
Abstract
To evaluate the impact of the integrated outpatient clinic for chronic diseases (IOC-CD) on the quality of life of hypertension patients in Rural medical alliance of Zhejiang Province, and offer optimization suggestions. We conducted a cross-sectional study using the EuroQol five-dimensional questionnaire (EQ-5D) from October to November 2023. A total of 295 outpatients with essential hypertension were enrolled through random sampling. Trained investigators collected data via face-to-face paper-based questionnaires in waiting areas, and health utility values were calculated accordingly. The average EQ-VAS and utility scores of hypertensive patients in the integrated chronic disease outpatient clinics of the sampled areas are both at a high level. Among the sampled population, the dimension with the most problems is pain/discomfort, while the dimension with the fewest problems is self-care. Multivariate analysis showed that being over 60 negatively impacted health utility and VAS scores. Have a family doctor and satisfaction with pre-/post-visit services positively affected these scores, while satisfaction with in-visit services improved health utility. Hypertensive patients in Zhejiang’s county-level medical alliances receiving chronic disease integrated outpatient care have good health-related quality of life. Future work should expand this integrated clinic model, optimize resource allocation, and improve clinic management and service quality to better meet patients’ health needs and enhance their quality of life.
Keywords
Summary Statement
Investigating the quality of life of hypertensive patients in medical communities of common destiny is crucial. It can inform targeted interventions to enhance patient well-being and optimize resource allocation within the healthcare system.
This study assesses the quality of life of hypertensive patients in rural medical alliance in Zhejiang Province and finds it to be relatively higher than that in other developing countries. It also demonstrates that the quality of life of hypertensive patients is positively correlated with the contracted family doctors and the satisfaction with medical services.
This study highlights that the quality of life of hypertensive patients in rural medical alliance in China is positively correlated with the contracted family doctors and the satisfaction with medical services. This is of great reference significance for improving the service quality of rural medical alliance.
Introduction
As a prevalent chronic condition, hypertension has become a major global public health challenge due to its systemic health risks. 1 Its prevalence ranges from 22% to 48% in developed countries and 24% to 25% in developing nations. 2 Common symptoms include headaches, dizziness, blurred vision, palpitations, and chest pain. Hypertension is strongly associated with severe complications such as stroke, myocardial infarction, heart failure, and kidney damage. These complications not only impair patients’ quality of life but also impose significant economic burdens on families and society. 3 Consequently, assessing the quality of life in hypertensive patients has remained a key focus of academic research.
Hypertension-related quality of life measurement tools are divided into 2 types: general scales like 36-Item Short Form Health Survey (SF-36), EuroQol Five Dimensions Questionnaire (EQ-5D) and World Health Organization Quality of Life Assessment (WHOQOL), and disease-specific scales such as Quality of Life Instruments for Chronic Diseases-Hypertension (QLICD-HY), Patient-Reported Outcome Instrument for Subjective Chronic Disease-Hypertension (PROISCD-HY) and Patient Assessment of Constipation Quality of Life (PAC-QOL).4,5 General scales are widely used internationally, whereas disease-specific scales, despite their greater precision, are less frequently applied. In this study, we selected the EQ-5D instrument to assess quality of life in hypertensive patients. The EQ-5D features a concise yet comprehensive multidimensional framework that effectively captures the impact of common hypertension symptoms (eg, fatigue and physical discomfort) and complications on daily functioning. Moreover, its utility value system enables cost-utility analyses. Recognized for its strong cross-population comparability, the instrument has been endorsed by international health technology assessment organizations. Its reliability and validity have also been well established in the Chinese context.6 -8
The factors currently affecting the quality of life of patients with hypertension mainly include sociodemographic characteristics, health status, lifestyle, cultural and environmental factors, and the accessibility and quality of healthcare services.9,10 These factors vary across countries and regions due to differences in economy, healthcare systems, and culture. In the United States, genetic factors and lifestyle habits lead to significant impacts from racial differences and obesity. 11 In Japan, where there is a general emphasis on healthy lifestyles, patients are mainly affected by socioeconomic factors such as high work stress and a fast-paced lifestyle. 12 In some European countries, the quality of life of hypertensive patients is supported by comprehensive healthcare systems and proactive health promotion policies.13 -15
In China, to enhance the level of primary healthcare services in rural areas, the construction of Rural medical alliance (similar to medical groups) began in 2019. These alliances are led by county-level hospitals and integrate several county-level medical institutions, township health centers, and community health service centers into a unified medical service consortium. 16 In the traditional healthcare model, patient care processes are fragmented, requiring patients to undergo multiple registrations for a single illness—each examination typically requires booking with separate departments, resulting in low efficiency and poor compliance. 17 This inefficient healthcare model has a particularly significant impact on patients with chronic diseases, especially those with hypertension. Hypertension patients require long-term medical management and health monitoring. However, under the traditional healthcare model, the frequent travel and complex procedures make it difficult for many patients to adhere to standardized treatment and follow-up, thereby affecting their quality of life. After medical resources were integrated by the Rural Medical Alliance, it set up clinics that combine outpatient and preventive health services. Patients now complete examination, diagnosis, follow-up, and health education with a single registration, avoiding department transfers. Pre-visit services encompass health screenings, record establishment, intelligent triage, and risk assessment. During visits, doctors develop personalized treatment plans using patients’ current conditions and electronic health records, alongside health education. 17 Post-visit services entail updating health records and active follow-up. 18 In the integrated chronic disease clinics, specific measures have been introduced for patients with hypertension, such as group exercise programs, personalized medication plans, free access to essential medications, and educational courses on health management. Since 2022, these measures have been in place. However, it remains unclear whether they have effectively improved the quality of life of hypertensive patients.
The aim of this study is twofold: (1) to evaluate the quality of life of hypertensive outpatients using the Chinese version of the EQ-5D scale; and (2) to analyze the impact of the integrated chronic disease outpatient services, implemented since the establishment of the Rural Medical Alliance, on the EQ-5D scores. The research findings will help optimize the service model of the integrated chronic disease outpatient clinics, provide scientific evidence for the construction of the Rural Medical Alliance, and further enhance the quality of life of hypertensive patients.
Methods
Participants
The data were collected from Zhejiang Province in eastern China. Considering the geographical distribution of northern, southwestern, and southeastern Zhejiang, as well as the counties with relatively early establishment and distinctive features in the construction of rural medical alliances, we selected 1 to 2 medical alliances in each of 4 regions—Linping, Jiashan, Jiangshan, and Yuhuan—to conduct a cross-sectional survey. One to two rural medical alliances in each region were chosen as survey sites. Each rural medical alliance comprises multiple community hospitals, from which 1 urban, 1 suburban, and 1 urban–rural combined community hospital were selected for the survey. In total, 18 community hospitals under 6 medical alliances were surveyed from October to November 2023. In the waiting area of the integrated chronic disease outpatient clinics at each hospital, approximately 17 hypertensive patients were intercepted and surveyed.
Sample Size
Sample size was determined based on a single population proportion formula with the following assumptions: P = .1 (considering 10% of the population distribution of patients with hypertension regarding HRQoL) to obtain a minimum sample size; W = 0.05 (5% of the marginal error for the two-tailed type I error); Z = 1.96 (at a two- sided 95% confidence level). 19

where, n is the sample size. After considering 10% of the possible non- respondents, the final sample size was at least 154.
Sample Selection
The inclusion criteria for the respondents were as follows: (1) 18 years old and above; (2) diagnosed with essential hypertension; (3) local resident population or floating population living in the area for more than half a year; (4) users of local primary health services; (5) having the ability to communicate independently. The exclusion criteria were: (1) patients with severe chronic diseases (eg, cardiovascular diseases, diabetes, chronic respiratory diseases) and related complications (eg, coronary heart disease complicating hypertension, nephropathy complicating diabetes), to ensure the homogeneity of the study population, reduce the interference of confounding factors, and enhance the accuracy of the research findings; (2) unwillingness to participate in the survey. A total of 305 questionnaires were distributed, and 295 were returned, yielding a response rate of 96.72%.
Quality Control
In the process of data collection, a series of quality control measures were implemented. Before the investigation began, the investigators were trained accordingly. Prior to the formal investigation, the respondents were informed of the purpose and content of the investigation. After obtaining their oral consent, a questionnaire survey was conducted. The questionnaire was filled out by the respondents themselves. After collecting the questionnaires, the investigators thoroughly checked the completeness and authenticity of the content, eliminated any questionnaires that did not meet the requirements, and cleaned the valid questionnaire data.
Measurement Tools
Health-related quality of life was measured using the EQ-5D scale developed by the European Quality of Life Group in 2005, which includes 2 parts: the health status self-assessment questionnaire and the visual analog scale score (EQ-VAS). 20 The self-assessment questionnaire consists of 5 items, covering 5 domains: mobility (MO), self-care (SC), usual activities (UA), pain/discomfort (PD), and anxiety/depression (AD). Each domain is divided into 5 levels on a Likert scale: no difficulty, slight difficulty, moderate difficulty, severe difficulty, and extreme difficulty, represented by the numbers 1 to 5, respectively. The EQ-VAS is a 0 to 100 point scale, where 0 represents the worst health status and 100 represents the best possible health status. Respondents are asked to rate their health status on the day of the survey. The health utility value is calculated using the Chinese version of the valuation system. 21 The formula for calculating the health utility value is 1 − (MO n + SC n + UA n + PD n + AD n ), with a value range of (−0.391, 1). 22 Here, n represents the level of each domain (from 1 to 5). The weight for level 1 of each dimension is 0, while the weights for the other levels are shown in Table 1. In previous studies, the overall Cronbach’s α coefficient of the Chinese version of the EQ-5D-5L scale was .857, indicating good internal consistency reliability. 23 In this study, the Cronbach’s α coefficient of the scale is .823, and the KMO value is 0.796, both of which indicate good reliability and validity.
China EQ-5D Utility Index System.

Satisfaction with integrated outpatient services for chronic diseases, using self-developed questionnaire. It includes 4 aspects: firstly, pre-visit services: (1) The doctor at the integrated chronic disease clinic has established a personal electronic health record for you; (2) The doctor at the integrated chronic disease clinic conducts health education activities to enhance your cognition of health literacy; (3) The doctor/nurse at the integrated chronic disease clinic measures your blood pressure, blood glucose, weight, and records your lifestyle; secondly, services during the visit: (1) The specialist doctor from the township hospital provides you with treatment services at the integrated chronic disease clinic; (2) The doctor at the integrated chronic disease clinic provides you with diagnosis and treatment for common primary care diseases and conducts health examination; (3) The doctor at the integrated chronic disease clinic provides you with diagnosis and treatment services for complex and difficult diseases; (4) The specialist doctor from the township hospital provides you with disease diagnosis and treatment, health education, health assessment, and issue medical and health prescriptions at the integrated chronic disease clinic; thirdly, post-visit services: (1) The family doctor team at the integrated chronic disease clinic provides follow-up and intervention services both online and offline; (2) The doctor at the integrated chronic disease clinic organizes your treatment information and updates it to the health record system; (3) The doctor from the integrated chronic disease clinic followed up to inquire about your recovery; fourthly, satisfaction evaluation: (1) the doctor from the integrated chronic disease clinic provides you with comprehensive and continuous services, covering prevention, treatment, rehabilitation, follow-up, health guidance, and psychological counseling. The Likert 5-level scoring method was used to evaluate the questionnaire items. From “very bad/unsatisfactory ” to “ very good/satisfactory,” 1 to 5 points were assigned respectively. The higher the score, the more satisfied the patients feel. This study selects patient satisfaction as an evaluation indicator based on the theoretical framework of patient-centered care. 24 This framework emphasizes that medical services should be centered around the needs and feelings of patients, and patient satisfaction is one of the important indicators for measuring the quality of medical services. In addition, existing studies have found through empirical analysis that there is a significant positive correlation between patient satisfaction and the quality, safety, and efficiency of medical services.25,26 Therefore, this study uses patient satisfaction as a proxy indicator for evaluating services before, during, and after the visit, which has both theoretical and empirical support.
Social demographic characteristics, including age, gender, household registration, education level, monthly income, marital status, duration of illness, have a family doctor.
Statistical Analysis
EpiData 3.0 (The EpiData Association, Odense, Denmark) was used to establish the database, and missing values in the questionnaire were imputed with the mean. The statistical software SPSS 26.0 (SPSS Inc., Chicago, IL, USA) was used for analysis. Cronbach’s α coefficient was used to measure internal consistency reliability. Structural validity was considered the most effective validity evaluation, and exploratory factor analysis was employed. Descriptive statistical analysis was used to measure the composition and score of each dimension of the EQ-5D-5L scale, the VAS score, and the health utility value. Quantitative variables were described as (mean ± standard deviation), and qualitative variables were described by composition ratio.For the univariate analysis of the impact of demographic characteristics on the quality of life of hypertensive patients, independent t-tests and Kruskal-Wallis (K-W) tests were used. For the multivariate analysis of the impact of demographic characteristics and measures related to the integrated chronic disease outpatient clinic on the quality of life of hypertensive patients, linear regression methods were employed. A P-value of less than .05 was considered statistically significant.
Statement of Compliance with Guidelines
This study adheres to the relevant guidelines provided by the EQUATOR Network to ensure the transparency and scientific rigor of the study design, implementation, and reporting. Specifically, this study follows the STROBE Statement and provides a complete EQUATOR checklist as a Supplemental File (see Supplemental Materials).
Results
Sample Characteristics
Table 2 shows the basic demographic characteristic of the subjects. In this study, a total of 295 hypertensive subjects were surveyed, with the mean age of 65.12 years old (SD = 11.41). 52.20% of them were male, and 74.92% had a countryside district. A majority of the subjects (83.73%) had an educational level of junior high school and below. More than half of the subjects (83.39%) have a monthly income of less than 5500 RMB. Over half of the subjects (52.54%) had a disease duration of more than 10 years.
Demographic Characteristics of Respondents (N = 295).

The Mean Score of EQ-5D Scale
As shown in Table 3, the total score of the scale was 1.21 points (SD = 0.35). Among these, the pain/discomfort domain had the highest score, at 1.46 points (SD = 0.69), while the self-care domain had the lowest score, at 1.08 points (SD = 0.33).
The Scores of Each Domain of EQ-5D Scale.

Single Factor Analysis of Influencing Utility Score and EQ-VAS Score
Table 4 shows the single-factor comparison of utility value and EQ-VAS score among hypertensive patients with different demographic characteristics. The average health utility value of the surveyed hypertensive patients was 0.94 (SD = 0.13), and the EQ-VAS score was 77.04 (SD = 12.09). The results of the single-factor analysis showed that age, having a family doctor, and years of illness had an impact on the health utility value of patients with hypertension (P < .05). Additionally, age, years of illness, and hospital level had an impact on the EQ-VAS score (P < .05).
Single Factor Analysis of Utility Value and VAS Score of EQ-5D SCALE Among Hypertensive Patients with Different Demographic Characteristics.

Note. With * is H value.
The Influence of Demographic Factors on Health Utility Value and VAS Score
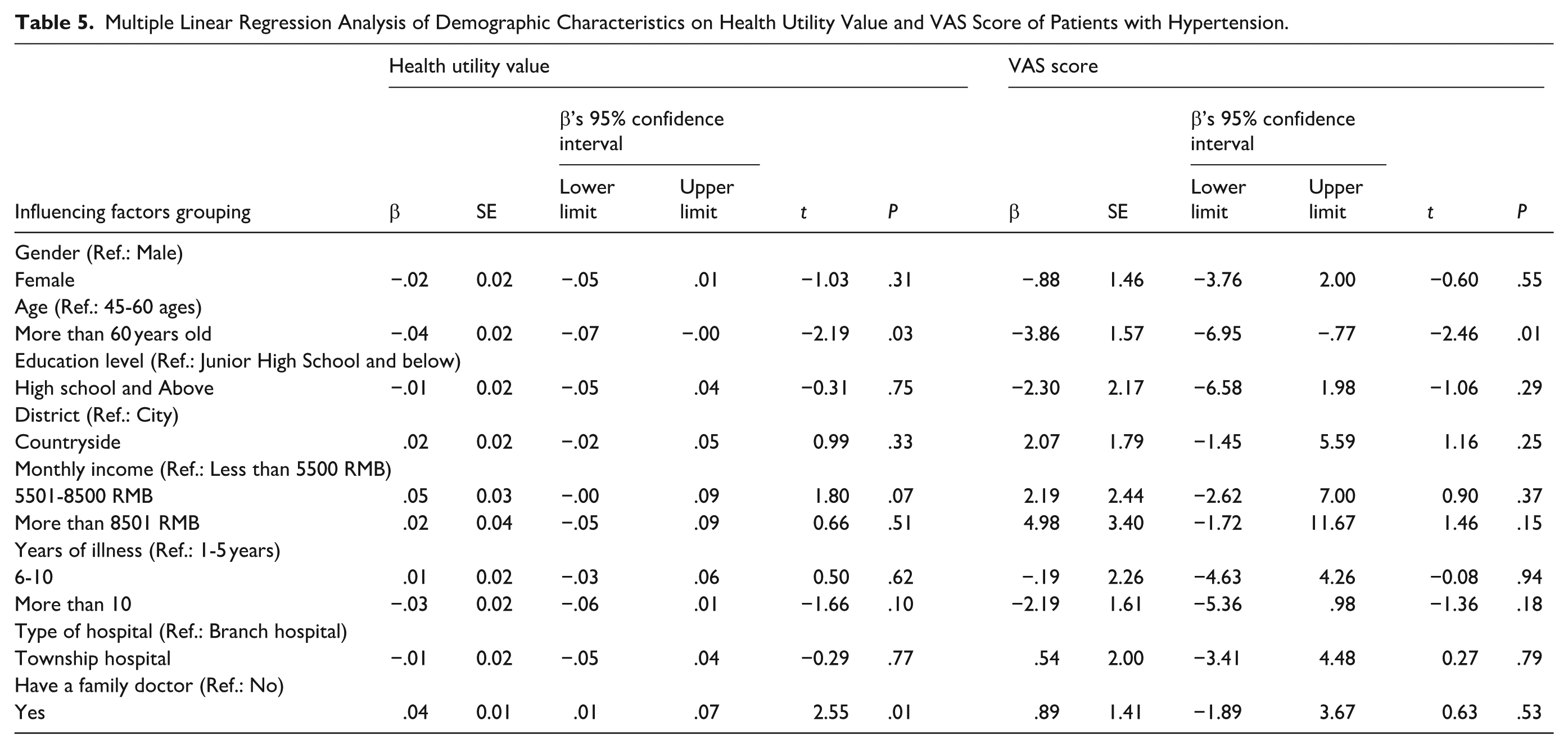
Table 5 presents the multiple linear regression model of the association between socioeconomic-demographic characteristics and health utility values as well as VAS scores among hypertensive patients. There was a positive and statistically significant relationship between higher health utility values and having a family doctor. Lower health utility values and VAS scores were associated with being over 60 years old.
Multiple Linear Regression Analysis of Demographic Characteristics on Health Utility Value and VAS Score of Patients with Hypertension.
The Influence of Integrated Outpatient Service Satisfaction for Chronic Diseases on Health Utility Values and VAS Scores
The multiple linear regression model regarding the association between satisfaction with integrated outpatient services for chronic diseases and health utility values as well as VAS scores is illustrated in Table 6. A statistically significant association was observed between higher health utility values and VAS scores and hypertensive patients’ satisfaction with the establishment of electronic health records by the hospital, the medical treatment services provided by doctors, and the updating of information to the health record system.
Multiple Linear Regression Analysis of the Influence of Integrated Outpatient Service Satisfaction for Chronic Diseases on Health Utility Values and VAS Scores of Hypertensive Patients.

The demographic characteristics such as gender, age, education, marital status, household registration, monthly income, years of illness, hospital type, and whether or not to sign a family doctor in Table 4 are used as the control factors of the regression model.
Discussion
Hypertension is one of the most common chronic non-communicable diseases in China, which can lead to severe complications such as cerebrovascular diseases, heart disease, heart failure, and renal failure. 27 This study was conducted in China following the establishment of the Rural Medical Alliance and the implementation of integrated outpatient clinics for chronic diseases. It is the first to apply the EQ-5D to assess the quality of life in outpatients with hypertension. The study also analyzed the impact of the evaluation score of integrated chronic disease outpatient services on the quality of life in outpatients with hypertension, aiming to provide references for optimizing grassroots chronic disease management services and deepening the construction of the Rural Medical Alliance.This study holds potential significance in 2 key aspects: (1) It can boost patients’ medication adherence, which is closely tied to quality of life. Enhanced quality of life encourages better adherence to prescribed medications, leading to improved blood pressure control. 28 (2) It helps mitigate the risk of cardiovascular diseases. By improving quality of life, it can effectively reduce the incidence and disability rates of hypertension-related cardiovascular and cerebrovascular diseases, ultimately enhancing patients’ long-term prognosis. 29
This study found that the health utility value of hypertensive patients in Zhejiang Province was 0.94, and the average VAS score was 77.40, both of which are at a relatively high level compared to other provinces in China and developing countries abroad (Health utility value: Guangzhou, 0.84; Ethiopia, 0.86. VAS score: Jiangsu Province, 70.00; Slovenia, 70.90).30 -33 This may be attributed to the following factors: Firstly, the active promotion of integrated outpatient clinics for chronic diseases has enabled full-cycle health management for hypertensive patients. These clinics provide one-stop services before, during, and after diagnosis, significantly enhancing patients’ medical experience and disease management level. 34 Secondly, integrated outpatient clinics for chronic diseases offer continuous, safe, and effective personalized medical and health management services to hypertensive patients through family doctor contract services. These services include regular follow-ups, health assessments, drug guidance, and lifestyle interventions. The services provided by family doctors can enhance the trust between medical staff and patients, break down barriers between doctors and patients, and effectively improve the health level of hypertensive patients. 35 Thirdly, the use of information technology in integrated outpatient clinics for chronic diseases, such as electronic health records and electronic medical records, as well as health education through information systems (providing patients with information on chronic disease prevention, treatment, and rehabilitation), has not only promoted the refinement and intelligence of hypertension management but also enhanced patients’ self-management capabilities, which is conducive to improving their quality of life. 36
Among the domains of the EQ-5D, the lowest domain score is pain/discomfort. This may be due to the relatively weak pain management for chronic diseases at the grassroots level in China. For instance, the establishment rate of pain management departments at the primary care level is relatively low, and there is insufficient equipment and technical support for pain management. 37 As a result, hypertensive patients may not receive timely and effective interventions for discomfort symptoms such as headaches and dizziness caused by blood pressure fluctuations. The highest scoring dimension in our EQ-5D assessment was self-care. This finding differs from Western studies where mobility typically scores highest.38,39 The discrepancy may reflect differences in chronic disease management priorities between healthcare systems. China’s primary care system emphasizes maintaining basic living capacities (eg, daily self-care), 40 while Western systems focus more on restoring functional mobility (eg, independent movement), 41 highlighting divergent cultural perspectives on health priorities. Notably, this cross-cultural variation has been corroborated by other research. Bai et al’s multinational comparative study demonstrated that Asian patients generally score higher in self-care dimensions compared to Western counterparts, who show better performance in mobility domains. 42 These differences may stem from varying societal perceptions of health concepts. Our findings further validate this phenomenon, suggesting that both healthcare delivery models and cultural values may jointly influence patients’ self-assessed health status.
This study found that age has a negative impact on the health utility values of hypertensive patients, while having a family doctor has a positive impact. These findings are consistent with other studies.43,44 As age increases, the physiological functions of hypertensive patients decline, the number of comorbidities rises, and their sensitivity to health impacts increases, all of which lead to a decrease in health utility value. 45 On the other hand, family doctors can provide continuous health management services for hypertensive patients, develop personalized treatment plans, and adjust treatment strategies in a timely manner. This long-term, targeted medical service significantly improves the health utility value of hypertensive patients. 46
This study also found that the measures implemented in integrated outpatient clinics for chronic diseases have a positive impact on the health utility value and VAS scores of hypertensive patients. This suggests that integrated outpatient clinics for chronic diseases have significant advantages in improving patients’ health status and quality of life, effectively enhancing their subjective feelings and overall health levels. Specifically, the pre-visit service of “The doctor at the integrated chronic disease clinic has established a personal electronic health record for you” and the post-visit service of “The doctor at the integrated chronic disease clinic organizes your treatment information and updates it to the health record system” both positively influence the health utility value and VAS scores of hypertensive patients. This may be attributed to the following reasons: First, compared with traditional paper-based records, electronic health records offer stronger information integration and security, higher medical service efficiency, and more convenient data sharing. These advantages enable patients to more easily access and manage their health information, thereby enhancing their confidence and participation in disease control, which in turn helps improve their health utility value and VAS scores. 47 Second, the continuity of information recorded in electronic health records before, during, and after visits allows doctors to grasp the overall health status and trends of patients, enabling more targeted personalized management and improved treatment outcomes, thus boosting health utility value and VAS scores. 48 The study also found that the during-visit service of “The specialist doctor from the township hospital provides you with disease diagnosis and treatment, health education, health assessment, and issues medical and health prescriptions at the integrated chronic disease clinic” has a positive impact on the health utility value of hypertensive patients. This might be due to the fact that, unlike traditional chronic disease clinics where doctors only focus on diagnosis and treatment, integrated outpatient clinics combine health education and assessment with medical services. For example, during the consultation, a standardized assessment form is used to screen patients’ medication adherence, dietary habits, and exercise routines. Immediate individualized lifestyle guidance is provided for those with poor blood pressure control. New patients are arranged to attend specialized health education courses to learn about blood pressure monitoring methods and how to recognize emergencies. Regular mental health screenings are also conducted to assess factors such as anxiety and depression. This model, which deeply integrates diagnostic and treatment services with preventive interventions, not only enhances patients’ understanding of the disease but also helps them acquire practical self - management skills, thereby significantly improving their health awareness and effectiveness in behavioral change. 49 Additionally, the implementation of dual health prescriptions (ie, medical prescriptions and health prescriptions including diet, exercise, and lifestyle adjustments) helps patients manage their conditions through lifestyle changes in addition to medication, thereby reducing the risk of complications and improving quality of life. 17
There were some limitations in our study. First, this study was limited to outpatients with essential hypertension in Zhejiang Province, excluding patients with severe complications, which restricts the generalizability of the findings and prevents a comprehensive assessment of quality of life in other hypertension subtypes or regions. Second, significant heterogeneity in health-related quality of life measures across studies—due to varying assessment tools and methodologies—further limits the comparability of conclusions, consistent with issues identified in recent systematic reviews on liver and lung cancers.50,51 Finally, the scales and satisfaction evaluations are based on patients’ subjective perceptions, which may introduce self-report bias and affect the accuracy of the results.
Conclusions
Zhejiang’s rural medical alliances have enhanced hypertensive patients’ health-related quality of life, as shown by higher EQ-5D and VAS scores. Self-care was optimal, while pain management was suboptimal. Integrating non-pharmacological therapies with optimized medication adjustments is recommended. Elderly patients and those with family doctor contracts showed better outcomes, suggesting that quality-of-life (QoL) metrics should be incorporated into physician evaluations. The “pre-visit, during-visit, and post-visit” management cycle improved outcomes. Future chronic disease big data platforms (combining electronic health records, wearables, and insurance data) can establish an intelligent, replicable “Zhejiang Model” for nationwide chronic care.
Supplemental Material
sj-docx-2-inq-10.1177_00469580251382053 – Supplemental material for Influence of Integrated Chronic Disease Management Measures in Rural Medical Alliance on Health-Related Quality of Life of Hypertension Outpatients
Supplemental material, sj-docx-2-inq-10.1177_00469580251382053 for Influence of Integrated Chronic Disease Management Measures in Rural Medical Alliance on Health-Related Quality of Life of Hypertension Outpatients by Xiaoling Lin, Jiajun Li, Qunfang Huang, Linjia Gao, Xu Li, Ping Shao and Chi Zhou in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-1-inq-10.1177_00469580251382053 – Supplemental material for Influence of Integrated Chronic Disease Management Measures in Rural Medical Alliance on Health-Related Quality of Life of Hypertension Outpatients
Supplemental material, sj-pdf-1-inq-10.1177_00469580251382053 for Influence of Integrated Chronic Disease Management Measures in Rural Medical Alliance on Health-Related Quality of Life of Hypertension Outpatients by Xiaoling Lin, Jiajun Li, Qunfang Huang, Linjia Gao, Xu Li, Ping Shao and Chi Zhou in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We thank the help of doctors and nurses from the six-county hospital and 18 community health centers of Hangzhou, Jiashan, Yuhuan, Jiangshan Counties from Zhejiang Province, and all the research staffs during the surveys.
Ethical Considerations
This study was approved by the Hangzhou Normal University Ethics Board (University of Zhejiang, China; No. 2022-1118). Participants have the right to withdraw from the survey at any time without penalty, and those who choose not to participate will not suffer any disadvantages.
Consent to Participate
Informed consent for the procedure was obtained from each participant. Written informed consent form was obtained from each participant prior to the enrollment. A copy of the signed consent form was given to each participant.
Author Contributions
Xiaoling Lin: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Writing-original draft, Writing-review & editing. Jiajun Li: Conceptualization, Data curation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing-original draft, Writing-review & editing. Qunfang Huang: Formal analysis, Investigation, Software. Linjia Gao: Investigation, Software. XuLi: Investigation, Software. Ping Shao: Funding acquisition, Project administration, Resources. Chi Zhou: Funding acquisition, Project administration, Resources, Supervision, Validation, Visualization, Writing-review & editing. All authors have read and agreed to the published version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by National Natural Science Foundation of China (No. 72274050), General Project of Zhejiang Province Medical and Health Science and Technology Program (No. 2024KY1427), Zhejiang Province Soft Science Research Program (No. 2024C35022), the HZNU scientific research and innovation team project (TD2025009).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.