
Abstract
To meet the personalized needs of patients, VIP (Very Important Person) outpatient clinics, operating as a private practice, are an important option for non-local patients who often lack familiarity with medical procedures and seek efficient care within a limited timeframe. This study aimed to address 2 core questions: what are the distinct satisfaction classes among non-local patients, and what factors determine membership in these patterns? Accordingly, it sought to identify these latent subgroups and analyze their determinants. A cross-sectional study was conducted among 1961 non-local patients who attended the VIP outpatient clinic at a tertiary hospital between June and July 2025. Quantitative data were collected using a 5-point Likert scale designed to measure patient satisfaction. Based on the Structure-Process-Outcome (SPO) Model, latent class analysis (LCA) was performed to identify distinct satisfaction subgroups, and chi-square tests and multiple logistic regression were applied. Three latent classes were identified based on Mplus 8.4: high satisfaction (69.4%), high medical care, low environmental service (19.8%), and low medical professionalism–high non-technical quality (10.8%). 47.4% patients aged 0 to 44, and the majority of participants (71.3%) communicated with the doctor no more than 20 min. Multiple logistic regression indicated that age, length of communication with the doctor, waiting time before consultation, and whether the check up in the clinical laboratory or endoscopy center were the main associated factors (all P < .05). For different patient groups, these data suggest that tools, the psychological needs of younger patients, and training doctors in efficient communication techniques may improve patient acceptance of health care. Additionally, optimizing the environment in auxiliary examination departments to better accommodate nonclinical needs is recommended.
Keywords
Introduction
Satisfaction refers to a patient’s evaluation of their healthcare experience and is a critical health outcome within a patient-centered care framework. 1 As a key component of the healthcare system, outpatient satisfaction reflects patients’ perceptions of service effectiveness and hospital management and, by extension, significantly influences subsequent health-seeking behaviors, treatment adherence, and disease outcomes, making it a vital indicator for assessing the quality of outpatient care.2 -4 Internationally, outpatient systems are commonly categorized into general clinics, specialty clinics, emergency services, and concierge medicine that offers personalized private care.5,6 In China, this high-end personalized care is delivered through VIP (Very Important Person) outpatient services, a form of tailored healthcare approved by regulatory authorities to accommodate diverse patient needs based on clinical conditions.7,8 The concierge medicine model was pioneered in 1996 by MD2 International to provide premium and customized healthcare. Numerous international studies have been conducted on this model, with recent research confirming that patient satisfaction is a persistent key metric in concierge medicine, which is closely linked to trust in healthcare providers and willingness to continue treatment.9,10 Using model comparisons, Ko et al found that patients receiving concierge care reported higher satisfaction levels in nursing care, communication time with doctors, and shared decision making than those in general outpatient clinics. 11 Other studies have identified key determinants of satisfaction in concierge medicine: comfortable and private environments, positive service attitudes, and sufficient consultation time enhance it, whereas prolonged waits or referrals to mid-level providers (eg, physician assistants or nurses) can diminish it.9,12,13 In the United States, some hospitals have implemented standing notice boards displaying appointment wait times since 2018, with concierge staff providing verbal explanations for delays exceeding 30 min. 14 Concierge medicine has emerged in developed countries, whereas its Chinese equivalent, VIP outpatient services, is a recent development. Early forms emerged in the 1980s, when physicians were permitted to offer supplementary medical services beyond their primary duties. 15 In 1994, Minister of Health, Chen Minzhang, formally defined this model as “VIP outpatient” care. 16 In 2022, the State Council encouraged insurance institutions to collaborate with hospitals to provide VIP outpatient services and further boost their development of it. 17 Despite these developments, research on VIP outpatient services remains limited, particularly regarding patient satisfaction. Nevertheless, given the advantages of VIP services in terms of hospital revenue and meeting patient needs of different levels, the number of hospitals offering such services has been steadily increasing in recent years.6,18
As a domestic model for high-end personalized care, VIP outpatient services merit dedicated research on patient satisfaction within the broader context of outpatient satisfaction. In response to diverse patient needs, the Chinese National Health Commission has issued multiple guidelines emphasizing that major medical centers should adopt patient-oriented approaches to optimize service delivery, rationalize staff-patient ratios, and further refine the outpatient care system.19,20 VIP outpatient services are designed to meet the demands of patients with higher expectations for healthcare, among whom a considerable proportion are non-local patients seeking medical care outside their residential area. These patients often encounter challenges such as time constraints, complex healthcare pathways, and overcrowding in general clinics; consequently, their primary needs include efficient, convenient access to care and complete procedures quickly at designated auxiliary examination departments, such as clinical laboratories, to enhance overall efficiency.6,21,22 Given the substantial time and efficiency concerns associated with long-distance travel, many patients are willing to incur higher costs for VIP outpatient services to gain access to personalized, high-end healthcare tailored to their needs. 22
To address the needs of non-local patients in VIP outpatient care, this study employs latent class analysis (LCA) to identify distinct satisfaction subgroups and examine their determinants. The analysis is guided by the Structure-Process-Outcome (SPO) model, a foundational framework for evaluating medical experience and service quality. According to the SPO model, well-designed processes may directly enhance outcomes, while sound structures may contribute to outcomes by facilitating effective care delivery. 23 Within this framework, structure encompasses the tangible and organizational foundations necessary for healthcare provision, reflecting what a facility has in place to deliver care. 24 This includes physical environment, medical equipment, and staff qualifications. 23 Process captures the dynamic interactions between patients and doctors during medical care, such as diagnostic accuracy, communication quality, and management of workflow, illustrating how care is individualized. 25 Outcome refers to the resulting changes in a patient’s health status and experience, and serves as the ultimate indicator of service effectiveness, including clinical improvement, mortality rates, and patient satisfaction. 24 These definitions offer conceptual clarity, enabling the effective deployment of the SPO model in practice. It is well-aligned with the objectives of our study, which serves to identify latent subgroups in satisfaction and their distinguishing factors among non-local VIP outpatients. For instance, key variables are corresponding to the SPO dimensions: environment of auxiliary examination departments represents the “structure”; waiting time and length of communication with the doctor relate to the “process”; and overall satisfaction constitutes the “outcome.” Accordingly, this alignment provides a coherent theoretical lens for data analysis. By grounding the analysis in the SPO framework, our study explores how structural and process factors differentially influence satisfaction across distinct patient subgroups, thereby offering new empirical evidence in support of this established theoretical perspective.
While existing studies have identified broad determinants of satisfaction (eg, sociodemographic characteristics, core healthcare process, and satisfaction evaluation system of medical experience), they predominantly rely on conventional analytical methods such as correlation and regression analyses. These approaches implicitly assume patient populations are homogeneous, thereby overlooking potential heterogeneity in satisfaction subgroups among non-local patients. Therefore, to better address differentiated needs, this study is guided by the following research question: what are the distinct latent classes of satisfaction among non-local patients in VIP outpatient settings, and what key factors determine class membership? It aimed to: (1) identify distinct latent classes of satisfaction among non-local patients using VIP outpatient services via LCA; and (2) explore the factors influencing each subgroup, thereby providing a precise basis for policy-making and service quality improvement to enhance satisfaction among non-local patients. The methodological approach of this study centers on LCA, a statistical technique that goes beyond analyzing variable associations to classify patient populations into distinct subgroups for targeted investigation. Accordingly, this study makes 3 key contributions: (1) it shifts the focus of patient population research toward identifying latent classes, thereby enabling a more nuanced analysis of satisfaction; (2) it highlights the scarcity of existing studies that apply LCA specifically to satisfaction among VIP outpatient and non-local patient populations; (3) by applying the SPO model to the context of non-local VIP outpatients, our study extends its scope of application and strengthens its analytical relevance; and (4) it proposes actionable service improvement strategies based on an analysis of the factors that influence satisfaction across different patient subgroups.
Material and Methods
Data and Sample
Based on the platform of a Chinese online survey platform similar to Amazon Mechanical Turk, using a convenience sampling method and consecutively recruiting participants for our survey, we conducted a cross-sectional study from June to July, 2025 at the VIP outpatient of a tertiary hospital to assess patient satisfaction among non-local patients. Based on the inclusion criteria, each patient (1) provided written informed consent and was willing to be investigated, (2) was admitted to a VIP outpatient, and (3) was in a stable condition. We excluded patients who (1) were emergency and/or (2) had an infectious disease. Upon on-site verification of VIP outpatient visit credentials (eg, appointment slips or booking records) and confirmation of eligibility, participants were directed to scan a QR code using their personal mobile devices to access a structured electronic questionnaire developed via the “Wenjuanxing” platform. The initial section of the questionnaire presented a digital informed consent form, which summarized the study background, objectives, and voluntary nature of participation. Access to the survey items was restricted until respondents had read and selected the “I understand the purpose of this survey and voluntarily agree to participate” option.
Under the face-to-face supervision of researchers, a series of technical and procedural safeguards were applied sequentially during data collection to secure a high-quality dataset: (1) The survey platform was configured to restrict submissions to 1 response per device/IP address, thereby preventing duplicate entries from individual participants. (2) Two attention-check items were embedded within the questionnaire (eg, “For quality control, please select ‘Very satisfied’”), and 31 responses that failed either of these checks were systematically excluded. (3) We removed submissions with implausibly short completion times (less than 45 s), as these were deemed unlikely to reflect considered patient feedback, thereby excluding 41 responses. Collectively, these sequential filters helped ensure the reliability of the data and supported the robustness of the findings. From the 2033 distributed questionnaires, we successfully collected 1961 questionnaires, yielding a high response rate of 96.46%.
This study was designed, conducted, and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies. 26 A completed STROBE checklist is provided as Supplemental Material 1.
Measures
Questionnaire Development and Adaptation
Building on previous studies, the items were adapted by integrating expert opinions with existing questionnaires in this area. It consists of 30 items across 3 dimensions: demographic characteristics, core healthcare processes, and satisfaction evaluation systems for medical experience. The inclusion of demographic characteristics as control variables was grounded in the established evidence from existing studies regarding the determinants such as age, gender, and education status on patient satisfaction. 27 The constructs within the core healthcare processes were informed by patient satisfaction assessment instruments, such as the Indian NIOPDSS scale and the Greek outpatient satisfaction questionnaire.28,29 In these studies, waiting time was recognized as a significant predictor of both healthcare efficiency and satisfaction, while the length of doctor-patient communication served as a key interactive indicator, and departmental examinations were consistently identified as important components. The satisfaction evaluation system for medical experience aligned with the classic 3-part classification of medical service satisfaction. Building on modifications and refinements derived from the aforementioned questionnaires, and to enable a more precise assessment of satisfaction with specific doctor behaviors including diagnosis, explanation, and respect for privacy, explicit reference was made to the dimension of the EUROPEP instrument and the medical communication dimension of the PSQ-18.28 -31
In addition to directly employing well-validated, internationally published instruments, we also adapted and refined certain items pertaining to the “core medical processes” to better accommodate the context of the VIP outpatient and the circumstances of non-local patients. Given the time constraints among this population, we deconstructed the broad construct of “efficiency of examination” into specific and observable departmental interactions within the VIP outpatient setting. The newly developed items primarily address 2 aspects: (1) incorporating patient behaviors related to payment and medicine purchase, and (2) specifying examination departments such as the clinical laboratory, medical imaging department, ultrasound department, nuclear medicine department, and endoscopy center. This adaptation process ensured that the questionnaire comprehensively captures the specific workflows experienced by non-local patients in VIP outpatient, thereby enhancing the content validity of this study. To ensure the clarity and contextual suitability of the adapted items for non-local patients receiving VIP outpatient service, the revised instrument underwent an internal review by a multidisciplinary team. This team included 5 clinical staff and researchers with medical experience in outpatient settings and expertise in patient satisfaction research. To ensure linguistic clarity and cultural appropriateness for the local context, the questionnaire items derived from English originals (eg, the Indian NIOPDSS scale and the Greek outpatient satisfaction questionnaire) were translated into Chinese through a process of cross-cultural adaptation conducted by bilingual researchers. Furthermore, a pilot test was conducted with a small sample of patients (n = 15) to evaluate item clarity and relevance.
In the interest of transparency, an English version of the full questionnaire in our study is available in Supplemental Material 2. And the original questionnaire (Chinese version) is provided in Supplemental Material 3.
Assessment of Scale Properties
The overall scale demonstrated excellent internal consistency, with a Cronbach’s alpha coefficient of .969. The KMO measure was 0.963 and the χ2 value of Bartlett’s test of sphericity was 671 792.782 (P < 0.001), indicating high consistency of the questionnaire and the connection of those items. Furthermore, the 3 subscales also showed high reliability: the Cronbach’s alpha coefficients were .915 for the doctor–patient interaction subscale (8 items), .915 for nursing care (3 items), and .910 for environment services (5 items).
To examine the structural validity of the scale, we performed an exploratory factor analysis (EFA) using principal component analysis with Varimax rotation. The analysis extracted a 3-factor structure: (1) doctor–patient interaction, (2) nursing care, and (3) environment service, which collectively explained 60.88% of the total variance. As presented in Supplemental Material 4, all items loaded significantly onto their intended theoretical dimensions, with factor loadings exceeding 0.5 for each corresponding subscale, thereby supporting the instrument’s structure.
Variables and Scoring
The questionnaire data were scored in reverse (eg, waiting time) to unify the direction of data interpretation and ensure consistency of the analysis results. The demographic measures included sex, age, and educational status. There were 2 categories of sex: 1 = female and 0 = male. Age was a continuous variable in years, and this variable was pre-processed (unit: years): 0 to 44 = 0; 45 to 59 = 1; ≥60 = 2. Educational status was an ordinal variable with 3 levels: 0 = high school and below, 1 = undergraduate/junior college, and 2 = postgraduate and above. The core healthcare process includes service flow and departmental examination. The payment method, waiting time, and face-to-face communication were subtypes of the former. Payment method: 0 = no medical insurance; 1 = medical insurance. Waiting time was an indicator of medical efficiency (min): >60 = 0; 31 to 60 = 1; ≤30 = 2. The length of communication was a continuous variable (units: minutes): ≤20 = 0, >20 = 1. For the departmental examination, the respondents were asked if they made a payment or bought medicine in the outpatient clinic or checked up in the clinical laboratory, medical imaging department, ultrasound department, nuclear medicine department, or endoscopy center (no = 0, yes = 1).
The satisfaction evaluation system of medical experience comprised 16 items across 3 subscales: doctor-patient interaction (1-8), nursing care (9-11), and environment service (12-16), including: (1) overall satisfaction with waiting time, (2) satisfaction with behavior of treating doctor, (3) doctor explained your treatment and respect privacy, (4) doctor gave some guidance and materials, (5) doctor diagnosed diseases, (6) doctor explained why and how to use medicine, (7) doctor advised the examination and treatment plan, (8) doctor informed follow-up arrangements, (9) satisfaction with nurses’ behavior, (10) nurses listened to your questions and problems, (11) nurses answered the questions correctly, (12) satisfaction with hospital services and hospital staff, (13) satisfaction with responsiveness of your needs, (14) satisfaction with outpatient environment, (15) satisfaction with outpatient guideposts, and (16) satisfaction with hygiene situation of the toilet. Finally, a conclusive rating item is included: “Overall satisfaction of the outpatient visit.” The satisfaction items were rated on a 5-point Likert scale ranging from 1 (“very dissatisfied”) to 5 (“very satisfied”). After reverse-scoring the negatively phrased items, higher scores consistently indicated higher satisfaction across all items. For analysis, subscale scores were computed as the mean of the items within each dimension, and a total satisfaction score was calculated as the mean of all satisfaction items.
Analytical Strategy
First, a descriptive analysis was conducted to determine respondents’ characteristics of the 1961 respondents. LCA was performed to identify subgroups of patients based on patient satisfaction. Additionally, chi-square tests were applied to examine the determinants of categorical membership, and multivariate logistic regression analysis was conducted to validate satisfaction and its influencing factors in non-local patients.
Statistical Analysis
For categorical variables, descriptive statistics are presented as frequencies (percentages). All analyses were conducted using SPSS 27.0 and Mplus 8.4. 32 LCA is a widely used statistical approach that classifies individuals into distinct latent subgroups based on their responses to observed variables, thereby capturing population heterogeneity, identifying relevant influencing factors, and yielding accurate results. 33 The goodness-of-fit indices were based on the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), adjusted Bayesian Information Criterion (aBIC), Entropy, Lo-Mendell-Rubin likelihood ratio test (LMR), and bootstrap likelihood ratio test (BLRT). Lower AIC, BIC, and aBIC values indicate better model fit. Entropy reflects the classification accuracy, ranging from 0 to 1 values ≥0.8 represents >90% classification accuracy, and values closer to 1 indicate a near-perfect classification. LMR and BLRT were used to evaluate the differences between competing models. Differences were considered statistically significant at P < .05.
Quality Control
Five researchers were involved in the data collection process and all research members were requested to receive unified training before conducting the survey. Prior to the questionnaire, participants were briefed on the study details and provided informed consent ahead of the formal items. Participants were assured of the confidentiality of their data and the protection of their privacy. Certain variables were categorized based on established literature. For example, in accordance with a UK standard recommending that optimal waiting time should not exceed 30 min, 34 thus the variable “waiting time before consultation” was grouped with 30 as the boundary.
Results
Demographic Characteristics of Medical Traveler in VIP Outpatient
A total of 1961 non-local patients were included in this study (Table 1). Of the participants, 51.1% were female. Nearly half of the participants were aged 0 to 44 (47.4%) and had an undergraduate or junior college degree (57.0%). Most participants (69.0%) did not have health insurance and communicated with doctors for no more than 20 min (71.3%). A total of 42.1% reported waiting for less than 30 min before consultation. The majority of participants (94.8%) were satisfied with their waiting times.
Descriptive Characteristics of the Respondents (n = 1961).
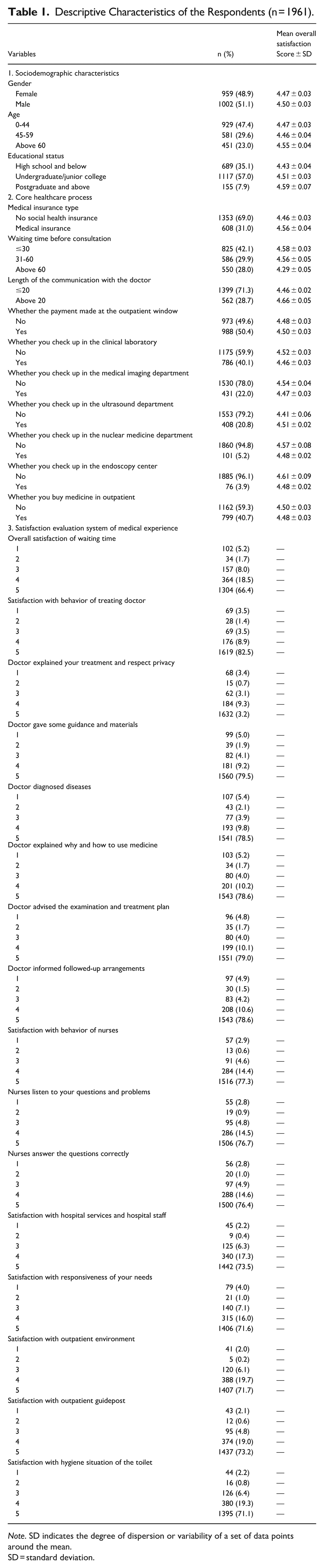
Note. SD indicates the degree of dispersion or variability of a set of data points around the mean.
SD = standard deviation.
Latent Class Analysis of Satisfaction Among Non-local Patients in VIP Outpatient
LCA was employed to analyze VIP outpatient services among non-local patients. Starting with a 1-class model, we incrementally increased the number of latent classes, ultimately testing 5 candidate models (see Supplemental Material 5). The results indicated that the 3-class solution demonstrated balanced class probabilities, high BIC values, and an entropy value of 0.986, reflecting high classification accuracy and excellent overall model fit. In contrast, models with more than 3 classes not only yielded a non-significant LMRT (P > .05) but also included classes with probabilities below 10%, along with a decreased BIC. Therefore, the 3-class model was selected as the optimal solution, and the proportions of the 3 latent classes were 19.8%, 10.8%, and 69.4%, respectively.
Figure 1 shows that the overall satisfaction of non-local patients among VIP outpatients can be divided into 3 categories. There were 389 patients in the first category (middle line in Figure 1), accounting for 19.8% of the total patients. The satisfaction level of this group is generally high in terms of the doctor-patient interaction dimension on a 5-point Likert scale, while the conditional probability of nurse services, outpatient environment, guidepost, and response to complaints are at a lower rate. Therefore, this category was named the “High doctor-patient interaction - Low non-clinical service group” (Class 1). There were 212 patients in the third category (bottom line in Figure 1), accounting for 10.8% of the total. This group had the lowest conditional probability in the dimension of doctor-patient interaction in the questionnaire, but higher satisfaction with supportive services, such as nurse-patient communication, outpatient environment, and response to complaints. Thus, this category was named the “Low doctor-patient interaction-High non-clinical service group” (Class 2). There were 1360 patients in the third category (top line in Figure 1), accounting for 69.4% of the total. All the item scores of the respondents were the highest, suggesting that the level of overall satisfaction of these patients was high. Hence, this category is named the “High satisfaction group” (Class 3).

Three-category latent class analysis of non-local patients’ satisfaction in VIP outpatient.
Univariate Factors of Non-local Patients’ Satisfaction in VIP Outpatient
Table 2 shows that there were statistically significant differences (P < .01) among the age, medical insurance type, waiting time before consultation, length of the communication with the doctor, whether the payment made at the outpatient window, whether you check up in the clinical laboratory, whether you check up in the endoscopy center.
Univariate Analysis of Latent Class Analysis of Non-local Patients’ Satisfaction in VIP Outpatient (n = 1961).

Note. C1, High doctor-patient interaction, low non-clinical service group (Class 1). C2, Low doctor-patient interaction-high non-clinical service group (Class 2). C3, High-satisfaction group (Class 3).
Multivariate Factors of Non-local Patients’ Satisfaction in VIP Outpatient
Taking the 3 sub-types of non-local patients’ satisfaction in VIP Outpatient as the dependent variable, the variables with statistically significant differences in the chi-square test (P < .05) were applied as independent variables for multivariate logistic regression. The assignments of the independent variables are presented in Supplemental Material 6.
Considering Class 3 as the reference, Table 3 presents the results of multivariate logistic regression analysis. For Class 1 (High doctor-patient interaction, Low non-clinical service group): compared to patients in the high-satisfaction group, patients who communicated with their doctor for more than 20 min were 2.12 times more likely to belong to Class 1 (aOR = 2.121, 95% CI: 1.608-2.797). Conversely, younger patients (aged 0-44 years) were less likely to be in Class 1 than those aged 60 and above (aOR = 0.732, 95% CI: 0.542-0.987). Longer waiting times also significantly reduced the odds of being in Class 1 relative to waiting 30 min or less (31-60 min: aOR = 0.695, 95% CI: 0.518-0.933; >60 min: aOR = 0.542, 95% CI: 0.410-0.716). Furthermore, patients who underwent examinations in the endoscopy center were less likely to be classified into Class 1 compared to those who did not (aOR = 0.467, 95% CI: 0.279-0.781). For Class 2 (Low doctor-patient interaction, High non-clinical service group): patients with communication durations exceeding 20 min were 4.09 times more likely to fall into Class 2 than into the high-satisfaction group (aOR = 4.087, 95% CI: 2.603-6.416). Additionally, having an examination in the clinical laboratory was associated with increased likelihood of belonging to Class 2 (aOR = 1.559, 95% CI: 1.121-2.166). Similar to Class 1, longer waiting times served as protective factors against membership in Class 2 (31-60 min: aOR = 0.559, 95% CI: 0.386-0.809; >60 min: aOR = 0.378, 95% CI: 0.266-0.538).
Associated Factors of Non-local Patients’ Satisfaction in VIP Outpatient: a Multivariate Logistic Regression Analysis (n = 1961).

SE = standard error; OR = odds ratio; CI = confidence interval.
Discussion
This study sought to uncover latent satisfaction classes among non-local VIP outpatients and identify factors differentiating these subgroups. Using the first-hand data, we identified 3 distinct latent classes of patient satisfaction: high satisfaction; high doctor-patient interaction, low non-clinical service that valued doctor services but lower support service; and low doctor-patient interaction–high non-clinical service with the lowest level of satisfaction with doctors’ behavior but non-technical quality. Although 69.4% of patients fell into the high-satisfaction group, 2 noteworthy profiles were identified that revealed notable differences in doctor-patient interaction and non-clinical service among the classes with respect to age, waiting time, length of communication with doctors, and environment. Grounded in the SPO model, this study advances our understanding of satisfaction dynamics within VIP outpatient services for non-local patients.
Waiting time, a key “process” factor defined as the duration patients spend queuing prior to consultation or treatment in VIP outpatient settings, is significantly linked to medical interactions (the “outcome”). Contrary to previous studies,35,36 an interesting finding of this study was that a longer waiting time significantly improved doctor-patient interactions. This is similar to research findings from America 37 and Ireland 38 and challenges the conventional view that shorter waiting times invariably lead to higher satisfaction, which has dominated recent discourse. Such counterintuitive findings are rarely reported; however, they can be explained through the unique context of our study population: non-local patients in VIP outpatient settings. The key drivers can be attributed to the following 3 factors. First, differed priorities among non-local patients in VIP outpatient settings. This prioritization stems from a deliberate decision-making process wherein non-local patients often elect to travel for health service based on local reputation, specialized clinical expertise, and anticipated therapeutic efficacy. 39 Given the substantial investment of time, finances, and personal effort involved in seeking medical care, and compounded by the premium cost of VIP services, non-local patients reasonably expect higher standards of disease treatment and clinical excellence. 40 This is consistent with the findings from a face-to-face interview. 41 Therefore, compared to the cognitively and physically undemanding act of waiting, many patients seeking high-level medical care are willing to tolerate longer waits if the perceived benefits such as receiving thorough psychological support or doctor-patient communication outweigh the negative emotions like anxiety and worry during the wait. 42 Parallel findings have also been reported in other sectors, including customer behavior in amusement parks. 43 Furthermore, this perspective extends beyond merely enduring a prolonged wait. To some extent, when non-local patients perceive that their substantial investment in VIP outpatient settings is nearing its clinical goal, the resulting sense of reassurance may help offset the monotony characteristic of lengthy waiting periods. A well-supported explanation points to a moderating effect of care quality perception, as suggested by Ko et al. 44 Their study, employing an algorithmic probability model, revealed a more nuanced relationship: the perceived importance of a doctor’s interpersonal and technical qualities can moderate the impact of waiting time on satisfaction. This challenges the oversimplified assumption that shorter waits invariably lead to higher satisfaction. 44 Here, interpersonal quality refers to the dynamics of the doctor-patient relationship, including attributes such as communication and manner, while technical quality denotes the specialization or professional competence of a service provider. 45 Second, professional support is delivered by the well-trained medical staff throughout the patient journey in VIP outpatient settings. As a form of premium medical care, a possible explanation is that patients who seek treatment in VIP outpatients could receive staff assistance to help divert their attention or have the opportunity to reschedule their appointments during visits, thereby sustaining the motivation to interact with doctors. 14 Additionally, it may also enable non-local patients to perceive their intrinsic worth as individuals in VIP outpatient settings, thereby mitigating frustration, enhancing the tolerability of waiting periods, and diminishing the propensity for dissatisfaction. A survey conducted in the United States on service quality improvement in VIP outpatient settings further corroborates this view. 14 Third, individual differences among non-local patients should be considered as well. For instance, the negative effect of waiting time on satisfaction is less pronounced or invalid among patients prioritizing technical quality, whereas it is more substantial among those emphasizing interpersonal quality. 44 One study also found that variations in patients’ cognition, prior experiences, and personality traits might lead to significant differences in their tolerance and prioritization of health concerns. 46 Nevertheless, the observed protective effect of waiting time should not discourage efforts to improve medical efficiency in healthcare settings and more in-depth research is required to explore the correlation between them. Intelligent appointments or real-time queuing systems must be implemented to minimize excessively long waiting times. In addition, screens, brochures, and interactive tools can be employed for patient education during waiting periods, which may help to sustain patients’ willingness to continue waiting and promote more effective communication with healthcare providers.
Another influential factor in subgroup analyses of patient satisfaction is the length of communication with the doctor, typically regarded as a component of the “process” dimension within the SPO framework, which is often closely associated with perceived efficiency. 47 Contrary to the conventional assumption that longer communication inherently enhances satisfaction, 48 our findings reveal a more complex relationship. Specifically, compared to highly satisfied patients, communication with doctors exceeding 20 min negatively impact 2 distinct patient subgroups: those who place high importance on doctor-patient interaction (Class 1) and those who prioritize non-clinical service (Class 2). Given the differing underlying mechanisms, these subgroups warrant separate analysis. For Class 1, overly extended communication may represent an inefficient form of interaction for non-local patients, diverting time and attention from non-clinical services and thereby potentially amplifying their dissatisfaction with VIP outpatient service. In Class 2, prolonged communication signal that patient expectations remain unmet despite repeated medical exchanges, or that critical clinical concerns are not being resolved in a timely manner. This indicates that the doctor–patient interaction does not align with their elevated expectations regarding both interpersonal communication and professional competence. Consequently, communication duration alone does not directly predict perceived care quality; rather, satisfaction outcomes are significantly influenced by service delivery and patient expectations. Therefore, merely extending communication time is inadequate; enhancing the efficiency and quality of interactions is critical to addressing the heterogeneous needs of diverse non-local patient subgroups. Previous studies have demonstrated that implementing the 5S management model, an efficient management method aimed at improving work efficiency among pharmacy staff, can enhance patients’ overall satisfaction and willingness to engage with healthcare providers. 49 Such approaches can elevate patient acceptance and satisfaction with patient-provider interaction. 50 This implies that achieving high consultation efficiency without the need for extra time for lengthy explanations may lead to satisfactory healthcare interaction, pointing toward a promising direction for continuous improvement in medical processes. Therefore, it is imperative for healthcare systems to pay attention to the psychological needs of different age groups and prioritize training doctors in efficient communication strategies to ensure effective transmission of essential information during time-constrained consultations for non-local patients.
Compared to patients in the high-satisfaction group, age may serve as critical factors for those who value doctor-patient interaction services. Aligning with previous studies suggesting that patients of different demographic backgrounds prioritize different aspects of care,51,52 we found that younger patients place greater importance on doctor - patient interaction. This observation is supported by the work of Lilly et al 53 and her colleagues, who allowed young and elderly patients to utilize a scoring table to assess 21 doctor behaviors, such as explanation, privacy protection, and guidance, and found that communication and professional competence were particularly important among younger patients. An earlier study conducted in northern India also highlighted the growing interest of young people in healthcare relationship. 54 Therefore, young patients represent an important population that prioritizes doctor-patient interaction as well.
Compared to patients in the high-satisfaction group, the auxiliary examination department environments, such as clinical laboratory, emerged as a critical determinant for patients who prioritize non-clinical services. This finding aligns with the SPO model’s emphasis on how “structure” fundamentally shapes satisfaction outcomes. It was confirmed by Mwebesa 55 and Lee et al, 56 whose studies identified a satisfactory environment as a key predictor of nontherapeutic services. Previous research has also shown that when doctors focus solely on treatment without ensuring a structured and predictable patient experience, patients’ visit-specific expectations may decline, leading to reduced satisfaction owing to unmet psychological needs. 57 This emphasis on the examination environment can be further understood through the lens of heightened patient expectations. Given this context, a comprehensive analysis of environmental management barriers in auxiliary examination departments is essential to effectively address patient needs and expectations. First, operational bottlenecks may directly affect the medical experience of non-local patients in VIP outpatient clinics. Despite the streamlined processes, auxiliary examination departments inevitably function as high-demand shared resources across the healthcare system, and this is a structural necessity. Combined with complex preparation requirements and strict scheduling, these bottlenecks exacerbate the burden on inherently time-constrained non-local patients. Such inefficiencies contradict their expectations for efficient, high-quality care, thereby fostering frustration and dissatisfaction. Second, environmental or workflow challenges cannot be ignored. Unfamiliarity with hospital layouts and procedures commonly leads to disorientation, especially for non-local patients in large, complex auxiliary examination departments. Additionally, unclear or misleading signage, overcrowded waiting areas, and insufficient privacy protections culminate in an unsupportive patient environment. 58 These issues are particularly acute and salient in VIP outpatient settings that are premised on delivering premium service, a context that directly contradicts the elevated expectations held by paying non-local patients. Finally, foremost among the influencing factors are the distinct navigation needs of non-local patients. Unlike local patients, non-local patients are constrained by distance and financial considerations, necessitating the consolidation of multiple health concerns into a single, condensed visit. The prolonged wait times associated with auxiliary examinations, driven by issues like unclear preparation instructions and long waiting periods for results, may disproportionately undermine overall visit efficiency. 59 Conversely, effective informational guidance coupled with well-coordinated services in auxiliary examination departments could foster an optimal care experience for non-local patients. In conclusion, identifying these clinical bottlenecks, procedural inefficiencies, and navigation barriers is central to meeting non-local patients’ expectations, enhancing the service’s value proposition, and ensuring the sustainable development of the VIP outpatient model.
Limitation
Because this study used a cross-sectional design, we could only deduce the correlations among these factors rather than establish causal relationships. Additionally, the use of a convenience sampling method may introduce selection bias, as it may not fully represent the medical experience of all non-local patients receiving VIP outpatient services. Furthermore, the sample was drawn from a single healthcare setting within a specific geographic region, which may not accurately represent the satisfaction levels of non-local patients in other regions. Finally, although this study explored factors as impact factors (ie, age, gender, medical insurance type, and length of communication with the doctor), some relevant factors or special factors such as stereotypes and cognitive or contextual influences were not considered in this study and could be worthy of future investigation. For instance, patients may face unfamiliarity with local hospital procedures or hold heightened expectations due to the higher cost of VIP services, all of which may substantially influence their perception of satisfaction. To enhance the generalizability and validity of these findings, future studies should be conducted on a larger, nationwide scale, considering these additional factors by incorporating qualitative interviews and examine their underlying mechanisms to provide a more comprehensive understanding of satisfaction among non-local patients within different organizational environments.
Conclusions
The present study utilized LCA to classify non-local patient satisfaction levels with VIP outpatient services into 3 distinct profiles: a group prioritizing doctor-patient interaction (Class 1), a group emphasizing non-clinical services (Class 2), and a High-Satisfaction Group (Class 3). These classes indicate varying emphases on “structure” and “process” within the SPO framework, illustrating how different patient subgroups weigh these determinants in shaping satisfaction outcomes. A reverse-scoring method was applied to improve the accuracy of the research findings and to provide a reference for hospital management. The results indicate that despite the waiting time yielding a beneficial result on medical interaction, tools can still be utilized during waiting periods to help maintain patient engagement and facilitate more effective communication with healthcare providers. Furthermore, policymakers should emphasize younger patients and train doctors to employ communication strategies that are crucial for conveying essential information efficiently during time-constrained consultations with non-local patients. Finally, improvements in the environment of auxiliary examination departments, such as clinical laboratories and endoscopy centers, remain significant for the fulfillment of nonclinical needs. This emphasis on improving non-clinical services aligns with the SPO model, wherein structural components are posited to influence the outcomes. Our study makes an innovative contribution by employing LCA to categorize non-local patients using VIP outpatient services into 3 distinct satisfaction subgroups and by identifying the key determinants associated with each pattern, thereby advancing the methodological application and contextual depth of this population. Accordingly, the findings may provide actionable insights for health policymakers to tailor outpatient services according to the differentiated needs and characteristics of various patient subgroups.
Supplemental Material
sj-doc-1-inq-10.1177_00469580261433923 – Supplemental material for A Cross-Sectional Latent Class Analysis of 3 Distinct Satisfaction Subgroups Among Non-Local Patients in VIP Outpatient
Supplemental material, sj-doc-1-inq-10.1177_00469580261433923 for A Cross-Sectional Latent Class Analysis of 3 Distinct Satisfaction Subgroups Among Non-Local Patients in VIP Outpatient by Huilin Wang, Hao Wang, Hongjun Fang, Sinan Guan and Jing Li in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580261433923 – Supplemental material for A Cross-Sectional Latent Class Analysis of 3 Distinct Satisfaction Subgroups Among Non-Local Patients in VIP Outpatient
Supplemental material, sj-docx-2-inq-10.1177_00469580261433923 for A Cross-Sectional Latent Class Analysis of 3 Distinct Satisfaction Subgroups Among Non-Local Patients in VIP Outpatient by Huilin Wang, Hao Wang, Hongjun Fang, Sinan Guan and Jing Li in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-3-inq-10.1177_00469580261433923 – Supplemental material for A Cross-Sectional Latent Class Analysis of 3 Distinct Satisfaction Subgroups Among Non-Local Patients in VIP Outpatient
Supplemental material, sj-docx-3-inq-10.1177_00469580261433923 for A Cross-Sectional Latent Class Analysis of 3 Distinct Satisfaction Subgroups Among Non-Local Patients in VIP Outpatient by Huilin Wang, Hao Wang, Hongjun Fang, Sinan Guan and Jing Li in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-4-inq-10.1177_00469580261433923 – Supplemental material for A Cross-Sectional Latent Class Analysis of 3 Distinct Satisfaction Subgroups Among Non-Local Patients in VIP Outpatient
Supplemental material, sj-docx-4-inq-10.1177_00469580261433923 for A Cross-Sectional Latent Class Analysis of 3 Distinct Satisfaction Subgroups Among Non-Local Patients in VIP Outpatient by Huilin Wang, Hao Wang, Hongjun Fang, Sinan Guan and Jing Li in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-5-inq-10.1177_00469580261433923 – Supplemental material for A Cross-Sectional Latent Class Analysis of 3 Distinct Satisfaction Subgroups Among Non-Local Patients in VIP Outpatient
Supplemental material, sj-docx-5-inq-10.1177_00469580261433923 for A Cross-Sectional Latent Class Analysis of 3 Distinct Satisfaction Subgroups Among Non-Local Patients in VIP Outpatient by Huilin Wang, Hao Wang, Hongjun Fang, Sinan Guan and Jing Li in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-6-inq-10.1177_00469580261433923 – Supplemental material for A Cross-Sectional Latent Class Analysis of 3 Distinct Satisfaction Subgroups Among Non-Local Patients in VIP Outpatient
Supplemental material, sj-docx-6-inq-10.1177_00469580261433923 for A Cross-Sectional Latent Class Analysis of 3 Distinct Satisfaction Subgroups Among Non-Local Patients in VIP Outpatient by Huilin Wang, Hao Wang, Hongjun Fang, Sinan Guan and Jing Li in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We would like to extend our gratitude to all those who participated in this study and the VIP outpatient department of Beijing University First Hospital, which facilitated our research and the investigators of this study.
Abbreviations
VIP very important person
CI confidence interval
AIC Akaike Information Criterion
BIC Bayesian Information Criterion
aBIC adjusted Bayesian Information Criterion
LMR Lo-Mendell-Rubin likelihood ratio test
BLRT bootstrap likelihood ratio test
SE standard error
aOR adjusted odds ratio
CI confidence interval
Ethical Considerations
The study was granted an ethical clearance certificate from the Ethics Committee of the Peking University First Hospital (NO. 2025R0051-0002). This study was conducted in accordance with the principles of the Declaration of Helsinki.
Consent to Participate
Written informed consent was developed for each respondent to read and sign before moving on to fill-in the questionnaire. All participants were informed about the purpose of the study, assured of confidentiality, and provided written consent prior to participation. Participation was voluntary, and respondents could withdraw at any time without consequence.
Author Contributions
Huilin Wang: Conceptualization, Methodology, Formal Analysis, and preparation of the first draft of the manuscript. Hao Wang: Investigation, Data Curation, Writing - Review & Editing. Hongjun Fang: Resources, Validation. Sinan Guan: Data Collection, Analysis. Jing Li: Supervision, Project administration, and provided critical comments in the revision of the manuscript. All authors agreed and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the Peking University First Hospital Scientific Research Project Fund (2025SF109).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Owing to the restrictive conditions of data provision, they cannot be shared publicly. Please contact the authors for further details.
Supplemental Material
Supplemental material for this article is available online.