
Abstract
Rural U.S. residents face higher mortality rates and reduced access to primary care physicians. Prior studies report mixed findings on physician supply and health outcomes, and few have examined whether increasing supply reduces rural–urban mortality disparities. The objective was to quantify the marginal benefits of additional primary care physician supply in rural and urban areas, independent of other healthcare and socioeconomic factors. We conducted a 23-year county-level longitudinal observational study of 2942 U.S. counties (1992-2014). Mortality rates were obtained from CDC WONDER, physician supply and socioeconomic characteristics from the Area Health Resource File, and rural–urban classification from the USDA’s 2013 Rural–Urban Continuum Codes. We estimated regressions of age-adjusted mortality rates as a function of physician supply, rurality, and county-level characteristics. Despite the higher per-capita supply of hospital beds and post-acute care services in rural areas, physician supply was lower and grow more slowly than in urban areas. County-level analysis showed a negative association between physician supply and mortality. In rural counties, greater physician supply was associated with lower mortality rate; an increase of 1 physician was associated with 1.4 (CI: −1.963 to −0.836) and 0.936 (CI: −1.411 to −0.462) fewer deaths per 100 k population of older adults in rural counties adjacent and non-adjacent respectively, compared to 0.038 fewer deaths per 100 k population of older adults in urban areas. The declining physicians supply in areas where the number of physicians is already low is an alarming problem for rural communities. Efforts by policymakers to broaden rural health networks and increase rural medical personnel may be needed to address disparities in access to care and associated mortality outcomes. Although the dataset covers 1992 to 2014, the findings remain highly relevant given the continued rural physician shortages and widening mortality disparities that persist across the United States.
Rural residents in the United States experience persistently higher mortality and lower physician availability compared with urban residents.
This 23-year longitudinal study of 2,942 U.S. counties (1992–2014) examined how changes in primary care physician supply relate to mortality across rural and urban areas.
Greater physician supply was associated with significantly lower mortality in rural counties, especially those non-adjacent to urban centers, but not in urban counties.
Post-acute care supply increased in rural areas but was linked to higher mortality, suggesting quality and access challenges. Findings underscore the urgent need for policies that strengthen the rural healthcare workforce and expand access to primary care.
Findings underscore the urgent need for policies that strengthen the rural healthcare workforce and expand access to primary care.
Introduction
Over the past century mortality rates of U.S. older adults declined quite rapidly. During the 1970s and early 1980s mortality rates of the urban and rural county communities were paralleled and there was virtually no gap in the urban-rural mortality rates. However, since mid-1980s mortality rate in urban counties declined more rapidly, resulting in rural-urban mortality gap—which has been widening over the past 3 decades. 1 Despite the long-term goal of US national health initiatives in reducing health disparities, 2 growing evidence suggests that rural residents face considerable disparities in disease, morbidity, potentially preventable deaths, longevity, life expectancy, and mortality compared to their urban counterparts.1,3-6 Causes of these disparities are not yet well understood and rural residents are predominantly affected by health disparities.7,8
Rural residents are typically poorer, less educated, have limited access to healthcare3,9-11 and worse health outcomes3,9 compared to their urban counterparts. Furthermore, rural areas are disproportionately inhabited by the elderly—although only 17% of overall US population reside in rural areas, about 22% of adults 65 years and over live in these areas. With the overall growing population of older adults and the increasing migration of baby boomers to rural communities12,13 accomodating their evolving health service needs becomes more challenging.
Evidence suggests that rural residents are largely affected by limited supply of health services and healthcare professionals.3,11 Despite federal and state programs and efforts to increase rural physician supply, there persists a longstanding disparity in the rural and urban physician supply, 14 and access to primary care physicians is among the top 3 most pressing concerns in rural communities. 2 Given that rural areas face higher mortality rates than their urban counterparts, understanding whether limited physician supply contributes to these disparities is essential. By quantifying the relationship between physician supply and mortality, our study directly examines whether structural workforce shortages are associated with the growing rural-urban mortality gap. According to the 2010 US census bureau data, only 9% of US physicians practice in rural areas, where 17% of the population reside 2 —creating a shortage of rural physicians. On the other hand, some rural communities have higher population-based supply of post-acute care (PAC) services compared to metro communities, especially in terms of skilled nursing facilities (SNF). 15 However, studies indicate a positive associations between supply of SNF and mortality rate. 16 Additionally rural communities have greater proportion of frail older adults compared to urban communities, 17 however, evidence suggests that there is a significant rural-urban disparity in the quality of nursing home, 17 staffing quality, quality of nursing home care, and even larger disparity in the more isolated nursing homes. 18 In terms of home health care, although studies find no difference in the likelihood of receiving formal home health care, there are fewer provider days in rural and remote area compared to urban areas. 19
In order to achieve equity, research is needed to determine health needs of rural communities. While rural-urban mortality disparity has been well-documented in prior studies,3,10,20 reasons behind this is unclear. Evidence on the relationship between physician supply and mortality are mixed.21-24 For example, Starfield et al 22 found a negative association between primary care physician supply and mortality after adjusting for state-level characteristics, and Chang et al 21 documented reductions in mortality among Medicare beneficiaries associated with greater primary care physician supply. In contrast, Krakauer et al 23 found negligible effects of physician supply and physician mix on mortality among Medicare beneficiaries, and Spencer et al 25 reported that county-level socioeconomic factors rather than physician supply explained rural-urban mortality differences. Prior studies, including Basu et al, 24 have also examined the association between physician supply and population health outcomes, and found significant associations with preventable mortality. However, much of this work has been limited in either timeframe, geography, or scope. These inconsistencies highlight the need for additional evidence. Our study builds on this literature by employing a 23-year county-level longitudinal design with stratification by rurality providing evidence on long-term structural workforce gaps. We examined the marginal benefits of additional physician supply on mortality rates in rural and urban areas. The concept of marginal benefits is important because the relationship between physician supply and population health outcomes is not linear: additional physicians provide greater gains when the baseline supply is low, as is often the case in rural areas, and diminishing returns when the baseline supply is high, as in many urban areas. Our analysis focuses on primary care physicians, who are the cornerstone of healthcare delivery in rural communities during the study period, and who play a particularly critical role in addressing disparities in access to essential services.
Methods
Data Sources
We conducted a county-level longitudinal observational study spanning 1992 to 2014. We created an analytic dataset that included 2942 U.S. counties across all 50 states and the District of Columbia. In the United States, counties are the primary administrative subdivisions within states, typically ranging in population from fewer than 1000 residents to several million, and they are a standard geographic unit for health data reporting and policy analysis. The study period was selected because these years represent the time frame for which consistent and complete county-level data on physician supply, mortality, and other health system characteristics were available across the Area Health Resource File (AHRF), CMS’s OSCAR data, and additional sources. More recent years were excluded because comparable county-level data on physician supply were not available. Despite the data ending in 2014, this 23-year window provides a unique opportunity to document historical workforce gaps and examine long-term rural-urban disparities.
Data were obtained from 4 different sources:
Area Health Resources and Administration Files (AHRF): National county level health resources database and contains data about the availability of different types of health care services as well as population and economic data in each county, gathered from the Census Bureau, Medicare and Medicaid Services (CMS), and the Bureau of Labor Statistics.26,27
Compressed Mortality Files (CMF): Longitudinal county-level national mortality file and a corresponding county-level national population database, produced by the National Center for Health Statistics (NCHS), at the Centers for Disease Control and Prevention (CDC). 28
Provider of Services (POS) which contains data on characteristics of hospitals and other types of healthcare facilities collected through the CMS Regional Offices.
Online Survey, Certification and Reporting (OSCAR): The most comprehensive facility-level source on the operations, patient census and regulatory compliance of nursing facilities, contain information on facility characteristics, aggregate resident characteristics, and staffing levels, collected by the CMS in cooperation with the state long-term care surveying agencies.
Study Population
The assembled longitudinal dataset includes 2942 counties from all 50 US states and the District of Columbia spanning 1992 to 2014, as described in the Rural-Urban Classification section. Missing values were imputed for the number of physicians (2942 observations imputed for year 2009) and per-capita income (2915 observations imputed for year 2009) using the average value of the observed variables in 2008 and 2010. No other variables had missing data, and therefore no additional imputations were required.
Variables
Outcome
The study outcome was county-level age-adjusted mortality rate of population 65 and older, obtained from CMF files. We used age-adjusted rates to eliminate variations caused by different age distributions across counties. The age-adjusted death rate is the weighted average of age-specific death rates, where the weights represent a fixed population by age. Rates are calculated per 100 k population and are based on the 2000 US standard population. 29
Main Explanatory Variable
The main explanatory variable was physician supply, defined as the number of active non-federal physicians in a given county-year, obtained from AHRF files. The non-federal physicians include non-Federal doctors of medicine (M.D.) and doctors of osteopathy (D.O.) providing direct patient care who practice principally in 1 of the 4 primary care specialties-general or family practice, general internal medicine, pediatrics, and obstetrics and gynecology. Physicians engaged solely in administration, research and teaching were excluded.
Rural-Urban Classification
We used US Department of Agriculture’s Economic Research Service (ERS) 2013 Rural-Urban Continuum Codes (RUCCs) to classify counties as rural or urban. RUCCs are 9-level county classification scheme that distinguishes counties as metropolitan (codes 1-3) and non-metropolitan (4-9) based on population size and adjacency to a metropolitan county. Since proximity to a metropolitan area may affect access to health services, we classified counties with codes 1 to 3 as urban and further classified non-metropolitan counties based on proximity to a metropolitan area as those adjacent (codes 4, 6, 9) and non-adjacent (codes 5, 7, 9) to an urban area.30-32 Using RUCC-2013, of the 3143 US counties, 93 were not in the 2013 Rural Urban continuum codes. Counties with unreliable mortality rates, defined as a rate with a numerator of 20 or less, were excluded. The final sample comprised 2942 US counties in 50 states and the District of Columbia (108 counties). Study size reflected the universe of U.S. counties meeting these data-quality criteria.
Covariates
Capacity of care measures included number of hospital beds, number of skilled nursing facility (SNF) beds, and Home Health Agencies (HHAs) in a given county-year, obtained from POS file, and OSCAR survey database. We also account for several socioeconomic controls such as percent female, percent Black, percent other non-White race, taken form CMF files, unemployment rate, and income per capita, taken from AHRF files, in each county-year.
Statistical Analysis
We examined trends in age-adjusted mortality rates in rural and urban counties from 1992 to 2014 and compared them with trends in physician supply and other capacity of care measures, all weighted by county population. To illustrate changes in physician supply and mortality lucidly we calculated and examined the change in these measures relative to the year 1992.
In our primary analysis we estimated the association between physician supply (number of physician in in a given county-year) and age-adjusted mortality using linear regression with county and year fixed effects, and the interaction of rurality with the main explanatory variable and all covariates, controlling for county-level capacity of care (total number of supply in a given county year), and socioeconomics characteristics, weighted by county population. Physician supply was scaled as physicians per 100 000 population, and regression coefficients are interpreted as the marginal association of 1 additional physician per county. Per-capita income and other continuous covariates were entered as linear terms without transformation. Missing values for physician supply and per-capita income in 2009 were imputed using the average of 2008 and 2010 values; no other variables had missing data. We used county fixed effects to account for unobserved, time-invariant differences between counties that may drive trends in physician supply or mortality. Year fixed effects were used to account for possible shocks to physician supply in any given year. Thus, the effect of physician supply is equal to the average within-county mortality change associated with within-county physician supply change—while holding constant changes in other socioeconomic characteristics and other healthcare service measures.
Bias: Several potential sources of bias were considered. Residual confounding is possible due to unmeasured county-level characteristics not captured in available datasets. The ecological nature of the study introduces the potential for ecological fallacy, as associations at the county level may not reflect individual-level relationships. Reverse causality may partly explain positive associations between post-acute care supply and mortality, as areas with greater illness burden may require more facilities. Measurement error is also possible in physician supply counts, as the AHRF does not distinguish workload, specialty detail, or practice intensity. To mitigate these concerns, we incorporated county and year fixed effects, adjusted for a broad set of sociodemographic and healthcare characteristics, and used clustered standard errors at the county level. No additional sensitivity analyses were conducted.
Results
Age-Adjusted Mortality and Physician Supply
Of the 3142 U.S. counties, 200 were excluded due to unreliable mortality rates (numerator ≤ 20). The analytic sample comprised 2942 counties contributing 67,666 county-year observations over 23 years of follow-up (1992-2014). From 1992 to 2014, age-adjusted mortality rates declined in all 3 types of counties (Figure 1 Panel A)—with the lowest mortality rate in urban counties and the highest in rural non-adjacent counties throughout the years of study. Age-adjusted mortality rate in urban counties decreased by 20%. However, mortality rates in in rural adjacent and non-adjacent counties declined by 12% (Panel B)—specifically, in urban counties mortality declined from 5175 deaths per 100 k persons in 1992 to 4120 deaths in 2014. In rural adjacent and non-adjacent counties mortality rate declined from 5376 and 5276 deaths per 100 k in 1992 to 4678 and 4622 deaths in 2014, respectively.

Trend in age-adjusted mortality rate of population 65 and older (1992-2014).
Figure 2 displays the change in physician supply and per capita physician supply from 1992 to 2014 by rurality. In urban counties per capita physician supply increased by 35% during the study period, from 2.5 in 1992 to 3.0 physicians per 1 k population in 2014. In rural counties, per capita physician supply was lower than that of urban counties in all years. Although rural physician supply increased between 1992 and 2002, there was a sharp, persistent decline afterward resulting in lower relative growth. Per capita physician supply in rural adjacent counties increased by 14%, from 0.9 in 1992 to 1.0 physician per 1 k population in 2014. In rural non-adjacent counties per capita physician supply has increased from 1.0 in 1992 to 1.2 physicians per 1 k population in 2014, a 20% increase.

Trends in physicians supply (1992-2014).
Supply of hospital beds declined in all 3 types of states, a decline which was faster (16% change) in urban counties and rural adjacent counties compared to rural non-adjacent counties (10% change; Figure 3 Panel A). SNF bed supply fell in all counties during the study period. In rural counties SNF beds per capita fell by about 20%, while in urban counties SNF beds supply initially increased by 40% between 1992 and 1996 and declined by 40% decline afterward (from 48 beds to 34 beds; Panel B). Although per capita supply of HHAs increased in all types of counties, growth was substantially higher in urban counties (120% change) compared with rural counties (40% change; Panel C). Unadjusted descriptive statistics and trends by rurality are shown in Table 1 and Figure 1, while regression models report confounder-adjusted associations with 95% confidence intervals.
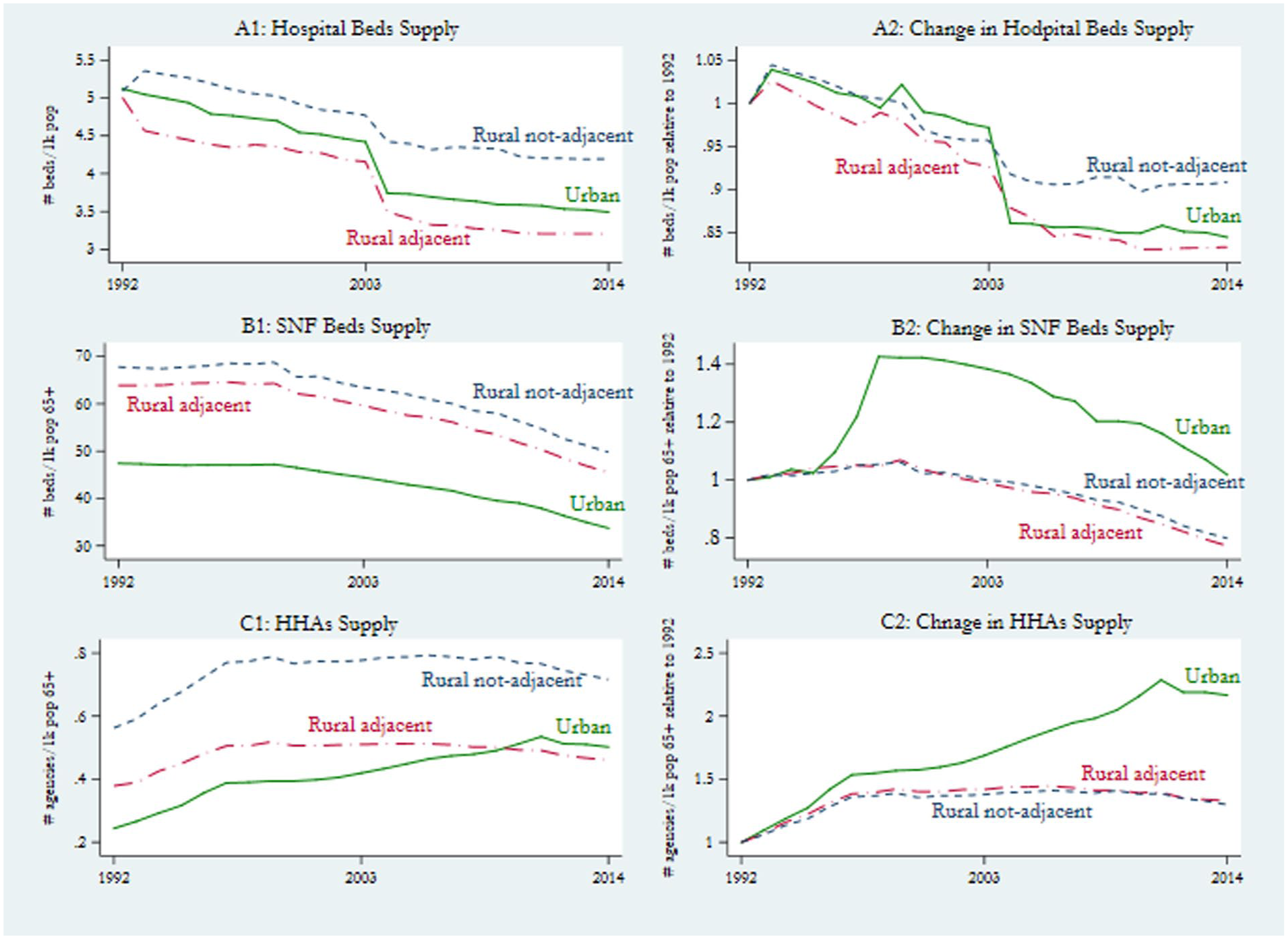
Trends in measures of capacity of care supply.
Descriptive Statistics (1992-2014).

Note. The sample includes 23 years of data on 2942 US counties from all 50 US states and the District of Columbia (New Jersey, Rhode Island, Delaware and District of Columbia do not have non-metropolitan counties). No missing data were observed for variables except physician supply and per-capita income in 2009, which were imputed using values from 2008 and 2010.
Association Between Physician Supply and Mortality
Greater physician supply was most strongly associated with lower mortality rate in rural counties—an increase of 1 physician in a rural non-adjacent county was associated with 0.936 fewer deaths per 100 k older population (95% CI: −1.411 to −0.462; Table 2). An increase of 1 physician in rural adjacent counties was associated with 1.400 fewer deaths per 100 k (95% CI: −1.963 to −0.836), while in urban counties increase in physician supply was associate with decline in mortality by −0.038 deaths per 100 k.
Association between availability of care and age-adjusted mortality rate in urban, rural adjacent and rural non-adjacent counties in 2942 US counties, 1992 to 2014.

Source. Authors’ calculation based on AHRF, CMF, POS and OSCAR data files.
Note. The estimates have been weighted by county population size. Robust standard errors in parentheses.
P < .01. **P < .05. *P < .1.
Change in hospital bed supply were also associated with reduced mortality in rural adjacent counties, however the magnitude of the effect was small (−0.019, 95% CI: −0.032 to −0.005). In urban and rural non-adjacent counties, change in hospital bed supply associated with higher mortality rate. Change in SNF bed supply was associated with slightly increased mortality in rural counties, however in urban counties an increase of 1 SNF bed per county is associated with fewer deaths per 100 k population. A 1-unit increase in SNF beds per county was associated with 0.015 fewer deaths per 100 k (95% CI: −0.028 to 0.003) in urban counties, 0.382 more deaths per 100 k (95% CI: 2.1 to 4.0) in rural adjacent counties, and 0.333 more deaths per 100 k (95% CI: 1.7 to 4.1) in rural non-adjacent counties. HHA supply was also positively associated with mortality. In rural adjacent counties a 1 unit increase in number HHA in a county was associated with an increase in deaths by 15.220 per 100 k (95% CI: 8.431 to 22.014). In rural non-adjacent counties, a 1 unit increase in HHA supply was associated with 27.730 more deaths per 100 k (95% CI: 18.061 to 37.399). However, in urban counties change in HHA supply and mortality were not associated. Subgroup analyses stratified by rurality (urban, rural-adjacent, and rural-nonadjacent counties) confirmed that associations between physician supply and mortality were concentrated in rural areas, particularly non-adjacent counties. No additional sensitivity analyses were conducted.
Discussion
In this historical national study of US older population, we found that between 1992 and 2014 mortality in urban counties declined more rapidly than mortality in rural counties; however, physician supply was steadily increasing in urban counties while concurrently declining in rural counties from early 2000s. These results should be interpreted as associations, not causal effects, given the ecological design and the potential for unmeasured confounding. We found that an increase in greater physician supply was associated with lower mortality rates in rural areas, but the association was not evident in urban areas. The association was strongest for rural counties non-adjacent to an urban area.
In contrast, no association was observed between physician supply and mortality in urban counties. We also found that greater supply of SNF beds and HHAs was positively associated with mortality, although these associations should be interpreted cautiously. These associations may in part reflect alternative explanations. For example, the positive association between SNF/HHA supply and mortality may reflect reverse causality, in which greater post-acute care supply is concentrated in areas with higher burdens of severe illness. Similarly, the absence of an association in urban areas may reflect a saturation effect, where baseline physician availability is already high and additional providers yield limited marginal benefits. These possibilities underscore the importance of considering both supply-side and population health demand factors when interpreting workforce–mortality relationships.
Furthermore, the gap in rural-urban age-adjusted mortality rate for the population 65 and over started in mid 1980s (Appendix Figure 1), however prior studies focusing on all US population detect the start of the gap to be in the 1990s.1,33 Older adults are more vulnerable to health issues since they have high prevalence of multiple chronic conditions, which may result in the earlier onset of healthcare needs and access to care and higher mortality rates.
We found that 1 additional physician per county was associated with 1.4 and 0.936 fewer deaths per 100 k population in rural adjacent and non-adjacent counties, respectively. Consistent with our study, in a 10-year temporal study on Medicare beneficiaries, Chang et al 21 found that an increase of 1 primary care physicians per 10 k population is associated with 15.1 fewer deaths per 100 k population. Starfield et al 22 and researchers found a negative association between primary care physician supply and mortality rate controlling for state-level economic and demographic characteristics in the overall population and similar results using different levels of rurality, but a positive association between increase in specialist and higher mortality. However, in a cross-sectional study on Medicare beneficiaries Krakauer et al 23 found a negligible effect of physician supply and the proportion of specialist and generalist on mortality rate, and in a 30 year study of all US counties, Spencer et al 25 and researchers explained rural urban mortality differences by county-level economic and demographic characteristics and did not find any association between supply of physicians and mortality. Our findings suggest that these mixed results in the literature may be partly explained by the concept of marginal benefits. Because the impact of physician supply depends on baseline levels, rural counties with lower supply exhibit larger health gains from additional physicians, whereas urban counties with already high supply levels show smaller or negligible effects. This framework helps reconcile why some prior studies reported strong associations between physician supply and mortality, while others observed little to no effect. The controversy in these studies could be due to the downward sloping nature of marginal benefits curve, implying that marginal benefits of additional physician being dependent on the level of supply. Thus, rural areas operating at lower levels of physician supply, their marginal benefits of additional physician would be higher compared to urban areas.
The shortage of rural physicians is a long-standing problem in the US. Although the Graduate Medical Education system has been producing more physicians in the last couple of decades, it has failed to produce more primary care physicians, to provide care to rural populations. 34 Family physicians are the main providers of health care services in rural areas.35,36 Although the creation of family practice residence as a separate specialty in the 1970s has led better preparation for future rural physicians, there has been a decline in medical students interest in family medicine over the past decades. 37
Rural-urban disparities in physician supply may worsen with the decline in interest in family medicine, which is the predominant specialty of rural practitioners declines among medical students,35,36 and increase in the number of female physicians 36 and the proportion of physicians with highly educated spouses, 38 which are less likely to serve in rural areas. Moreover, despite numerous federal- and state-level initiatives aimed at attracting physicians and medical students to serve in rural areas, there are several reasons for why rates of turnover are high and retention are low.14,39 For instance, many programs incentivizing rural employment obligate physicians to practice in rural areas for only fixed period of time, after which many physicians choose to leave. There is high mobility of primary care physicians within the rural communities, particularly in the very remote locations and those already having poorer physician supply. 40 Attrition is particularly high in extremely remote areas and may not only impact community health directly by reducing health care supply, but also by diminishing the quality of available care. For instance, in rural communities fewer physicians are responsible for more patients compared with physicians in urban areas.41,42 In addition, attrition among physicians may impact individuals’ level of confidence in the healthcare system, when a physician leaves and a new physician is sent to serve them, while it takes time for human beings to trust a physician and seek their health visits, as trust has been shown to be positively related to patient enhanced continuity of care and medication adherence,43,44 leading to underutilization of healthcare that may be conflated with cultural resistance to healthcare. Policy makers must be aware of the key problems that the low supply along with high attrition of physicians bring to the society and more effectively target policies to provide additional support needed by these vulnerable communities.
Although rural physician supply has decreased over time, per capita supply of post-acute care services has grown at higher rates in rural areas, a finding consistent with other studies. 15 However, we found that both SNF bed supply and HHAs supply in rural counties were associated with increased mortality, which has also been previously documented. 16 These results may be driven by the differences in the lower quality of care provided by SNFs17,18 and significantly fewer number of provider days received from HHAs in rural areas compared to their urban counterparts. 19 While the data span ends in 2014, more recent studies confirm that the structural shortages in rural physician supply and the rural-urban mortality gap have not improved significantly, and in some areas have worsened. 24 By documenting long-term associations over a 23-year period, our analysis provides historical grounding for understanding the policy inertia that has contributed to persistent disparities. These findings remain timely as rural health workforce issues continue to challenge health system planning and mortality outcomes today. Although our study includes nearly all U.S. counties, findings may not generalize beyond the United States, given differences in health systems and physician distribution internationally; within the U.S., however, the county-level scope enhances external validity across diverse geographic contexts.
Limitations
Our study has several limitations. First, a statistical association between mortality and its predictors does not necessarily indicate causation. We therefore advise caution in interpreting the results. However, our study employed a national county-level longitudinal study design that generated findings with stronger inference than a cross-sectional design. Second, to identify physicians and their practice locations, we used Area Health Resource File and used active non-federal physicians as the measure of physician supply. We assumed that all active physicians practiced with similar effort despite their specialty and years of experience. Third, we did not have sufficient information on nurse practitioners and physician assistants, who represent an essential part of the rural healthcare workforce and, in many cases, provide the majority of primary care services in rural areas. Their exclusion is a notable limitation of our analysis. Moreover, state-level variation in scope-of-practice policies governing nurse practitioners and physician assistants introduces additional complexity that cannot be adequately captured in the present dataset. Future work, including our ongoing research using more recent data from 2010 onward, will incorporate APP supply and regulatory context to provide a more comprehensive understanding of the rural health workforce. Additionally, our dataset covers the years 1992 to 2014, which does not capture more recent changes in healthcare delivery, particularly the expansion of telemedicine and the shifts that occurred during the COVID-19 pandemic. While these developments are important and may have altered access to primary care in rural communities, our analysis provides essential historical grounding that highlights the persistent nature of rural workforce shortages and mortality disparities. Moreover, recent studies confirm that rural physician shortages and mortality disparities have continued, and in some cases worsened, since 2014, underscoring the continued relevance of our findings. For example, a 2024 USDA Economic Research Service report documented that prime working-age mortality in rural areas was 43% higher than in urban areas by 2019—a stark increase from just a 6% difference in 1999. 45 Loccoh et al 46 similarly demonstrated widening rural–urban mortality disparities, particularly among low-income populations, and CDC/NCHS surveillance data show that rural counties continue to exhibit higher age-adjusted mortality rates across the leading causes of death through 2019.
Moreover, recent studies confirm that rural physician shortages and mortality disparities have continued, and in some cases worsened, since 2014, underscoring the continued relevance of our findings. In addition, while family physicians represent a critical component of primary care in rural areas, specialty-specific physician counts were not consistently available across all counties for the 1992 to 2014 study period. Therefore, our analysis used overall physician counts rather than restricting to family physicians. Future research with more detailed specialty data will be able to provide further insight into the unique role of family physicians and other primary care providers in addressing rural-urban disparities. Residual confounding would likely attenuate the observed associations, whereas reverse causality could partly explain the positive associations between post-acute care supply and mortality.
Conclusions
In conclusion, we found that greater physician supply was associated with lower mortality. These findings suggest that policies to increase physician supply in rural areas may help address disparities in mortality and other adverse health outcomes for older adults residing in these areas. Declining physicians supply in areas where the number of physicians is already lower is an alarming problem for rural communities. Although residents of rural areas adjacent to urban communities may have access to some of the same healthcare resources, a lack of community medical personnel may still exacerbate growing health problems. Efforts by policy makers to broaden rural health networks and increase rural medical personnel may be needed to strengthen access to care and mitigate observed rural–urban disparities.
Footnotes
Appendix
Association between availability of care and age-adjusted mortality rate in urban, rural adjacent and rural non-adjacent counties in 2942 US counties, 1992 to 2014.

| Model 1 | Model 2 | Model 3 | Model 3 | Model 4 | Model 5 | |
|---|---|---|---|---|---|---|
| Physician supply | ||||||
| Urban | −0.0441*** | −0.0365*** | −0.0376*** | −0.0389*** | −0.0430*** | −0.0478*** |
| Std. err. | (0.00563) | (0.00527) | (0.00646) | (0.00644) | (0.00867) | (0.00710) |
| 95% CI | −0.0551 to −0.0330 | −0.0468 to −0.0262 | −0.0503 to −0.0249 | −0.0515 to −0.0263 | −0.0600 to −0.0260 | −0.0617 to −0.0339 |
| Rural, adjacent | −1.146*** | −1.134*** | −1.400*** | −1.560*** | −1.270*** | −1.186*** |
| Std. err. | (0.278) | (0.278) | (0.287) | (0.288) | (0.387) | (0.286) |
| 95% CI | −1.691 to −0.601 | −1.679 to −0.589 | −1.963 to −0.836 | −2.125 to −0.994 | −2.029 to −0.511 | −1.747 to −0.626 |
| Rural, not adjacent | −0.840*** | −0.840*** | −0.936*** | −0.981*** | −0.932** | −0.822*** |
| Std. err. | (0.215) | (0.214) | (0.242) | (0.247) | (0.379) | (0.254) |
| 95% CI | −1.262 to −0.419 | −1.260 to −0.421 | −1.411 to −0.462 | −1.465 to −0.496 | −1.675 to −0.188 | −1.319 to −0.325 |
| Hospital bed supply | ||||||
| Urban | 0.0203*** | 0.0225*** | 0.0211*** | 0.0105** | 0.0213*** | |
| Std. err. | (0.00351) | (0.00419) | (0.00424) | (0.00424) | (0.00440) | |
| 95% CI | 0.0134-0.0271 | 0.0142-0.0307 | 0.0128-0.0294 | 0.00221-0.0188 | 0.0126-0.0299 | |
| Rural, adjacent | −0.0160** | −0.0188*** | −0.0187*** | −0.0211 | −0.0205 | |
| Std. err. | (0.00688) | (0.00683) | (0.00696) | (0.0317) | (0.0288) | |
| 95% CI | −0.0295 to −0.00251 | −0.0322 to −0.00543 | −0.0324 to −0.00508 | −0.0833 to 0.0411 | −0.0769 to 0.0359 | |
| Rural, not adjacent | 0.143 | 0.149* | 0.152* | 0.181 | 0.118 | |
| Std. err. | (0.0905) | (0.0901) | (0.0904) | (0.110) | (0.0919) | |
| 95% CI | −0.0338 to 0.321 | −0.0280 to 0.325 | −0.0255 to 0.329 | −0.0353 to 0.398 | −0.0620 to 0.298 | |
| SNF bed supply | ||||||
| Urban | −0.0152** | −0.0112* | −0.0112* | −0.0146** | ||
| Std. err. | (0.00605) | (0.00583) | (0.00672) | (0.00646) | ||
| 95% CI | −0.0271 to −0.00337 | −0.0227 to 0.000199 | −0.0244 to 0.00194 | −0.0273 to −0.00195 | ||
| Rural, adjacent | 0.382*** | 0.368*** | 0.296*** | 0.330*** | ||
| Std. err. | (0.0628) | (0.0630) | (0.0848) | (0.0648) | ||
| 95% CI | 0.259-0.505 | 0.245-0.492 | 0.130-0.462 | 0.204-0.457 | ||
| Rural, not adjacent | 0.333*** | 0.316*** | 0.261* | 0.294*** | ||
| Std. err. | (0.101) | (0.100) | (0.140) | (0.103) | ||
| 95% CI | 0.136-0.531 | 0.120-0.513 | -0.0144-0.536 | 0.0912-0.496 | ||
| HHA supply | ||||||
| Urban | 0.0216 | 0.0240 | −0.0338 | 0.00136 | ||
| Std. err. | (0.0606) | (0.0592) | (0.0602) | (0.0595) | ||
| 95% CI | −0.0971 to 0.140 | −0.0921 to 0.140 | −0.152 to 0.0841 | −0.115 to 0.118 | ||
| Rural, adjacent | 15.22*** | 14.29*** | 6.486 | 13.70*** | ||
| Std. err. | (3.465) | (3.461) | (5.450) | (3.742) | ||
| 95% CI | 8.431-22.01 | 7.510-21.08 | −4.196 to 17.17 | 6.362-21.03 | ||
| Rural, not adjacent | 27.73*** | 26.41*** | 16.74** | 31.34*** | ||
| Std. err. | (4.933) | (4.876) | (7.444) | (5.547) | ||
| 95% CI | 18.06-37.40 | 16.85-35.97 | 2.148-31.33 | 20.47-42.21 | ||
| Per capita income | ||||||
| Urban | −0.00868*** | −0.00857*** | −0.00836*** | −0.00782*** | −0.00653*** | |
| Std. err. | (0.000631) | (0.000620) | (0.000643) | (0.000620) | (0.000825) | |
| 95% CI | −0.00992 to −0.00745 | −0.00978 to −0.00735 | −0.00963 to −0.00710 | −0.00904 to −0.00661 | −0.00815 to −0.00491 | |
| Rural, adjacent | −0.000584 | −0.000688 | −0.000490 | 0.000647 | 0.00287** | |
| Std. err. | (0.000918) | (0.000913) | (0.000939) | (0.000914) | (0.00120) | |
| 95% CI | −0.00238 to 0.00121 | −0.00248 to 0.00110 | −0.00233 to 0.00135 | −0.00114 to 0.00244 | 0.000511-0.00523 | |
| Rural, not adjacent | 0.00280*** | 0.00290*** | 0.00224*** | 0.00333*** | 0.00386*** | |
| Std. err. | (0.000843) | (0.000843) | (0.000858) | (0.000841) | (0.00104) | |
| 95% CI | 0.00115-0.00445 | 0.00125-0.00455 | 0.000560-0.00392 | 0.00168-0.00498 | 0.00182-0.00589 | |
| Unemployment rate | ||||||
| Urban | −8.921*** | −9.705*** | −10.61*** | −17.61*** | −15.39*** | |
| Std. err. | (1.557) | (1.527) | (1.523) | (1.667) | (1.572) | |
| 95% CI | −11.97 to −5.869 | −12.70 to −6.712 | −13.60 to −7.626 | −20.87 to −14.34 | −18.47 to −12.31 | |
| Rural, adjacent | −0.716 | −1.141 | −0.460 | −8.266*** | −3.141* | |
| Std. err. | (1.675) | (1.666) | (1.661) | (2.003) | (1.707) | |
| 95% CI | −3.999 to 2.567 | −4.407 to 2.125 | −3.716 to 2.797 | −12.19 to −4.339 | −6.487 to 0.204 | |
| Rural, not adjacent | −0.275 | −0.629 | 1.836 | −6.320** | 1.097 | |
| Std. err. | (2.359) | (2.353) | (2.335) | (2.786) | (2.404) | |
| 95% CI | −4.899 to 4.349 | −5.241 to 3.982 | −2.740 to 6.412 | −11.78 to −0.861 | −3.615 to 5.808 | |
| Population male | ||||||
| Urban | 7.527*** | 6.873** | 7.425*** | 6.027** | 7.786** | 2.055 |
| Std. err. | (2.772) | (2.769) | (2.803) | (2.788) | (3.369) | (2.843) |
| 95% CI | 2.093-12.96 | 1.446-12.30 | 1.930-12.92 | 0.563-11.49 | 1.182-14.39 | −3.517 to 7.628 |
| Rural, adjacent | 9.202*** | 9.094*** | 9.185*** | 9.988*** | 10.59*** | 10.38*** |
| Std. err. | (2.151) | (2.150) | (2.155) | (2.156) | (2.330) | (2.265) |
| 95% CI | 4.986-13.42 | 4.880-13.31 | 4.962-13.41 | 5.762-14.21 | 6.027-15.16 | 5.944-14.82 |
| Rural, not adjacent | 3.841** | 3.803** | 3.728** | 4.279** | 6.628*** | 4.870** |
| Std. err. | (1.824) | (1.823) | (1.828) | (1.833) | (2.050) | (1.931) |
| 95% CI | 0.265-7.416 | 0.229-7.377 | 0.145-7.311 | 0.686-7.872 | 2.610-10.64 | 1.085-8.654 |
| Population Black | ||||||
| Urban | −10.61*** | −10.26*** | −9.826*** | −10.16*** | −4.794*** | −10.67*** |
| Std. err. | (1.496) | (1.459) | (1.413) | (1.380) | (1.810) | (1.458) |
| 95% CI | −13.54 to −7.673 | −13.12 to −7.405 | −12.60 to −7.056 | −12.86 to −7.451 | −8.341 to −1.247 | −13.53 to −7.814 |
| Rural, adjacent | 19.05*** | 19.05*** | 19.34*** | 19.23*** | 22.25*** | 19.10*** |
| Std. err. | (2.395) | (2.394) | (2.399) | (2.407) | (2.505) | (2.485) |
| 95% CI | 14.36-23.74 | 14.36-23.74 | 14.64-24.04 | 14.51-23.95 | 17.34-27.16 | 14.23-23.97 |
| Rural, not adjacent | 17.67*** | 17.75*** | 18.77*** | 18.79*** | 19.21*** | 20.34*** |
| Std. err. | (3.629) | (3.628) | (3.642) | (3.632) | (4.137) | (3.758) |
| 95% CI | 10.56-24.79 | 10.64-24.86 | 11.64-25.91 | 11.67-25.90 | 11.10-27.32 | 12.98-27.71 |
| Population Other race | ||||||
| Urban | −29.53*** | −28.62*** | −28.81*** | −29.10*** | −23.32*** | −21.06*** |
| Std. err. | (1.858) | (1.740) | (1.713) | (1.673) | (2.192) | (1.966) |
| 95% CI | −33.17 to −25.88 | −32.03 to −25.21 | −32.17 to −25.46 | −32.38 to −25.83 | −27.62 to −19.02 | −24.91 to −17.21 |
| Rural, adjacent | −0.108 | −0.0873 | 0.132 | 0.503 | −6.379 | −0.157 |
| Std. err. | (5.248) | (5.242) | (5.302) | (5.295) | (6.653) | (5.510) |
| 95% CI | −10.39 to 10.18 | −10.36 to 10.19 | −10.26 to 10.52 | −9.874 to 10.88 | −19.42 to 6.661 | −10.96 to 10.64 |
| Rural, not adjacent | 10.88** | 11.03** | 11.81** | 11.68** | 20.34*** | 12.55** |
| Std. err. | (4.981) | (4.996) | (5.243) | (5.269) | (4.841) | (5.519) |
| 95% CI | 1.116-20.64 | 1.239-20.82 | 1.531-22.08 | 1.351-22.00 | 10.85-29.83 | 1.732-23.37 |
| Population ≥ 65 years | ||||||
| Urban | −21.87*** | −22.50*** | −21.87*** | −22.89*** | −21.63*** | −22.10*** |
| Std. err. | (2.015) | (1.981) | (1.993) | (1.973) | (2.420) | (2.061) |
| 95% CI | −25.82 to −17.92 | −26.38 to −18.61 | −25.77 to −17.96 | −26.75 to −19.02 | −26.37 to −16.89 | −26.14 to −18.06 |
| Rural, adjacent | −35.06*** | −34.63*** | −34.80*** | −32.51*** | −27.72*** | −28.80*** |
| Std. err. | (2.815) | (2.817) | (2.824) | (2.797) | (3.448) | (2.824) |
| 95% CI | −40.58 to −29.54 | −40.16 to −29.11 | −40.33 to −29.26 | −37.99 to −27.03 | −34.48 to −20.97 | −34.34 to −23.27 |
| Rural, not adjacent | −37.10*** | −36.97*** | −36.98*** | −34.45*** | −35.71*** | −32.65*** |
| Std. err. | (3.335) | (3.337) | (3.343) | (3.299) | (4.050) | (3.423) |
| 95% CI | −43.64 to −30.57 | −43.51 to −30.43 | −43.53 to −30.42 | −40.92 to −27.99 | −43.65 to −27.77 | −39.35 to −25.94 |
| Population in poverty | ||||||
| Urban | 2.429 | |||||
| Std. err. | (1.536) | |||||
| 95% CI | −0.583 to 5.440 | |||||
| Rural, adjacent | 2.002 | |||||
| Std. err. | (1.953) | |||||
| 95% CI | −1.826 to 5.830 | |||||
| Rural, not adjacent | 8.693*** | |||||
| Std. err. | (2.489) | |||||
| 95% CI | 3.815-13.57 | |||||
| Median household income | ||||||
| Urban | −0.00974*** | |||||
| Std. err. | (0.000607) | |||||
| 95% CI | −0.0109 to −0.00855 | |||||
| Rural, adjacent | −0.00357*** | |||||
| Std. err. | (0.00106) | |||||
| 95% CI | −0.00564 to −0.00149 | |||||
| Rural, not adjacent | 0.000142 | |||||
| Std. err. | (0.00116) | |||||
| 95% CI | −0.00213 to 0.00241 | |||||
| Constant | 5654*** | 5567*** | 5579*** | 5546*** | 5528*** | 6096*** |
| (101.0) | (100.0) | (104.8) | (103.9) | (128.8) | (110.7) | |
| 5456-5852 | 5371-5763 | 5374-5785 | 5342-5749 | 5275-5780 | 5879-6313 | |
| 67 504 | 67 504 | 67 504 | 67 504 | 52 794 | 64 719 | |
| 0.874 | 0.874 | 0.875 | 0.874 | 0.888 | 0.878 | |
Note. Robust standard errors in parentheses.
P < .01. **P < .05. *P < .1.
Acknowledgements
The authors thank Deepak Adhikari for preparing the analytic dataset used in this study.
Ethical Considerations
This study analyzed secondary, de-identified, publicly available data from the Area Health Resource File (AHRF), CDC WONDER mortality data, and USDA Rural–Urban Continuum Codes. As such, this research was exempt from institutional review board oversight. Ethical approval was not required.
Consent to Participate
Not applicable. No human subjects were directly involved, and all data were de-identified and publicly available.
Author Contributions
Nasim Ferdows, PhD: Conceptualization, study design, data analysis, interpretation, drafting of the manuscript, and final approval. Momotazur Rahman, PhD: Conceptualization, study design, supervision of data analysis, interpretation, and critical revisions of the manuscript. Cyrus Kosar, PhD: Interpretation of results and manuscript revisions. Orestis Panagiotou, MD, PhD: Interpretation of results and manuscript revisions. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the U.S. National Institute on Aging under grant numbers T32 HS-000011 and 1R21AG053712-01A1. The funder had no role in study design, data analysis, interpretation of results, or manuscript preparation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data used in this study are publicly available. Mortality data are available from the CDC WONDER database (https://wonder.cdc.gov/). Physician supply, per-capita income, and post-acute care supply were obtained from the Area Health Resource File (https://data.hrsa.gov/topics/health-workforce/ahrf). Rural–Urban Continuum Codes (RUCC) are available from the USDA Economic Research Service (![]() ).
).