
Abstract
People with disabilities (PWD) are vulnerable to underlying and chronic conditions and often face barriers to healthcare access, resulting in unmet needs and poor health outcomes. Mobile health (mHealth), defined as the use of mobile technologies to deliver or support healthcare, may help address these gaps by enabling symptom monitoring and self-management, supporting medication adherence, and providing remote care beyond traditional in-person clinical settings. To assess the feasibility and effectiveness of a tailored hybrid mHealth intervention in improving health outcomes, physical function, and self-management behaviors among PWD. This single-arm pre–post study was conducted from April to August 2023 and included 48 participants with physical disabilities, brain injuries, or visual impairments recruited from disability service facilities. The hybrid mHealth platform comprised synchronous telehealth sessions (medication, nutrition, exercise) and asynchronous app-based modules that were developed specifically to support monitoring and self-management. Effectiveness was evaluated using behavioral and health-related outcomes, including medication adherence, physical function, and chronic disease management. Significant improvements were observed in medication adherence (2.6 ± 2.2 vs 3.4 ± 2.5, P = .0001) and medication knowledge (6.8 ± 1.9 vs 9.3 ± 1.6, P < .0001). The physical function results were also significantly improved for participants who completed the exercise intervention. Preliminary findings suggest that the mHealth intervention may enhance chronic disease management, physical function, and self-management among PWD, potentially improving healthcare accessibility. Further research with larger, more diverse populations and longer follow-up periods is warranted to confirm and expand these results.
Keywords
Introduction
Background
The World Health Organization has reported that, as of 2021, about 1.3 billion people, or 16% of the global population, were living with a disability. 1 In South Korea, the number of people with disabilities (PWD) is steadily increasing due to the aging population. As of December 2022, more than 2.65 million people were registered as disabled, accounting for 5.2% of the total population. 2 PWD are prone to chronic diseases at an earlier age than those without, due to their relatively poor health status,3,4 In South Korea, 79.3% of the population with disabilities have chronic diseases. 5 Secondary health conditions, difficulty maintaining a healthy lifestyle, and lack of access to medical care and health services increase the risk of negative health outcomes in the disabled.6 -10 Therefore, for people with disabilities, continuous assessments and management of their health status would improve the treatment of their chronic diseases and may improve their health.
Mobile health (mHealth) is a new tool for chronic disease management that can be implemented at home. 11 It is a subset of eHealth and is defined as the use of mobile technologies such as smartphones, tablets, and wearable devices to enhance the quality of and access to healthcare. 12 mHealth can help address gaps in care by enabling symptom monitoring and self-management, supporting medication adherence, and providing remote care beyond traditional clinical settings. As of December 2017, 325 000 mHealth applications (apps) were available 13 and this number had surpassed 350 000 by 2023, reflecting the rapid growth of mHealth. This increase has been especially evident since the COVID-19 pandemic. 14 According to the National Rehabilitation Institute of Korea’s survey on “COVID-19 Experiences and Problems of People with Disabilities,” 14.7% of PWD are more likely to have developed a health problem or to have experienced a deterioration in their health since the COVID-19 outbreak, compared to 9.9% of people without disabilities. 15
The purpose of mHealth is to enable patients to manage their health as part of their daily lives or to receive the necessary treatment from medical professionals if they cannot visit a medical institution in person.16 -19 mHealth for the disabled can improve quality of life and reduce medical expenditures by providing customized healthcare and enhancing healthcare accessibility for people with different types of disability.20,21 However, few mHealth programs are specifically designed for people with disabilities, and even fewer are certified for mobile app accessibility (eg, usability). Such certification would ensure equal access to mobile content for people with and without disabilities.22 -26
Study Objective
This study aimed to assess the feasibility and examine the effectiveness of a tailored mHealth intervention in improving health outcomes, physical function, and self-management behaviors among people with disabilities. To achieve this, we established a hybrid mHealth platform providing medical support services and customized healthcare programs to the disabled. The improved delivery of healthcare for the disabled was assessed by comparing health outcomes (eg, medication adherence, physical function, and chronic disease management) before and after the use of the app.
Methods
Study Design and Recruitment
The study participants were people with disabilities, 19 years and older, and residing in Cheongju, South Korea. Recruitment was through press releases and the distribution of promotional materials (leaflet, poster, banner) at facilities frequently used by people with disabilities (including Chungbuk National University Disability Support Center, Welfare Facilities for Disabled Persons, Organizations of Persons with Disabilities, and Braille Library).
Recruitment was conducted from September 2022 to February 2023 and, due to slower-than-expected enrollment and early attrition, was extended through May 2023, even after the demonstration project had begun. During the initial recruitment period, the target sample size was achieved (n = 69). However, 24 participants either withdrew immediately before study initiation or discontinued participation during follow-up for the following reasons: incompatibility of the mHealth app with older smartphones; difficulties operating connected devices such as blood pressure monitors and blood glucose meters; and skin irritation or allergic reactions caused by the fitness-tracker wristband. An additional 3 participants were recruited during the extended recruitment period, resulting in a final sample of 48 participants with physical disabilities, brain injuries, or visual impairments.
Study Implementation
As of June 1, 2023, the COVID-19 pandemic stage in South Korea was downgraded from severe to alert, such that the Infectious Disease Prevention and Control Act prohibited synchronous telehealth, which had been allowed for a limited time only during the severe stage. Because whether synchronous telehealth would still be allowed was unclear, we designed a demonstration scenario in which the initial medical visit was in-person and repeat visits were presumed to be synchronous telehealth.
The classification of PWD was based on the criteria established by Korea’s Disability Registration System, as defined in the Act on Welfare of Persons with Disabilities (Republic of Korea). 27 This registry recognizes 15 legally defined types of disability. For this pilot study, participants and their helpers (activity assistance services staff) were recruited, with the target population including individuals with physical disabilities, brain injuries, and visual disabilities. Physical disabilities include impairments such as amputations, joint disorders, limb dysfunction, and deformities. Disability with brain lesion is defined as a complex condition resulting from brain injury, while visual disability refers to impaired vision or visual field defects.
To ensure smooth access to the mHealth platform, each participant with a disability was paired 1:1 with a trained helper who provided targeted assistance only when necessary. While app usage, exercise tracking, and dietary reporting were primarily managed by participants, helpers supported tasks that could not be performed safely or feasibly alone. These included guiding exercise posture, accompanying participants to hospital visits for study procedures such as blood tests and physical function, and verifying measurement accuracy. Support for core self-management tasks, such as app navigation and data entry, was intentionally minimized to avoid influencing adherence or usability outcomes.
The intervention was primarily community-based, reflecting a community-based participatory research approach. Participants were recruited through local disability community, and the program was designed and implemented by the research team in collaboration with community nurses, dietitians, and exercise specialists. Chungbuk University Hospital served as the clinical partner, conducting baseline medical assessments, laboratory testing, and functional evaluations, and providing specialty consultations in family medicine, endocrinology, and rehabilitation. All intervention procedures were carried out according to a standardized protocol and operations manual to ensure consistency across participants and settings.
In addition, a fitness tracker, blood pressure monitor, and glucometer were distributed to allow physical measurements by the participants themselves through their connections to the app. And a preliminary survey was conducted to assess the general characteristics, disability characteristics (type and severity of disability, age of disability onset), health behaviors, disease history, and current eating habits.
Based on these results, synchronous telehealth sessions were delivered, including real-time medical consultations, counseling, and individualized coaching. In addition, ongoing monitoring and self-management were supported through the asynchronous mHealth platform, ensuring continuity of care between scheduled telehealth interactions.
On the day of the first in-person consultation, participants visited the hospital to undergo basic blood tests and physical function; based on the results, they were matched with a primary care physician (family medicine, endocrinology, or rehabilitation; Figure 1).

Study flowchart.
According to the chronic disease status and health risk factors, participants with 2 or more chronic diseases were classified into the disease group, those with 1 or more or borderline diseases were placed in the high-risk group, and those with no diseases made up the general group. This classification allowed the provision of customized healthcare services. All participants received medication education and counseling as well as nutrition education and health counseling; the exercise intervention program was offered only to 23 participants, as those who were physically unable to participate were excluded. To compare health status before and after participation, the same health surveys, blood tests, and physical function were administered at the end as at the beginning of the program. Usability surveys were administered midway through the program and at the end. Physical function assessments were not adjusted for disability type or impairment and were conducted uniformly across participants.
Intervention
The intervention programs were implemented from April to August 2023, with each participant engaging in their assigned components over a period of approximately 4 months. Counseling sessions, averaging approximately 15 min in duration, were conducted primarily in participants’ homes via synchronous telehealth to ensure accessibility and convenience. These sessions included physician consultations, counseling by nurses/dietitians, and exercise sessions.
The research team used the mHealth platform to continuously monitor participants’ engagement with the intervention and track session durations. Technical issues encountered during app use were promptly addressed, and necessary corrections were implemented efficiently.
Medication Education and Counseling
The medication education and counseling program was provided by licensed nurses with 10 years of experience. A total of 3 counseling sessions were conducted. The first session included rapport building with the participants and an educational program for disability awareness, adaptation, and acceptance. The second session consisted of medication counseling, medication adherence assessment, and general drug knowledge education. The third session provided counseling on digestion and bowel movements, sleep, obesity, depression, and the relationships needed to promote healthy living. For participants requiring additional support, individualized counseling was offered, addressing specific health conditions and including personalized discussions of diagnosed diseases, current medications, and inquiries about health foods.
Nutrition Education and Counseling
Participants received 3 to 7 sessions of nutrition education and disease counseling. These sessions focused on chronic disease management and were delivered by a nationally certified dietitian with a master’s degree in clinical nutrition and prior experience at a university hospital. Counseling was provided in a minimum of 3 and a maximum of 7 sessions, depending on individual needs. Dietary intake was assessed through the “Health On” mHealth app, and personalized dietary recommendations were made based on participants’ health conditions. Educational materials were also provided through the app to encourage healthier eating habits. In addition, weekly nutrition education materials were developed for each intervention group, tailored to participants’ chronic conditions and health risk factors, to ensure standardized counseling.
Exercise Intervention
The exercise intervention program was led by a licensed physical therapist currently working in a hospital setting. A rehabilitation physician provided ongoing medical oversight, including monitoring participant safety, reviewing program modifications, and offering consultations as needed to address specific medical considerations. The physical therapist was responsible for the program’s design and implementation. Exercise materials were uploaded to the mHealth platform to help participants remain active on days when formal sessions were not conducted. Exercise intensity was controlled using props such as resistance bands (eg, TheraBands). Heart rate and blood pressure were measured before and after each session to educate participants on the physiological changes resulting from exercise.
All exercise sessions were conducted synchronously in a virtual format, with groups of 1 to 5 participants to foster motivation and peer interaction despite physical distance. However, for participants with visual disabilities who had difficulty maintaining proper posture during these sessions, one-to-one helpers visited their homes to provide individualized support and ensure safe and correct performance.
The program was customized by the physical therapist based on participants’ self-reported feedback and disability-specific characteristics. This tailoring process was iterative, with adjustments made when participants experienced difficulties during exercises. Factors such as fall risk and joint use were also considered to ensure safety and appropriateness. For example, when a participant had difficulty maintaining a sitting posture due to joint strain—often occurring when one side bears more load because of an amputation—the movement was modified from prolonged sitting to repeated sit-to-stand exercises to reduce joint stress.
Although all participants received individualized support, additional assistance was provided to those with visual disabilities according to their specific needs. For these participants, professional video and audio guidance was supplemented with real-time, one-to-one support from assigned helpers.
Outcomes
In this study, a variety of assessment tools were employed to comprehensively evaluate participants before and after the intervention, including clinical measures, functional tests, survey-based outcomes, and usability ratings. Except for the usability assessment, all questionnaires and measurement tools were administered twice—prior to the start of the intervention and after its completion—to capture changes over time. These assessments were designed to objectively verify the effects of the intervention.
Clinical indicators and functional measures were obtained under the supervision of professional healthcare staff, including a clinical laboratory technologist at Chungbuk National University Hospital to ensure data reliability. Each outcome domain was assessed by the corresponding professional: nurses evaluated medication adherence, dietitians assessed nutrition-related outcomes, and physical therapists measured exercise and functional performance. This approach enabled a systematic assessment of the appropriateness and fidelity of each educational component according to its intended theme.
After the completion of all intervention components, participants who completed the program were additionally assessed for usability. This evaluation aimed to examine participants’ actual experiences with the program and to ensure alignment with the overarching goal of enhancing healthcare accessibility through mHealth services.
Statistical Analysis
Categorical variables are presented as frequencies and percentages; intervention groups were compared using a chi-square test. An analysis of variance (ANOVA) was used to assess differences in continuous variables between groups. Differences pre- versus post-intervention with respect to drug education, healthcare counseling, nutrition counseling and education, and exercise intervention were assessed using a paired-t-test. All analyses were performed using the SAS Enterprise Guide 8.3 (SAS EG). A P-value <.05 was considered to indicate statistical significance.
Results
Study Participants
The 48 participants were divided into 3 groups based on chronic disease status and overall health: the disease group (n = 19), the high-risk group (n = 20), and the general group (n = 9). The mean age was 61.1 years, with the disease group being the oldest (68.8 ± 7.2 years). A higher proportion of participants in the disease group were aged ≥ 65 years compared with the other groups (P < .0001). The sample included 26 males (54.2%) and 22 females (45.8%), with no statistically significant sex differences between groups. In terms of employment status, 36 participants (75.0%) were unemployed and 12 (25.0%) were employed, with no significant group differences (P = .829). Regarding educational attainment, 9 participants (18.8%) had completed elementary school, 11 (22.9%) middle school, 18 (37.5%) high school, and 10 (20.8%) college or higher (P = .415). The main types of disabilities were physical disability (n = 17, 35.4%), brain injury (n = 11, 22.9%), and visual disability (n = 20, 41.7%), with no significant differences across groups (P = .961). Overall, 32 participants (66.7%) had severe disabilities and 16 (33.3%) had mild disabilities (P = .206; Table 1).
Baseline Characteristics of Participants by Intervention Group.

Those participants with 2 or more chronic diseases.
Those with 1 or more or borderline diseases.
Those with no diseases.
The corresponding P-value represents the differences among the 3 groups as determined via ANOVA.
Effectiveness Outcomes
Medication Adherence
The medication-related intervention sessions were evaluated using 3 sets of questions: 6 items assessing participants’ counseling experiences regarding their current medications, 6 items measuring self-reported medication adherence behaviors, and 10 items evaluating general knowledge of medication use. Detailed results for each item are presented in the Supplemental Table 1.
The pre- and post-intervention comparison showed that General drug knowledge, significantly increased, from 6.8 (SD ± 1.9) to 9.3 (SD ± 1.6) (P < .001), with significant differences among the disease, high-risk, and general groups (P < .05). The provision of health counseling and medication adherence, increased from a mean of 2.6 (SD ± 2.2) to 3.4 (SD ± 2.5; P = .001). Analysis according to chronic disease status and health risk factors in the 3 groups showed that adherence significantly increased, from 3.4 (SD ± 2.0) to 4.3 (SD ± 1.8), in the disease group (P = .001).
Nutrition Practice
Mean total nutrition knowledge scores, which included topics such as sodium and sugar identification, increased from 11.7 (SD ± 2.5) to 12.2 (SD ± 2.5) following the program, although the difference was not significant (P = .114). For food safety and hygiene practices, the composite score increased from 23.2 (SD ± 3.0) to 24.6 (SD ± 4.0), but this change also did not reach statistical significance (P = .085). Within the 6-item questionnaire, participants demonstrated improvement in specific practices such as storing leftovers in the refrigerator (P = .014). The pre- and post-intervention outcomes of the nutrition education and counseling programs are shown, with detailed item-level results provided in Supplemental Table 2.
Exercise Physical Function
Physical function were assessed on 23 participants in the virtual exercise intervention program. Improvements were observed across all measures, with significant gains in 10 m walking speed, 2-min walking in place, arm curl, and the Timed Up and Go test (P < .05). Other measures showed improvement but did not reach statistical significance (Supplemental Table 3).
Table 2 presents a summary of overall effectiveness outcomes and after the intervention across the total sample (N = 48) and stratified by disease group, high-risk group, and general group. Outcomes of the sequential intervention components labeled A (Medication), B (Nutrition), and C (Exercise) were analyzed to capture comprehensive changes in participant health and behaviors.
Summary of Overall Effectiveness Outcomes Before and After Intervention.
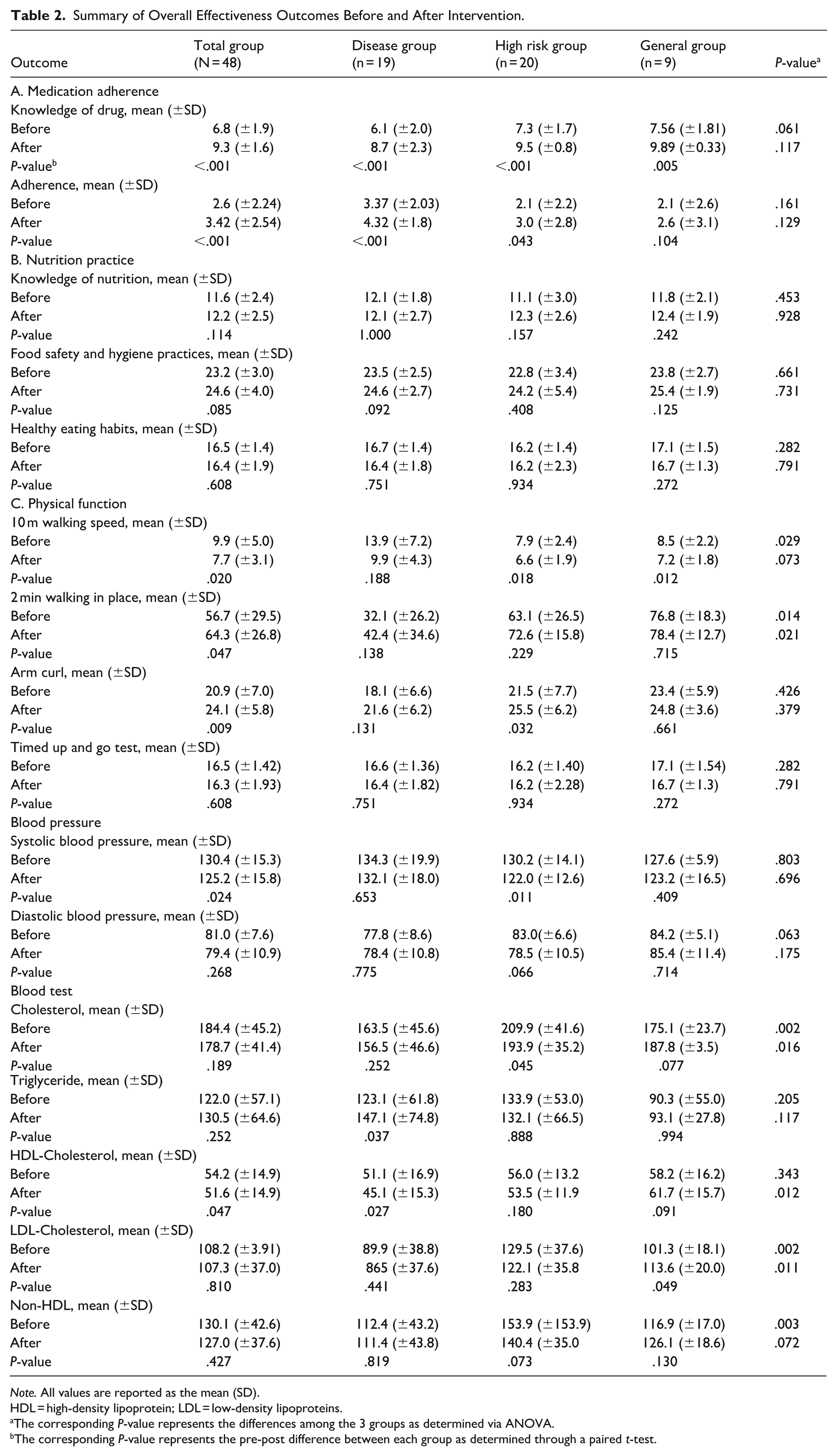
Note. All values are reported as the mean (SD).
HDL = high-density lipoprotein; LDL = low-density lipoproteins.
The corresponding P-value represents the differences among the 3 groups as determined via ANOVA.
The corresponding P-value represents the pre-post difference between each group as determined through a paired t-test.
Additionally, statistical comparisons within groups (pre- vs post-intervention) and between groups are included to highlight significant changes attributed to the intervention.
Key clinical and physiological indicators, including blood pressure and laboratory tests, were assessed to evaluate the effectiveness of the intervention program as summarized in Supplemental Table 4. Regarding blood pressure, the intervention group showed a statistically significant decrease from a mean of 130.4 mmHg (SD ± 15.1) before the intervention to 125.2 mmHg (SD ± 15.7) after the intervention, showing an average reduction of 5.2 mmHg (P = .022). Also among the blood tests, HDL-cholesterol (HDL-C) was significantly decreased (P = .023).
Feasibility Outcomes
This study was evaluated in accordance with Proctor et al’s Implementation Outcomes Framework (2011). This approach enabled systematically define, measure, and interpret feasibility indicators, thereby providing robust insights into the intervention’s clarity and accessibility.
A total of 69 individuals were initially recruited for the study. Before the start of the intervention, 24 participants withdrew, resulting in a 34.8% attrition rate. Following an extension of the recruitment period, 3 additional participants joined, leading to a final sample of 48 who completed the intervention. 66.6% of participants had severe disabilities, intentionally included to assess feasibility among those facing the greatest challenges, thereby enhancing study validity. Also, interviews with individuals with developmental disabilities indicated that several components of the digital and self-directed aspects of the program were challenging to implement in this population.
Participants reported that the program was easily accessible, noting simple procedures and remote counseling that minimized visits to healthcare facilities. Some technical difficulties, particularly with the synchronization between the mobile app and wearable devices monitoring heart rate and step counts, which highlighting areas needing improvement.
Telehealth sessions were delivered once per week for approximately 15 min by nurses, dietitians, and exercise specialists following a standardized protocol. Participants self-reported high engagement and perceived fidelity to the intervention procedures, with mean scores of 4.05 (SD ± 0.93) for focused preparation and 4.57 (SD ± 0.50) for active communication during synchronous telehealth, with an overall mean of 4.31.
Among the participants, 38 individuals (79.2%) used the app independently, while 10 individuals (20.8%) received assistance from a helper. For these independent users, ease of use was assessed using a 5-point Likert scale, with overall mean score of 3.47 ± 1.02 (Figure 2).

Users of the mHealth APP.
As this was a pilot study, detailed evaluation of implementation costs and penetration was limited. The mobile application remains active and available for ongoing use in self-management, suggesting preliminary evidence for sustainability beyond the study period.
Discussion
Key Findings
This pilot study demonstrated that a structured mHealth-supported health intervention yielded clinically meaningful improvements in multiple health indicators among adults with disabilities. After the 4-month intervention, participants demonstrated reductions in blood pressure, improved medication adherence, and enhanced physical function.
Comparison with Previous Work
Multidisciplinary and personalized mHealth improved the overall physical function and health status of the participants. The positive changes in health outcomes, particularly in body composition and blood pressure are consistent with previous studies showing that mHealth interventions can effectively improve these and other parameters.16,28,29 The improvements can at least in part be attributed to the impact of counseling and education on health management as well as the inclusion of an exercise programs as reported in other studies.30,31
Specifically, we observed a marked reduction in systolic blood pressure among participants, and a similar study reported that an mHealth interventions that included telemedicine education significantly reduced blood pressure in hypertensive patients. 32 This finding may reflect the fact that the disabled participants were able to take part in regular exercise programs in familiar places without transportation difficulties. In addition, drug counseling and education programs, as well as improved patient–provider communication, including medication reminders and individualized feedback on blood pressure trends, may have contributed to the positive outcomes. 33 In our study, education was provided on adherence to individualized medications, including dietary supplements, nutraceuticals, and disease-specific treatments. In addition to effective blood pressure management, mHealth interventions may help prevent or delay the onset and progression of chronic complications associated with hypertension. A meta-analysis found that a 10 mmHg reduction in systolic blood pressure reduces the risk of major cardiovascular events by 20%, the risk of coronary heart disease by 17%, and all-cause mortality by 13%. 34 These results demonstrate the importance of mHealth as a tool for blood pressure management in high-risk populations, including people with disabilities, and the potential of this approach to more effectively support chronic disease management.
We observed a decrease in HDL-C levels, which contrasts with some previous studies reporting improvements in HDL-C.29,35 HDL-C, often referred to as “good cholesterol,” plays a protective role in cardiovascular health, as higher levels are associated with a reduced risk of cardiovascular disease. 36 This divergence may be attributable to the relatively short intervention period; HDL-C typically requires 3 to 6 months to show meaningful elevation,37,38 whereas our study may not have provided sufficient duration for such changes to manifest. Nevertheless, the findings suggest that mHealth interventions may help maintain normal HDL-C levels, and longer-term follow-up studies would be needed to assess whether HDL-C levels improve with extended intervention duration.
PWD may find it more difficult to eat healthily, control their weight, and be physically active. 39 This might be due to physical limitations that can reduce a person’s ability to exercise, a lack of healthy food choices and medications that can affect weight and appetite. According to Lee et al’s analysis of obesity trends among persons with disabilities in Korea from 2008 to 2017, obesity and underweight were both more prevalent among persons with disabilities compared to persons without disabilities (PWoD). 40 Previous studies have shown that weight management interventions using mobile devices can promote weight loss and increase physical activity.41,42 In the present study, although no statistically significant changes were observed in body weight, body fat, body fat percentage, or basal metabolic rate (BMR), trends toward reductions in body fat and body fat percentage, as well as an increase in BMR, were noted. In contrast, significant improvements were observed in physical function, including faster 10 m walking speed and reduced 2-min walking-in-place time, indicating enhanced physical function among participants.
In addition, studies using mobile applications to improve nutrition behaviors among PWoD have shown that nutrition knowledge delivered through short-term nutrition education, health coaching, reminders, and/or diet tracking tools can lead to favorable dietary and health behavior changes in app users. 43 These findings suggest that similar mobile-based strategies may support nutrition-related behaviors change among PWD, as reflected in the positive trends observed in the present study.
Drug adherence is crucial for maximizing therapeutic benefits and minimizing adverse events. mHealth interventions were previously shown to have positive effects on drug adherence in patients with chronic diseases. 44 The disabled often have difficulty taking prescribed medications. For example, drug adherence for people with brain injuries estimated to be 49.5%, 45 ranging from 65.6% for stroke patients and 60% to 80% for those with multiple sclerosis.46,47 Moreover, compared to the non-disabled with chronic diseases, disabled people are less likely to be allowed to participate in drug adherence studies. Schwartz and Unni 48 reported that 34% of the studies excluded people with difficulty hearing, walking, seeing, and learning. We found that mHealth interventions can improve drug adherence in the disabled. Sufficient knowledge about medications is essential for patients to manage their own treatment and to understand the importance of drug adherence. The increase in medication knowledge scores demonstrates the effectiveness of patient education programs.
Overall, this study adds to the limited body of research examining mHealth interventions for people with disabilities, who are frequently excluded from clinical and digital health research. By implementing an integrated program addressing exercise, nutrition, and medication adherence, our findings provide new evidence for the feasibility and health benefits of inclusive mHealth strategies for reducing disparities in chronic disease management.
Implementation Insights
For people with disabilities, relying exclusively on mHealth tools for health support has inherent limitations. A hybrid model that integrates digital technologies with appropriate human interaction may therefore represent the more effective approach, combining technological efficiency with the personalized guidance and support often essential for this population.
The feasibility of implementing such hybrid approaches is reinforced by Korea’s established national activity support infrastructure. The Activity Assistance Services for People with Disabilities (AASPD) system, based on the 2011 Act on Activity Assistant Services for Persons with Disabilities, was created to support independent living for individuals with disabilities who face difficulties in daily and social activities. The program, known as Personal Assistant Services (PAS), has since evolved into a representative welfare initiative by progressively expanding its coverage. Moreover, with the abolition of the disability grading system in July 2019—previously used as the criterion for welfare service provision—eligibility has been broadened to include all persons with disabilities.49,50 Notably, the helper who facilitated technology adoption and program participation in our study are already deployed nationwide through this system, making the transition from research to real-world application highly feasible.
Also, the mobile app used in this study complied with the “Mobile Application Content Accessibility Guidelines 2.0” and was officially certified for accessibility by the Korea Web Accessibility Certification and Evaluation Institute under the Korea Federation of Organizations of the Disabled. This certification ensured usability equivalent to that of non-disabled users and enabled independent use by visually impaired participants through built-in smartphone accessibility features such as Apple’s VoiceOver and Samsung’s TalkBack.
Such strengths are also important in addressing the digital divide, as it can help reduce barriers to accessibility and engagement. In the era of AI, tackling the digital divide has gained new importance, resulting in policies targeting the digitally vulnerable not only in Korea but also around the world.51 -53 Even among OECD countries, digital divides with respect to geography, education, age, income, and company size have been identified. It is essential to bridge these gaps to create an inclusive digital future. Improving digital accessibility for PWD and limited access can include the further development of mHealth systems in response to user feedback on accessibility and usability.
Limitations
While the study provides valuable insights, several limitations should be acknowledged.
First, Participants were recruited from a subset of individuals engaged with disability-related services and those capable of using mobile devices. This recruitment strategy may have introduced selection bias, including Berkson’s bias, as such individuals may differ systematically from the broader population of people with disabilities. In particular, limiting participation to individuals already able to operate smartphones may have resulted in technology-related selection bias, thereby underrepresenting those with lower digital literacy or limited access to mobile devices.
Secondly, the small sample size (n = 48), the restriction to only 3 disability types, and the absence of a control group limit the generalizability of the findings and reduce the extent to which the observed changes can be attributed solely to the mHealth intervention.
Thus, careful consideration is needed regarding whether the limited sample adequately represents the target population and provides sufficient statistical power to validate the observed outcomes.
Third, a substantial attrition rate during recruitment raises concerns about the feasibility and acceptability of the intervention. Technology-related barriers, including incompatibility with legacy devices, usability challenges, and discomfort with wearable devices, were primary contributors. These findings highlight the need to incorporate strategies addressing technological barriers in future intervention designs.
Implications
The tailored hybrid mHealth intervention demonstrated preliminary effectiveness in improving health outcomes, physical function, and self-management behaviors among people with disabilities. These findings suggest that digital health services utilizing mHealth platforms can offer scalable and inclusive healthcare strategies for individuals with disabilities who experience limited healthcare accessibility. Building upon the current findings and limitations, future research should go beyond large longitudinal studies by adopting mixed-methods designs that incorporate stratified recruitment across disability types, include control groups, and integrate cost-effectiveness analyses.
Conclusions
This pilot study evaluated the potential of mHealth as a tool for improving healthcare accessibility for PWD and demonstrated its preliminary effectiveness in supporting health outcomes. Nevertheless, mHealth used in isolation remains insufficient in addressing the complex needs of PWD. A hybrid model that integrates technological interventions with personalized human support may provide a more effective solution for this population.
Building on the promising findings of this pilot study, large-scale and rigorous evaluations are warranted to examine the generalizability and sustained impact of such interventions across diverse disability populations. Additionally, proactive development and implementation of hybrid health system protocols, especially for emergency and disaster situations such as pandemics, along with active community education and engagement, are critical to ensuring equitable and sustainable healthcare access for PWD.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251411643 – Supplemental material for Feasibility and Preliminary Effectiveness of a Hybrid mHealth Intervention for People with Disabilities: A Pilot Study
Supplemental material, sj-docx-1-inq-10.1177_00469580251411643 for Feasibility and Preliminary Effectiveness of a Hybrid mHealth Intervention for People with Disabilities: A Pilot Study by Tae Hui Jang, Yu Jin Kim, Jong Eun Park, So Young Kim, Jae Woo Lee, Dong-Hwa Lee, Hyun Ho Kong, Hyo Jong Kim, Young Sung Lee and Jong Hyock Park in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board (IRB) of Chungbuk National University Hospital (CBNUH-2022-07-036-014). All participants provided written informed consent before their enrollment in the study. For participants who were unable to give consent due to difficulties with writing, verbal consent was obtained and written proxy consent was obtained from their legal guardians. Special attention was given to ensure that all information was communicated in an accessible manner to the disabled participants. To protect the privacy and confidentiality of participants, all data are presented in aggregate, and no personally identifiable information is included.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the Korea Agency for Infrastructure Technology Advancement (KAIA), and by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Korean government (No. 2022R1I1A3070074 and No. RS-2024-00394642), and by the Regional Innovation System & Education (RISE) program through the Chungbuk Regional Innovation System & Education Center, funded by the Ministry of Education (MOE) and Chungcheongbuk-do, Republic of Korea (No. 2025-RISE-11-014-02).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.