
Abstract
Telehealth has expanded access to psychotherapy for veterans, yet little is known about how art therapy is experienced in remote formats. In this paper, we describe a thematic analysis that involved male and female veterans with PTSD and TBI (aside from one participant without a TBI) in individual telehealth art therapy. This paper explores the similarities and differences in male and female veterans’ engagement in art therapy. Nine veterans (6 male, 3 female) diagnosed with PTSD (with most also having TBI) participated in eight sessions of individual telehealth art therapy. Clinical notes, session summaries, and artwork were analyzed using thematic analysis to identify key patterns in veterans’ therapeutic experiences. Three primary themes emerged from the data: a) Striving to manage self and emotions; b) Diverse relationships with artmaking and media; and c) Seeking to improve interpersonal connection. Telehealth art therapy supported emotional expression, trauma processing, and relational insight in veterans with PTSD and TBI. The findings underscore the value of flexible, personalized approaches in remote care and demonstrate how art therapy can be meaningfully adapted for telehealth delivery and meet the needs of diverse participants. Future research should explore hybrid models, individualized interventions, and the influence of identity and environment on therapeutic engagement and outcomes, as well as the possibly unique experiences of male and female veterans.
Keywords
● Art therapy delivered via telehealth offers increased access to psychotherapy for veterans with PTSD and TBI, addressing barriers to in-person care.
● The study compared how male and female veterans engaged with art therapy, revealing both shared and distinct patterns in emotional and relational processing.
● Three central themes were identified: (a) managing self and emotions, (b) diverse relationships with artmaking and media, and (c) seeking interpersonal connection.
● Telehealth art therapy fostered emotional expression, trauma processing, and relational insight, demonstrating adaptability and efficacy in remote care.
● Further studies should examine hybrid models, individualized interventions, and how identity and environment influence engagement and outcomes.
Background
Active-duty military personnel and veterans often grapple with the dual challenges of post-traumatic stress disorder (PTSD) and traumatic brain injury (TBI). Diagnosing and treating these conditions can be complex due to overlapping symptoms. PTSD develops after traumatic events, with symptoms such as hypervigilance, intrusive memories, and emotional numbness. Early identification and intervention are crucial. 1 TBI occurs when the brain is damaged from head trauma, with symptoms ranging from mild (headaches and dizziness) to severe (loss of consciousness and seizures). 2 Many symptoms, such as poor concentration and irritability, overlap with PTSD. This co-occurrence complicates treatment, as both conditions can fluctuate in response to stress and sleep quality. Veterans with PTSD with/without history of TBI show altered brain activity, particularly in regions related to emotional regulation, potentially complicating recovery. 3 Irritability and anger are common in this population. 4
PTSD and TBI in Military Populations
PTSD with/without history of TBI is common among veterans, particularly those with combat exposure.1,5 Exposure to combat environments with constant threat, witnessing death or injury among peers, military sexual trauma (MST), and extended deployments can significantly impact mental health. 6
Mild TBI (mTBI), the most common head injury type in veterans, is characterized by a brief loss of consciousness or altered mental status mostly due to deployment-related head injuries, particularly resulting from blast exposures. 7 Most people recover quickly from mTBI, but it can increase the risk of emotional dysregulation and PTSD. The mechanistic link between TBI and PTSD is unclear. Repetitive mTBI carries an increased risk of accelerated trajectories of altered brain health, chronic traumatic encephalopathy, other neurodegenerative disorders, and life-long diseases. 8 Recovery from TBI and PTSD is heterogeneous, with some patients experiencing more chronic symptoms as well as relapse.1,7 A gap remains in understanding the neuropathology of impact and blast exposure and the combined effects of TBI and PTSD on veterans’ mental health. 1 Nevertheless, some studies suggest that veterans with history of both PTSD and mTBI are less responsive to first-line treatments, 9 experience underemployment, and decreased access to treatments.
Impacts of PTSD
PTSD imposes a significant illness burden on military personnel, often co-occurring with depression, substance use disorders, and TBIs.5,10 Up to 17% of US veterans are affected by PTSD, with female veterans experiencing a 2.5 times higher risk of suicide than civilian females.10 –12 The Department of Veterans Affairs, reported the suicide rate among veterans is 1.5 times higher than among civilians, with an estimated 6042 male and 350 female suicide deaths in 2021. Male veterans often face higher rates of substance use disorders, while female veterans are disproportionately affected by depression and suicide.13,14 Studies show mixed findings on differences in PTSD relating to male and female identities, with higher risk reported for women in some cases but not universally.3,14 –16 Women are less likely to be exposed to TBI and combat stress in the military, but report higher rates of MST and interpersonal violence.6,17 With female veterans’ pre-existing vulnerabilities, social support, health profiles, and experiences are also different. 18 Servicewomen consistently report higher PTSD symptoms than servicemen, particularly after combat trauma. 19
PTSD causes challenges with relationships, employment, and well-being, often leading to a diminished sense of purpose and fulfillment. 10 While female veterans are more likely to seek mental health services, they often discontinue psychotherapy and psychopharmacology earlier than male veterans. 20 Race and ethnicity are related to PTSD, as Black and Hispanic veterans report more severe PTSD, depression, and anxiety symptoms. 21 Marginalized identities relating to race and sexual orientation (among others) are associated with increased rates of homelessness and suicide.22,23 Perceptions of therapist care, therapeutic milieu, and attitudes and compliance with medication management, influence treatment retention and outcomes.20,24
Treatment Approaches
Efforts to increase accessibility to mental health services for veterans have produced incremental improvements, but significant stigma and barriers remain surrounding leadership attitudes and negative impacts on career.25,26 Various interventions offer different strengths, underscoring the need for consistent, evidence-based care. 27 Family and peer support are vital for recovery, yet caregivers often face their own psychological burdens. 27 Empirically supported psychotherapies such as Prolonged Exposure (PE), Cognitive Processing Therapy (CPT), and Eye Movement Desensitization and Reprocessing (EMDR) have mixed effectiveness for military-related PTSD, with studies indicating that between 30% and 51% of patients did not experience clinically meaningful improvement and 60% to 72% continued to meet diagnostic criteria following treatment.28,29 High dropout rates with PE and CPT were observed, highlighting the need for more personalized approaches. 30 Art therapy shows promise in alleviating symptoms and improving well-being,31,32 but more research is needed to understand the impact of a range of methods and approaches. 33
Art Therapy with Military Populations
Art therapy has been used in military settings for supporting service members’ mental health, offering an alternative and complement to CPT and PE.34 –36 Art therapy is a “mental health profession” that integrates “active art-making”, creativity, and psychology “within a psychotherapeutic relationship” to enhance cognition and “emotional resilience,” improve insight, and reduce distress. 37 In the US, art therapists have a Master’s degree or higher, national credentials, and/or state licenses and develop individualized art therapy interventions to support clinical goals by offering a diverse range of art forms and techniques. In this way, art therapy is conceptualized as a profession that uses clinical, art-based psychotherapeutic interventions to support the needs of those receiving art therapy services. The art therapy approach described in this study is an example of one such intervention aimed at reducing symptoms of PTSD and improving quality of life among veteran participants.
Art therapy offers parallels to empirically supported psychotherapies, such as supporting individuals in expressing and processing their experiences when words are insufficient, making it helpful in addressing symptoms of TBI and PTSD.38,39 Research highlights its effectiveness in reducing PTSD and TBI symptoms while building coping mechanisms. 40 The heterogeneity and flexibility of art therapy support individually tailoring interventions, underscoring agency and empowerment, which are critical for those navigating trauma. 41 A study of 204 military service members with PTSD and TBI found that long-term art therapy facilitated trauma processing, evoked positive emotions, and reduced feelings of guilt and grief. 42
The treatment goals of art therapy for active-duty military personnel and veterans share similarities in addressing trauma, fostering emotional regulation, and promoting identity integration. However, differences reflect their life circumstances and challenges. Both groups benefit from art therapy’s nonverbal processing of trauma, externalization of emotions, and reduced isolation.32,42 –44 Common goals include enhancing emotional regulation, promoting self-efficacy through artmaking, and fostering interpersonal connection.38,45 Group art therapy supports shared experiences, enhancing group cohesion for active-duty members and reducing isolation for veterans.36,46Active-duty military members often focus on short-term stabilization and safety to meet the demands of military life. 46 In contrast, veterans prioritize reconstructing their identities and creating visual narratives to make sense of past experiences. Art therapy for veterans also addresses grief and trauma in a safe, non-military environment, often focusing on re-entering civilian life and fostering overall well-being. 36
Art therapists use various techniques, such as drawing, collage, and quilting to help veterans express emotions and process trauma. 47 Mixed-media montage painting helped active-duty service members articulate combat-related symptoms. 38 In addition, innovative participatory approaches, such as involving veterans and active-duty military in co-researching art therapy methods, have been explored to deepen engagement and enhance therapeutic impact. 48 A variety of art therapy approaches have been effectively used to support veterans’ mental health, each tailored to address specific challenges relating to military experience. Art therapy interventions can be categorized into individual, group (including family interventions), and telehealth (synchronous) modalities.
Telehealth
Telehealth as defined by the Health Resources and Services Administration (HRSA), is “the use of electronic information and telecommunication technologies to support long-distance clinical health care.” 49 In veteran populations, telehealth initiatives, such as the Rural Veterans Tele-Rehabilitation Initiative Creative Arts Therapies Project (RVTRI CAT), have expanded access to art therapy, particularly for veterans in rural or underserved areas. Notably, 24% of all veterans and 36% of those with a service-connected disability live in rural or highly rural regions, where distance, disability, and transportation costs often create significant barriers to in-person care. 50 Evidence supports the efficacy of virtual interventions including PE and CPT for PTSD treatment, though technological barriers and limited therapeutic alliance persist. 51
Rationale
While research highlights the benefits of art therapy for veterans, 41 few studies explore differences in outcomes between male and female veterans in telehealth settings, especially concerning MST and caregiving responsibilities disproportionately affecting female veterans.10,13 Differences in trauma experiences between men and women remain underexplored, limiting understanding of how these factors shape art therapy, delivery, and outcomes.
This qualitative study explores the experiences of six male and three female veterans with PTSD and/or TBI who engaged in short-term, individual, synchronous telehealth art therapy. Through reflexive thematic analysis,53,54 the study sought to examine how different identities may shape therapeutic engagement, emotional processing, and recovery outcomes. The research aimed to identify both shared and divergent experiences across male and female veterans to address gaps in the literature on how telehealth art therapy supports veterans with diverse identities and needs.
Methods
This paper is an analysis of qualitative data from a larger mixed methods study examining the impact of telehealth art therapy on physiological and psychosocial symptoms of PTSD and TBI. 52 Through an adapted version of reflexive thematic analysis53,54 of this data, this study sought to deepen our understanding of how male and female veterans intersect with the art therapy processes and outcomes in this context. By examining veterans’ perspectives, this research will contribute to a more nuanced understanding of the potential benefits and challenges of telehealth art therapy in addressing this population’s complex mental health needs. This study followed the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines. 55
Research Team Positionality
The research team includes GK and JW (co-leads for the overall research project, study design, data collection, and analysis
Participants
Nine veterans (three self-identified females and six self-identified males
Demographic Characteristics.
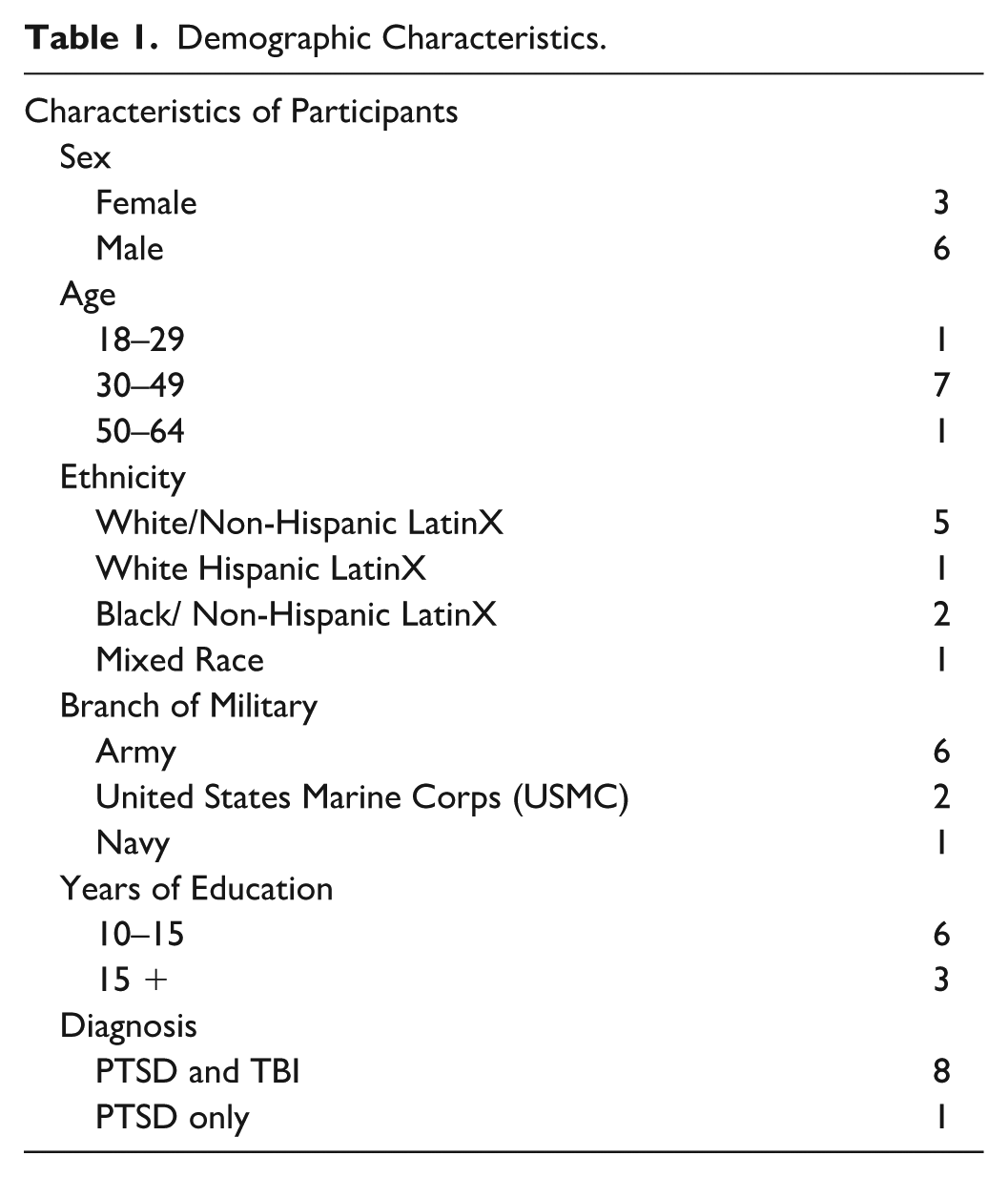
All participants were diagnosed with PTSD by a healthcare provider at a Veteran’s Affairs (VA) facility. All but one participant had a co-occurring diagnosis of TBI. Recruitment occurred at a VA medical center in the Southeastern United States. Inclusion criteria stipulated that participants must be between the ages of 18 and 55 years, have a current PTSD or TBI diagnosis, be eligible for magnetic resonance imaging (MRI), be physically capable of engaging with art materials, be proficient in English, and be able to use a telehealth platform. Additionally, participants had to provide informed consent willingly. Exclusion criteria included the presence of a neurological condition that could affect neuroimaging outcomes, autism spectrum disorder, psychotic psychiatric disorders, significant uncorrected sensory deficits, prior experience with art therapy, severe medical conditions with potential neurological implications (e.g., liver or kidney failure), intentions of becoming pregnant during the study, and concerns related to substance abuse.
Out of the initial cohort of twelve, three participants were excluded from the final analyses due to redeployment, having an inactive PTSD diagnosis, and/or technical connectivity challenges. The study protocol and procedures received approval from the Institutional Review Board (IRB) at the University of Florida and the North Florida/South Georgia Department of Veterans Affairs Medical Center. Informed written consent was obtained from all participants before their study enrollment.
Procedure
Participants engaged in eight individual telehealth sessions with the art therapist. The sessions were conducted using VA Video Connect. Before beginning the sessions, the participants were mailed a packet of art materials (with mixed media paper, dry and wet media, collage materials, a mask, and plasticine clay). All sessions were led by the same therapist and were semi-structured to ensure consistency. Session one, which did not include artmaking, was used to introduce art therapy, build rapport, gather biopsychosocial information, and identify program goals. The next six sessions incorporated artmaking. Session two focused on multi-dimensional wellness. All participants made a wellness model drawing using water soluble colored pencils and identified areas where they wished to change. Sessions three through seven focused on addressing the veterans’ trauma symptoms and self-identified goals. When possible, art interventions incorporated veterans’ artistic interests and focused on metaphors and descriptions that the veteran’s themselves brought to sessions. The therapist would direct the veterans towards specific media and themes based on how they responded to each week’s intervention and their therapy goals. Interventions commonly addressed themes related to establishing a sense of safety, exploring past experiences or trauma, integrating past experiences into one’s current identity, and future goals. The seventh session (and final artmaking session) focused on therapy closure and maintenance planning, as well as offering referrals for other services and exploring how ongoing arts engagement can support wellbeing. The eighth session was used for a post-therapy assessment.
Throughout the six telehealth art therapy sessions, clinical notes taken by the art therapist captured the veterans’ reflections on their journeys, perceptions of change, and overall experiences with art therapy. These qualitative data were analyzed to better understand the veterans’ experiences and the role of telehealth art therapy in facilitating emotional and psychological recovery.
KV led the review of the clinical notes and created session summaries for each participant, capturing the initial consultation, session details, and available artwork. The summaries were then reviewed and compiled by KS and KV into individual profiles for each veteran. These profiles contained demographic and psychosocial data, session descriptions, therapist and veteran feedback, artwork, and quantitative measures. An adapted reflexive thematic analysis approach was used to identify, analyze, and report patterns in the data.53,54 The team involved in data analysis (GK, KS, KV, VS) printed out the session summaries, focusing on veteran feedback, artwork, and therapeutic processes, and immersed themselves in reading the notes and viewing participant artwork to familiarize themselves with the data. 53 Notes and memos were created on the session summaries based on team members’ initial thoughts, questions, and impressions. These initial impressions were then compiled in a discussion as a research team and distilled into emerging themes. 53 These were cross checked with each participant’s profile and final themes were defined based on visual representations, self-expression, and references to self and relationships. Finally, they organized the manuscript into three themes with related subthemes as they related to similarities and differences by male and female identifying veterans.
Trustworthiness and Credibility
Several measures were taken to ensure the trustworthiness and credibility of our findings. 56 The qualitative analysis team (GK, KV, VS, KS) wrote memos during individual case study reviews, discussed discrepancies as a team until reaching consensus, and triangulated data from clinical notes, artwork, and participant reflections.
Results
Analysis of the data (including clinical notes and artwork) resulted in three main themes: 1) Striving to manage self and emotions; 2) Diverse relationships with artmaking and media; and 3) Seeking to improve interpersonal connection. Table 2 provides themes and sub-themes as well as artwork, demonstrative veteran quotes, and therapist observations from across the participant data.
Themes, Sub-themes, Artwork, Veteran Quotes, and Therapist Observations.

Striving to Manage Self and Emotions
This theme encompassed several key subthemes: the ability to recognize and manage emotions, engaging in self-regulation and coping through artmaking, sensory engagement and embodiment, self-care, and experiencing pleasure, positive emotions, and joy. These subthemes highlight how veterans used artmaking as a therapeutic tool to navigate their emotional landscapes, process trauma, and cultivate moments of self-compassion. The creative process often enabled participants to confront challenging emotions, regulate their responses, and engage their senses while fostering self-awareness and personal growth.
The ability to recognize and manage emotions: Veterans engaged in artmaking as a way to identify and respond to emotions such as depression, grief, anger, despair, and disillusionment, often using symbolic imagery to externalize complex feelings. For example, Veteran A created a clay box with its lid blown off, symbolizing the inevitable release of contained emotions, and he reflected on how “those boxes eventually won’t hold everything.” Similarly, Veteran E described how she worked on a sculpture of self-sacrifice, allowing her to recognize emotions, stating, “the more I shape my figure, the more I think about what I’m trying to express.”
Engaging in self-regulation and coping through artmaking: Veterans described using art to calm heightened emotional responses, distract from distress, and develop healthier coping mechanisms. For example, Veteran A depicted a bridge supported by family and social connections, which transformed a previously drawn cliff-edge narrative of emotional overwhelm. In addition, Veteran J described how painting “calms me when I’m overly reactive” and “gives space for quietness,” while Veteran C used art as a distraction and a way to explore new perspectives, emphasizing how it helped her “see the whole picture.”
Sensory engagement and embodiment: The sensory and tactile dimensions of artmaking were critical in self-soothing and grounding veterans while deepening their emotional connection. For instance, Veteran G noted that working with clay evoked memories and heightened his connection to his emotions. Veteran B, noted that the tactile act of artmaking helped her relax and connect with feelings of “warmth, sensuality, and comfort,” and Veteran E used her body to pose for her sculpture.
Self-care: Artmaking created space for veterans to focus on their needs and healing, rather than solely serving others. Moments of creative satisfaction provided veterans with opportunities to reflect, create, and experience emotional release. Veteran E described how creating art “for myself, rather than as a gift to others,” was a new and transformative experience, and Veteran L discussed his desire to give himself more focus.
Experiencing pleasure, positive emotions and joy: Many veterans reported moments of enjoyment, satisfaction, and emotional release during the creative process. Veteran B described feeling “vibrant and complete” while engaged in artmaking, indicating the restorative potential of pleasurable experiences. Veteran L, while working on a mask symbolizing both trauma and strength, shared the empowering realization: “I survived because the fire within me burned brighter than the fire around me.” These moments underscored the capacity of creative expression to foster resilience, pleasure, and renewed meaning.
Diverse Relationships with Artmaking and Media
This theme explores veterans’ different relationships with creative processes and materials in their art therapy process. This theme includes three sub-themes: (a) engagement with media, focusing on the attributes, techniques, and mastery of artistic materials; (b) art as emotional and cognitive processing, using art to externalize emotions, explore personal metaphors, navigate self-consciousness, and foster self-acceptance; and (c) art as a coping mechanism, utilizing art for relaxation, mindfulness, and distraction.
Engagement with media, focusing on the attributes, techniques, and mastery of artistic materials: Each veteran experienced an individualized trajectory of artmaking sessions and used a variety of art materials. Some focused on more mastery of specific materials (such as Veteran J focusing deeply on painting), while others explored a broader range of techniques with structured support by the art therapist. Veteran B explored multiple kinds of media, tissue paper collage, painting, oil pastels, and drawing, and seemed to create her own metaphors for self-expression and exploration. Self-consciousness related to art making occasionally surfaced in sessions. Veteran L became self-critical while attempting to recreate flames in his artwork and was at times distracted by a desire for technical perfection.
Art as emotional and cognitive processing: using art to externalize emotions, explore personal metaphors, navigate self-consciousness, and foster self-acceptance: Two veterans emphasized deep engagement with a specific media to process their emotions and thoughts. For example, Veteran J remained committed to painting, describing it as a method to “put everything into my paint” and externalize his pain. This consistent engagement fostered mindfulness, helping him to “pause when angry” and reflect on his life and relationships. Veteran E used the majority of her artmaking sessions to explore the theme of self-sacrifice through a wooden sculpture. She reflected that shaping the figure helped her “pay attention to feelings” and gave her “permission to come out of the dark.”
Symbolic imagery and the expression of inner life metaphors played a central role in helping veterans articulate internal experiences that were otherwise difficult to express. Veteran L’s mask symbolized disillusionment, secrecy, and trauma, incorporating an upside-down flag, flames, and a padlock. Veteran A’s clay box, depicted with its lid and sides blown off, visualized the pressure of repressed emotions and the inevitability of release, a metaphor he described as “good and scary at the same time.” In contrast, Patient C used art as a distraction. She described how learning something new, like creating and discussing the giraffe metaphor, provided an enjoyable and relaxing experience that helped her “see the whole picture.”
Art as a coping mechanism: utilizing art for relaxation, mindfulness, and distraction: Many Veterans discussed how artmaking provided them with a way to cope with their emotions and find relaxation. Veteran E remarked that the embodied experience of shaping her sculpture allowed her to “fully feel her emotions.” Veteran B discussed how creating vibrant images allowed her to represent feelings she struggled to internalize. Veteran G reflected on how working with clay slowed him down and helped him “be in the moment,” indicating mindfulness and sensory engagement. Veteran J remarked that he knew he could return to his painting when he needed to express his feelings. Some veterans, such as Veterans A and C found that art making could help distract from distressing feelings.
Seeking to Improve Interpersonal Connection
The desire to improve connections with others emerged as a critical focus of telehealth art therapy, reflecting veterans’ efforts to navigate their relationships. This theme was divided into three key sub-themes: a) seeking and working on personal boundaries, b) seeking and working on connection with family, and c) seeking and working on social engagement.
Seeking and working on personal boundaries: Veterans used art as a medium to establish and reflect on personal boundaries, often representing themes of self-preservation, inner retreat, and emotional containment. Through art therapy sessions, Veteran K learned to balance familial, spiritual, and personal commitments, using art to regulate emotions and gain clarity. Veteran E focused on self-focus, self-discovery, and self-compassion through her sculpture, which symbolized her shift from caregiving to prioritizing her own needs.
Seeking and working on connection with family: Veterans externalized their struggles to explore and repair familial relationships. Veteran A visualized a bridge symbolizing reconnection with family after isolation, while Veteran F used a doorway to represent his longing to rebuild bonds. These metaphors helped them process emotions and reframe relational dynamics. Veteran J noted that painting improved his emotional regulation, enhanced his listening skills, and fostered peace within family interactions. In familial relationships, veterans also emphasized emotional openness and shifts in perspective. Veteran B found that the art therapy sessions built resilience and helped her recognize her value within her family, fostering positive relational changes. Veteran C used artmaking as a means of distraction, which helped clarify her understanding of her family’s role.
Seeking and working on social engagement: Veterans externalized their struggles relating to social connections through vivid metaphors like bridges and doorways. Veteran F used drawings of war and emptiness to express both a desire for deeper relationships and fears of vulnerability. Veteran J found that painting allowed him to externalize pain, facilitating personal growth and improving interactions with others. Another facet of social engagement for veterans was deeply tied to self-expression and exploration of identity, especially for female veterans. For example, following her self-exploration in art therapy, Veteran B reported establishing positive relationships with others.
Across these themes, veterans highlighted the power of metaphor to support externalization, emotional exploration, and personal growth in connections with others facilitated by art therapy.
Discussion
This study examined how veterans with PTSD and TBI engaged with eight sessions of individual telehealth art therapy. Three key themes emerged from the analysis: 1) Striving to manage self and emotions; 2) Diverse relationships with artmaking and media; and 3) Seeking to improve interpersonal connection. These themes and subthemes (Table 2) align with identified treatment needs of this population. Peer and family support are vital for recovery, for example, individual telehealth art therapy supported progress toward improved family connection for veterans with this goal (theme #3). Altered brain activity, particularly in regions related to emotional regulation, leading to symptoms such as irritability and anger, are common for veterans with TBI and PTSD.3,4 Theme #1 indicates that art therapy addressed this area. These findings also align with prior research on veterans’ use of art therapy as a means of externalizing trauma and managing emotions.57,58
PTSD manifests in challenges with relationships, employment, and overall well-being, reducing sense of purpose and fulfillment. 10 Subthemes identified in this study, including cultivating moments of joy, technical engagement, and fostering social connections may directly relate to building a sense of purpose and fulfillment. In this study, some female veterans seemed to engage in an exploratory, embodied, and sensory-driven approach, shifting between media and using tactile experiences to foster relaxation and self-awareness. Subthemes of theme #1 seem to support the use of telehealth art therapy to address the identified treatment need of improvements in well-being.
Male veterans often depicted combat-related imagery, aligning with findings that men frequently portray graphic war scenes, destruction, and violent experiences in their artwork. 57 This study extends that observation, as they used symbolic representations such as explosions and depictions of combat to process emotional overwhelm and relational conflicts. In contrast, female veterans gravitated toward metaphorical self-representations and often did not directly depict traumatic imagery. 58 While all veterans were asked about their combat experiences as part of their therapy, they were not required to describe them in detail. Therefore, it was not possible to determine if these differences could be attributed to combat experience or other factors.
Another key contribution of this study is identifying how veterans engaged differently interpersonally. While both groups used art to navigate relationships, some male veterans externalized their struggles through symbolic metaphors such as bridges or doors representing reconnection, while some female veterans emphasized self-discovery in their relational themes. These patterns suggest that art therapy can support diverse interpersonal processing strategies, and that therapeutic approaches are enhanced by remaining responsive to individual and group variations rather than assuming uniform experiences.
Telehealth art therapy offers veterans a flexible and accessible way to engage in creative expression, particularly for those in rural or underserved areas or those with limited mobility. 59 Several veterans expressed appreciation for the ability to create from a location of their choosing, with Veteran E incorporating personal materials into her artwork, which may have enhanced her sense of ownership and connection to the process. External factors such as family presence or home environments may have influenced how openly some veterans shared their experiences, either by providing less privacy or by increasing the veterans’ comfort. While this was not explicitly noted as a barrier in clinical notes, it is a consideration for future telehealth interventions.50,60 Telehealth can enhance therapeutic rapport, as veterans engage in therapy within their personal, social, and family environments and can share this with the therapist. This flexibility fosters deeper connections between veterans and their work while ensuring continuity in care. 60 This study extends the existing literature on telehealth art therapy by demonstrating how veterans adapted to remote creative processes.50, 59 While prior research has shown that telehealth increases accessibility, this study uniquely highlights how the home environment influenced veterans’ engagement with art materials
This exploration is innovative as it offers insight into how clinical notes, session summaries, and participant-created artwork can be triangulated and thematically analyzed as qualitative data within a telehealth intervention. Additionally, it illustrates a novel method of capturing embodied, expressive, and symbolic dimensions of participant experience through asynchronous, image-informed documentation, providing insights into male and female differences in artistic themes and engagement styles.
Limitations: This exploratory study did not reach data saturation due to its limited sample size, however, saturation may not be applicable in reflexive thematic analysis, where themes are "generated” through analysis rather than inherently present in the data. 61 Future research should aim to gather data from more veterans, especially females, to learn more about their uses of telehealth art therapy.
While notes were detailed and included several verbatim comments, these were not direct participant narratives and may not fully reflect their voices. Access to art materials was a key consideration. Each veteran in the study received a standardized art kit. The art kits were limited compared to the supplies and resources often available in an art therapy studio setting. However, many veterans supplemented the kits with supplies they had access to at home, including craft materials, digital art tools, materials in their home workshops or supplies they purchased. Veterans sometimes connected from alternate locations when traveling, and as a result did not always have their art supplies readily available, limiting their ability to engage fully in telehealth art therapy sessions. 59 Additionally, documentation practices and the absence of member-checking present challenges, 62 as interpretations are recorded without participants’ confirmation or opportunity to refine meaning.
Remote art therapy may not allow for a clear view of the art process or image, requiring therapists to rely on the veterans’ verbal accounts. These interpretations may overlook critical aspects of emotional or symbolic expressions.48,50 Some veterans misplaced artwork throughout the intervention, disrupting continuity, reducing the ability to reflect and track progress, and resulting in some missing data. While confidentiality is an essential factor in all telehealth interventions, this study did not capture whether veterans’ ability to express themselves was impacted by their environment. Future research should explore whether home-based settings affect veterans’ willingness to engage openly, particularly in cases where family members or caregivers are present.
Some theoretical limits on the applicability of this study’s benefits arise from the fact that assessing veterans’ emotional states and risks remotely presents unique challenges. Without in-person embodied interactions, therapists rely on virtual cues and may have a limited view of environmental factors, making it more difficult to fully assess distress, suicidal ideation, or other risk factors that are important for this population. 51 Telehealth restricts in-person sessions’ immediacy and full visual context, complicating risk assessment and response during crises. These limitations highlight the need for secure, adaptable approaches to telehealth art therapy with veterans, including clear emergency procedures prioritizing reliable connectivity, controlled confidentiality, and strategies to better capture and interpret veterans’ input for effective and responsive care.60,63 Additionally, while connectivity issues were not a significant challenge in this study, prior research suggests they can disrupt therapeutic flow and engagement. 51
It remains unclear how prevalent the themes identified may also be in other intervention formats. Their presence in our analysis is meant to illustrate the potential effectiveness of this individualized telehealth art therapy intervention with a small sample by elucidating the experiences of participants based upon their reflections and artwork, supported by clinical observation.
Recommendations for Research and Practice
Telehealth art therapy shows promise in overcoming stigma and geographical barriers, but its effectiveness depends on technical support, cultural sensitivity, and adaptable practices. To support the breadth and plurality of our nation’s veteran population, it is essential to adopt culturally informed, trauma-sensitive approaches that address veterans’ unique needs. The findings of this exploratory study suggest that one’s identity may be associated with unique approaches to expression and communication in the context of art therapy interventions for PTSD and TBI. It is unclear how these differences relate to the effectiveness of art therapy for this population, including mechanisms of change related to variations in direct engagement with traumatic content versus more self-reflective content. Specific areas for further inquiry include exploring the impact of cultural identity on therapeutic engagement and examining how veterans’ varying trauma experiences influence their interaction with telehealth platforms. Clinical recommendations include integrating family-centered approaches where possible, considering the challenges faced by military families, such as frequent relocations and TBI/PTSD-related dynamics. Family follow-up could be a valuable strategy to strengthen relational support systems and enhance therapeutic outcomes. Additionally, ensuring access to appropriate art materials and fostering safe, non-judgemental therapeutic spaces are key to improving the efficacy of telehealth art therapy. These practices should be tailored to meet the individual needs of veterans, recognizing their unique circumstances and backgrounds.
Recommendations for research include researching how aspects of identity interact with TBI and PTSD experiences, along with help-seeking behaviors, can guide telehealth providers in designing interventions that resonate with veterans’ lived experiences. Future research should explore the specific impacts of telehealth on therapeutic outcomes for men, women, and other veterans, to develop more tailored and effective interventions. Additionally, research should seek to determine if hybrid models that combine in-person and telehealth care increase access. Amplifying veterans’ voices through qualitative studies can further refine telehealth modalities, ensuring that they meet individual symptoms and psychosocial needs.
Conclusions
This study is among the first to examine distinct patterns in veterans’ engagement with telehealth art therapy, revealing how symbolic imagery, sensory processes, and identity work intersect with trauma recovery in remote contexts. The findings build on existing telehealth research by showing that art therapy can be meaningfully adapted for virtual delivery while preserving its relational, expressive, and trauma-informed benefits. Clinically, these results point to the importance of tailoring interventions to align with each participant’s modes of expression, personal history, and relational priorities, thereby enhancing engagement and therapeutic relevance. Future research should explore hybrid service models, strategies to strengthen therapeutic alliance in virtual settings, and the ways unique identities, such as cultural background, lived experience, and caregiving roles shape outcomes in telehealth art therapy for PTSD and TBI.
Footnotes
Acknowledgements
We would like to thank Dr. Bani Malhotra for her support with data curation and Delaine Due for their support with reviewing and editing the manuscript.
Ethical Considerations
The study protocol and procedures received approval from the Institutional Review Board (IRB) at the University of Florida and the North Florida/South Georgia Department of Veterans Affairs Medical Center (IRB202101906, 3/23/2022,7/11/2025).
Consent to Participate
Informed written consent was obtained from all participants before their study enrollment.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Drexel University provided funding to their graduate students through Research Fellowships. The authors declare that financial support was received for the research, authorship, and/or publication of this article. This study was funded in part by Creative Forces®: NEA Military Healing Arts Network, an initiative of the National Endowment for the Arts in partnership with the US Departments of Defense and Veterans Affairs that seeks to improve the health, wellbeing, and quality of life for military and veteran populations exposed to trauma, as well as their families and caregivers. Creative Forces is managed in partnership with Civic Arts, the Henry M. Jackson Foundation for the Advancement of Military Medicine, and Mid-America Arts Alliance. Funding for Drexel graduate students was provided by Drexel University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Due to the nature of the research, supporting data is not available.
Author Disclaimer
The opinions contained herein represent the private views of the authors and are not to be construed as official or as reflecting the views, opinions, or policies of the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc., the Department of Defense, the National Endowment for the Arts, or the U.S. Government. Mention of trade names, commercial products, or organizations does not imply endorsement by the U.S. Government. This material was created free of branding or market affiliations. The authors are operating solely as contributors. The work of John Williamson was authored as part of their official duties as an employee of the United States Government and is therefore a work of the United States Government. In accordance with 17 USC. 105, no copyright protection is available for such works under US Law. Neither the Defense Health Agency, any other component of the Department of Defense, nor the U.S. government has approved, endorsed, or authorized this product [or promotion, or service, or activity]