males, who may have different attitudes toward psychological health technologies. On the other hand, this study did not conduct a formal power or sample size analysis prior to data collection. Instead, the sample size was determined based on previous studies using the UTAUT model in comparable settings. While this approach is common in exploratory behavioral research, it may limit the statistical power and generalizability of the findings. Second, the study relied on self-reported data, which may be subject to social desirability bias, especially given the cultural stigma surrounding mental health. Although the survey was anonymous, future research could incorporate objective behavioral data, such as app usage logs or longitudinal assessments of engagement. Third, while UTAUT offers a strong foundation, it may not fully capture the cultural and emotional nuances of mental health help-seeking behavior in conservative societies. Expanding the theoretical framework to include cultural or stigma-related constructs could enrich explanatory power. Finally, the cross-sectional nature of the study limits causal inference. Longitudinal research could better explore how behavioral intention evolves over time with continued exposure or changes in cultural perceptions.
Future research should aim to explore the perspectives of underrepresented groups, including older adults, males, and rural populations in Saudi Arabia. These groups may experience different barriers and motivators to adopting psychological health applications. Investigating gender-specific or generational dynamics could yield more nuanced intervention strategies. Moreover, qualitative methods such as in-depth interviews or focus groups could be employed to explore underlying motivations and concerns that quantitative models might overlook. Understanding emotional and cultural triggers for digital help-seeking could lead to more culturally resonant app designs. Researchers should also consider extending UTAUT by incorporating constructs related to perceived stigma, confidentiality, and trust. These dimensions may be particularly salient in conservative societies and could significantly influence user adoption. Finally, future studies could explore the efficacy of the Labayh app or similar interventions through experimental or longitudinal designs, assessing whether perceived intention translates into sustained use and actual psychological improvement.
Conclusion
This study contributes to understanding the determinants of Saudi individuals’ willingness to adopt digital psychological health tools, using the Labayh app as a representative case. Guided by the UTAUT model, the findings highlight that performance expectancy, effort expectancy, and social influence are central drivers of behavioral intention, while facilitating conditions play a minimal role in this digitally advanced context. These insights underscore that perceived usefulness, ease of use, and social endorsement are critical for encouraging mental health app adoption in collectivist societies such as Saudi Arabia.
Beyond theoretical implications, the study offers practical guidance for developers, policymakers, and health professionals. Designing culturally attuned, user-friendly applications and leveraging trusted social figures can enhance acceptance and engagement. By acknowledging cultural norms, social dynamics, and evolving digital behaviors, future research can refine the UTAUT framework and contribute to building inclusive, effective digital mental health ecosystems in Saudi Arabia and beyond.
Supplemental Material
sj-docx-1-inq-10.1177_00469580261437649 – Supplemental material for The Willingness to Utilize Psychological Health Applications Among Saudis: A Study Guided by the Unified Theory of Acceptance and Use of Technology (UTAUT)
Supplemental material, sj-docx-1-inq-10.1177_00469580261437649 for The Willingness to Utilize Psychological Health Applications Among Saudis: A Study Guided by the Unified Theory of Acceptance and Use of Technology (UTAUT) by Hessah F Alhugbani in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
This study received no specific funding and reflects the author’s independent academic efforts.
Ethical Considerations
On August 20, 2024, the author submitted the initial report to the Research Ethics Committee of King Saud University (IRB), which included the basic information about this research, and the informed consent form for the respondents. The ethical approval consent was received on September 8, 2024, and the ethics approval number ID is KSU-HE-24-714. The procedures used in this study adhere to the tenets of the Declaration of Helsinki. This research received no external funding. This study received no specific funding and reflects the author’s independent academic efforts. Ethics approval was exempted/waived on September 8, 2024. The scope of approval included the design and distribution of an online survey, voluntary participation of adult respondents in Saudi Arabia, data anonymization, and statistical analysis of the collected responses.
Consent to Participate
Informed consent was obtained from all participants involved in this study. Participants were provided with a written consent form at the beginning of the online survey, which clearly outlined the purpose of the research, the voluntary nature of participation, the assurance of anonymity and confidentiality, and the intended use of the data for academic publication. The consent was obtained electronically on September 8, 2024 by the principal investigator Hessah F Alhugbani, from adult participants residing in Saudi Arabia. In detail, on August 20, 2024, the author submitted the initial report to the Research Ethics Committee of King Saud University (IRB), which included the basic information about this research, and the informed consent form for the respondents. The ethical approval consent was received on September 8, 2024, and the ethics approval number ID is KSU-HE-24-714. The scope of the consent included agreement to participate in the study, permission for the use of anonymized data in academic research and publications, and acknowledgement that no personal identifiers would be collected. Participants were informed that there were no anticipated risks to their participation and that they could withdraw from the survey at any time prior to submission. For non-interventional research purposes, all respondents were fully informed about the nature of the study, how their responses would be stored and analyzed, and that all data would be handled in compliance with ethical standards and data protection regulations. Data were collected between October 10 and 31, 2024.
Author Contributions
The sole author is responsible for all aspects of the paper. This study received no specific funding and reflects the author’s independent academic efforts: The Author’s roles were conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, software, supervision, validation, visualization, writing – original draft, and writing – review & editing the final version. The Author directly accessed and verified the underlying data reported in the manuscript. The Author contributed to the data curation, investigation, methodology, resources, software, validation, visualization, writing – original draft, and writing – review & editing the final version. The Author has read and agreed to the published version of the manuscript.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analysed during the current study are not publicly available due participants privacy, but are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.