
Abstract
Non-suicidal self-injury (NSSI) and suicidal ideation (SI) represent significant mental health challenges among university students. In low- and middle-income contexts like Bangladesh, there is limited understanding of how these behaviors differentially affect students with and without mental illness. This study addresses these gaps by investigating the prevalence and risk factors of NSSI and SI, with stratified analyses by mental illness status, to predict these behaviors. This cross-sectional study recruited 1401 university students between December 2024 and January 2025. Data was collected via a self-administered questionnaire assessing socio-demographics, and psychological factors. Traditional statistical analyses, including chi-square tests and logistic regression, were conducted in SPSS 27. The prevalence of NSSI and SI was 21.4% and 17.2%, respectively. Both NSSI and SI were more common among students with symptoms of depression or anxiety (mental illness) than those without. Multivariable analyses identified smoking, cyberbullying, and probable eating disorder as significant predictors of both NSSI and SI, with these associations persisting after stratification by mental illness status. Subgroup analyses showed that among students without mental illness, female gender, older age, smoking, cyberbullying, and eating disorder symptoms significantly predicted NSSI, while smoking, cyberbullying, eating disorder, and older age predicted SI. In students with mental illness, smoking and cyberbullying remained robust predictors of both NSSI and SI, while eating disorder was significantly associated with NSSI but not SI. The regression models explained 12.9% of the variance in NSSI and 16.6% in SI. The findings highlight the necessity to adopt interventions that address modifiable risk factors, with a strong emphasis on behavioral and mental health variables, to effectively reduce self-harming and suicidal behaviors in young adults.
● This study provides the first comprehensive assessment of non-suicidal self-injury (NSSI) and suicidal ideation (SI) among Bangladeshi university students, drawing on data from 1,401 participants.
● The prevalence of NSSI and SI was 21.4% and 17.2%, respectively, with higher rates observed among students exhibiting symptoms of depression or anxiety.
● Smoking, cyberbullying, and probable eating disorder were identified as significant predictors of both NSSI and SI across all analytic models.
● Stratified analyses revealed differential risk patterns by mental illness status, highlighting distinct behavioral and psychosocial pathways.
● The findings emphasize the need for university-based mental health interventions, including screening, smoking cessation, and anti-cyberbullying initiatives, to reduce self-harming and suicidal behaviors.
Introduction
Suicide is a major global public health concern, claiming approximately 727 000 lives each year and impacting on individuals, families, and communities worldwide. 1 Non-suicidal self-injury (NSSI), defined as the deliberate act of harming oneself without suicidal intent, is often used as a maladaptive coping mechanism for intense emotional distress. Common forms include self-poisoning, cutting, burning, head-banging, or self-hitting. 2 Though not intended to be fatal, NSSI can result in serious or life-threatening outcomes, especially when individuals misjudge the lethality of their actions due to impaired judgment during psychological crises. 3 Suicidal ideation (SI), characterized by persistent thoughts of ending one’s life, is often linked to major depressive episodes and is a strong predictor of future suicide attempts, even though most individuals with SI do not act on it. 4 Despite differences in intent, NSSI and SI frequently co-occur and share underlying psychological risk factors such as emotional dysregulation, depression, and trauma. Individuals engaging in NSSI face a significantly elevated risk of developing SI and attempting suicide 5 ; a meta-analysis of over 139 000 individuals found that 9.6% had experienced both. 6 SI exists along a continuum, ranging from passive thoughts to active planning and completed suicide. 7
The relationship between non-suicidal self-injury and suicidal ideation is complex and multifaceted. Individuals who self-harm often experience heightened emotional and interpersonal distress that contributes to suicidal vulnerability. 8 For example, a German study reported that 39.6% of those with a history of NSSI had attempted suicide, while 66.3% of individuals with suicidal behavior also engaged in NSSI. 9 In the U.S., 70% of adolescents with a history of NSSI had attempted suicide at least once, and more than half had made multiple attempts. 10 Longitudinal evidence from college students shows that NSSI significantly predicts both current and future suicidality, with an odds ratio of 2.8 after adjusting for confounders. 11 While NSSI may temporarily relieve emotional pain, repeated use can lead to habituation and an escalation in self-harming behavior, increasing the risk of transition to suicidal actions. 12 This progression can be conceptualized through Joiner et al’s 13 Interpersonal Theory of Suicide, which posits that serious suicidal behavior emerges when individuals experience perceived burdensomeness and thwarted belonging alongside an acquired capability for suicide. Recurrent engagement in NSSI may diminish the natural fear of pain and death, thereby increasing this acquired capability, while the accompanying emotional suffering and social disconnection may amplify feelings of isolation and burden, ultimately intensifying suicide risk.
University students face unique stressors related to academic demands, identity development, and shifting social roles, placing them at heightened risk for both NSSI and SI.14,15 The World Mental Health International College Student survey found that 17.7% of students across 24 universities in 9 countries reported lifetime NSSI, 16 while the lifetime prevalence of SI, suicide plans, and attempts were 27.4%, 12.7%, and 3.4%, respectively. Among those with ideation, 46.4% developed a plan and 23.2% attempted suicide. 17 In 17 countries, lifetime rates were 9.2% for SI, 3.1% for planning, and 2.7% for attempts, with 60% of transitions to planning or attempts occurring within the first year of ideation onset. 18 Additional studies reported 17.8% NSSI prevalence among Brazilian undergraduates, 19 16.2% lifetime self-harm among young adults in Scotland, 20 and rates of 19.6% for NSSI and 22.6% for SI in Norwegian university students. 21 In the U.S., 7% of students reported NSSI in the past 4 weeks. 22 Comparable SI prevalence has been documented in Ghana and South Africa at 24.5%.23,24 Empirical research revealed that eating disorder frequently co-occur with self-injurious behaviors. For example, about 27% of patients with a diagnosed eating disorder report a history of NSSI. 25 Another study conducted UK reported that 50.8% of female university students who self-harmed reported a possible eating disorder, and 20.1% with a possible eating disorder reported self-harm. 26 These findings suggest a strong comorbidity between disordered eating behaviors and NSSI in young adults.
In South Asia, self-injury and suicidality are also prevalent among youth. One Pakistani study reported a 28.4% NSSI rate among medical students, 27 while an Indian study found a 31.2% annual NSSI prevalence among college students. 12 In Bangladesh, 13.8% of university students reported past-year SI, 28 and among homosexual males, 47.1% experienced SI, 40.2% reported self-harm, and 32.4% had attempted suicide. 29 Despite growing global attention, studies on NSSI and SI among Bangladeshi university students remains sparse. Notably, no studies have concurrently explored their prevalence or psychosocial predictors, despite evidence showing that NSSI strongly predicts future suicide attempts.12,18 University students represent a high-risk group due to academic and developmental challenges, with global estimates suggesting 20% to 30% experience a mental disorder annually. 15 Depression and anxiety are highly prevalent in Bangladeshi student populations, with 15% reporting moderately severe depression and 18.1% experiencing severe anxiety. 30 However, no Bangladeshi studies have examined NSSI and SI jointly, nor differentiated risks based on students’ mental illness status, which is a critical gap, given the interconnection between these phenomena31,32 and their associations with mental health disorders. 23
The need for robust research into non-suicidal self-injury (NSSI) and suicidal ideation (SI) among university students is particularly urgent in Bangladesh, where suicide claims an estimated 11 000 lives annually, approximately 30 deaths daily. 33 Challenges such as stigma, underreporting, and limited mental health infrastructure further complicate prevention efforts, underscored by a media analysis reporting only 0.3 suicide-related articles per newspaper per day. 34 To address these critical gaps, the current study is the first in Bangladesh to predict both NSSI and SI among university students using diverse psychological, behavioral, and sociodemographic variables. Unlike previous Bangladeshi studies, which predominantly focuses on depression and anxiety, this study’s stratified analysis based on the presence or absence of mental illness, specifically depression and anxiety, which provides more significant understanding of the predictors of non-suicidal self-injury and suicidal ideation among university students in Bangladesh. By providing nuanced risk profiling and actionable insights, our findings can inform targeted, evidence-based interventions and national suicide prevention strategies tailored specifically to the academic setting and youth populations in Bangladesh and similar low-resource environments.
Methods
Study Design, Site, and Participants
This cross-sectional study was conducted among students at Jahangirnagar University, located in Dhaka, Bangladesh. Data collection was conducted using a self-administered and semi-structured questionnaire between 18 December 2024 and 10 January 2025. The target population included students who were residing in university residential halls (dormitories) during the study period. Eligibility criteria for participation included: (i) current residence in a dormitory, (ii) age 18 years or older, and (iii) willingness to participate with informed consent. A convenience sampling technique was used due to logistical constraints; while a formal sample size calculation was not performed, we achieved a high response rate (96.82%) and a final sample of 1401 participants after exclusions (eg, incomplete responses). Prior to participation, students were informed about the purpose of the study and provided written informed consent. The questionnaire took approximately 30 min to complete. However, the responses with older than 29 years old, and those who did not answer most of the questions in the outcome variables were removed from the final dataset. Participants older than 29 years were excluded to ensure sample homogeneity, as university students with 29 years in Bangladesh are typically not common. Older respondents are rare and may represent atypical educational trajectories, which could bias prevalence estimates. This study followed the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for cross-sectional studies (Supplemental Material). 35
Measures
Sociodemographic Factors
The questionnaire collected information on sociodemographic variables, including age, gender, education level, family type, father’s and mother’s education, and monthly family income (which was categorized into 4 groups: <25 000 BDT, 25 000-<50 000 BDT, 50 000-75 000 BDT, and >75 000 BDT). Participants also reported their height (feet/inches) and weight (kg), which were used to calculate Body Mass Index (BMI) following WHO guidelines. In the family type section, a “nuclear family” was defined as a household consisting of parents and their unmarried children living together, whether a “joint family” was defined as a household where extended family members such as grandparents, uncles, aunts, or cousins live together under the same roof. In addition, the questionnaire included items on lifestyle behaviors, specifically: (i) smoking status in the past month (Yes/No) and (ii) engagement in moderate or vigorous physical activity during the past 7 days. Physical activity was defined in accordance with WHO recommendations, either 150 to 300 min of moderate-intensity, 75 to 150 min of vigorous-intensity aerobic activity, or an equivalent combination per week (Yes/No). 36
Bullying-Related Information
This study collected data on participants’ experiences with both traditional bullying and cyberbullying. Traditional bullying was assessed by asking participants: “Have you ever been a victim of traditional bullying (eg, being mocked for your name, insulted for your skin color, criticized for your clothing, weight, height, socio-economic status, etc.)?.”37,38 Similarly, cyberbullying was assessed with the question: “Have you ever been a victim of cyberbullying (eg, receiving rude comments on social media, being called inappropriate names, or being harassed with sexually suggestive comments or gestures)?.”39,40 Both items used a binary response format (Yes/No), and participants were asked to report experiences that occurred within the past 12 months.
Mental Health Problems
To assess depression and anxiety, this study utilized the Patient Health Questionnaire (PHQ-2) 41 and the Generalized Anxiety Disorder (GAD-2), 42 respectively. Both scales follow a 4-point Likert scale, where responses range from 0 = “not at all” to 3 = “nearly every day”. The total score for each scale ranges between 0 and 6, with a score of ≥3 considered a positive screening for depression or anxiety, respectively. These tools are widely used for their brevity and effectiveness in identifying mental health concerns in community-based and clinical settings. 43
To assess eating disorders, the study employed the Eating Disorder Screen for Primary care (ESP-5). 44 The scale consists of 5 binary-response items (Yes/No), with each “Yes” response scored as 1 and each “No” scored as 0. The total score ranges from 0 to 5, and a score of ≥2 was used as the cutoff for identifying individuals at risk of probable eating disorder. The scale is designed as a rapid screening tool and is effective for identifying disordered eating behaviors in non-clinical populations. 44
Non-suicidal Self-Injury and Suicidal Ideation
This study utilized a single item to assess the rate of their past-year non-suicidal self-injury and suicidal ideation of the participants, as following the previous literature.45 -49 Participants were asked if they had hurt themselves but didn’t want to die, with activities such as taking sleeping pills for some reason, cutting hand, banging head on the wall, punching the wall, etc., to access self-harm behaviors.45 –47 On the other hand, whether they had you ever wanted to die or planned how to commit suicide or tried to die (eg, by taking poison, hanging, jumping from a high place, etc.) was used to assess suicidal behavior.48,49
Ethics Statement
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. Ethical approval for this study was obtained from the CHINTA Research Bangladesh Institutional Review Board on 17 October 2024 [Ref: CHINTA/IRB/10-2024/17(3)]. Prior to commencing the survey, informed written consent was obtained from all participants. Prior to data collection, participants were informed about the study’s objectives, procedures, potential risks, and their rights, including the option to withdraw at any time without consequences. Written informed consent was obtained to confirm their understanding and agreement to participate. To ensure confidentiality, data were securely stored, accessible only to the research team, and used exclusively for research purposes. No monetary or non-monetary incentives were provided.
Statistical Analysis
Data analysis was conducted using the IBM SPSS software version 27. Descriptive statistics (ie, frequency, percentages, mean and standard deviation) and inferential statistics (chi-square test and binary logistic regression) were carried out to analyze the data. The association between the study variables and the outcomes (non-suicidal self-injury and suicidal ideation) was estimated using chi-square test. Binary logistic regression analysis was conducted to examine the associated factors with the outcome variables.
Variance Inflation Factors (VIFs) were assessed for all models and confirmed no evidence of problematic multicollinearity (all VIFs < 5). Subgroup analyses were conducted stratified by mental illness status, defined as scoring ≥3 on either the PHQ-2 or GAD-2 (for depression and anxiety, respectively); participants meeting this cutoff were classified as “with mental illness,” and those below the threshold on both instruments as “without mental illness.” For transparency, we note that the SI model in the “without mental illness” subgroup had a limited number of events per predictor (~2), which may affect model stability and estimate precision.
The results of the logistic regression were reported as adjusted odds ratios (AORs), with corresponding 95% confidence intervals (CIs). For the non-suicidal self-injury model, omnibus test indicated that the model was statistically significant, with the Hosmer-Lemeshow test confirmed adequate model fit, and the Nagelkerke R2 indicated a larger proportion of the variance being explained by the model. Similarly, for the suicidal ideation model, omnibus test indicated that the model was statistically significant, with the Hosmer-Lemeshow test indicating good fit and Nagelkerke R2 indicated a larger proportion of the variance being explained by the model. A P-value <.05 was set as statistical significance with a 95% confidence interval.
Results
Characteristics of the Study Participants
Table 1 presents the demographic, socioeconomic, and health-related characteristics of the study participants (N = 1401). The mean age of participants was 22.96 ± 2.01 years, with the majority (62.5%) aged between 22 and 25 years. Males accounted for 51.7% of the sample, and 24.5% were in their fourth year of study. In terms of family background, 78.2% of participants reported living in nuclear families, and 42.2% had a monthly family income between 25 000 and 50 000 BDT. Regarding parental education, 34.3% of fathers had attained a bachelor’s degree, while 25.5% of mothers had completed high school.
Demographic characteristics of the study participants (N = 1401).
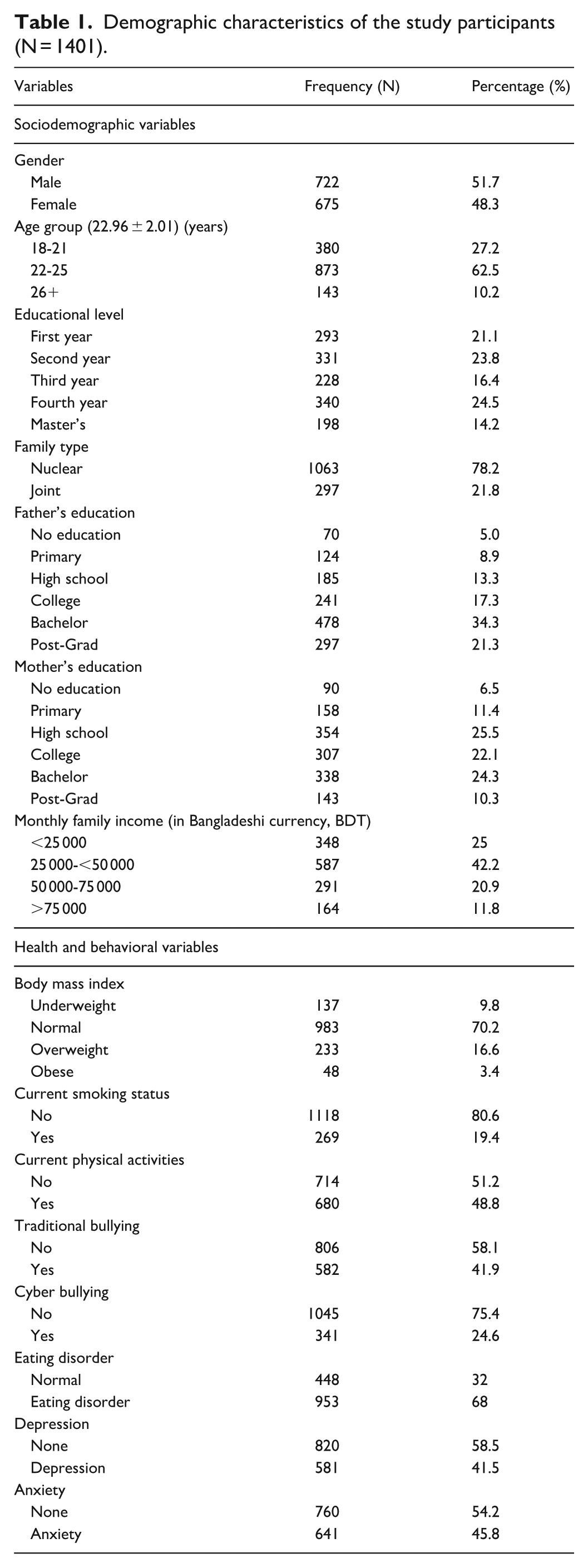
For health-related characteristics, 16.6% of students were classified as overweight and 3.4% as obese. Current tobacco use was reported by 19.4% of participants, and 51.2% indicated not engaging in regular physical activity. With respect to psychosocial and mental health factors, 41.9% of them had experienced traditional bullying, and 24.6% reported cyberbullying in the past year. Additionally, 68.0% met the screening criteria for eating disorders, while symptoms of depression and anxiety were present in 41.5% and 45.8% of participants, respectively (Table 1).
Prevalence of Non-suicidal Self Injury and Suicidal Ideation
In the total sample, 21.4% of the participants reported past-year non-suicidal self-injury; with higher prevalence among those with a mental illness (23.5%) compared to those without (18.1%; χ2 = 5.567, P = .018). Similarly, 17.2% reported suicidal ideation; with rates of 19.6% among students with mental illness and 13.3% among those without (χ2 = 9.233, P = .002). While NSSI was found significantly associated with SI (χ2 = 259.758, P < .001), among respondents who did not engage in NSSI, only 8.7% reported suicidal ideation, while 91.3% did not. In contrast, among those who did engage in NSSI, 48.3% reported suicidal ideation, while 51.7% did not (Figure 1).
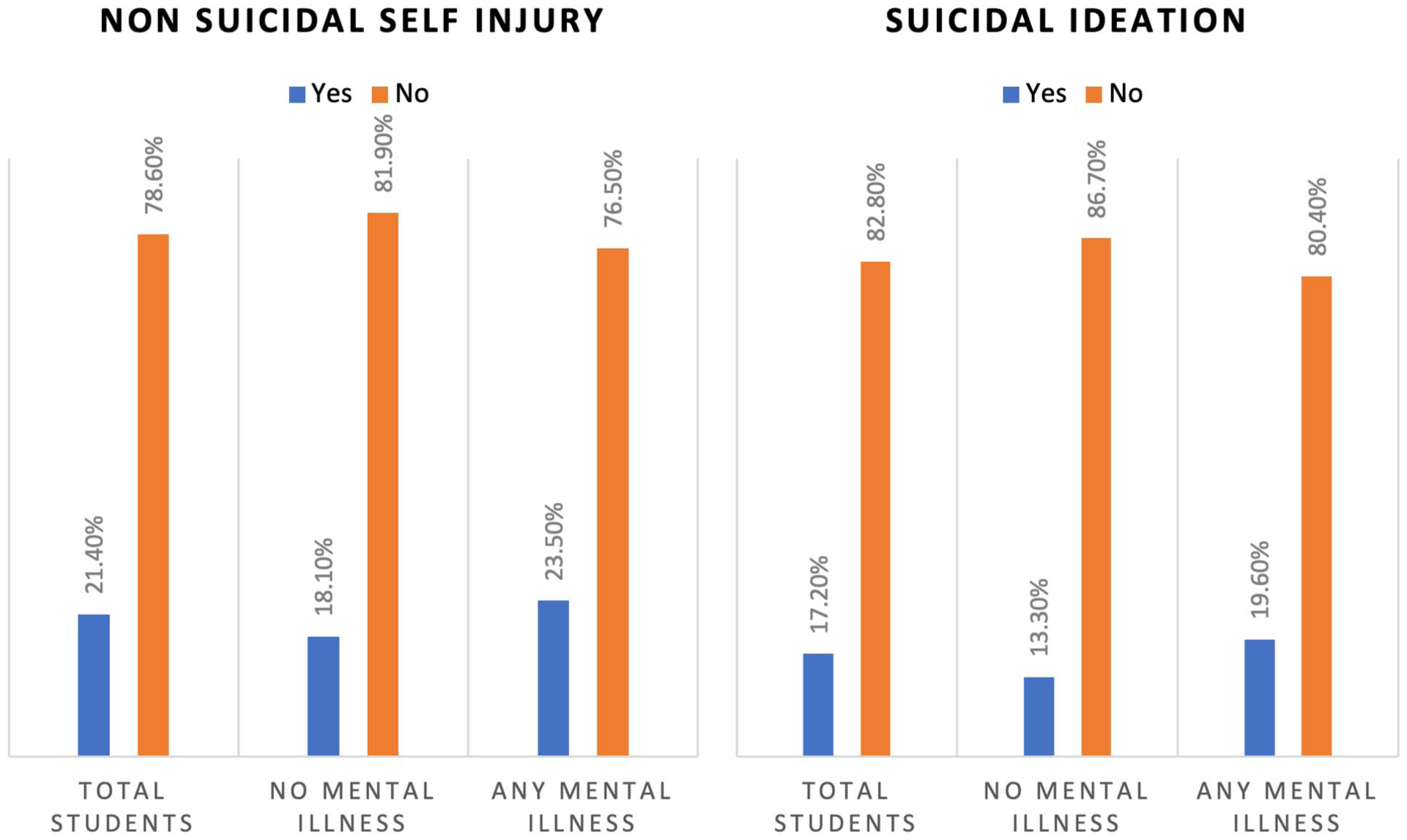
The prevalence of non-suicidal self-injury and suicidal ideation in the total sample, subgroup with mental illness and subgroup without mental illness.
Associations Between Study Variables and Non-Suicidal Self-Injury
In the total sample, several variables showed significant associations with self-harm (Table 2). Educational level was significant (χ2 = 14.187, P = .007), with the highest NSSI prevalence observed among second- (26.3%) and third year (25.0%) students. Current smokers reported NSSI at nearly twice the rate of non-smokers (34.9% vs 17.7%; χ2 = 38.748, P < .001). Experiences of cyberbullying were strongly linked to NSSI (31.7% vs 17.8%; P < .001), as was traditional bullying (24.7% vs 18.7%; P = .007). Additionally, 25.1% of participants with eating disorder symptoms reported NSSI, compared to 13.6% without such symptoms (χ2 = 23.794, P < .001). These patterns remained consistent when stratified by mental illness status. Among students both with and without symptoms of depression or anxiety, educational level, current smoking, cyberbullying, and eating disorders were significantly associated with NSSI, showing consistent strength and patterns of association. Traditional bullying remained significant only among students with mental illness.
Associations of the variables with non-suicidal self-injury in total sample, and with and without mental illness.

Bold P-values indicate statistically significant results.
Associations Between Study Variables and Suicidal Ideation
In the total sample, several variables showed significant associations with suicidal ideation (Table 3). Educational level was significantly associated (χ2 = 11.99, P = .017), with SI most common among second-year students (21.5%) and least common among Master’s-level students (11.1%). Current smokers reported SI at a markedly higher rate than non-smokers (33.8% vs 12.9%; χ2 = 67.62, P < .001). Cyberbullying also showed a strong association with SI (31.1% vs 12.4%; χ2 = 63.26, P < .001), as did traditional bullying (21.3% vs 14.1%; χ2 = 12.20, P < .001). Additionally, 20.0% of participants with eating disorder symptoms reported SI, compared to 11.2% without (χ2 = 16.88, P < .001). These patterns remained largely consistent across subgroups, with students both with and without symptoms of depression or anxiety showing similar associations. Notably, in students without mental illness, educational level and traditional bullying were not significant, whereas physical inactivity emerged as an additional factor in the mental illness subgroup (P = .048).
Associations of the Variables with Suicidal Ideation in Total Sample, and Without Illness and with Mental Illness.

Bold P-values indicate statistically significant results.
Binary Logistic Regression Analysis of Non-suicidal Self-Injury
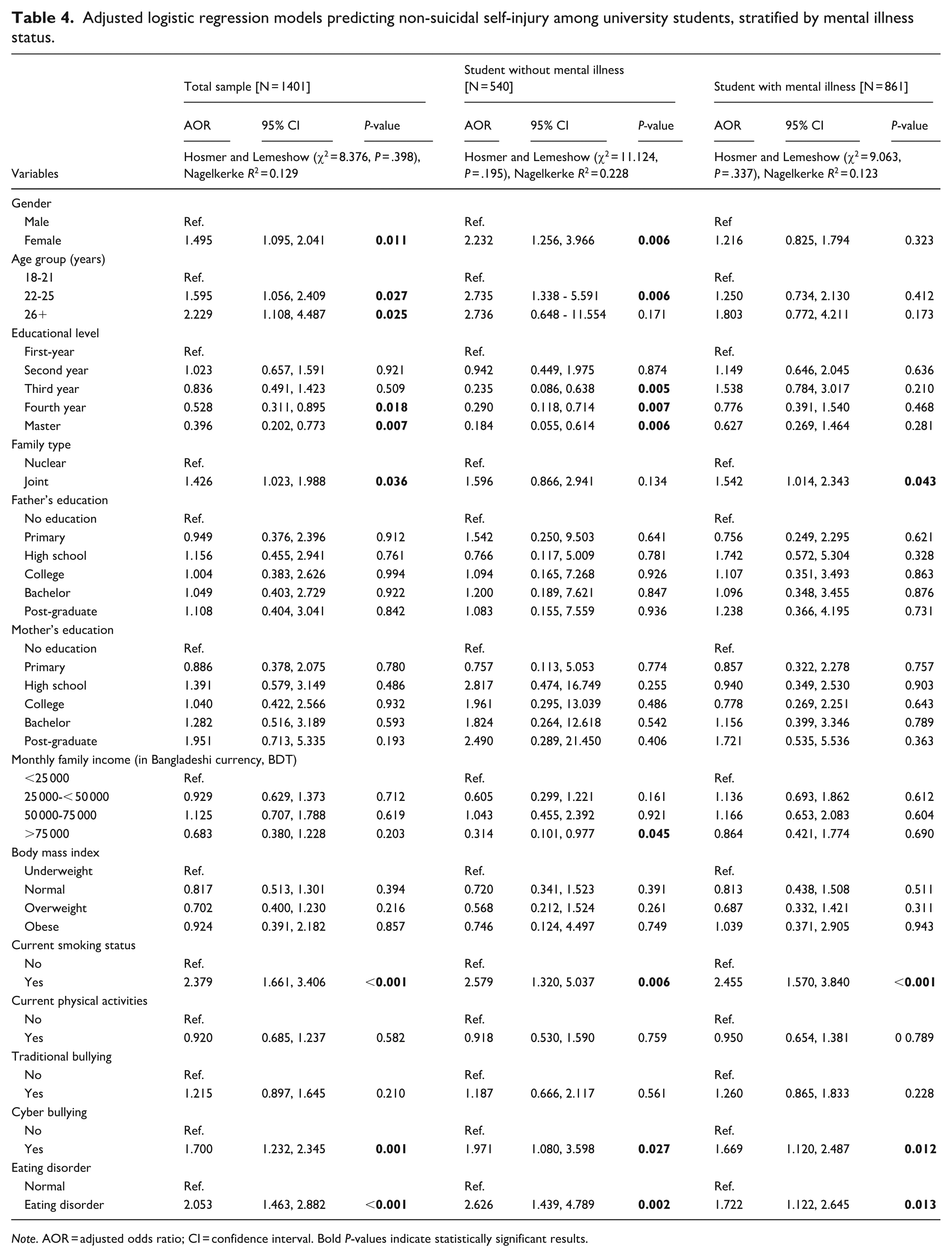
Adjusted logistic regression models identified several significant predictors of non-suicidal self-injury (Table 4). The omnibus test indicated that the model was statistically significant (χ2 (31) = 112.511, P < .001). The Hosmer and Lemeshow test confirmed adequate model fit (χ2 (8) = 8.376, P = .398), and the Nagelkerke R2 indicated that the model explained 12.9% of the variance in self-harm.
Adjusted logistic regression models predicting non-suicidal self-injury among university students, stratified by mental illness status.
Note. AOR = adjusted odds ratio; CI = confidence interval. Bold P-values indicate statistically significant results.
Adjusted logistic regression models identified several significant predictors of non-suicidal self-injury (Table 4). In the total sample, females had higher odds of NSSI compared to males (AOR = 1.495, 95% CI: 1.095-2.041, P = .011), and older students (22-25 and 26+ years) also showed increased odds compared to those aged 18 to 21. Higher education levels (fourth year and master’s) were associated with significantly lower odds of NSSI compared to first-year students. Smoking (AOR = 2.379, 95% CI: 1.661-3.406, P < .001), cyberbullying (AOR = 1.700, 95% CI: 1.232-2.345, P = .001), and eating disorder symptoms (AOR = 2.053, 95% CI: 1.463-2.882, P < .001) remained significant predictors of NSSI.
Subgroup analyses revealed that among participants without mental illness, being female (AOR = 2.23, P = .006), aged 22 to 25 (AOR = 2.74, P = .006), and having an eating disorder (AOR = 2.63, P = .002) significantly predicted NSSI. Additionally, third- and fourth-year students had reduced odds of NSSI, and cyberbullying and smoking were also significant predictors. Among participants with mental illness, current smoking (AOR = 2.455, P < .001), cyberbullying (AOR = 1.669, P = .012), and eating disorder symptoms (AOR = 1.722, P = .013) remained significant predictors, while educational level and gender did not show significant associations (Table 4).
Binary Logistic Regression Analysis of Suicidal Ideation
The adjusted logistic regression model identified several significant predictors of suicidal ideation (Table 5). The overall model was statistically significant (χ2 = 135, P < .001), with the Hosmer–Lemeshow test indicating good fit (χ2 = 3.408, P = .906) and a Nagelkerke R2 of 0.166, suggesting that the predictors accounted for 16.6% of the variance in suicidal ideation.
Adjusted Logistic Regression Models Predicting Suicidal Ideation Among University Students, Stratified by Mental Illness Status.

Note. AOR = adjusted odds ratio; CI = confidence interval. Bold P-values indicate statistically significant results
In the total sample, current smoking was the strongest behavioral predictor of SI (AOR = 2.96, 95% CI: 2.03-4.33, P < .001), followed by cyberbullying (AOR = 2.38, 95% CI: 1.69-3.36, P < .001) and eating disorder symptoms (AOR = 1.74, 95% CI: 1.20-2.59, P = .003). While educational level showed a declining trend, only postgraduate education reached borderline significance (AOR = 0.48, P = .052). Maternal education at the bachelor’s (AOR = 2.78, P = .094) and postgraduate levels (AOR = 4.19, P = .015) also emerged as significant predictors of SI.
Among participants without mental illness, current smoking (AOR = 4.03, P < .001), eating disorders (AOR = 3.30, P < .001), and cyberbullying (AOR = 1.99, P = .037) remained significant, while older age (25+ years) also emerged as a strong predictor (AOR = 6.35, P = .014). Higher maternal education levels (college to postgraduate) also showed significant associations with increased SI risk. In contrast, among participants with mental illness, cyberbullying (AOR = 2.64, P < .001) and current smoking (AOR = 2.92, P < .001) remained significant, whereas eating disorder symptoms were not independently associated (Table 5).
Discussion
This study is the first in Bangladesh to concurrently examine the prevalence, associated factors, and predictive patterns of non-suicidal self-injury and suicidal ideation among university students. We found that 21.4% of students reported engaging in NSSI and 17.2% reported experiencing SI, figures that align with global estimates and highlight the significant mental health burden in academic settings. Significant behavioral and psychosocial predictors, including smoking, traditional and cyber-bullying, physical inactivity, depressive and anxiety symptoms, and disordered eating behaviors, were consistently associated with both NSSI and SI. While certain sociodemographic variables (eg, gender, education level) showed significance in univariate models, their effects varied in multivariable analyses and across mental illness subgroups. These findings emphasize the complex interplay between individual vulnerabilities and environmental stressors and highlight the insights for informing targeted, context-specific mental health interventions.
In this study, 21.4% of university students reported engaging in non-suicidal self-injury within the past year, representing the first documented prevalence estimate among Bangladeshi undergraduates. Stratified findings showed a higher prevalence among students with self-reported mental illness (23.5%) compared to those without (18.1%), highlighting the increased vulnerability of this subgroup. Our overall rate is broadly consistent with regional trends; for example, NSSI prevalence among Indian college students was reported at 31.2%, 12 and among Pakistani medical students at 28.4%, 27 both likely influenced by intense academic demands and pervasive mental health stigma. Conversely, our observed rate exceeds that of a Chinese adolescent sample (13.4%) over 1 year, 50 which may reflect age differences and more robust mental health infrastructure in China. Furthermore, our findings surpass the 17.7% lifetime prevalence reported in a large multinational college student survey, 16 reinforcing the need for context-specific mental health strategies in Bangladesh. In response, universities should prioritize evidence-based interventions such as Dialectical Behavior Therapy, proven effective in reducing self- harm, 51 and implement systemic improvements to mental health services and student support structures on campus.
Our study identified a 17.2% prevalence of past-year suicidal ideation among Bangladeshi university students, with a notably higher rate among those with self-reported mental illness (19.6%) compared to those without (13.3%). This figure reflects an upward trend compared to earlier national estimates of 13.4% and 13.8% in similar populations,28,52 suggesting a growing mental health burden potentially driven by increasing academic stress, social isolation, bullying, and limited access to psychological support. The observed prevalence also exceeds several international benchmarks for 12-month SI rates; for example, a study in South Africa reported a rate of 9.6%. 23 While lifetime SI prevalence is naturally higher in some contexts, such as 24.5% among Ghanaian students, 24 and 12.1% among U.S. adolescents, 53 the comparatively elevated 12-month prevalence in our study indicates an urgent, immediate risk within the Bangladeshi university context. This may reflect deficiencies in mental health infrastructure and awareness. In light of these findings, integrating evidence-based interventions such as Dialectical Behavior Therapy (DBT) into campus counseling services could significantly reduce suicidality, depression, and NSSI among students. 54 Equally important are institution-wide awareness campaigns to design help-seeking and create a supportive, responsive campus environment.
Educational attainment emerged as a significant predictor of both self-harming and suicidal ideation, with adjusted regression models indicating that students in advanced academic years faced lower odds of self-harming and suicidal thoughts compared to first-year students. This pattern held true even after stratifying by mental illness status, implying that academic transition points, particularly between early and middle undergraduate years, are critical stress periods. While past research has linked such transitions to heightened vulnerability due to the cumulative burden of identity negotiation, academic performance pressure, and weakened support networks,16,55 recent Bangladeshi research highlights that students in later years may suffer more due to cumulative academic demands, mounting performance pressure, and increasing uncertainty about post-graduation career paths.56,57 Another large-scale cross-cultural study conducted in Bangladesh found that final-year university students reported significantly higher depressive symptoms and suicidal ideation, largely attributed to career insecurity, lack of job prospects, and the pressure of meeting family expectations. 58 These findings collectively highlight that psychological vulnerability is not confined to the early years of higher education. Rather, the chronic and escalating pressures faced by students in later academic stages, particularly in resource-limited or highly competitive contexts, necessitate tailored interventions. To mitigate these risks, universities should develop year-specific mental health strategies that include career counseling, stress management training, and support for managing academic workload and future planning.
Global studies consistently identify smoking as a significant predictor of both self-injury and suicidality; a trend echoed in our findings. Smoking significantly predicted both NSSI and SI, with smokers showing over twice the odds of these behaviors across all groups. Specifically, odds of NSSI and SI were 2.379 and 2.958 in the total sample, 2.579 and 4.034 among those without mental illness, and 2.455 and 2.917 among those with mental illness. These findings suggest that the link between smoking and self-harming behaviors is robust and independent of mental illness status, echoing prior Bangladeshi studies that reported similar associations.28,52 Evidence from the U.S. also supports this connection, with 1 study showing a 2.43-fold increase in SI among adolescent smokers. 59 Biological mechanisms, such as nicotine-induced alterations in serotonin pathways, may contribute by increasing emotional dysregulation and impulsivity. 60 Given the strength and consistency of this association, university mental health initiatives should integrate targeted smoking cessation programs as a core component of suicide and self-harm prevention strategies, ensuring that support is extended to both clinically diagnosed and undiagnosed students.
Our findings mirror global patterns, indicating cyberbullying was a significant predictor of both non-suicidal self-injury and suicidal ideation across all groups (in total sample, students without mental illness and with mental illness). In contrast, traditional bullying did not retain significance in any adjusted model, indicating that online victimization may exert a more potent influence on self-harm behaviors than offline forms of bullying. This is consistent with previous studies showing that students who report NSSI often have a history of being bullied 19 and that the odds of suicidal ideation are higher among those who have experienced bullying. 23 Similarly, an Italian study also indicated that suicidal ideation was significantly associated with bullying. 61 To address this bullying problem, the concerted and coordinated time and attention of parents, educators and school administrators, health care providers, policy makers, families, and others concerned with the care of children. 62 The pervasive nature of cyberbullying, enabled by digital platforms, demands urgent institutional action, including strict anti-harassment policies, digital literacy workshops, and accessible reporting mechanisms. Counseling services should incorporate trauma-informed care to help victims rebuild emotional resilience. The present study identified probable eating disorder as a significant predictor of both self-harm and suicidal ideation. In the total sample, students exhibiting eating-disorder symptoms had twice the odds of engaging in NSSI and 1.64 times higher odds of experiencing SI. Stratified analyses by mental illness status showed that these associations remained significant for NSSI among students both with and without mental illness. However, eating disorder symptoms predicted SI only in those without mental illness. These findings highlight the role of maladaptive coping strategies in managing emotional dysregulation, particularly among students struggling with disordered eating patterns. 63 Prior studies have similarly reported significant associations between eating disorders and both self-injurious behaviors19,22 and suicidal ideation. 61 Given these interconnected risks, universities should implement integrated, multidisciplinary care models that combine nutritional counseling, cognitive-behavioral therapy, and psychiatric support to holistically address eating pathology and reduce the risk of self-harm.
To effectively address self-harming and suicidal behaviors among university students, a suite of evidence-based interventions is warranted based on our study findings. First, routine mental health screenings should be integrated into student registration and significant academic transitions to enable early identification of at-risk individuals. 64 Integrating structured therapeutic programs, such as Dialectical Behavior Therapy and Cognitive Behavioral Therapy, within campus counseling services is crucial, as both have shown strong efficacy in reducing self-injurious behaviors and suicidal ideation.20,31,32 Parallel to this, tobacco cessation programs should be prioritized, given the well-documented association between nicotine use and increased psychological risks. 65 To combat bullying, institutions must enforce robust anti-harassment policies and implement digital literacy workshops, both of which have been shown to reduce victimization and associated mental health risks. 66 Addressing comorbid conditions like disordered eating requires a multidisciplinary model combining nutritional counseling, psychiatric support, and psychotherapy. Lastly, campus-wide mental health awareness campaigns, led by trained student ambassadors and professionals, can normalize help-seeking behavior and reduce stigma, thereby increasing service uptake. 67 Collectively, these strategies can help cultivate a safer, more supportive academic environment that promotes student mental well-being.
This study offers several notable strengths. It provides a comprehensive analysis of the prevalence and predictors of non-suicidal self-injury and suicidal ideation among a large and gender-balanced sample (N = 1401, 51.7% male) of Bangladeshi university students. To our knowledge, this is the first study to report on the prevalence of NSSI in this population. Another key strength of this study lies in its stratified analysis based on the presence or absence of mental illness, specifically depression and anxiety, which provides a more nuanced understanding of the predictors of non-suicidal self-injury and suicidal ideation among university students in Bangladesh. Unlike prior studies that often treat student populations as homogeneous, our analysis revealed that certain risk factors, such as cyberbullying, eating disorders, and smoking, exerted differential effects depending on the presence of mental illness. For example, while smoking and cyberbullying were strong predictors of both NSSI and SI across all groups, eating disorders significantly predicted both outcomes only among students without mental illness, suggesting distinct underlying mechanisms in subclinical populations. These subgroup-specific findings underscore the complexity of self-harming and suicidal behaviors and highlight the need for tailored interventions that account for comorbid psychological conditions.
Several limitations should be noted. First, the cross-sectional design limits the ability to establish causal relationships or temporal sequencing between risk factors and outcomes. Second, self-reported data may be subject to recall bias or social desirability bias, potentially compromising the accuracy of the responses. Third, we relied on single-item self-report measures for NSSI and SI, which, while used in prior research and chosen for feasibility in a large-scale survey, may limit construct validity and do not capture distinctions such as 1-time versus repeated NSSI or passive versus active SI. As our study did not collect data on suicide attempts, we were unable to differentiate between students with ideation only and those who acted on suicidal thoughts. Fourth, the use of brief screening tools (PHQ-2 and GAD-2) for mental illness classification may lead to over- or under-classification compared to structured clinical interviews. Fifth, some subgroup analyses, especially for SI among students without mental illness, were limited by small event counts, which may affect the stability and precision of model estimates. Sixth, although we included a wide range of individual-level predictors, we lacked information on important background confounders such as family history of mental illness or use of mental health services, which may lead to unmeasured confounding. Lastly, the sample was drawn exclusively from students at Jahangirnagar University, which may limit the generalizability of findings to other university populations in Bangladesh. Future studies should employ longitudinal designs, validated multi-item instruments, collect data on suicide attempt, and use broader and more diverse samples to enhance generalizability and deepen understanding of NSSI and SI trajectories.
Conclusions
This study offers the first comprehensive evidence on the prevalence and psychosocial correlates of non-suicidal self-injury and suicidal ideation among university students in Bangladesh. Nearly 1 in 5 students reported experiencing these behaviors, with substantially higher rates among those with mental illness, highlighting a growing mental health crisis within this population. The identification of consistent risk factors, particularly smoking, cyberbullying, and mental health problems, across both mentally healthy and at-risk subgroups provides actionable entry points for institutional intervention. These findings call for universities and policymakers to integrate mental health screening, therapeutic programs, and campus-wide prevention strategies into student support services. Without prompt and sustained action, these preventable behaviors may continue to affect a significant portion of the country’s youth.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251382395 – Supplemental material for Predicting Non-suicidal Self-Injury and Suicidal Ideation Among University Students: A Cross-Sectional Study
Supplemental material, sj-docx-1-inq-10.1177_00469580251382395 for Predicting Non-suicidal Self-Injury and Suicidal Ideation Among University Students: A Cross-Sectional Study by S. M. Rakibul Hasan, Tasnim Tamanna, Md. Emran Hasan, Mahjabin Tasnim Sadia, Al Mahmud, Abu Bakar Siddique, Most. Soudia Hamid Hiya, Tanzim Shahriar Mahin, Sayeda Alvi Khorshed, Bipin Tripura, Alethea Dey, Md. Aminul Islam, Diptta Dey, Sabiha Sultana, Kashfia Mawa, Soma Binta Mostofa, Shahed Hossain, Jahid Hasan, Moneerah Mohammad Almerab, Abdullah Al Habib, Firoj Al-Mamun and Mohammed A. Mamun in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580251382395 – Supplemental material for Predicting Non-suicidal Self-Injury and Suicidal Ideation Among University Students: A Cross-Sectional Study
Supplemental material, sj-docx-2-inq-10.1177_00469580251382395 for Predicting Non-suicidal Self-Injury and Suicidal Ideation Among University Students: A Cross-Sectional Study by S. M. Rakibul Hasan, Tasnim Tamanna, Md. Emran Hasan, Mahjabin Tasnim Sadia, Al Mahmud, Abu Bakar Siddique, Most. Soudia Hamid Hiya, Tanzim Shahriar Mahin, Sayeda Alvi Khorshed, Bipin Tripura, Alethea Dey, Md. Aminul Islam, Diptta Dey, Sabiha Sultana, Kashfia Mawa, Soma Binta Mostofa, Shahed Hossain, Jahid Hasan, Moneerah Mohammad Almerab, Abdullah Al Habib, Firoj Al-Mamun and Mohammed A. Mamun in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors thank all the study participants.
Author’s Note
S. M. Rakibul Hasan is now affiliated with University of South Asia, Dhaka, Bangladesh.
ORCID iDs
Ethical Considerations
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. All procedures involving human subjects were approved by the ethics committee on 17th October 2024 at CHINTA Research Bangladesh [Reference: CHINTA/IRB/10-2024/17(3)]. Prior to commencing the survey, informed written consent was obtained from all participants. Prior to data collection, participants were informed about the study’s objectives, procedures, potential risks, and their rights, including the option to withdraw at any time without consequences. Written informed consent was obtained to confirm their understanding and agreement to participate. To ensure confidentiality, data were securely stored, accessible only to the research team, and used exclusively for research purposes. No monetary or non-monetary incentives were provided.
Consent for Publication
Not applicable.
Author Contributions
SMRH planned the study with guidance and supervision from MMA, FAM, and MAM. SMRH performed the data analysis, wrote the results, and coordinated the overall manuscript preparation. SMRH, TT, MEH, FAM, MAM, and AAH wrote the first draft of the manuscript, contributed to data interpretation, and conducted subsequent edits and review with final input from FAM and MAM. MTS, AM, ABS, MSHH, TSM, SAK, BT, AD, MAI, DD, SS, KM, SBM, SH, JH, and AAH contributed to data collection, data entry, project management, and assisted in data analysis by validating the analyses through individual cross-checking. They also participated in cross-checking and reviewing the manuscript draft. All authors have approved the final version and are accountable for ensuring the accuracy and integrity of the work, committing to investigating and resolving any questions related to the work’s accuracy or integrity.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: MMA is currently receiving funding support from the Princess Nourah Bint Abdulrahman University Researchers Supporting Project (Number PNURSP2025R563), Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data is available at reasonable request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.