
Abstract
The use of complementary and alternative medicine (CAM) is rapidly increasing for various non-communicable diseases, including cancer, presenting a complex challenge. However, few studies have examined CAM utilization in Nepal. A cross-sectional, quantitative, descriptive study design was conducted in a cancer-specialized hospital in Nepal to determine the use of CAM using a 29-item survey questionnaire designed to collect data on demographic and clinical characteristics and CAM utilization practices, based on the existing literature. Descriptive statistics and multivariate binary logistic regression were conducted in SPSS version 29 to identify significant influencing factors, with P-values < 0.05 considered statistically significant. Out of 101 participants, more than half (56.4%) used it for over a year. The commonly observed CAM was naturopathy and herbal products (such as amala, tulushi, aleovera, barley & wheat grass) (53.4%) and dietary supplements (43.6%). Majority of CAM users perceived it as effective (88.1%) and helpful in mostly alleviating nausea (76.4%). In multivariate analysis, only the use of yoga and meditation was independently associated with planning to continue CAM use (AOR: 8.939; 95% CI: 1.68-47.567). Majority of the patients with cancer were using CAM for more than a year, with naturopathy and herbal products among the highest modalities of CAM. The prolonged use of CAM among patients underscores the need to further educate patients on its long-term consequences, along with patient safety.
Keywords
Introduction
There is a gradual increase in the trend of consumption of complementary and alternative medicine (CAM) in non-communicable diseases, especially in patients with cancer and at the end stage of life.1 -7 A systematic review conducted in 2018 to identify the prevalence of use of CAM by patients with cancer in lower middle income countries (LMICs) reported a median use of 54.8% in a total survey of 6121 patients. 8 Among these median use of CAM within the South Asia world region accounted for 51.3%. 8 Several reasons exist for an increased use of CAM, among which are self-care, increased patient health care demands, poor availability of conventional treatment methods, and people’s perception regarding its cost-effectiveness and safety.1,3,8
World Health Organization (WHO) global report on traditional and complementary medicines 2019 defines the terms “complementary medicine” and “alternative medicine” as “a broad set of health care practices that are not part of that country’s own traditional or conventional medicine and are not fully integrated into the dominant health care system.” 9 The report also defines traditional medicine modality as an aggregated form of knowledge, skills, and applications based on a particular set of theories and experiences inherent to particular cultures used in the treatment, diagnosis, and mitigation of diseases. 9 The National Cancer Institute (NCI) classifies CAM into 5 different categories: mind-body therapies (meditation, biofeedback, hypnosis, yoga, tai chi, imagery, creative outlets), biologically based products (vitamins, dietary supplements, botanicals, special foods or diets), manipulative and body-based practices (massage therapy, chiropractic therapy, reflexology), energy healing (reiki, therapeutic touch), and whole medical systems (ayurvedic medicines, traditional Chinese medicines, naturopathic medicine). 10 Within the South Asian region, different types of CAM modalities, such as the use of herbal medicines, spiritual healing, nutritional and dietary therapy, meditation, yoga, psychological therapies, laughter therapy, and several healing therapies, were observed. 8
In today’s context, both conventional treatment and CAM, commonly known as integrative medicine, are increasingly used. 10 Literatures shows that the concomitant use of CAM along with conventional medicines accounted for a median use of 32.7% in LMICs, accounting for 26.7% from countries belonging to the South Asian world region.3,8 As a consequence, the safety risk increases with the concomitant use of CAM with systemic chemotherapies in patients with cancer, as the latter inherently possesses the risk of side effects and adverse drug reactions. 11 On the contrary, the literature also reports that the use of CAM may help reduce side effects, thereby providing survivorship support. 8 A report published by the Nepal Health Research Council (NHRC) titled “Mapping the availability of Ayurveda and other Complementary Medicine Services Centers in Nepal 2018” concludes that CAM practices are widely prevalent in Nepal. Among these, Ayurveda is the most commonly practiced modality, followed by homeopathy. 12
Limited literatures from Nepal deals with the utilization and concepts of CAM in cancer patients.1,13 A study conducted on more than 900 participants in Kathmandu, Nepal, found that almost 30% of the participants used one of the CAM modalities after the diagnosis of cancer, with the majority of the participants getting the information from informal sources and not sharing the information about their use with their physician. 1 Another article, however, explains the harms caused by CAM and comments on how patients with cancer taking CAM modalities could be huge in the context of Nepal compared to the conventional treatment. 13 Hence, this study was conducted to examine awareness, experience, and utilization practices of CAM, and to identify factors influencing the willingness to continue its use among patients with cancer in Nepal.
Methods
Study Design and Setting
A cross-sectional quantitative descriptive study design was conducted to determine the use of CAM among patients with cancer from June to August 2024 in Kathmandu Cancer Center (KCC), Tathali, Bhaktapur, Nepal. KCC is a specialized cancer hospital providing comprehensive treatment for various types of cancer in the Nepalese population.
Study Participants and Sampling
Patients diagnosed with any form of cancer visiting both the out-patient and in-patient departments of the KCC, aged 20 or above, and receiving any form of cancer treatment were included in the study, while those who were not willing to participate and unable to respond to the study questionnaires were excluded.
A prevalence-based approach was taken to calculate the sample size, as the previous study reported that 31.6% of patients with cancer used CAM in Kathmandu, Nepal. 1 Considering a 90% confidence interval and 7.5% margin of error, a sample size of 105 was estimated for the study.
Survey Instrument
Based on existing literature, a survey questionnaire was designed to collect data on demographic and clinical characteristics, and CAM utilization practices.1,14 -17 The draft questionnaires were reviewed by experienced researchers, colleagues, and oncology professionals at KCC hospital to ensure they adequately covered the key domains of interest and enhanced content validity. Then, the questionnaire was pre-tested with a 10% sample of patients with cancer to assess the appropriateness, understandability, and clarity of the questions. The received feedback was reviewed and discussed with the investigators’ team, and the draft was amended to produce the final version of the questionnaires.
Data Management and Analysis
Data were manually cross-checked and entered into the IBM Statistical Package for the Social Sciences (SPSS) version 29 to minimize duplication and errors. Descriptive statistics, such as frequency and percentage, were used to interpret the variables, while regression analysis was conducted to explore the factors influencing patients with cancer decisions to continue using CAM. For the logistic regression analysis, “No” and “Not sure” responses to future CAM use were combined into a single “No category.” All socio-demographic and disease-related variables that showed significant relationships in the univariate binary logistic regression analysis were included in a multivariate binary logistic regression analysis to identify the significant influencing factors. A p-value of less than 0.05 was considered statistically significant.
Results
Socio-Demographic and Clinical-Related Characteristics of Participants
Altogether, 101 cancer patients completed the data collection form, while 105 were estimated and approached for the study. Most of the participating patients with cancer were male (50.5%), less than 50 years old (42.6%), married (97%), belonging to Hindu (60.4%) and Brahmin/Chhetri (51.5%) groups. Gynecological cancer with less than 1 year of diagnosis at the first stage was the most common clinical characteristic of patients. Participating patients were mostly in chemotherapy treatment (Table 1).
Socio-Demographic and Disease-Related Characteristics.

Means multiple-choice questions.
Awareness, Experience, and Utilization Practices of CAM
All participants were aware of using CAM, as most used it for over a year (56.4%). The most used CAM modalities were naturopathy and herbal products (such as amala, tulushi, aloe vera, barley & wheat grass) (53.4%), followed by dietary supplements (43.6%). Family/friends (79.2%) and CAM-partitioning healthcare workers (71.3%) were the primary sources for learning about CAM use. Majority of CAM users perceived it as effective (88.1%) and helpful in mostly alleviating nausea (76.4%). Majority of the participants (91.1%) said they had discussed it with their oncologist, whereas 53.3% appeared supportive of them. Most participants (73.3%) did not experience a financial burden from CAM use; around 45.5% spent less than 1000 Nepalese Rupees (NPR) per month on CAM treatments. More than half of CAM users were satisfied with it. All patients who continued using CAM said they would continue using conventional medicines (Table 2).
Awareness, Experience, and Utilization Practice of Complementary and Alternative Medicines.
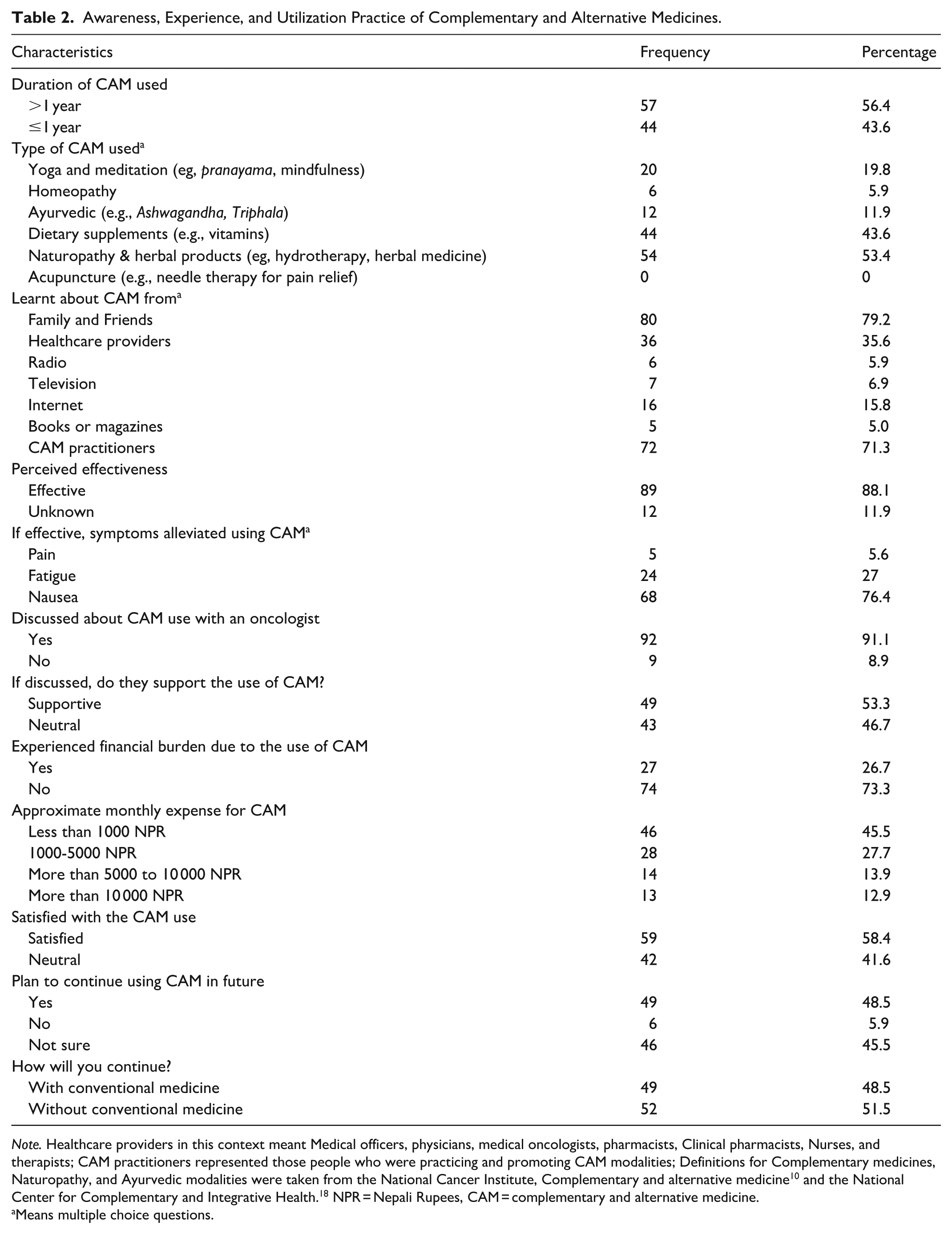
Note. Healthcare providers in this context meant Medical officers, physicians, medical oncologists, pharmacists, Clinical pharmacists, Nurses, and therapists; CAM practitioners represented those people who were practicing and promoting CAM modalities; Definitions for Complementary medicines, Naturopathy, and Ayurvedic modalities were taken from the National Cancer Institute, Complementary and alternative medicine 10 and the National Center for Complementary and Integrative Health. 18 NPR = Nepali Rupees, CAM = complementary and alternative medicine.
Means multiple choice questions.
Factors Influencing the Plan to Continue Using CAM in Future
On univariate logistic regression analysis, age groups, using yoga and meditation, learning about CAM from the internet, experiencing financial burden due to the use of CAM, and approximate monthly expense for CAM variables were found to significantly influence the planning of continuing CAM use in the future. However, only those who use yoga and meditation were found to be substantially influenced to continue using CAM in the future, with an odd value of 8.939. Table 3 illustrates the variables that are significantly associated in both univariate and multivariate binary logistic regression analyses.
Factors Influencing the Plan to Continue Using CAM in the Future.

Note. COR = crude odd’s ratio; AOR = adjusted odd’s ratio.
Significance level at <.05; The unmentioned group or subcategory of each variable is set as a reference.
Discussion
This study explored the prevalence and pattern of CAM among patients with cancer undergoing cancer-related treatment at KCC, Bhaktapur, Nepal, where the most used CAM modality was found to be Naturopathy & Herbal products (53.4%), followed by Dietary supplement (43.6%) and Yoga and Meditation (19.8%). This is contrary to the study conducted in a tertiary hospital in the Sub-Himalayan city of India 19 and 2 National hospitals in Kathmandu, Nepal 1 where both studies showed a higher prevalence of Ayurvedic modalities. In both studies, naturopathy was the second most commonly observed CAM modality.1,19 A study from Northern India also reported that Ayurvedic treatment was the most commonly used CAM modality, with an overall CAM use of 38.7%. 20 In the context of Nepal, a report published by NHRC indicates the considerable prevalence of Ayurvedic practices such as CAM within the country, followed by homeopathy. 12 Similarly, a systematic review analyzing a huge number of participants also reports several systems of CAM followed within the South Asian region, including Ayurveda and Naturopathy. 8 The immense prevalence of Ayurvedic products could be attributed to Nepal’s long traditional history of Ayurveda, which was derived from India, with the notion that Ayurvedic products display fewer side effects.1,21
In the present study, regarding perceived effectiveness, most CAM users (55.4%) were satisfied with their CAM use. Study from the Cancer Specialty Hospital of Nepal also supports this finding, where 89.1% of participants expressed their satisfaction with CAM use, as 59.4% participants reported using CAM to reduce their cancer treatment side-effects. 6 This finding also supports various other studies conducted in Ethiopia, 22 Saudi Arabia 23 and Mongolia. 14 They found that CAM was useful to the majority of users and were recommending other to use it. They said that it was beneficial in reducing side effects of cancer-related treatments. This first-hand experience is substantial in influencing people in Nepal, as most participants (79.2%) reported that family and friends were the major sources of information about CAM, followed by CAM practitioners (71.3%). Similar results were also observed from a study conducted in Japan, where CAM users got motivation from family and friends (77.7%) rather than personal choice. 24 Studies from India and Malaysia also reported on how the use of CAM therapies by users was mainly influenced by their friends and family members.20,25 However, studies from Ethiopia, 22 Rural Australia, 26 and another study done in a National hospital survey in Mongolia showed that CAM users got their information from other CAM users (24.7%). 14 That might be because an individual’s health-seeking behavior varies on various factors, including personal experiences.
More than 90% of the patients were found to discuss their CAM use with their oncologist in this study. On the contrary, the studies conducted in Nigeria and Japan showed that considerable proportion of people use CAM without proper consultation with oncologists and physicians.2,24 In the study conducted in Nigeria, more than 50% of the participants didn’t give information regarding their CAM use to physicians. 2 Literature shows that patients under CAM not disclosing the information to their physician could be because of several factors, including the misinformation and belief that their physician does not have to know about it, not letting physicians use CAM because of potential side effects, discouragement on the use of CAM in the past period, negative answers from physicians, physician knowledge on CAM, and time issues to discuss on its importance and use. 27 Literature points out that the high use and prevalence of CAM among patients with cancer definitely underscores the need for CAM disclosure so as to prioritize CAM safety, efficacy, and for better patient monitoring.20,28 In contrast to several studies reporting substantial non-disclosure of CAM use among patients with cancer, our study found that the majority of participants (91.1%) discussed their CAM use with their oncologist. This high disclosure rate may reflect growing awareness among patients regarding the importance of informing healthcare providers about all therapies they use, or it may indicate a relatively open communication environment within the study setting. While disclosure is encouraging, it does not necessarily guarantee appropriate monitoring or evidence-based guidance regarding CAM use. Many CAM products in Nepal are easily accessible and may be purchased without formal consultation with either allopathic or Ayurvedic physicians. Without structured documentation and clinical evaluation of potential interactions, especially in patients undergoing chemotherapy or other systemic treatments, the risk of adverse events or herb-drug interactions remain a concern. Therefore, beyond encouraging disclosure, there is a need to strengthen clinician knowledge regarding commonly used CAM modalities and to establish clearer communication and monitoring frameworks to ensure patient safety in integrative cancer care.
In the present study, although several demographic and behavioral variables showed associations with future CAM use in univariate analysis, only yoga and meditation use remained significant predictors in the multivariate model. Patients practicing yoga and meditation were more likely to plan to continue CAM use in the future. This may reflect the cultural acceptability, accessibility, and perceived holistic benefits of yoga and meditation in the Nepalese context. As yoga is deeply rooted in South Asian traditions and widely promoted for physical and psychological well-being,29 -31 patients who adopt these practices may be more inclined toward integrative approaches alongside conventional cancer treatment. The strong association observed in this study underscores the importance of understanding mind-body therapies in cancer care and ensuring appropriate guidance and monitoring to ensure their safe integration.
Most participants (56.4%) were using CAM for over a year. This underscores the need for collective counseling on the possible long-term consequences, as the literature still recommends understanding the influence and safety of cumulative use of these agents.3,6 -8,20 Studies from several settings assessing the interaction between CAM, over the counter and prescription drugs showed a considerable prevalence of interaction between the agents thereby emphasizing the need to increase awareness among healthcare professionals and patients so as to decrease the risk and enhance patient safety.32,33 With cancer, the involvement of both conventional and CAM therapy can increase the risk of unprecedented interactions underscoring the need for better patient-provider communication with enhanced documentation system and the need to check interactions.1,34 Similarly, study also revealed that individuals who were delaying in seeking treatment to conventional therapy were more likely to use CAM modalities. This may have been due to the systemic barriers within the conventional healthcare system making it inaccessible, as such, because of these barriers, individuals are forced in using numbers of CAM modalities. 35 Similarly, literatures also highlights on how the use of CAM modalities are often linked to delaying of conventional treatment, and delay in the presentation, resolution of a diagnosis and suitable treatment.1,36,37
Although most participants did not report experiencing financial burden from CAM use, a proportion of patients incurred additional out-of-pocket expenses. Previous studies from Southeast Asia have shown that complementary medicine expenditures can contribute substantially to household health spending and may increase the risk of financial strain, particularly in lower-income settings. 38 Given that cancer treatment itself imposes significant economic pressure, even modest additional costs from CAM use may compound financial vulnerability. These findings highlight the importance of discussing not only the clinical safety but also the economic implications of CAM use within oncology care.39,40 All of these factors emphasizes the need for a robust patient-provider communication for effective clinical practice.
Implications
The findings of this study have important clinical and policy implications for oncology care in Nepal. The high prevalence of CAM use, prolonged duration of use, and strong intention to continue CAM, particularly among patients practicing yoga and meditation, highlight the need for structured integration of CAM discussions into routine oncology consultations. Healthcare providers should proactively inquire about CAM use and ensure systematic documentation to minimize potential herb-drug interactions and adverse effects, especially among patients receiving chemotherapy and other systemic treatments.
The high rate of patient disclosure observed in this study provides an opportunity to strengthen patient-provider communication and establish formal monitoring mechanisms for CAM use. However, disclosure alone does not guarantee appropriate clinical oversight. Many CAM products are easily accessible and may be purchased without formal consultation with either allopathic or Ayurvedic physicians. Therefore, clinicians should receive training on commonly used CAM modalities in Nepal, particularly herbal and naturopathic products, to enable evidence-informed counseling and appropriate risk assessment.
At the policy level, the findings underscore the need for national or institutional guidelines on the safe use of CAM in cancer care. Clear regulatory oversight, improved labeling standards, and public awareness initiatives may help reduce unsupervised or inappropriate CAM consumption. Further multicenter and longitudinal research is needed to evaluate clinical outcomes, economic implications, and potential interactions between CAM and conventional cancer therapies within the Nepalese healthcare context.
Strengths and Limitations
This study provides important baseline data on the utilization pattern of CAM among patients with cancer in Nepal, a setting where limited empirical evidence exists. To our knowledge, few recent studies have explored both awareness and continuation intentions of CAM use within a specialized oncology center in Nepal. The use of a structured, pre-tested questionnaire and the inclusion of multivariate logistic regression analysis strengthen the methodological rigor of the study. Additionally, the high rate of disclosure of CAM use to oncologists observed in this study offers valuable insight into patient-provider communication dynamics within this clinical setting.
However, several limitations should be considered. First, the study was conducted in a single center with a relatively small sample size, which may limit generalizability to the broader cancer population in Nepal. Second, the cross-sectional design prevents causal inference regarding factors influencing CAM use or continuation. Third, CAM utilization was self-reported, which may introduce recall bias or social desirability bias. Additionally, the study did not verify the specific types, dosages, or duration of CAM products used, nor did it assess potential herb-drug interactions or adverse effects. Future multicenter studies with larger sample sizes and more detailed clinical verification are warranted to strengthen the evidence base.
Conclusion
Most participants reported using CAM for more than 1 year, with naturopathy and herbal products being the most commonly utilized modalities. Many participants reported learning about CAM through family and friends. Among users, the primary reason for CAM use was to alleviate the side effects associated with cancer treatment, and many expressed satisfaction with its use. These findings highlight the importance of open patient–provider communication and structured monitoring to ensure safe and informed integration of CAM within conventional cancer care.
Footnotes
Acknowledgements
The authors would like to express their sincere gratitude to all the participants for their cooperation and willingness to share their experiences.
Ethical Considerations
The study received the ethical approval from Star Hospital Research Center Institutional Review Committee (SHRC-IRC) [Reference number: 329/080/081].
Consent to Participate
Eligible participants were provided with a detailed explanation of the study’s purpose before taking verbal and written consent. The research was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. Patients were asked to fill out the questionnaires themselves, and if they could not do so, the data collector interviewed them and filled in their responses in the survey sheet. The patient’s caregivers were interviewed in case the patient could not respond appropriately. All respondents were treated equally, with dignity and respect for their privacy. Participants’ medical conditions, the surrounding environment, and cultural characteristics were all considered.
Author Contributions
SP and SS (a) and SS(b) conceptualized the idea. SP and NP wrote the initial version of the manuscript. SP, NP, RS helped with the data analysis and further editing of the manuscript. PR and SS(a) reviewed the manuscript critically and provided the critical contrusctive feedback. SS(b) reviewed the final version and supervised throughout the study. Finally, all authors agreed on the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Available upon valid request to the corresponding authors.*