
Abstract
Using AI-powered mobile applications for mental health screening can help reduce maternal mental health disparities among Black mothers who are pregnant or parenting in the United States. A maternal health education question and answer mobile application chatbot has the potential to intervene in the maternal depression cascade, specifically screening. Extant research demonstrates the usability of mobile applications addressing mental health. However, limited scholarship explores the intersection between AI-powered mobile application chatbots and maternal mental health. This study uses a multimethod analysis to evaluate the usability of an AI-powered mobile application to address maternal mental health among Black women. Data sources, including mobile application engagement, mental health disorder scales, and secondary qualitative analysis from focus group discussions (n = 5), will be assessed through a multimethod approach. The study team previously collected data across the United States for this clinical intervention in 2022. Findings indicate that the mobile application demonstrated promise in the application’s usability to screen for maternal health depression indicators. This was achieved using the mobile application’s intent classification functionality that classified users’ questions that contained targeted search terms (e.g., postpartum depression) or specific inquiries about mental health and appropriate follow-up from the study team to provide mental health resources. Critical interconnected themes were assessed and reflected high confidence, acceptance, and usability of the mobile application in addressing maternal mental health inquiries. Findings contribute to evidence about the usability of AI-powered mobile applications informed by Black mothers in appropriate screening for maternal depression indicators and inquiries. This study provides insight into closing the gap in maternal health disparities in depression outcomes for Black mothers.
Introduction
Addressing maternal mental health disparities among Black mothers who are pregnant, or parenting is a key component to reducing maternal health disparities and improving the maternal health equity care continuum. Black mothers are disproportionately affected by maternal mental health conditions and disorders. Most Black mothers experience maternal mental health symptoms (40%), which is twice the rate of mothers across racial and ethnic groups. 1 This disparity is further reflected by their higher rates of perinatal and postpartum depression.2,3 As Black mothers are more likely to experience trauma during birth, their risk of postpartum depression is elevated. 4 Approximately 29% to 44% of Black mothers experience postpartum depressive symptoms.5,6 Further along the depression continuum, Black mothers are 1.6 times more likely to develop postpartum depression compared to White mothers. 7
This disparity is further evidenced in preventive maternal mental health and postpartum care. There is a lack of mental health services offered to and received by Black women, including screenings and treatment (e.g., initiation, continuation).6 -9 Among these Black mothers affected by maternal mental health symptoms, data suggest that only 13.5% of Black women with Perinatal or Postpartum Mood and Anxiety Disorders (PMAD) symptoms receive treatment during pregnancy, demonstrating treatment gaps in the care continuum. 10 Evidence suggests this trend is exacerbated by socioeconomic status, where Black mothers of low socioeconomic status have the lowest postpartum depression treatment initiation rates at only 4%. 9 Moreover, Black mothers experience a high incidence of hospital-based care for postpartum depression across racial and ethnic groups. 2 Interestingly, when Black mothers receive treatment, there are notable differences in the quality of care and information shared that further exacerbate maternal mental health disparities.11,12
While effective screening tools and treatment strategies for addressing depression have been developed and tested, detection and treatment rates are low, especially for historically underrepresented racial and ethnic groups.9,13 -17 Scholarship suggests that early screening for depressive symptoms during pregnancy, optimizing referral networks, and utilizing systems to report those with depressive symptoms are essential for initiation and continuation of care, particularly for Black women. 18 This early identification process for depressive symptoms can improve maternal mental health and birth outcomes for Black women. 18
Moreover, these mobile applications have gained heightened significance during the pandemic, evidenced by their proliferation and adoption.19 -21 There are nearly 20,000 mental health mobile applications, yet approximately 5% are evaluated. 22 These mobile applications continue to proliferate, rapidly improve, and increase access to mental health care. Compared to traditional therapy, mobile health interventions are effective in providing mental health services and resources.13,14 These virtual, instant applications can address mental health issues, support navigation, provide education, share health information, identify and monitor symptoms, and enhance access to mental health care.23 -25 These mobile applications are significant in both clinical and public health practice; however, they are limited in disaggregation across specific mental health conditions, including depression. 22
Mobile applications have also demonstrated their ability to manage depression among Black women, which was evaluated with high acceptability and accessibility.26,27 The functionality, usability, and comfort among Black women in receiving and using mental health services through mobile application technology are significant.26 -28 However, there remain gaps in the identification and monitoring of depressive symptoms among Black women using mobile applications. Notably, at least 80% of Black women reported owning smartphones and spending an average of 19 hours per week on smartphone applications, demonstrating the accessibility of mobile technology.26 -28
Chatbot mobile applications have demonstrated promise in positively impacting public health outcomes. An example is Rosie the Chatbot, which provides tailored, real-time maternal and child health information to support mothers by sharing information from verified sources through generative artificial intelligence.29,30 There are also other generative artificial intelligence chatbot interventions with conversational features focused on mental health support, including depression.31,32 Chatbots have also supported health behavior change, demonstrated high usability, and used personalization and targeted information features, particularly in substance use.33,34 More broadly, mobile application chatbots have gained increased usage in health promotion and the public health landscape.32,35
Existing scholarship demonstrates the usability of mobile applications to address mental health indicators and inquiries. While mobile applications focus on mental health broadly, there remain gaps in the assessment of depression and among subgroups. Limited scholarship explores mobile applications’ ability to track and target maternal mental health indicators and inquiries among application users of color, specifically Black mothers. Based on stark maternal mental health disparities like depression, and evidence base of accessible and acceptable mobile applications among Black women, mobile applications may have the ability to identify and screen for maternal depression indicators and inquiries. Mobile applications that are trauma-informed and targeted to detect maternal mental health symptoms, coupled with the coordination of mental health screenings, are promising methods to reduce mental health disparities. To address the research gap, this study seeks to assess the usability of a mobile chatbot application in intervening on maternal mental health disparities, specifically depression, among Black mothers involved in perinatal and maternal health clinical research.
Materials and Methods
Rosie the Chatbot, an AI-Powered Mobile Application Chatbot
Background
Rosie the Chatbot is a clinical intervention trial of a generative artificial intelligence-powered chatbot that shared health information in response to health inquiries posed by users. Rosie the Chatbot aims to enhance maternal and infant outcomes and support improved health information sharing from reliable sources.29,30 Rosie the Chatbot was also informed and co-developed by mothers of color.
Study Setting
The pilot study occurred in 2022 across the United States among mothers of color aged 14 years and older, who were either pregnant or parenting a child under 6 months old. During the pilot phase of Rosie the Chatbot, a Focus Group Discussion (FGD) was conducted to assess feasibility and acceptability.
Study Involvement
Participants involved in the pilot study posed health inquiries of interest, whereby Rosie the Chatbot provided instant responses from verified sources. Topics focused on a wide range of health topics, including mental health, such as depression. Participant engagement in the pilot study for Rosie the Chatbot spanned a total of 3 months. During this time, participants were asked to interact with the chatbot whenever they desired by posing any and all inquiries they had, exploring available features, and interacting with the chatbot as desired.
Study Sample
The sample size for the pilot study was N = 30, which aligns with the optimal size for a pilot study to assess the feasibility and acceptability of an intervention. 36 This sample size was also supported by the ideal FGD sample size for each focus group (n = 4-6 per group). 37 Recruitment methods for the study included social media advertisements on Facebook and Instagram, through referral networks, and in-person outreach at community events like health fairs, back-to-school events, and community baby showers. Participants were compensated for their FGD and study enrollment in Rosie the Chatbot. This clinical trial received ethics approval from the University of Maryland Institutional Review Board (#1556200).
Secondary Data Approach
Study Design
We conducted a secondary analysis using a multimethod approach. Our approach supported a comparative assessment of multiple data sources focused on maternal depression indicators and inquiries, that supported triangulation. The following data analytic approaches were conducted from secondary datasets: a quantitative data analysis in conjunction with a template analysis and a content analysis of qualitative data.38,39 Data were analyzed through an interpretivism-constructivism paradigm, emphasizing the exploration of experiences, interactions, and contexts, which was most aligned with understanding factors influencing maternal depression indicators and inquiries.38,39 Data sources included mobile application engagement, user-centered inquiry, mental health disorder scales, and a FGD. Rosie the Chatbot participants described their experiences with maternal mental health indicators and inquiries during the FGD. This study was conducted in compliance with the Standards for Reporting Qualitative Research (SRQR) checklist (Supplemental File 1). 40
Data Collection
Data for this study were collected from a clinical intervention trial entitled Rosie the Chatbot, conducted during the pilot phase to assess feasibility and acceptability. Data were collected at baseline by the research team. The research team included several research assistants and professors from interdisciplinary backgrounds in public health, social work, and information sciences.
Eligibility Criteria
For this secondary data analysis, the sample was restricted to only Black women (n = 17). This subsample was selected for the secondary data analysis.
Depression Disorder Scale and Demographic Data
Participants completed a pre-trial study enrollment form using the Qualtrics Survey tool (www.qualtrics.com). The form collected self-reported parenting status (pregnant or parenting) and depression scores from the PHQ-9, which were then assessed through descriptive analysis.
Focus Group Discussion (FGD)
A single focus group discussion (FGD) involving 5 participants was conducted in English by 2 senior interviewers. The FGD fostered an interactive dialog where participants could respond to and expand on one another’s ideas. Purposive sampling was employed to select participants who were invited to participate in the FGD. The focus group interview guide was developed by the research team leaders (Supplemental File 2). This interview guide encompassed questions regarding acceptability and frequency of technology utilization, suggestions and improvements for Rosie the Chatbot, and proposed inquiries for Rosie the Chatbot. The interview guide also included questions on pregnancy and parenting experiences, navigating parenthood, practices for identifying parenthood resources and health information, and exploring pregnancy and parenting facilitators and barriers. The interview guide was pilot tested during this study. Participants provided written and verbal consent in English and were interviewed on Zoom video conferencing software (www.zoom.com). Transcripts were transcribed and coded by at least 2 coders to ensure inter-rater reliability. Data from the FGDs were de-identified, and pseudonyms were used.
Mobile Application Engagement and User-Centered Inquiry
To assess mobile application engagement and user-centered inquiry, questions and topics posed to Rosie the Chatbot were collected both indirectly (during FGD by the interviewer) and directly (from mothers using Rosie the Chatbot). All questions were qualitatively assessed through content analysis.
For questions asked directly to Rosie the Chatbot, the researcher tabulated the questions asked by participants. All questions were filtered through intent classification using Rasa (www.rasa.com), which uses natural language understanding and machine learning models to identify mental health incidents. When a potential mental health emergency or concern was detected through this algorithm, a research member notified the team of the potential mental health emergency or concern. Importantly, mothers who asked these questions received responses containing targeted, and focused resources and/or follow-up contact conducted by a licensed social worker. Questions filtered by the system that were not determined to relate to mental health emergencies or concern (e.g., how to sanitize bottles, how to relieve baby rashes, best first foods to feed baby) were simply answered by Rosie the Chatbot without the need for staff follow-up.
Measures
PHQ-9 Scale.
The PHQ-9 screens for depression and depressive symptoms. 41 This 9-item scale ranges from 0 to 27, with scoring categorized as follows: Minimal (0-4), Mild (5-9), Moderate (10-14), Moderately Severe (15-19), and Severe (20-27). Responses were rated on a scale ranging from 0 = Not at All to 3 = Nearly Every day. The scale demonstrates high internal reliability, test-retest reliability, and validity; further supported by a Cronbach’s alpha (α) of .89 when tested in a study based in a primary care setting and .86 in a study based in an obstetrics and gynecology clinical setting. 31
Secondary Data Analysis
The data underwent several steps of cleaning, including (1) selection to include Black women only, (2) coding and recoding variables, and (3) screening to remove missing data (n = 2). Following the preparation of the data, descriptive analysis was conducted across the following demographic domains: parenting status (Pregnant or Parenting a child under 6 months old), income categories (0-$30,000, $30,001-$50,000, $50,001-$75,000, $750,001-$100,000, $100,001-$200,000, $200,000+USD), Education Level (High School/GED, Associate’s Bachelor’s, Master’s, Doctoral/Professional Degree), insurance status (Insured, Uninsured), and PHQ-9 Scale (Mild, Moderate, Severely Moderate) and Positive Depression Screen. Descriptive statistics were conducted where sample characteristics and prevalence of positive depression screen were reported. A total sum score of the 9-item PHQ-9 scale was calculated to estimate prevalence, with scores categorized into established intervals of depression severity. Additionally, a variable named “positive depression screen” was created to include participants with an aggregated PHQ-9 score greater than or equal to 10.
Data were further analyzed through qualitative coding, utilizing template analysis and content analysis with NVivo software for management and analysis (www.1umivero.com/product/nvivo).38,39 The template analysis sought to identify themes from the FGD informed by a priori codes. 38 Codes were developed through an a priori template by the first author. The codebook was developed through review of a subset of transcripts, based on a systematic review of literature, familiarity with the dataset, and identification of important themes by the research team through peer debriefing. Line-by-line coding was conducted by 2 researchers for each transcript. Through discussion among the team, the coding template was revised. This iterative process allowed the codebook to be refined, which ensured rigor and informed the development of the coding template. An initial deductive codebook with definitions was created, followed by inductive coding by the coding team for the FGD, as well as mobile application engagement and user-centered inquiry. Discrepancies were resolved through consensus. Emergent themes related to mental health, navigation, and coping mechanisms were identified and synthesized. The content analysis examined the presence of certain concepts from the mobile application engagement and user-centered inquiries posed by participants during the FGD and using the mobile application, based on the template described above. 39 This template was iteratively developed. Our team then quantified the frequency of concepts through conceptual analysis. Furthermore, we analyzed the relationships between codes in relation to one another through relational analysis.
Descriptive statistics were utilized for joint display in conjunction with qualitative analysis, including template analysis and content analysis. The FGD was assessed through template analysis, while mobile application engagement and user-centered inquiry were assessed through content analysis. Findings were shared with the community members and leaders who participated in and supported this study to ensure dissemination and potential implementation of results.
Results
Secondary Quantitative Analysis
Patient characteristics are presented in Table 1. Mothers included Parenting (n = 8) and Pregnant (n = 9). For the educational level, the majority of mothers had a Bachelor’s (n = 7); followed by a Master’s (n = 4), and High School or GED (n = 2), Associate’s (n = 2), and a Doctoral or professional degree (n = 2). Most mothers were insured (n = 13), and a couple were uninsured (n = 2). For household income, the majority of mothers reported $75, 001-$100,000 (n = 5) and $100,001-$200,000 (n = 5); followed $50,001-$75,000 (n = 3); $30,001-$50,000 (n = 2); and 0-$30,000 (n = 1) and $200,001+ (n = 1).
Participant Characteristics of Black Women Enrolled in Rosie the Chatbot Pilot Study (n = 17).

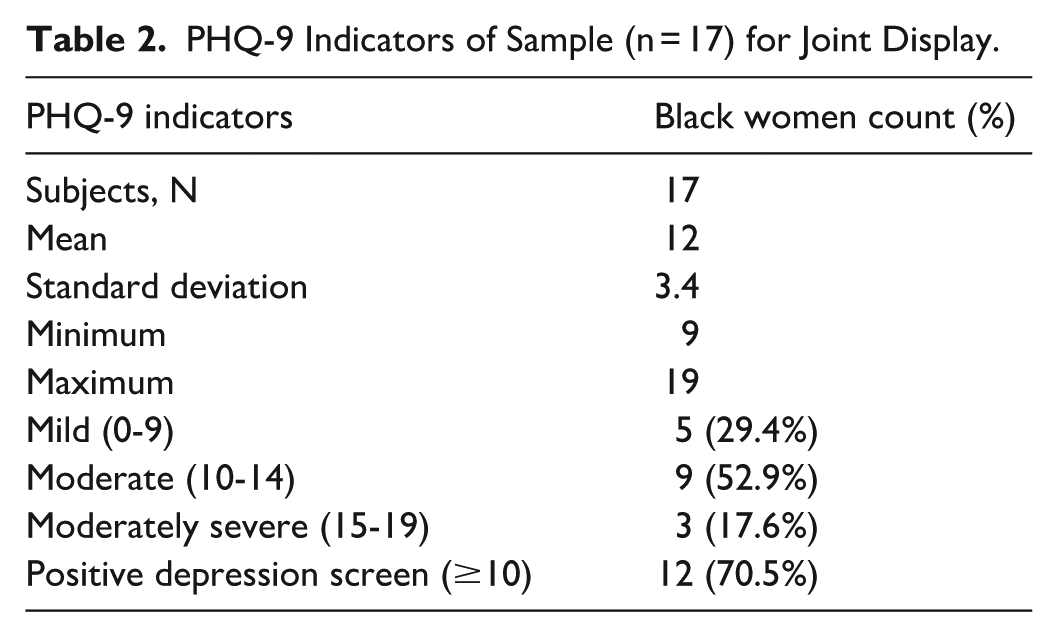
Of Black women included in the pilot study (n = 17), nearly half had a moderate PHQ-9 depression score (n = 9, 52.9%), followed by a mild score (n = 5, 29.4%), and a moderately severe score (n = 3, 17.6%). The majority (n = 12) had a positive depression screen (n = 12, 70.5%). The mean score was 12, with a standard deviation of 3.4, a minimum of 9, and a maximum of 19. Results are presented in Table 2.
PHQ-9 Indicators of Sample (n = 17) for Joint Display.
Content Analysis
Among the questions and topics hypothetically asked during the FGD, 17% (10 of 58) of the questions and topics focused on mental health. Mental health was defined as an indication of a distressing experience, mental health concern, mental health symptoms, mental health disorder, or strong emotional response. This could include distress, stress, anxiety, depression, discrimination, and excessive sleep. For example, selected sample questions included: How to deal with my emotions?, Why am I crying?, How to get happy when I am sad?. For example, selected sample topics included: anxiety, depression, mood swings, and temper. Among the questions that triggered responses from Rosie the Chatbot and follow-up from the research team, 25% (6 of 24) of the questions focused on mental health. Of these questions (N = 6) triggering a response and follow-up, more than half (n = 4) addressed postpartum depression or depression, and some (n = 2) focused on sleep regression.
Template Analysis
Mental Health
The majority of participants during the FGD described mental health indicators related to depression and sadness. Mothers discussed new experiences of navigating motherhood that involve the onset of feelings, responsibilities, and concerns. They reported feelings of fear and apprehension contributing to mood fluctuations and emotional challenges. Mothers also described anticipated stress and anxiety often emerging in connection with new parenting experiences and surrounding changes in daily life and practice. The complexities of these new experiences brought about inquiries and concerns surrounding depression and sadness. Within this framing, mothers also underscored their desire to prioritize both their own health and well-being, which is central to their parenting experience. These quotes highlight mothers navigating new and existing emotions in the midst of their pregnancy and parenting status, with increases in distressing experiences and concerns. Below are selected quotes of textual evidence to support this finding, where * denotes the self-selected pseudonym.
I got anxiety, this fear in me. I don’t want to lose my child. I want to feel that joy within me, so that (is) what bothers me a lot. . .and I don’t want to harm my baby in any way. So my number-one question from day one has always been about depression. (Millie)* when I found out I was pregnant there are a lot of changes for me, especially because my mood, my feelings, my emotion actually change, what I enjoyed doing before, I couldn’t do that again. For example I just get sad for no reason, and sometimes, I just start to cry, and I will be like, ‘What is the reason, why I am actually crying?’ (Norsly)*
Technology
All participants discussed their confidence, familiarity, comfortability, acceptance, and high usage of technology, including mobile applications. Most participants underscored the fundamental integration of technology as central in their daily lives and practice. Inquiries using Rosie the Chatbot were particularly important for key subgroups of mothers, as described by participants. Inquiries were useful for new mothers who were new to navigating parenthood. Mothers also described inquiries focusing on sensitive and potentially stigmatized questions as being of great importance and relevance when using Rosie the Chatbot, for example. An illustrative quote is shared by a participant here:
I'll say without technology, life would be not valid for me because I love technology a lot. I won’t lie without a phone, how would you do all the stuff? How would you search for how to be a mom, all the stuff? So, technology is really essential. (Alexa)*
Information and Navigation
Participants discussed how they intend to identify information and navigate using Rosie the Chatbot. Many participants described using Rosie the Chatbot to receive trusted and reliable information that would efficiently and sufficiently respond to their inquiries about mental health concerns and emotional distress. There was high confidence in Rosie the Chatbot’s ability to respond to mental health concerns. There was also demonstrated favorability of Rosie the Chatbot supporting mothers to receive information that was high-quality. Additionally, mothers described using Rosie the Chatbot to navigate their emotional challenges and complexities, as well as strategies for wellness practices. Participants sought to use Rosie the Chatbot to cope with mental health concerns and to preliminarily identify potential indicators and inquiries about depression. The usage of Rosie the Chatbot was evidenced by the following quotes.
I just want to say I would love to ask Rosie in a basic way on how to deal with my emotions because I could remember when I was pregnant from my first daughter, like sometimes I get emotional. Sometimes I just get sad without a reason and I start to cry. I was like, why am I crying? And there's no reason why I am crying. So I would tend to ask Rosie on how to deal with those emotions when it comes around, so maybe how to get happy when I'm sad. (Nita)* If it's that every answer here has been validated by top-notch doctors, the good doctors, that will give me a lot more confidence to even introduce that to someone and maybe even my support group. I could tell them, oh, there's an app called Rosie. Like top-notch doctors have validated it. It can give you top answers. Everything there is certified. Even my doctor can recommend it. (Sandra)*
Discussion
Summary
To our knowledge, this multimethod analysis with content analysis, template analysis and descriptive statistics provides the first assessment of a mobile application screening for depression indicators and inquiries among Black women who are pregnant or parenting. It is one among a still small but growing number of studies that focus on mobile application engagement and usability among Black women. We identified elevated rates of depressive symptoms and clinically defined depression among Black women who are pregnant or parenting, along with an increased likelihood of inquiring about depression-related content. We found 3 interconnected themes denoting high confidence, acceptance, and usability of the mobile application: (1) technology played an integral part in daily lives, (2) comfort in engaging in sensitive or stigmatized inquiries focusing on depression, and (3) acceptance of the application, effectively responding to mental health inquiries through demonstrated navigation. Based on these findings, the mobile application can further be expanded to intervene and screen for depression indicators and inquiries.
Comparison of Population-Based and Cohort Studies
When comparing PHQ-9 scores among Black women in our study with the general Black population, the elevated rates of depressive symptoms and positive depression screening are notable. Studies report mean scores of 5.7 to 6, and positive depression screening of 17.7%.41 -43 The contrast between these findings and our study’s findings shows that our sample of pregnant and parenting Black women exhibited higher rates of a positive depression screen than the general Black population and Black women. Studies among Black women during pregnancy and the postpartum period that used PHQ-9 scales or related abbreviated scales have consistently identified higher rates of depression and depressive symptoms. 10 Similar to our study findings, Black mothers during pregnancy and early parenting stages exhibit higher rates of clinical depression diagnosis and depressive symptoms.
Maternal health, depression symptoms, and clinical diagnosis were prevalent among Black women who were pregnant or parenting in our study. These indicators were elevated compared to population-based studies and cohort studies among the general Black population, Black women, and mothers across racial and ethnic groups, using the PHQ-9. These indicators were also comparable with national trends and data suggesting disproportionate prevalence of depression and depressive symptoms among Black women in perinatal and postpartum periods. The observed high prevalence of mental health depression symptoms and clinical diagnosis may contribute to increased maternal health disorders. This observation is further supported by the literature indicating gaps in screening, initiation, and linkage to mental health care, specifically depression, among Black women.
Comparison of Mobile Application and Chatbot Studies
Technology, specifically mobile applications, emerged as a central tool in addressing mental health needs and intervening in depressive indicators and inquiries. Participants demonstrated high confidence and familiarity with mobile applications for mental health support that aligns with prior trends among Black women.26 -28 Transformative technology, like mobile chatbot applications, was viewed as essential for navigating sensitive topics, including mental health, accessing information, and seeking assistance in managing depressive indicators and inquiries. Situated in this context, Rosie the Chatbot emerged as a trusted and reliable information source for Black women, providing support for maternal mental health concerns. Participants expressed confidence in Rosie the Chatbot’s ability to deliver efficient responses to inquiries and provide high-quality information tailored to their needs. Thus, the pivotal role of technology is underscored in facilitating access to mental health resources and support for Black mothers navigating the challenges of pregnancy and parenting, including the onset or elevated risk of depressive symptoms. Mobile application interventions highlight the importance of integrating transformative technology into maternal mental health care to effectively screen and intervene for mental health needs and concerns with this vulnerable population.
Other postpartum mental health chatbots, like Woebot, Moment for Parents, and another chatbot produced in collaboration with Postpartum Support International (PSI), focused on key components of acceptability, engagement, and design characteristics that Rosie the Chatbot encompasses. Woebot emphasized acceptability among women in the postpartum period, while it lacked a specific assessment of depression over time. 44 Moment for Parents engaged pregnant and postpartum women with high retention and re-engagement over time among users. 45 The other chatbot, produced in collaboration with PSI, a non-profit focused on postpartum mental health, integrated human-centered design and conversational style, but required greater integration with human moderators on their platform. 46 These chatbots either included less than 2% of Black women or did not report race and ethnicity. Rosie the Chatbot, focusing on Black women, demonstrated acceptability, usability, and integrated human moderators who responded to trigger questions, which is essential to ensure these chatbots are being safely tested and refined across diverse communities to advance population health.
There is high acceptance and favorability of using mobile applications among Black women, including those who may be pregnant and parenting, which is consistent with trends observed in other studies.26 -28 These mobile applications play a critical role in efficiently providing reliable information on sensitive or emotionally distressing topics. 32 Mobile applications can also facilitate mothers navigating mental health concerns by sharing information to address depressive symptoms and indicators. In sum, mobile applications, like Rosie the Chatbot, can function as a forum for Black mothers to express their questions in an open, safe, and receptive environment, where they receive appropriate information addressing their concerns, without stigma or bias, which is crucial for addressing sensitive inquiries, such as mental health.
Contextualization of Findings
The elevated prevalence of depression symptoms and clinical diagnosis among our sample may be correlated with Rosie the Chatbot application triggers. Our research team received significant inquiry triggers and conducted numerous mental health follow-ups during the intervention. The inquiry keywords promoting application response and follow-up included “postpartum,” “depression,” “sadness,” “excessive sleep,” and other mental health indicators from the PHQ-9 score. A follow-up conducted by a licensed social worker was administered to screen and provide a referral to mental health care. Our findings suggest that the triggers adequately identified early indications of depression and excessive sleep, where appropriate response and follow-up occurred.
Study findings highlight significant maternal depression symptoms and clinical diagnosis among Black women during the perinatal and postpartum periods. The majority of participants expressed experiences of depression and related indicators, aligning with evidence of elevated rates of depression and depressive symptoms among Black women.47 -52 Our findings also suggest the pressing need for emotional support and resources, in conjunction with early depression screenings among Black mothers.
Mobile applications demonstrate promise in identifying mental health concerns through user inquiry, based on the application’s ability to screen and discern targeted keywords focused on depressive indicators. The prompt application functions as a potential mechanism to screen for early signs of depression indicators and inquiries. Based on study findings, Rosie the Chatbot, a generative artificial intelligence chatbot, demonstrated promise in the application’s usability to screen for maternal health depressive symptoms and clinical diagnosis. This was achieved through targeted search terms and specific inquiries among participant responses and appropriate follow-up from the study team. Lessons learned include (1) identifying targeted keywords in mobile applications can activate automatic information sharing and resource provision with appropriate follow-up, monitoring, and maintenance, and (2) integrating transformative technology in response to addressing perceived needs and important topics within the community.
Strengths and Limitations
Strengths of this study include the multimethod approach, which combines content analysis, template analysis, and descriptive statistics to provide a rich joint display of qualitative and quantitative data analysis. This approach explores the usability of a mobile application in addressing maternal mental health disparities among Black mothers. Another strength was the assessment of a mobile chatbot application, which emphasized centered on transformative technology in addressing a complex health inequity issue. By leveraging a multimethod approach to analyze the usability of the mobile application, we underscored the importance of using technology-based interventions to bridge gaps in access and provision of care.
However, there are limitations to the conclusions that can be reached from our study. The primary limitation is the small sample size attributed to the pilot study data, which is reported from a single case study of participants in a mobile application and clinical intervention. We also did not perform a power analysis for this study, given that this met the requirements for a pilot study sample size. Moreover, the generalizability of study findings is restricted to Black women. A secondary limitation is that the data collection instruments, specifically from the FGD, did not explicitly focus on or contain relevant questions on mental health and depression. While the FGD contained probes on inquiries and topics of interest, mental health topics emerged. The FGD interview guide was not validated, as it was conducted for the pilot testing during this study.
Conclusions and Future Directions
Our results suggest that mobile chatbot applications may be promising tools to screen for depression indicators and inquiries during the perinatal and postpartum periods. However, further evaluation of this screening tool over time is needed to assess its accuracy in terms of indicators and diagnosis during follow-up. Findings contribute to evidence about usability and show promise for the efficacy of maternal health mobile applications in appropriate screening for maternal mental health indicators and inquiries. Findings also provide insight into closing the gap in maternal health disparities among Black mothers. This mobile application has the potential to be integrated as a tool within a comprehensive care model for screening and early intervention during the perinatal and postpartum periods. Future research could continue to focus on these 2 areas: (1) evaluating the effectiveness of mobile application chatbots among larger samples and conducting assessments over time, and (2) identifying risk factors and barriers to depression screening in perinatal and postpartum care. By continuing to explore these areas of research, the use of mobile applications like chatbots in maternal health can be further optimized and utilized in detecting maternal mental health conditions; and therefore, contribute to improved outcomes for Black mothers during the perinatal and postpartum periods.
Supplemental Material
sj-docx-1-inq-10.1177_00469580261417580 – Supplemental material for Using an AI-powered Mobile Application Chatbot to Address Maternal Depression Indicators and Inquiries in the Perinatal and Postpartum Periods: A Multimethod Analysis
Supplemental material, sj-docx-1-inq-10.1177_00469580261417580 for Using an AI-powered Mobile Application Chatbot to Address Maternal Depression Indicators and Inquiries in the Perinatal and Postpartum Periods: A Multimethod Analysis by Carson J. Peters, Valerie Aldana Lainez, Kaili Clark, Michelle Jasczynski, Quynh C. Nguyen and Elizabeth M. Norell in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580261417580 – Supplemental material for Using an AI-powered Mobile Application Chatbot to Address Maternal Depression Indicators and Inquiries in the Perinatal and Postpartum Periods: A Multimethod Analysis
Supplemental material, sj-docx-2-inq-10.1177_00469580261417580 for Using an AI-powered Mobile Application Chatbot to Address Maternal Depression Indicators and Inquiries in the Perinatal and Postpartum Periods: A Multimethod Analysis by Carson J. Peters, Valerie Aldana Lainez, Kaili Clark, Michelle Jasczynski, Quynh C. Nguyen and Elizabeth M. Norell in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We would like to thank the Community THRIVES Laboratory and Rosie the Chatbot Team for their contributions throughout Rosie the Chatbot study. Specifically, Francia Ximena Marin Gutierrez and Heran Mane for their support with data collection.
Ethics Considerations
This clinical trial received ethics approval and consent to participate from the University of Maryland Institutional Review Board (#1556200).
Consent to Participate
Informed consent was written and participants provided consent, as approved by the University of Maryland Institutional Review Board.
Consent for Publication
Not applicable. All participant identifying information has been de-identified, and pseudonyms were used in this manuscript.
Author Contributions
Study conceptualization, design, and implementation were completed by QCN and EMN. CJP, VAL, and KC analyzed and interpreted the qualitative data. CJP analyzed, interpreted, and created the tables and diagrams based on the study’s quantitative data. CJP, VAL, and KC completed the analysis of current literature about maternal mental health, mobile applications, and implications of previous studies, and provided a critical analysis of integrated results. CJP, VAL, and KC drafted and revised the iterations of the manuscript. CJP, QCN, EMN, MJ, VAL, and KC edited and reviewed the manuscript.
Authors’ Information
Reflexive Statement: The authorship team of this study is composed of researchers, professors, community-based scholars, and a licensed social worker from interdisciplinary backgrounds including public health, social work, and information sciences. Specifically, the team includes two doctoral students, one undergraduate public health student, one epidemiologist, one social worker, and one information scientist. The majority of the authors possess familiarity and expertise in maternal and child health and mental health. Our roles and identities were continually considered, centered in our discussion, and actively leveraged during the process of the study to enhance program design, analysis, and evaluation. Through reflexive journaling and peer debriefing, the authors continually engaged with how their lived experiences, backgrounds, and identities influenced the interpretation of the data, which enriched the overall research process and outcomes.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study reported in this paper was supported by research grants from the National Institute on Minority Health and Health Disparities (QCN and EMN; grant number R01MD016037) and by the National Library of Medicine (QCN; grant number R01LM012849). This research was supported [in part] by the NINR Intramural Research Program of the National Institutes of Health. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. Authors do not have any conflicts of interests relevant to this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The deidentified versions of data sets generated and analyzed during this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.