
Abstract
Rabies is a fatal zoonotic disease and a significant public health threat in Zimbabwe, especially in rural areas where domestic dogs are the main reservoir. This study examined factors behind low rabies vaccination coverage in dogs in Ward 2, Gutu District. A cross-sectional survey combining quantitative and qualitative methods was conducted with 60 dog-owning households through structured questionnaires. GPS coordinates for 200 dogs were collected for spatial analysis, and in-depth interviews were held with 10 key informants until thematic saturation was achieved. Vaccination coverage was 57.5%, below the 70% needed for herd immunity. Spatial analysis showed significant clustering of unvaccinated dogs in certain areas (P < .05). Of 14 dog bite cases recorded during the intensive study period, 3 (21.4%) involved vaccinated dogs, while 11 (78.6%) involved unvaccinated dogs or dogs of unknown status. Thematic analysis identified 5 main themes: financial barriers, knowledge gaps, cultural beliefs, accessibility issues, and communication challenges. A significant association was found between bites from unvaccinated dogs and fatal outcomes (P = .04). The low vaccination coverage stems from the interplay of behavioural, structural, and spatial factors. The convergent parallel design revealed that spatial clusters of unvaccinated dogs correspond to areas where qualitative respondents cited accessibility and financial barriers. Interventions should include targeted mobile vaccinations in hotspots and culturally sensitive awareness campaigns.
Introduction
Rabies, an insidious and fatal zoonotic disease, poses a significant challenge to global public health, particularly in regions where healthcare infrastructure remains fragile and populations are vulnerable. 1 The World Health Organisation estimates that rabies claims the lives of approximately 59 000 people annually. 2 Alarmingly, the overwhelming majority of these deaths are as a result of bites from rabid dogs, with children under 15 years most affected, accounting for nearly 40% of these cases. 2 The disease, though preventable through vaccination, persists in more than 150 countries, with Africa and Asia shouldering a significant portion of the global burden. 2 Economic losses associated with rabies, including treatment costs and productivity losses, are staggering, estimated at $8.6 billion annually. 3
In response to this important issue, the WHO, in collaboration with key global partners such as the Food and Agriculture Organisation (FAO), the World Organisation for Animal Health (WOAH), and the Global Alliance for Rabies Control (GARC), launched the ‘United against Rabies’ initiative in 2017. 3 This ambitious campaign aims to eradicate human rabies deaths by 2030, with a particular focus on mass vaccination of dogs, which are considered the primary vector for the disease. 3 As documented by WHO, successful examples from countries such as Mexico, which achieved rabies-free status for humans in 2019, provide compelling evidence that widespread dog vaccination, coupled with public education and increased access to post-exposure prophylaxis (PEP), can drastically reduce human rabies cases. 4 Nevertheless, challenges persist in under-resourced regions, where achieving and sustaining high vaccination coverage remains difficult. 5
Within Africa, the burden of rabies is particularly heavy, with an estimated 21 000 deaths annually, approximately 36% of the global rabies mortality rate. 3 Low vaccination coverage and limited healthcare services, especially in rural regions, are significant issues.5,6 In countries like Tanzania, rabies remains endemic, often unreported due to inadequate surveillance and gaps in public understanding of vaccination importance. 6 The economic impact of rabies in Africa is substantial, with annual expenses related to treating dog bites, livestock losses, and reduced productivity. 2 Nevertheless, there have been encouraging developments, such as mass vaccination initiatives in these nations, showing that rabies can be effectively managed through consistent efforts and resource commitment.7,8
In Zimbabwe, rabies is a critical public health issue, particularly in rural areas like Ward 2 in Gutu. The transmission is often linked to bites from rabid dogs, worsened by the scarcity of vaccination services. Reported vaccination rates are as low as 30% in some areas, far below the WHO-recommended 70% coverage needed to prevent outbreaks. 5 This situation is aggravated by limited resources, poor public awareness, and cultural barriers that hinder vaccination efforts, which weaken the initiatives to control the disease and safeguard the community from rabies. 5 Despite occasional vaccination drives, coverage remains inadequate, leaving the region at risk for rabies outbreaks.5,9 A significant gap exists in consistent data on vaccination rates and understanding of socio-demographic and behavioural factors affecting dog owners’ choices, particularly in rural Zimbabwe.
Although rabies vaccines are available, uptake among dog owners remains critically low. 10 Contributing factors are complex, ranging from limited access to veterinary services and poor health infrastructure to socio-cultural misconceptions and insufficient community awareness. 5 The continued prevalence of dog bites, coupled with suboptimal vaccination coverage, signals a serious gap in disease prevention strategy. 9 There is a pressing need to explore the underlying reasons why dog owners in Ward 2 remain hesitant or unable to vaccinate their dogs, including spatial, behavioural and systematic factors. This study, therefore, seeks to investigate the socio-demographic, behavioural, and spatial determinants of low rabies vaccination coverage among dogs in Ward 2, Gutu District, with the ultimate aim of informing targeted, effective, and sustainable public health interventions.
Materials and Methods
The quantitative component of this study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies. 11 The qualitative component follows the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines. 12
Study Area
This study was conducted in Ward 2 of Gutu District, located in Masvingo Province, in south-eastern Zimbabwe. The ward is predominantly rural, with an estimated human population of 3509 13 and a dog population of approximately 540 based on local veterinary records. The majority of residents in Ward 2 rely on subsistence farming and small-scale gardening. Dogs are primarily kept for guarding homesteads and livestock. Veterinary services are limited, with only 1 veterinary officer stationed at Denhere Veterinary Clinic, which serves as the primary fixed dog vaccination point. The rolling terrain and poor road networks complicate access to health and veterinary services, particularly during the rainy season. The population is largely Shona-speaking, and local beliefs and customs may influence attitudes towards dog bites, traditional healing, and modern veterinary practices, as reported by the study done in the same setting. 5 The study area map is presented in Figure 1.

The detailed area map.
Study Design
A descriptive cross-sectional convergent parallel mixed-methods design was employed. In this design, quantitative and qualitative data were collected concurrently during the same period (May-July 2024), analysed separately, and then integrated during interpretation to provide a comprehensive understanding of the factors influencing rabies vaccination coverage. The quantitative component focussed on measuring vaccination coverage, dog bite prevalence and socio-demographic factors. The qualitative component explored underlying barriers, motivations, and perceptions of dog owners regarding rabies vaccination. The integration of both data types allows for triangulation of findings and a more nuanced explanation of the quantitative results through qualitative insights.
Study Population, Sample Size and Sampling
The target population was dog-owning households in Ward 2. For the quantitative component, a sample size of 60 households was calculated using the Raosoft Sample Size Calculator, 14 setting parameters at a 90% confidence level and a 10% margin of error with a 50% response distribution due to logistical constraints of this exploratory field study. Households were selected using systematic random sampling from a community roster provided by the local health office. The first household was randomly selected, and every ninth household was approached thereafter. For the qualitative component, a purposive sampling approach was used to select 10 key informants, including community leaders (village heads, ward councillors) and dog owners. To ensure capture of diverse perspectives on barriers to vaccination, we purposively included owners of unvaccinated dogs. The final sample comprised: 3 village heads (K1_2, K1_8, K1_10), 1 ward councillor (K1_5), 1 village health worker (K1_1), and 5 dog owners (K1_3, K1_4, K1_6, K1_7, K1_9). This diverse composition was intentionally sought to capture perspectives from both community authorities and ordinary dog owners. A detailed breakdown of informant characteristics is provided in Table 5. All participants were residents of Ward 2. Recruitment continued until thematic saturation was reached, defined as the point where no new themes emerged from subsequent interviews, 15 which occurred at the 10th interview.
Inclusion and Exclusion criteria
For both components, participants were eligible if they were aged 18 years or older, resided in Ward 2, and were dog owners. Participants under 18 were excluded due to ethical considerations related to obtaining informed consent from minors in the context of a community-based study without a parent or guardian present during household visits. Additionally, the study questionnaire included questions about household income and decision-making regarding animal health topics for which minor household members (under 18) may not have complete information or authority to speak on behalf of the household. This criterion ensured that respondents were adults capable of providing informed consent independently and possessing comprehensive knowledge of household dog ownership and vaccination decisions. For the qualitative interviews, an additional criterion was ownership of at least 1 unvaccinated dog. Non-residents and those without dogs were excluded.
Data Collection Tools and Procedures
Quantitative data were collected using structured questionnaires administered electronically via the Kobo Collect Toolbox 16 in Shona or English by the first author. The questionnaires gathered data on socio-demographics, dog ownership, and vaccination history. GPS coordinates were collected for all dogs owned by the 60 participating households, representing approximately 37% of the estimated dog population in Ward 2 (based on veterinary records of approximately 540 dogs). All GPS coordinates were collected from households within Ward 2; however, due to the mismatch between administrative boundaries and actual settlement patterns, some points may appear marginally outside the boundary line on the map while still representing Ward 2 residents. Data collection took place between May and July 2024. Health records on dog bites and suspected rabies cases (defined as patients presenting with a dog bite and clinical symptoms consistent with rabies, or reports of aggressive/abnormal dog behaviour) from January 2020 to July 2024 were reviewed at Denhere Clinic, the primary health facility serving the ward.
Qualitative data were collected through face-to-face, semi-structured interviews using an interview guide. Data was collected by the first author (PGM), an undergraduate Public Health student trained in both quantitative and qualitative research methods. PGM completed a university-certified course in qualitative research methodology, including modules on conducting semi-structured interviews, taking field notes, and qualitative data analysis. Data collection was supervised by the second author (PLM) and third author (MYK), both experienced qualitative researchers and lecturers with multiple publications using qualitative methods. PGM collected data with assistance of a community health worker who helped with navigation and community introductions but did not conduct interviews. Field notes were taken during and immediately after each interview by PGM to document contextual details, non-verbal cues, and initial reflections; these notes were used to supplement audio recordings during analysis. Regarding prior relationships: PGM had no established relationship with participants before the study. The field assistant, being a community health worker, had professional familiarity with some households but was not involved in recruitment decisions or interviews to minimise bias. All interviews were conducted by PGM, who introduced herself as a researcher from the university.
Interviews were conducted in locations chosen by participants for their convenience and privacy, typically in their homesteads (either inside their houses or in shaded outdoor areas). Appointments were scheduled in advance through community leaders or during household visits for the quantitative survey. Interviews were conducted in Shona or English by the first author (PGM), who was trained and supervised by the second (PLM) and third authors (MYK). Each interview lasted between 10 and 15 min, was audio-recorded with participants’ consent, and was subsequently transcribed and translated for analysis. The interview guide (provided in Supplementary materials) was designed to efficiently explore key domains: knowledge about rabies, attitudes towards vaccination, economic considerations, accessibility issues, and cultural beliefs. The focussed nature of the inquiry allowed for meaningful data collection within this timeframe, and thematic saturation was achieved by the 10th interview, indicating that the depth and duration were adequate to capture the range of relevant perspectives.
Data Analysis
Quantitative data were analysed using Microsoft Excel 17 and Stata Version 26. 18 Descriptive statistics (frequencies, percentages) were calculated. Dog bite prevalence was calculated per 1000 population. A 2 × 2 contingency table and Fisher’s Exact Test were used to assess the association between dog vaccination status (vaccinated vs unvaccinated/unknown) and bite outcome (recovery vs death). Spatial data were analysed using QGIS 3.28 19 and ArcGIS Pro. 20 Spot maps visualised vaccination distribution, and the Getis-Ord Gi* statistic and Kernel Density Estimation (KDE) were used to identify hotspots and the density of unvaccinated dogs.
Qualitative data were analysed using reflexive thematic analysis following the six-phase framework described by Braun and Clarke. 21 This process involved: (1) familiarisation with the data through repeated reading of transcripts; (2) generating initial codes inductively from the data; (3) searching for themes by grouping related codes into sub-themes, then grouping sub-themes into major themes; (4) reviewing potential themes and subthemes against coded extracts and the entire dataset; (5) defining and naming final themes; and (6) producing the report with representative quotes. Coding was conducted manually by the first author (PGM), and themes were reviewed by second and third authors (PLM and MYK) to ensure consistency and credibility. Discrepancies were resolved through discussion until a consensus was reached. Representative quotes were selected to illustrate the identified themes; all participants are identified by codes (eg, K1_1) to maintain anonymity.
Results
Socio-Demographic Characteristics of Respondents
A total of 60 participants were included. The majority of respondents (28.3%) were in the 35 to 44-year age range. The sample comprised 55% males (n = 33) and 45% females (n = 27). The majority (63.3%) were married or cohabiting, and the most common education level was secondary school (41.7%). Subsistence farming was the main livelihood (38.3%), and over a third (35.0%) reported a monthly household income of USD 50 to 100, highlighting the economic constraints in the area. Most households (86.7%) owned at least 1 dog. Refer to Table 1.
Socio-Demographic Characteristics of Respondents (N = 60).

Dog Bites Prevalence and Outcomes
A review of records at Denhere Clinic (2020-2024) revealed a total of 588 dog bite cases, with only 61 (10.4%) involving vaccinated dogs (Table 2). During the intensive study period (January 2023-July 2024), 14 dog bite cases were recorded at the clinic. Of these, 3 cases (21.4%) involved vaccinated dogs, while 11 cases (78.6%) involved unvaccinated dogs or dogs of unknown vaccination status. Among the victims, 8 (57.1%) were children under 15, and 6 (42.9%) were adults. Four (28.6%) resulted in death, while 10 (71.4%) recovered. Among those who recovered, all received post-exposure prophylaxis (PEP) at the clinic; none were reported to have developed clinical symptoms of rabies. All fatalities occurred among individuals who presented to the clinic more than 48 h after the bite incident.
Dog Bite Cases and Suspected Rabies Cases Recorded (2020-2024).

Prevalence Rate and Association Analysis
Based on Denhere Clinic service population data (approx. 3220 residents), the annual dog bite prevalence rate was 4.35 per 1000 population. Table 3 shows the association between the vaccination status of the biting dog and the victim’s outcome. Fisher’s Exact Test indicated a statistically significant association between the vaccination status of the biting dog (vaccinated vs unvaccinated/unknown) and the victim outcome (recovery vs death; P = .04). The Odds Ratio (OR) was 4.2 (95% CI: 1.1-18.3), suggesting that victims bitten by unvaccinated or unknown-status dogs were 4.2 times more likely to die than those bitten by vaccinated dogs.
Association Between Dog Vaccination Status and Bite Outcome (N = 14).

Vaccination Coverage and Spatial Distribution
Spatial data from 200 owned dogs indicated that 115 (57.5%) were vaccinated, while 85 (42.5%) were not (Table 4). Mobile outreach campaigns accounted for the highest proportion of vaccinations (43.5%). Spatial analysis revealed uneven vaccination coverage, with peripheral zones significantly underserved compared to centrally located villages like Madzimure, Dungiro and Hwenga (Figure 2). Hotspot analysis (Getis-Ord Gi*) identified statistically significant clusters (P < .05) of unvaccinated dogs in peripheral areas of the ward (Figure 3). Kernel Density Estimation (KDE) further confirmed these areas as high-density zones for unvaccinated dogs (Figure 4). All GPS coordinates were collected from households within Ward 2; however, due to the mismatch between administrative boundaries and actual settlement patterns, some points may appear marginally outside the boundary line on the map while still representing Ward 2 residents.
Rabies Vaccination Coverage Among Dogs in Ward 2, Gutu (N = 200).


Spatial distribution of vaccinated and unvaccinated dogs in Ward 2.
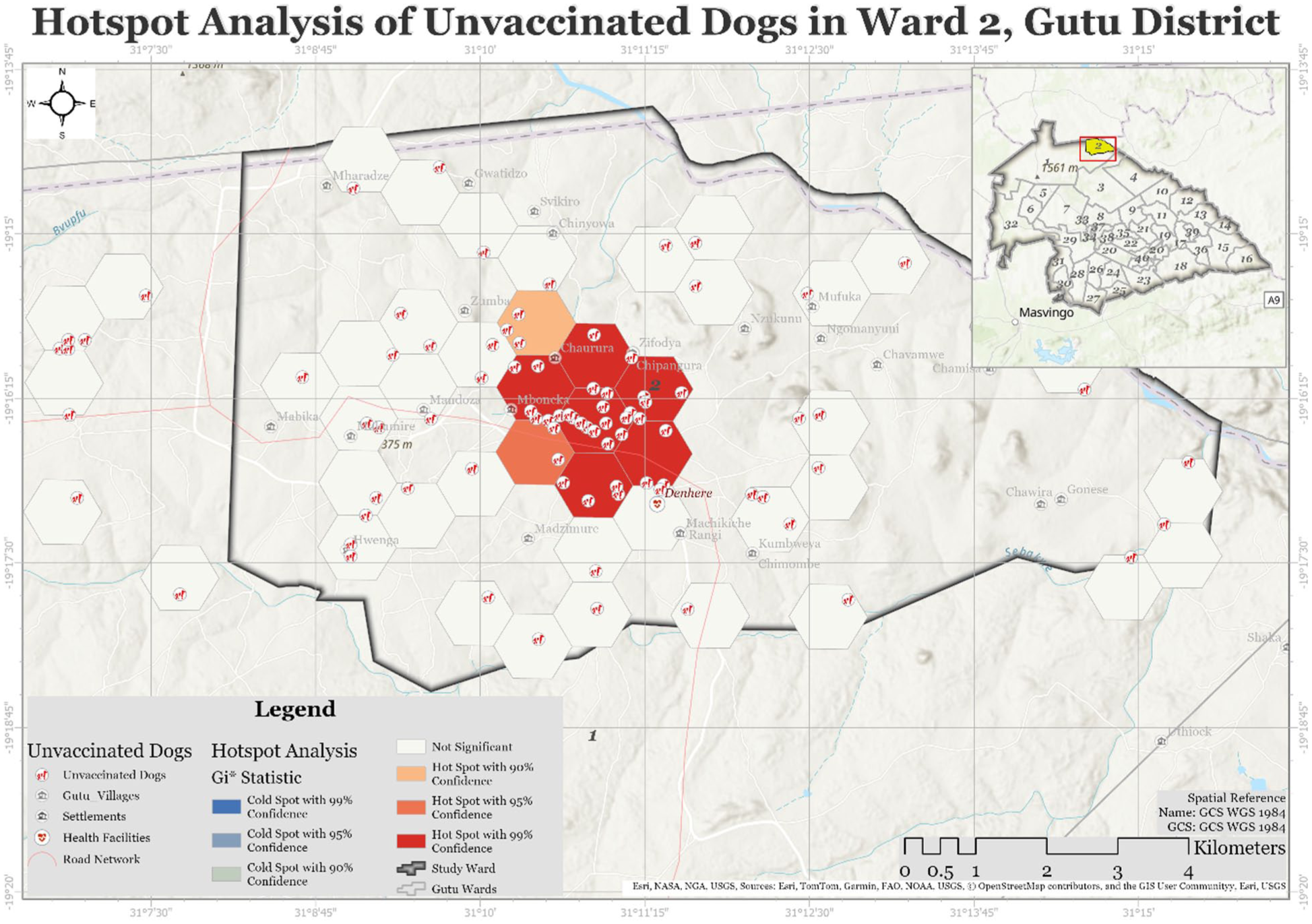
Spatial clustering of unvaccinated dogs in Ward 2.
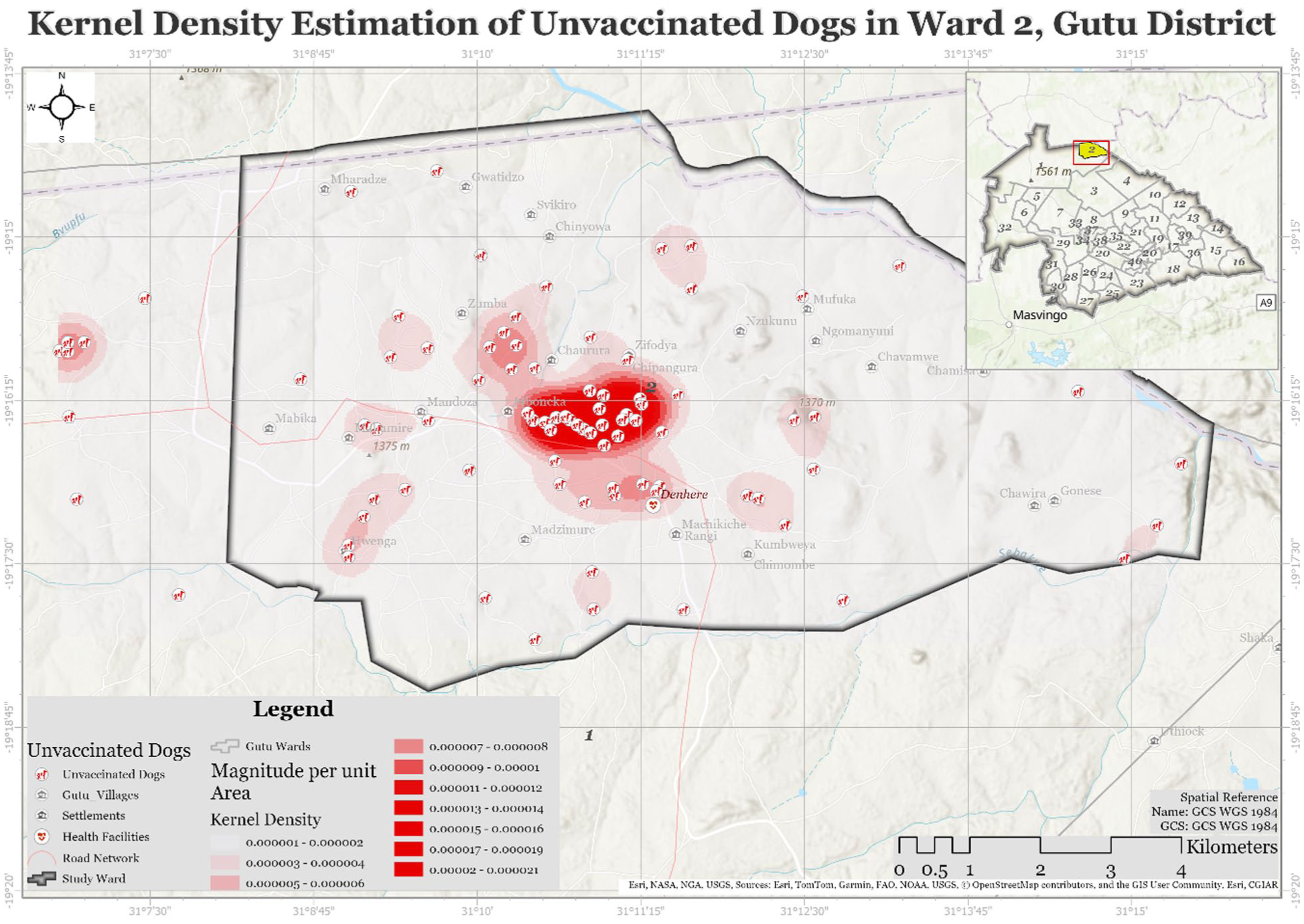
Heat map of the occurrence of unvaccinated dogs in Ward 2.
Qualitative Findings on Barriers to Vaccination
Thematic analysis of 10 key informant (Table 5) interviews identified 5 main themes: Financial Barriers, Knowledge Gaps, Cultural Beliefs, Accessibility Issues, and Communication Challenges (Table 6).
Interview Respondents’ Demographics.

Summary of Main Themes and Sub-Themes for Thematic Analysis.

Financial Barriers
Cost of vaccination and economic constraints
Several participants expressed concerns about the financial burden of vaccinating dogs, indicating that economic hardships create barriers to accessing veterinary services and prioritising animal health expenditures. This subtheme reflects a larger social trend where individuals with limited financial resources find it difficult to afford preventive healthcare for their animals, suggesting that economic constraints are linked to lower vaccination uptake. Participants indicated that vaccination of dogs is to be recognised as a fundamental right. This reflects participants’ considerations of the value of vaccination relative to other household expenses, suggesting that both affordability and perceived value influence decision-making.
‘I love my dog, but right now, the vaccination costs are just too high for me.’ K1_3 ‘Whenever I consider the expenses, I can’t help but question if it’s worth it in light of my other bills.’ K1_2 ‘It’s really painful to have to choose between my pet’s health and putting food on the table.’ K1_1 ‘When finances are tight, getting vaccines isn’t a top priority.’ K1_6 ‘I have to prioritise bills and groceries; my dog’s vaccinations can wait.’ K1_4 ‘It’s tough in this economy; I’m barely making ends meet as it is.’ K1_7
Lack of affordable veterinary services
Dog owners indicated that a lack of enough staff in the ward can also be a barrier that hinders them from vaccinating dogs. They cited that there is only 1 veterinary worker in the ward, the fees become unaffordable, therefore workforce is needed. The subtheme also reveals the geographical and financial challenges dog owners encounter.
‘There’s just one veterinarian in the area, and their fees are high.’ K1_4 ‘I wish there were more affordable care options available; it feels like a luxury.’ K1_2 ‘I can’t travel for hours to find a vet who won’t charge a fortune.’ K1_5
Knowledge Gaps
Lack of awareness about vaccination benefits
This subtheme highlights a gap in understanding the significance of vaccines, which leads to an undervaluation of vaccinations, highlighting the importance of educational outreach. There is a notable lack of understanding of the importance of vaccinations for dogs, leading to diminished perceived value of preventive measures. Participants admitted they did not realise the importance of vaccines in animal health until it was too late. Additionally, social circles contribute to this lack of awareness, as noted by one of the participants.
‘I didn’t understand how crucial vaccinations were until it was too late.’ K1_4 ‘Most of my friends are unaware of the dangers of not vaccinating.’ K1_8 ‘I thought my dog was healthy enough; I didn’t comprehend the necessity for shots.’ K1_9
Misconceptions about the vaccine
Misunderstanding about vaccine is a major problem for vaccination rates, as dog owners and key informants hold onto myths concerning vaccine safety and effectiveness. Also, they fear the potential side effects which impede their willingness to vaccinate their pets. This uncertainty is increased by societal myths questioning the necessity of the vaccine.
‘I heard that vaccines might cause more harm than good, which made me hesitant.’ K1_1 ‘There’s so much conflicting information out there; I was confused about what to believe.’ K1_5 ‘Some people claim vaccines are unnecessary, which made me question everything.’ K1_2
Little knowledge about the disease risk
Underestimating the severity of the disease by dog owners contributes to hesitancy regarding vaccinations. This subtheme suggests that educational initiatives should focus on the vaccine-preventable diseases which contribute to reluctance to vaccinate their pets, underscoring the need for educational initiatives to bridge these gaps.
‘I never thought my dog could catch anything serious; I assumed we were safe.’ K1_3 ‘Without witnessing the impact of these diseases, it’s difficult to feel concerned.’ K1_9 ‘I had no idea how prevalent these illnesses are; it’s frightening to think about now.’ K1_10
Cultural Beliefs
Cultural Attitudes About the Vaccine
Belief in traditional medicine can obstruct acceptance of medical practices. Narratives reveal a strong cultural identity that favours traditional remedies over vaccines, indicating that effective health interventions must take cultural contexts into account, need for culturally sensitive education and involve community leaders to build trust in vaccination.
‘In my community, we don’t trust vaccines; we depend on home remedies.’ K1_7 ‘Cultural beliefs significantly influence our perspective on pet health; changing that is challenging.’ K1_2 ‘I grew up believing vaccines are harmful; breaking that mindset is tough.’ K1_6
Traditional Practices and Beliefs
This subtheme indicates that traditional health practices can foster resistance to vaccination; it requires a respectful dialogue that honours traditional practices while offering evidence of vaccination benefits, promoting an integrated approach and reflecting the challenge of integrating modern veterinary practices with traditional views.
‘My family use herbs for treating pets; I never thought about vaccinations.’ K1_5 ‘I prefer natural remedies; vaccines just don’t align with my beliefs.’ K1_6 ‘Tradition is important to us, and vaccines feel unfamiliar and unnecessary.’ K1_9
Religious objections
Dog owners and key informants perceive vaccines as conflicting with their spiritual values, viewing them as a spiritual divine will. The preference for spiritual solutions over medical treatments is evident in 1 owner, suggesting a need for respectful dialogue that honours these values while promoting health.
‘My religion advises are against modern medicine; I feel wrong to vaccinate.’ K1_4 ‘I can’t betray my beliefs, even for the sake of my dog’s health.’ K1_1 ‘We value spiritual healing over medical treatments like vaccines.’ K1_7
Accessibility Issues
Access to a Veterinary Clinic
Distance to vaccination sites and time required to access services were reported as significant barriers. Participants living in rural and remote areas indicated that limited proximity to vaccination points, combined with the time needed to travel (often on foot or by donkey cart), made accessing veterinary services challenging, as indicated by 1 owner emphasising the barriers presented by distance and transportation. One owner expressed a need for improved access to services, highlighting the importance of addressing existing barriers to accessibility.
‘Getting to a vet is difficult; I can’t always find the time or means to go.’ K1_9 ‘If only there were more clinics nearby, I’d ensure my dog got vaccinated.’ K1_10 ‘It’s frustrating knowing help is available, but I can’t access it.’ K1_3
Availability of Vaccination Services
Dog owners indicated that insufficient availability of vaccination services in the ward contributes to low uptake. Participants expressed that limited information about the importance of vaccination, rather than just service unavailability, affected their decisions. Several noted that if they had fully understood the risks and consequences of not vaccinating, they would have prioritised it. The quotations reflect a need for not only more vaccination events but also clearer communication about why vaccination matters.
‘I just didn’t realise how important vaccinations were. If I had known, I wouldn’t have hesitated to get my dog vaccinated to avoid any risk.’ K1_8 ‘Nobody ever explained to me that not vaccinating my dog could lead to bites. I thought it was just a choice; I didn’t see the bigger picture.’ K1_6 ‘I wish the vet had been clearer about the consequences of skipping vaccinations. If I had understood better, I would have made a different decision for my dog’s health and safety.’ K1_3
Communication Challenges
Ineffective communication channels emerged as a barrier to vaccination uptake. Participants reported that information about vaccination campaigns often fails to reach them or arrives too late. This theme highlights the need for diversified communication strategies that reach remote households through multiple channels, including community gatherings, religious institutions, and direct village-level announcements.
‘We usually hear about the vaccination after it has already happened.’ K1_6 ‘The announcements are made at the business centre, but we live far from there and don’t always get the news.’ K1_8 ‘If they could tell us through the church or at village meetings, more people would know and bring their dogs.’ K1_3
Discussion
The study found that vaccination coverage in Ward 2 was 57.5% substantially below the World Health Organisation’s recommended threshold of 70% required to achieve herd immunity and prevent outbreaks. 2 The mixed-methods approach revealed that this low coverage results from multiple interacting factors; financial constraints, knowledge gaps, cultural beliefs, accessibility issues, and communication challenges. Spatial analysis identified significant clustering of unvaccinated dogs in peripheral areas of the ward, while quantitative analysis demonstrated a statistically significant association between bites from unvaccinated dogs and fatal outcomes. These findings align with documented challenges in sustaining high coverage in rural, resource-limited settings across sub-Saharan Africa.5,6,22
The suboptimal coverage likely stems from systemic issues within veterinary service delivery, including a lack of resources for large-scale campaigns, as has been noted in similar contexts. 22 Spatial analysis revealed a significant clustering of unvaccinated dogs in peripheral areas of the ward, a pattern associated with heightened outbreak risk. This pattern can be explained by the accessibility barriers reported in our qualitative findings: residents in these peripheral zones specifically cited distance to vaccination points and transportation difficulties as major obstacles. These areas are characterised by poor road networks, particularly challenging during the rainy season, and are the furthest from the fixed vaccination point at Denhere Clinic. This geographical inequity in coverage aligns with findings from other studies in rural Africa, where remote settlements consistently show lower vaccination uptake due to poor access to services.6,23 The study findings do not support inferences about dogs’ movement patterns; rather, the static GPS points indicate that unvaccinated dogs are concentrated in specific, underserved locations. This clustering creates persistent reservoirs of susceptibility. The implication is that achieving equitable coverage requires targeted outreach to these peripheral areas, not merely overall coverage targets. The proximity of these unvaccinated dog clusters to human settlements is a well-established risk factor for rabies transmission to humans, as highlighted in studies from the region.5,24 Furthermore, the presence of unvaccinated dogs poses a risk to the broader dog population, including vaccinated individuals whose immunity may wane over time, potentially facilitating renewed transmission cycles.3,25
The study reveals that these spatial clusters of unvaccinated dogs correspond precisely to the areas where qualitative respondents cited profound accessibility issues and financial constraints. This synergy, revealed through the convergent parallel design, powerfully pinpoints the populations most at risk and the multifaceted reasons behind low coverage. The integration of quantitative and qualitative findings demonstrates how mixed methods can provide a more comprehensive understanding than either approach alone. The strong association between bites from unvaccinated dogs and fatal outcomes in our case series, while based on a small sample, highlights the lethal consequences of these coverage gaps. This finding is consistent with the global evidence base demonstrating that dog vaccination is the most effective intervention for preventing human rabies deaths.3,25
The qualitative findings reveal that financial barriers are not merely about the absolute cost of vaccination but reflect deeper economic vulnerabilities in a subsistence farming community where cash is scarce, and household priorities compete. This economic context explains why even modest vaccination fees can be prohibitive, and why mobile outreach campaigns that provided free vaccination achieved the highest coverage (43.5%). Similarly, the knowledge gaps identified particularly the lack of awareness about disease risk and misconceptions about vaccine safety operate within a social context where informal information networks (friends, family) often substitute for formal health education, perpetuating myths and hesitancy.
The findings of this study must be understood within the broader Zimbabwean socio-economic context, characterised by persistent economic challenges, rural poverty, and a strained healthcare system. Zimbabwe has experienced prolonged economic instability, with high inflation and unemployment rates that disproportionately affect rural communities. 26 In Ward 2, this economic reality is reflected in our finding that 73.3% of respondents reported monthly household incomes below USD 100. Rabies exemplifies the characteristics of a neglected tropical disease (NTD): it affects impoverished populations with limited access to healthcare, receives insufficient attention and resources, and perpetuates cycles of poverty through preventable deaths and economic losses.2,3,25 The clustering of unvaccinated dogs in peripheral areas reflects broader patterns of health inequity in Zimbabwe, where geographic marginalisation compounds economic disadvantage to create pockets of vulnerability. Addressing rabies, therefore, requires not only veterinary interventions but also attention to the structural determinants of health that characterise NTDs.
The annual dog bite prevalence rate of 4.35 per 1000 population represents a substantial public health burden in this rural community. This rate is comparable to findings from other studies in sub-Saharan Africa27,28 but likely underestimates the true burden, as many bite victims, particularly in remote areas, may not present to health facilities due to access barriers. 3 The disproportionate impact on children (57.1% of cases during the intensive study period) is particularly concerning, as children are more likely to sustain severe bites (often to the head and neck) and may not report exposures promptly. This age-specific vulnerability, combined with the finding that 78.6% of biting dogs were unvaccinated, creates a high-risk situation for paediatric rabies deaths. The association between delayed presentation (>48 h) and fatal outcomes underscores the need for both improved access to post-exposure prophylaxis and community education on the urgency of seeking care after dog bites.
The spatial analysis revealed that peripheral areas of the ward had the highest concentrations of unvaccinated dogs, directly corresponding to areas where residents reported the greatest difficulties accessing veterinary services. This geographic inequity in service delivery reflects a common pattern in rural health systems, where fixed facilities are centrally located, and outreach services are infrequent or logistically challenging to sustain.22,29,30 The fact that mobile outreach campaigns accounted for the highest proportion of vaccinations (43.5%) demonstrates both the demand for and effectiveness of decentralised service delivery. However, the continued existence of unvaccinated clusters indicates that current outreach efforts are either insufficient in frequency, scope, or geographic coverage to reach all peripheral communities. These marginalised areas face a double burden: they are furthest from fixed facilities and may be last to receive outreach services due to poor road networks, particularly during rainy seasons when accessibility is further compromised.
The clustering of unvaccinated dogs in outlying zones has profound implications for rabies control and reflects the poverty-associated nature of the disease. These peripheral areas, characterised by lower incomes and poorer access to services, serve as potential reservoirs for rabies transmission. Unvaccinated dog clusters create spatial heterogeneity in herd immunity, meaning that even if overall coverage approaches the 70% threshold, pockets of susceptibility remain where outbreaks can ignite and spread. This spatial pattern perpetuates the cycle of rabies as a disease of poverty: impoverished communities with limited resources are least able to access preventive services, making them most vulnerable to outbreaks, which then impose additional economic burdens through healthcare costs and livestock losses.
The peripheral areas identified as hotspots for unvaccinated dogs in Ward 2 are also fringe areas that border communal lands and, in some cases, conservation areas where wildlife, including potential rabies reservoir species such as jackals and mongooses, may be present. While our study did not directly investigate wildlife-livestock interactions, the spatial overlap between unvaccinated dog clusters and these fringe zones raises important considerations for rabies ecology. In similar Zimbabwean rural settings, spillover events from wildlife to domestic dogs have been documented, particularly in areas where dogs roam freely and come into contact with wildlife (jackals) at the interface of human settlements and natural habitats. 5 Unvaccinated dogs in these fringe areas could serve as a bridge host, acquiring infection from wildlife and transmitting it to other dogs and humans in more densely populated areas. This potential for wildlife-domestic animal interaction underscores the importance of achieving high vaccination coverage not only in central areas but particularly in peripheral zones where ecological interfaces create additional transmission pathways.
The qualitative findings on barriers to vaccination align closely with established literature. The financial constraints cited by participants corroborate studies identifying cost as a primary deterrent to dog vaccination in rural Zimbabwe and similar low-income settings.5,29 Similarly, the profound knowledge gaps and misconceptions observed, particularly regarding rabies risk and vaccine safety, have been consistently documented as critical drivers of low uptake in Nigeria, 31 Peru 32 and Tanzania, 6 sometimes outweighing economic factors. Furthermore, the reliance on traditional remedies and cultural hesitancy reported here echoes findings from other regions of Zimbabwe 9 and Tanzania, 6 confirming these as deeply rooted, systemic challenges.
The communication challenges identified in this study, particularly the failure of information about vaccination campaigns to reach remote households, represent an underappreciated barrier in the literature.32,33 While many studies focus on knowledge, attitudes, and practices, few examine the communication infrastructure through which health information is disseminated. 33 Our findings suggest that even when communities are willing to vaccinate, they cannot act on this willingness if they do not receive timely information about when and where vaccination services are available.
These findings collectively demonstrate that effective interventions must extend beyond the mere provision of vaccines to actively address the underlying socio-cultural and economic landscape. This necessitates a shift from standardised campaigns to strategies that are co-developed with communities to build trust, dismantle misconceptions, and make vaccination both financially and logistically accessible. 33 The identified spatial hotspots represent priority targets for such tailored interventions, including mobile vaccination outreach.
Limitations
The household survey sample size was limited (n = 60), and the use of a 90% confidence level reduces the precision of estimates, potentially affecting the generalisability of findings. The bite outcome analysis is based on a small number of cases (n = 14) and should not be generalised beyond this context. The study was conducted in a single ward, limiting transferability to other settings with different socio-demographic or ecological characteristics. Fifteen dog locations could not be mapped due to accessibility issues (rough terrain, restricted access during rainy season), and GPS accuracy (±4 m) may introduce minor spatial error. Vaccination status was based on owner recall and clinic records, which may be subject to misclassification bias (recall bias for owners, incomplete records at the clinic).
The purposive sampling used in the qualitative component may introduce selection bias, as participants were not randomly selected but chosen based on specific criteria (community leaders, owners of unvaccinated dogs). While this approach was appropriate for exploring in-depth perspectives on barriers, it may not capture the full range of experiences within the community. Data on dog bites and suspected rabies cases were collected from only 1 primary care facility (Denhere Clinic). Given that respondents reported difficulties accessing care, it is likely that some bite cases, particularly in remote areas, never presented to this facility, potentially underestimating the true burden of dog bites and limiting the representativeness of clinical records. Cases presenting to traditional healers or those managed at home without formal healthcare contact would not be captured in our data.
Conclusion
This study found that low rabies vaccination coverage in Ward 2, Gutu, is determined by an interplay of behavioural, structural, and spatial factors. The mixed methods approach reveals not only the extent of low coverage but also the complex reasons behind it, including financial constraints, knowledge gaps, cultural beliefs, accessibility issues, and communication challenges. The spatial analysis identified peripheral areas as priority targets for intervention, while qualitative findings illuminated the lived experiences behind these patterns. The study identifies several areas requiring further research: (1) investigation of dog movement patterns and their role in rabies transmission between vaccinated and unvaccinated clusters; (2) exploration of wildlife-domestic dog interactions at the interface of fringe areas to assess spillover risk; (3) evaluation of different mobile outreach strategies to determine the most cost-effective approaches for reaching remote communities; (4) assessment of community-based education interventions that respectfully engage with cultural beliefs; and (5) longitudinal studies to track changes in vaccination coverage following targeted interventions. The findings illustrate Zimbabwe’s urgent need to decentralise and tailor rabies control strategies. While the sample size limits broad generalisation, the study findings offer locally relevant evidence to inform One Health strategies in similar rural African settings
Recommendations
Based on our findings and their interpretation, we propose the following recommendations. To address the spatial clustering of unvaccinated dogs in peripheral areas (Figures 2-4) and the accessibility barriers reported in qualitative interviews, health authorities should implement regular mobile vaccination outreach teams that specifically target remote communities, complementing fixed-point vaccination schedules at Denhere Clinic. Given the communication challenges identified, engagement with traditional leaders and use of diverse media, including village meetings, religious institutions, and local radio, should be strengthened to enhance public awareness and trust in vaccination programmes, ensuring that information reaches all households, not just those near central locations. In response to the knowledge gaps and misconceptions documented, culturally sensitive rabies awareness initiatives should be developed and sustained, respecting local beliefs while providing clear, accessible information about vaccine safety and the importance of timely post-exposure prophylaxis. To address the financial barriers identified, vaccination services should be provided free of charge or at highly subsidised rates, particularly in this low-income setting where 73.3% of households earn less than USD 100 monthly. Building on the association between delayed presentation and fatal outcomes, community education should emphasise the urgency of seeking care immediately after dog bites. Finally, to improve monitoring and evaluation, record-keeping practices at health clinics and veterinary departments should be strengthened, enabling better tracking of vaccination coverage, dog bite incidents, and outbreak detection, a need highlighted by the incomplete records encountered during data collection.
Supplemental Material
sj-doc-1-inq-10.1177_00469580261437011 – Supplemental material for Spatial and Behavioural Determinants of Low Rabies Vaccination Coverage Among Dogs in a Rural Zimbabwean Ward: A Mixed-Methods Study
Supplemental material, sj-doc-1-inq-10.1177_00469580261437011 for Spatial and Behavioural Determinants of Low Rabies Vaccination Coverage Among Dogs in a Rural Zimbabwean Ward: A Mixed-Methods Study by Priscillah Gamuchirai Mudzanire, Perez Livias Moyo and Methembe Yotamu Khozah in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580261437011 – Supplemental material for Spatial and Behavioural Determinants of Low Rabies Vaccination Coverage Among Dogs in a Rural Zimbabwean Ward: A Mixed-Methods Study
Supplemental material, sj-docx-2-inq-10.1177_00469580261437011 for Spatial and Behavioural Determinants of Low Rabies Vaccination Coverage Among Dogs in a Rural Zimbabwean Ward: A Mixed-Methods Study by Priscillah Gamuchirai Mudzanire, Perez Livias Moyo and Methembe Yotamu Khozah in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Author Note
PGM is a BSc Public Health student at the National University of Science and Technology in Zimbabwe. This paper was part of the research project that was a partial fulfilment of the BSc in Public Health. PLM and MYK are a Master of Science Degree in Environmental Health holders at the National University of Science and Technology in Zimbabwe. The Authors are both Lecturers in the Department of Environmental Health in the Faculty of Environmental Science at the National University of Science and Technology.
Ethical Considerations
Ethical approval was granted by the National University of Science and Technology Institutional Review Board (Ref: NUST/IRB/2025/64).
Consent to Participate
Informed consent was obtained from all participants. Confidentiality was assured, and participants were informed of their right to withdraw. For key informants, additional consent for audio recording was obtained.
Consent for Publication
An information sheet outlining the study’s purpose was provided to participants before they gave their consent to participate. Written consent was secured from all participants.
Author Contributions
PGM conceptualised the research idea and drafted the manuscript. PLM and MYK coordinated the manuscript writing process, guided the manuscript writing process and revised the draft manuscript. All the authors read and approved the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Attached as Supplemental File.
Supplemental Material
Supplemental material for this article is available online.