
Abstract
Site-neutral payment reforms seek to align Medicare reimbursement rates for common outpatient services across care sites. Recent reports have assessed the composite impact of site-neutral payment policies on beneficiaries, federal savings, and the commercial market. This analysis builds on such work, focusing on the potential patient-level savings of site-neutral reform for high-utilizing Medicare beneficiaries facing common chronic cancers. We compiled the outpatient services of standard treatment regimens for a typical lung, ovarian, prostate, and colon cancer patient over their first year of treatment. By simulating scenarios for these patients in which hospital outpatient rates were and were not aligned with those of independent physician offices for the 57 service classifications recommended by the Medicare Payment Advisory Commission (MedPAC), we were able to estimate the effect of site-neutral payments on patient out-of-pocket cancer costs. We found that expanding site-neutral payments for MedPAC’s recommended services would greatly reduce Medicare cancer patients’ outpatient out-of-pocket share, with certain beneficiaries saving over $1000 in out-of-pocket spending in their first year of cancer treatment. Along with patient savings, site-neutral payment expansion would produce larger Medicare fee-for-service savings that average over $5500 per cancer patient for the 4 standard cancer treatments analyzed. The largest portions of Medicare and patient savings with site-neutral payments for these 4 cancers came in the form of drug administration costs, particularly when chemotherapy was included as a part of treatment. The findings of this analysis suggest that existing regulatory and legislative site-neutral proposals have the ability to save Medicare and its higher-need beneficiaries thousands of dollars per patient when treating typical lung, ovarian, prostate, and colon cancer cases.
Introduction
Due to rising healthcare costs, elderly Americans are facing significant increases in out-of-pocket (OOP) spending on their healthcare. OOP spending for consumers over 65 comprised 13.6% of individuals’ expenditures in 2019, and total out-of-pocket expenditures increased by 41% since 2009. 1 Over 1 in 5 elderly Americans now report debt due to medical bills. 2 The increase in OOP spending for Medicare beneficiaries is directly related to the increase in Medicare spending, which now extends to over $1 trillion a year. 3 However, as Medicare costs continue to grow each year, service prices and reimbursement levels have not risen evenly across all facilities. Between 2017 and 2022, the commercial prices of common services at hospital outpatient departments (HOPDs) grew 13 times faster than at independent physician offices. 4 Medicare payment policy contributes to and reinforces these disparities by reimbursing HOPDs 2 to 4 times more than independent physician offices for identical services. 5 The sizable and growing discrepancy in Medicare payment rates for common outpatient services based on the site of service has prompted bipartisan calls for more balanced payment rates.
Site-neutral payment policies can address these longstanding payment disparities. Under current policy, Medicare reimburses hospital outpatient departments at higher rates than independent physician offices, even when the specific clinical care delivered is functionally identical. This creates incentives that drive unnecessary Medicare spending growth, market consolidation, and higher patient cost-sharing obligations. In contrast, site-neutral payment policies seek to equalize Medicare payment rates for health services regardless of the type of facility in which they are provided. Site-neutral policies do this by adjusting Medicare’s service rates for HOPDs, paid under the outpatient prospective payment system (OPPS), to align with those of lower-cost sites, including physician offices, which are reimbursed under the Medicare physician fee schedule (MPFS).
While much of the policy discussion around site-neutral payments has focused on federal program savings, its implications for Medicare beneficiaries’ out-of-pocket (OOP) costs, particularly those suffering from chronic conditions, warrant closer examination. Medicare spending on cancer-related care has grown steadily over the past 20 years and is expected to balloon to over $246 billion by 2030. 6 Alongside a larger Medicare population, survival rates and treatment costs have increased the average cost per beneficiary, while patients increasingly struggle to afford their subsequent out-of-pocket portion. 7 Medicare beneficiaries with new cancer diagnoses spent on average 23.7% of their household income on OOP expenditures alone. 8 Consequently, 53% of cancer survivors on Medicare reported a degree of difficulty affording their OOP cancer costs. 9 More than ever, finding ways to lower OOP cancer costs can meaningfully benefit Medicare and patients alike.
Cost-sharing obligations in Medicare are typically calculated as a percentage of the Medicare-allowed payment amount; therefore, reducing the underlying payment rates for certain services can lower costs faced by patients. For outpatient services covered by Medicare Part B, beneficiaries are typically responsible for paying 20% of the Medicare-approved rate out of pocket. 10 This cost-sharing mechanism ensures that a portion of the government savings generated from reducing reimbursement rates is necessarily passed on to the Medicare beneficiary receiving the service. An evaluation by Actuarial Research Corporation estimates that comprehensive site-neutral reform would lead to Medicare beneficiaries saving an average of $114 per year. 11 However, in practice, sicker and higher-need beneficiaries can be expected to save significantly more.
The Leukemia and Lymphoma Society, with Wakely, estimated that for a standard non-transplant multiple myeloma patient, site-neutrality would save a patient $1220 in OOP costs for 1 cycle of treatment. 12 When evaluating the potential savings for a hypothetical breast cancer patient, the American Cancer Society Cancer Action Network (ACS CAN) estimated that aligning rates would save a beneficiary $1550 in OOP costs over 1 year. 13 Our analysis builds on these findings by looking at the prospective patient-level savings from applying site-neutral payment policies to the first year of treatment for some of the most common types of cancers in older Americans. 14 Collectively, along with breast cancer, lung, ovarian, prostate, and colon cancers make up over half of all new cancer cases. 14 Analyzing the effects of site-neutral payments on a typical case of these additional cancer types offers insight into how reform could affect millions of older Americans, while also contributing to a larger discourse on how higher-utilizing Medicare beneficiaries with cancer may be uniquely impacted by this policy.
We find that site-neutral payment savings are notably pronounced for cancer cases due to the high frequency and cost of diagnostic and treatment procedures, in particular chemotherapy. This is largely due to significant payment differentials between hospital drug administration and other sites. Outpatient hospital administration costs are approximately 4 and 8 times higher than physician office and home infusion, respectively. 15 Using the Centers for Medicare and Medicaid Services (CMS)’s claims-based payment rates, we estimate the specific cost-sharing reductions a typical beneficiary would see under a policy scenario that aligns HOPD reimbursement rates with those of physician offices. For expected outpatient services involving drug administration, imaging, labs, and supportive care, we find that cancer patients would see significant savings from an expansion of site-neutral payments. Lung and colon cancer patients would be expected to see over $1000 in savings in their first year of treatment, while ovarian and prostate cancer patients would see between $750 and $950 in savings. By quantifying the out-of-pocket savings for standard cancer cases in Medicare beneficiaries, this analysis aims to inform ongoing policy debates about the patient-level impacts of site-neutral payment reforms. Its results highlight the capability for site-neutral policies to improve affordability for patients undergoing cancer treatment.
Legislative Proposals
Past administrations have implemented a highly limited application of site-neutral payments, which current proposals seek to expand. The Bipartisan Budget Act (BBA) of 2015 initiated site-neutral payment reform for services provided in new off-campus HOPDs. In 2019, the first Trump Administration expanded the regulation to include clinical office visits (services with CPT evaluation and management [E&M] codes) at off-campus HOPDs, ending grandfathering for these clinic visits; however, the updated 2019 rule maintained the “grandfather” exceptions in Section 603 of the BBA for other services at hospitals in operation prior to 2015. 16 Since implementation began in 2021, site-neutrality only applies to 19% of HOPD facility spending and less than 1% of OPPS spending. 17
Congress has recently proposed several legislative reforms to expand site-neutrality to additional facilities and services. In May 2025, Senator John Kennedy (R-LA) introduced S.1629, the Same Care, Lower Cost Act, which would both close the BBA grandfather exemption and establish site-neutrality for 66 ambulatory payment classifications (APCs)—and any additional ones determined by the Secretary—for all facilities, including on-campus HOPDs. 18 This policy is in accordance with the recommendations made by the Medicare Payment Advisory Commission (MedPAC), a nonpartisan commission established by Congress to advise it on Medicare, which identified 57 APCs that are regularly provided at non-hospital sites and can be safely provided in freestanding offices and an additional 9 APCs they recommend aligning with ambulatory surgical center (ASC) rates. 19 These 57 APCs are frequent, but low-cost services. While they account for 71% of Medicare’s total volume in terms of the number of services performed, the total spending on these services is between $11 and $12 billion (around 20% of OPPS spending). 20 While an official budget score has yet to be released, based on past ratings by the Congressional Budget Office (CBO), some estimate that this bill could save $150 billion over the next 10 years. 21
Last year, Senators Bill Cassidy (R-LA) and Maggie Hassan (D-NH) released the Lowering Health Costs For Seniors Framework, which recommends applying current site-neutral service requirements to all off-campus HOPDs by removing the BBA hospital grandfather exemptions or extending site-neutrality to all common outpatient services. 22 The framework also considers methods to reinvest part of the federal government savings back into rural and high-need hospitals.
Not all site-neutral reforms require Congressional action, however. CMS also has large discretion over Medicare payment rates. In July 2025, CMS released the first outpatient fee schedule of the new Trump administration, which included applying site-neutral payment rates to drug administration (ranging from simple IV injections to chemotherapy drugs) services performed in grandfathered off-campus HOPDs. Specifically, these services would be reimbursed at 40% of the standard OPPS rate. CMS estimates that, if implemented, this rule would reduce OPPS expenditures by approximately $280 million in 2026. 23
In line with recent legislative discussions, this analysis will consider the scenario in which site-neutral payment reform applies to the 57 service classifications that MedPAC recommends aligning OPPS payment rates across care sites. For MedPAC’s recommended services, we calculate the potential savings a given individual would experience with site-neutral payments on a model treatment plan. Thus, our patient-level findings will not differentiate based on which HOPDs are included; however, the scope of HOPDs to which site-neutrality applies determines whether or not an individual can access the estimated savings in practice. Policy reform could cover only off-campus HOPDs, which would come from eliminating the BBA grandfather exemption, or all HOPDs, as is applied in Senator Kennedy’s bill and considered in Senators Cassidy and Hassan’s framework. The more expansive policies that apply to all HOPDs would broaden the number of individuals able to access OOP savings, as well as substantially increase total Medicare savings.
Methods
To assess the potential impact of site-neutral payment reform on common cancer patients’ OOP savings, we created an archetypal Medicare patient profile with lung, ovarian, prostate, and colon cancer, respectively. Patients were assumed to have original fee-for-service (FFS) Medicare coverage (this excludes Medicare Advantage [MA] members and dual Medicaid-Medicare enrollees) and have a standard case of cancer, without high levels of malignancy or spread. All cancer patients were assumed to be responsive to treatment, with no extraneous side effects that may require further outpatient services beyond the cancer diagnosis and treatment. Using real-world claims data and the National Comprehensive Cancer Network (NCCN)’s Clinical Practice Guidelines in Oncology, we compiled lists of the typical outpatient services and their frequency that each type of cancer patient would be expected to receive in their first year of treatment (see Supplemental Appendices B–E). 24
For each outpatient service that corresponded with an APC on MedPAC’s site-neutral recommended list, we calculated the difference between CMS’s listed OPPS reimbursement payment rate and MPFS rate for CY2025. Considering site-neutral policies would reduce OPPS rates to match those of the MPFS, the combined difference in payment rates for all services represents the total Medicare savings for a given cancer patient in their first year of treatment. This method follows how MedPAC recommends aligning payment rates under site-neutrality and is consistent with those used by Wakely and ACS CAN to predict patient-level savings. For more information on how savings were calculated, including in special cases involving split payment services, see Supplemental Appendix A. Using Medicare’s 20% cost-sharing rate, an individual cancer patient’s expected out-of-pocket savings for their first year of treatment is then one-fifth of the total Medicare reimbursement difference.
Results
We found that aligning outpatient payment rates would substantially reduce a standard lung, ovarian, prostate, or colon cancer patient’s out-of-pocket costs in their first year of treatment. Implementing site-neutral payments would save Medicare between $4000 and $8000 per patient, depending on the type of cancer, with a patient averaging over $1000 in savings across the 4 types of cancer we analyzed.
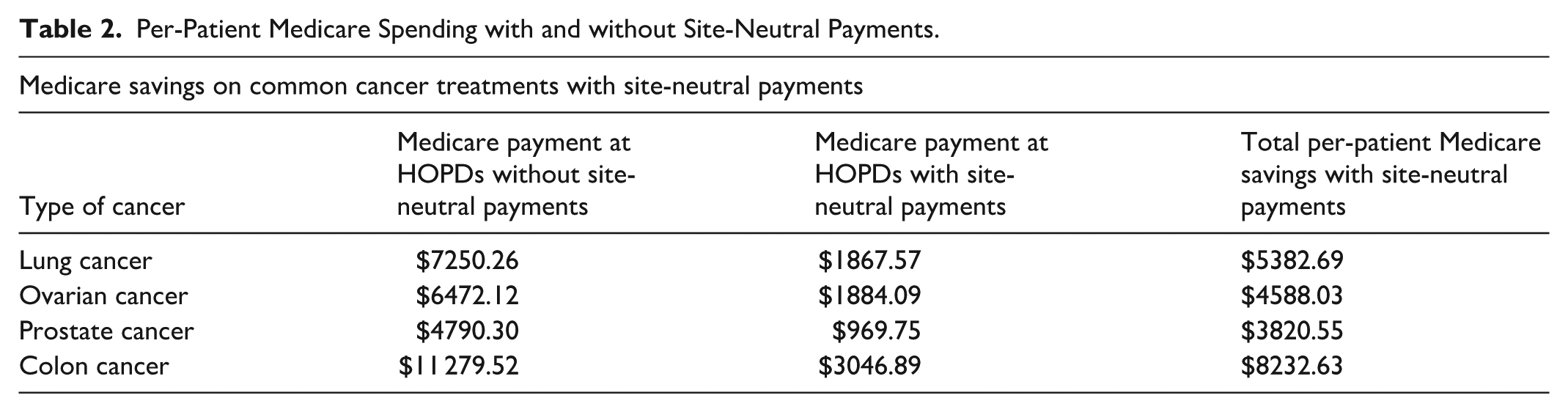
Specifically, the total estimated savings for Medicare of implementing site-neutral payment for a lung cancer patient is $5382.69. Due to the 20% copayment, a typical patient would save $1076.54 in OOP costs for their first year of treatment. Applying that same calculation to ovarian, colon, and prostate cancers reveals a similar breakdown across all 4 cancers (see Table 1).
Cancer Patients’ Out-of-Pocket Costs with and without Site-Neutral Payments.

Table 1 shows the expected out-of-pocket patient costs for the respective cancer treatments in the status quo in comparison to if OPPS and MPFS payment rates were aligned with site-neutral reform. For each of the cancer treatments, site-neutrality could reduce the vast majority of patients’ OOP costs. The difference between these estimates with and without aligning payment rates represents the expected patient savings in their first year of treatment that would be gained from implementing site-neutral payment policies.
In addition to the out-of-pocket savings, although we do not include it in our estimates here, patients would also expect to see a separate reduction in their Medicare Part B premium rates.
This is because premium rates are adjusted by CMS according to service price changes and assumed utilization, such that federal budgetary savings from site-neutral payments would result in lower Medicare Part B premium rates. 25 Estimates in Part B premium reductions from expanding site-neutrality range from $43 billion to $67 billion over 10 years. 26 Site-neutral payment savings for the Medicare program, hence, rollover to further benefit patients through premium reductions. Table 2 shows the drop in Medicare spending per patient from applying site-neutral payments to HOPDs for the 4 types of cancer.
Per-Patient Medicare Spending with and without Site-Neutral Payments.
Discussion
These results suggest aligning Medicare payment rates across sites would significantly reduce the cost on cancer patients for life-saving treatment. A significant portion of the estimated patient savings is attributable to payment differentials for drug administration services. For lung, ovarian, and colon cancer patients, these services come in the form of chemotherapy and related services. This is consistent with average treatment methods, where over half of colon cancer patients receive chemotherapy and around three-quarters of ovarian and lung cancer patients are recommended for chemotherapy.27 -29 For prostate cancer patients, who we did not assume underwent chemotherapy in our analysis, drug administration services in the form of hormone therapy and bone health infusions comprised over half of patient savings.
Our results for lung, ovarian, prostate, and colon cancer are consistent with prior analyses estimating high site-neutral savings for curative cancer treatments, and in particular for chemotherapy. In their report on savings for a hypothetical breast cancer patient, ACS CAN noted that the vast majority, or around $1305, of expected savings were from chemotherapy administration alone. 30 In a broader evaluation of proposed site-neutral policies, a report from Actuarial Research Corporation estimated that an average chemotherapy patient would gain over $400 in cost-sharing savings, with high-need patients saving upward of $1000. 31 Taken together, these findings reinforce the plausibility and significance of our estimates.
In its proposed 2026 rule for the OPPS, CMS includes a version of site-neutrality for drug administration services. But rather than aligning OPPS rates to match MPFS, as we did in our analysis and Congressional site-neutral proposals have sought to do, CMS has proposed a blanket reduction of OPPS to 40% of current drug administration service rates. This is consistent with previous site-neutral rules implemented by CMS from the 2015 BBA and 2019 expansion. 32 While this policy would help to reduce the disparity between OPPS and MPFS payment rates, its blanket application would result in less savings than if OPPS and MPFS were truly aligned. Our analysis suggests that for many common cancer outpatient services, Medicare presently reimburses HOPDs as much as 1.5 to 6 times more than freestanding clinics for the same services. For the 4 cancer treatment regimens analyzed, we quantified the difference in potential patient and Medicare savings from implementing a 40% benchmark as compared with our site-neutral results from aligning payment rates. Tables 3 and 4 show the difference in savings potential for drug administration services in common cancer treatments under each of these site-neutral policies. Differences in savings potential for all MedPAC-recommended APCs under this alternative site-neutral rollout can be found in Supplemental Appendix F.
Patient Savings Potential under Different Site-Neutral Payment Policies.

Per-Patient Medicare Savings Under Different Site-Neutral Payment Policies.

Under site-neutral payment reform where OPPS rates are tied directly to MPFS, cancer patients have the potential to save up to a few hundred dollars more in out-of-pocket costs on drug administration services in their first year of treatment than if a 40% OPPS “haircut” policy were enacted. Likewise, for these compiled standard cancer treatment regimens, the Medicare program has the potential to save from a few hundred dollars to almost $1500 more per patient under a policy where rates are exactly aligned.
Beyond drug administration services, limiting site-neutral application only to services included in MedPAC’s current classification list plays a role in these calculations. Our analysis identified several outpatient services commonly used in standard cancer care that fall outside MedPAC’s list despite being routinely delivered in both independent physician offices and HOPDs. This is especially true for imaging services used for diagnoses and monitoring, such as CTs with contrast, MRIs with or without contrast, full-body PET scans, and bone scans. Additionally, certain categories of outpatient services are bundled or packaged differently in APCs and so do not receive a separate reimbursement. This notably includes lab panels, which are paid according to CMS’s Clinical Laboratory Fee Schedule (CLFS), though still packaged under OPPS when provided in HOPDs. 33 Despite not having cost-sharing payments for Medicare beneficiaries under CLFS, lab panels may induce higher patient costs when bundled into larger OPPS payments. Moreover, while CMS expanded site-neutrality to encompass clinical visits at all off-campus HOPDs in 2019, certain office visits and all visits at on-campus HOPDs are excluded. If these or additional services were considered in future site-neutral policies, Medicare savings and reductions in beneficiary cost-sharing could be greater than our estimates here. The specific outpatient services common to cancer treatments that were excluded from our final savings calculations are noted accordingly in the tables in the Supplemental Appendices.
Implications and Limitations
Our results estimate the patient-level savings if a site-neutral policy aligning payment rates was applied to current OOP and Medicare program costs for standard cancer treatments. However, it can be anticipated that following the implementation of comprehensive site-neutral payment reform, there will be recalibrations in the provider market. Hospitals may try to offset these losses by increasing the frequency of services not covered by reform, redirecting more people to inpatient or emergency care, or adjusting financing schemes and political appeals to extract revenue from other channels. Each of which would erode savings for patients in the aggregate.
Conversely, by eliminating a financial incentive for hospital systems to buy out independent physician offices, site-neutral payment reform has been predicted to lead to more long-term competition in the healthcare market, which could lower service prices. There would likely also be a direct reduction in negotiated rates. Because Medicare FFS rates serve as the benchmark for the rates of many private plans (both employer-sponsored insurance and ACA marketplace plans), a reduction in OPPS rates would reduce the fee benchmarks in the negotiations between insurers and providers, putting further downward pressure on prices. It is unclear at this time the extent to which these shifts will occur following the enactment of site-neutral reform, though the outcomes will no doubt help determine where precise patient and program savings land.
Rather, our savings estimates for cancer patients are best understood as a reduction in the hypothetical patient’s financial responsibility. Forty-two percent of traditional Medicare beneficiaries, especially those with heavier utilization patterns, opt to purchase Medigap policies to cover their remaining OOP costs. 34 As a result, those individuals with comprehensive Medigap coverage would not experience the patient-level savings directly, as they do not pay their coinsurance costs out-of-pocket. However, we can expect that a robust site-neutral payment policy would result in a reduction in Medigap premiums due to lower claims paid out by Medigap insurers. This is because when Medicare’s allowed charge for a service drops, the amount that Medigap must pay on behalf of its enrollees also decreases.
While this paper does not provide savings estimates for Medicare Advantage beneficiaries, site-neutral payments may additionally have important implications for MA premiums. We can expect that a reduction in hospital outpatient payments will lower overall plan costs and would allow MA plans to make lower bids. These lower bids and decrease in plan costs should have the spillover effect of reducing supplemental premiums charged to enrollees. Studies estimate that broadly adopting site-neutral payments could lower private health plan premiums by around 0.75%, which includes MA premiums. 35 But without a body of research that explores the relationship between site-neutral payments and MA premiums, exact impacts remain difficult to estimate.
Notably, for the standard cancer regimens used in our analysis, we assumed treatment was the goal of all health services. However, many older patients may forego best-outcome treatments in favor of those known to lead to fewer side effects. This is particularly true of chemotherapy, which can be intensive with potential for complications. Likewise, some patients may decide to pursue palliative care routes instead. For this analysis, we followed curative treatment recommendations and did not consider these scenarios. To analyze the potential savings of treatment costs, we made judgments based on real-world data and professionals’ recommended best practices. Nonetheless, we recognize that individuals’ specific cancer treatment decisions can be highly personal, and patients’ savings results may vary considerably from our estimates accordingly.
Finally, our results should be viewed as baseline savings, pertaining only to direct outpatient cancer costs for a hypothetical patient. Patients with more intensive regimens, procedure complications, or treatment side-effects—all of which are more likely for older adults—may incur higher service utilization, leading to higher levels of savings. Those who receive care at cancer hospitals and large urban hospitals, where costs tend to be higher in the status quo, are likely to see more savings relative to those who typically receive care at independent oncology clinics or smaller hospitals. And, while this analysis focuses on the initial year of cancer treatments, ongoing follow-up and surveillance care in subsequent years may extend the policy’s financial impact. Each individual’s cancer treatment will undoubtedly vary on a case-by-case basis. These estimates represent a starting point based on common treatment patterns, demonstrating that even under limiting assumptions, potential patient savings can be substantial.
Conclusion
Almost half a million Medicare beneficiaries will face new lung, ovarian, prostate, or colon cancer cases this year. 36 Our findings show that those patients could experience, on average, over a thousand dollars in annual savings if site-neutral payments are expanded to hospital-owned or operated outpatient clinics.
As policymakers seek strategies to contain Medicare spending, site-neutral payment policies present a rare opportunity for both substantial federal and patient-level savings. Between ongoing bipartisan legislative efforts to align payment rates and the recent proposal from CMS to make drug administration services site-neutral, lawmakers have vetted, proven options for improving the sustainability of the Medicare program and reducing the financial burden on its most vulnerable beneficiaries.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251401460 – Supplemental material for Estimating Out-of-Pocket Savings From Medicare Site-Neutral Payments on Colon, Lung, Ovarian, and Prostate Cancer Patients
Supplemental material, sj-docx-1-inq-10.1177_00469580251401460 for Estimating Out-of-Pocket Savings From Medicare Site-Neutral Payments on Colon, Lung, Ovarian, and Prostate Cancer Patients by Sage Mehta and Lawson Mansell in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Ethical Considerations
Ethical approval was not required.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by Arnold Ventures.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This work was supported in part by Arnold Ventures, an organization that promotes site-neutral payment policies.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.