
Abstract
Excessive salt consumption has remained a critical public health issue in Malaysia where the average daily consumption has far exceeded the recommended limit by the World Health Organization (WHO). Driven by the cultural dietary patterns and limited public knowledge, it poses a significant challenge to attitudes, beliefs, and self-reported salt intake practices among Malaysian adults. This nationwide cross-sectional study was conducted from August to November 2023 using a multistage random sampling method.The study employed the validated MySalt Literacy instrument, designed to suit Malaysia’s multicultural context and comprising domains on knowledge, beliefs, attitudes, practices, and salt intake among adults aged 18 years and older. A total of 4400 respondents participated in the study, with the majority being female (64.7%) and the remainder male (35.3%). Most respondents had attained tertiary education (54.2%) and resided in rural or semi-rural areas (55.7%). The study findings revealed only 30.9% of respondents correctly identified the recommended daily limit for salt intake, and 65.7% were unaware of the relationship between salt and sodium. In terms of behavioural practices, only 15.6% respondents reported actively limiting their daily salt intake, while merely 13.9% consistently paid attention to labels indicating “no salt added,” “low,” or “reduced sodium” when purchasing food. Further analysis indicated a significant correlation between attitudes, beliefs, and label-reading practices with salt intake behaviour. This study reveals that Malaysian adults are generally aware of the health risks due to excessive salt intake and express positive attitudes towards salt reduction, however significant knowledge gaps and cultural barriers impedes the progress. Thus, efforts to reduce salt intake must go beyond raising awareness by addressing cultural beliefs, taste preferences and behavioural habits. Effective interventions should incorporate culturally tailored strategies and relatable messages that consider taste preferences and behavioural norms. A coordinated, multi sectoral approach involving health promotion, nutrition education (including label-reading skills), and food policy reforms such as front of pack labelling and mandatory reformulation is essential for sustainable, population wide salt reduction.
Introduction
In recent decades, there has been a significant shift in global dietary patterns, largely influenced by increased consumption of processed foods, urbanization, and changing lifestyles. 1 The accessibility and affordability of highly processed foods containing high levels of sodium, fat, and sugar leads to significant impact on population health. 2 The Global Burden of Disease (2019) estimated that there were over 1.8 million deaths and 44 million loss of disability-adjusted life years (DALY), including 40.5 million DALYs from cardiovascular disease (CVD) and stroke due to excess sodium consumption. 3
Meanwhile, salt intake studies among the worldwide population reveal average daily salt consumption surpasses the recommended levels with adults estimated to consume approximately 4000 mg of sodium per day (equivalent to 10 g of salt), with greater consumption observed in Asia compared to other regions. 4 This trend is mirrored in Malaysia where findings from the Malaysian Community Salt Survey 2017-2018 (MyCoSS) reported Malaysians are consuming an average of 7.9 g (1.6 teaspoons) salt or 3167 mg sodium per day which exceeds the recommended intake. 5
High salt consumption has been linked to obesity where the National Health and Morbidity Survey 2023 (NHMS) has reported that the obesity rate has increased from 19.7% in 2019 to 21.8% in 2023. Previous study shows that being overweight is significantly associated to higher non-communicable diseases (NCD) such as diabetes and hypertension. 6 The Ministry of Health, Malaysia (MOH) has also identified obesity as the key component of the rising NCD burden which places significant strain on the healthcare system in Malaysia 7
The World Health Organisation (WHO) has set a global target as part of its strategy to combat premature mortality from NCDs aiming to reduce the population salt intake by 30% in 2025. 8 Aligned with the global goal, Malaysia has also launched its Salt Reduction Strategy to Prevent and Control NCD (2021-2025) which focuses on 3 pillars known as MAP strategy which are Monitoring, Awareness, and Product reformulation. 9 Additionally, the MOH is working to introduce the mandatory sodium limits through amendments of the Food Act 1983, reinforcing Malaysians to commit towards achieving the WHO sodium reduction target. 10
However, it is vital to assess the knowledge, behaviour related to salt intake, and the sources of the dietary sodium to reduce the salt intake with effective interventions that could result in impactful outcomes. 11 Currently, information is scarce regarding the salt literacy of the Malaysian population, particularly concerning knowledge, attitudes, beliefs, and practices regarding sodium-related label reading. The understanding of this gap is critical as it directly affects salt intake behaviour and there is a pressing need for comprehensive data to inform and advocate for effective public health interventions.
This paper explores the knowledge, attitudes, beliefs, and key predictors influencing salt intake practices among Malaysian adults. The insights gained aim to support stakeholders and policymakers in addressing information gaps and behavioural barriers related to salt consumption. Strengthening these efforts can enhance sodium reduction initiatives and contribute to lowering the national burden of non-communicable diseases.
Methodology
This nationwide cross-sectional study was conducted by using multistage random sampling from August to November 2023 involving Malaysian adults aged 18 years and above. The sample size was calculated using the prevalence of mean score from the original paper whereby this instrument was adopted. 12 After accounting for a 20% loss to follow-up, the final sample size was determined as 4400 respondents. The sampling process was conducted in several stages where it started by systematically selecting of districts across all states stratified by rural and urban classifications. The final stage involved random selection of the residential areas and living quarters (LQs), enhancing the representativeness across population in Malaysia.
After the identification of the LQs was made, trained research assistants were deployed to brief and distribute the self-administered questionnaire to the respondents that met the inclusion criteria, which are Malaysians aged 18 and above, able to read and understand Malay or English language, and consented to participate in the study. The subject’s privacy and the confidentiality of the data collected were preserved, as it were gathered anonymously and without any identifiable information.
Study Instrument
The instrument implemented for this study was initially developed to assess health literacy pertaining to salt intake among the Hong Kong population. 12 This instrument was adapted and validated to fit the multicultural population in Malaysia with modifications conducted for culturally specific items such as common types of food consumed by local people and nutrition label reading questions whereby food label designs food label designs were developed in accordance with local food labelling guidelines. The adapted instrument shows good internal consistency with Cronbach’s alpha value ranging from .624 to .818, and the intraclass correlation coefficient (ICC) obtained was .522 (95% CI, 0.423-0.611). The adapted and validated instrument comprised of 52 items with scores ranging from 0 to 104 and renamed as renamed as MySalt Literacy. 13
Domains in the Instrument
The domains of the instrument were developed based on key elements of health literacy relevant to salt intake, as identified in previous studies. These include functional literacy, factual and procedural knowledge, awareness of salt consumption, and the ability to read and interpret nutrition labels. 12
Knowledge
The knowledge component assessed respondents’ knowledge of salt content in different food items based on the portion, knowledge about the effect of high salt intake on health conditions, awareness on differences between sodium and salt, and recommended daily limit for salt intake by WHO. For each correct answer, the highest score given was 2, followed by a score 1 for a probable correct answer and a score 0 was given for the wrong answer.
Perceptual Beliefs & Attitudes on Salt Intake
For the section on a perceptual belief regarding salt, respondents were asked to choose their agreement on the statements provided such as perception on salt as an important taste enhancer, whether flavour enhancer can be used to replace salt, salt content in outside food, and whether Rock salt, Kosher or Himalaya salt contains less sodium. The attitude towards salt intake assessed respondents’ agreement on statements pertaining to effect of salt on health, the importance of adding salt to food, the importance of controlling salt intake for disease prevention, and confidence in limiting daily salt intake. Similarly, for each correct answer that depicts a positive attitude and belief towards salt reduction, the highest score given was 2, followed by a score of 1 for a probable correct answer, and a score of 0 was given for the wrong answer.
Salt Intake Practices
In this section, respondents were assessed on behaviours related to salt intake in a week, for example, efforts taken to reduce salt, adding salt at the table, consumption of fast food, fermented or pickled food, and whether efforts were taken to minimize daily salt intake. Practices were assessed based on the self-reported frequency of behaviours over a 1-week period, categorized as: Always (daily), Often (4-6 times per week), Sometimes (2-3 times per week), Rarely (fewer than 2 times per week), and Never (0 times). Scores were given based on the frequency of practices within a week. For good practices on salt reduction, example; minimize salt intake in a week, for those reporting practicing it always, and often were given 2 marks, whereas those who reported sometimes, were given 1 mark and for those who reported rarely and never, they were given 0 marks. Whereas for negative practices, reverse scoring was given. For an example, consumption of canned food or processed food, those reported practicing it always and often were given 0 marks, whereas those reported sometimes, given 1 mark and for those reported rarely and never, they were given 2 marks.
Salt Related Label Reading Practices
Under this section respondents were assessed on the frequency of practices associated with salt related label reading practices; in terms of paying attention to low salt labelled food products, reading sodium content in nutrition information label and practise of purchasing food with low salt content. For those who’ve answered always, 2 marks were given, whereas those who reported sometimes, were given 1 mark and for those who reported never, they were given 0 marks.
Statistical Analysis
SPSS version 29 (IBM Corp., Armonk, New York, USA) was used to analyse the data in achieving the objectives of the study. The descriptive analysis was carried out to examine the sociodemographic properties, the general knowledge of salt consumption, the attitude about salt intake, the perceptual beliefs about salt intake, the label reading practice, and the salty food consumption of the respondent. The data were presented in a table with both the frequency and percentages tabulated.
The categorization of levels in each domain was determined by referencing another paper that similarly assessed the knowledge, attitude, perception, and practice towards salt intake whereby if participants answered less than 50% of the questions accurately, they were considered to have a limited level of knowledge, attitude, or practice. If they answered between 50% and 75% accurately, they were classified as having a fair level of knowledge, attitude, or practice. If they answered more than 75% of the questions accurately, they were considered to have a high level of knowledge, positive attitude, or good practice. 14
The multiple logistic regression analysis was further carried out to find the predicting factors of salty food consumption. A significance level with P-value less than .05 was chosen to show variables with a significance effect on the dependent variable (salty food consumption). The odds ratio was tabulated in the same table and further explained to examine the strength of the predicting variables towards the model.
Result
Sociodemographic Background of the Respondent (n = 4400)
As shown in Table 1, the respondents were mostly females (2846; 64.7%), aged 20 to 25 (1496; 34.0%), and slightly more than half resides in rural or semi-rural areas (2452; 55.7%). Most respondents also possessed a tertiary level of education (2383; 54.2%) whereby only 0.4% (17) of them did not possess any formal education. The household income of the respondents was classified into lower, middle- and higher-income groups based on their position within the income distribution percentile of the population which refers to the Department of Statistics Malaysia (DOSM), 2022 classification. Most of the respondents (3409; 77.5%) were from the lower income group whereby they were among the primary group for assessment in this study as national health data shows higher prevalence of Non-Communicable Diseases (NCDs) were reported among lower income group. 15 In terms of self-reported Body Mass Index (BMI) status, nearly half of the respondents were in the normal range of BMI (2067; 47.0%). About 10% of the respondents reported an existing illness with hypertension (267; 6.1%) as being the most frequently reported health problem among this section of respondents.
Sociodemographic Background (n = 4400).

General Knowledge on Salt
The general knowledge on salt consumption assessed respondent’s awareness on differences between salt and sodium, knowledge on recommended level for daily salt intake by international health regulatory bodies, knowledge on diseases related to high salt consumption, and knowledge on the amount of salt in food.
Table 2 shows awareness among respondents on differences between salt and sodium, whereby only 34.3% (1509) of the respondents are aware that salt contains sodium instead of the other way around. Meanwhile, 34.2% (1505) of the respondents did not know the relationship between salt and sodium.
Relationship Between Salt and Sodium.

Table 3 shows most of the respondents were still unaware of the recommended level for daily salt intake by World Health Organization (WHO; 2500; 56.8%) and the amount of salt in 1 teaspoon (2243; 51.0%).
Knowledge on Recommended Level for Daily Salt Intake.

Table 4 presents respondents’ knowledge of diseases associated with high salt consumption. While most were aware of the links of high salt intake with hypertension, cardiovascular diseases (including heart disease and stroke), kidney disease, and obesity, however over half of them were unaware that conditions such as osteoporosis, stomach cancer, and asthma are also related to excessive salt intake.
Knowledge of Disease Related to High Salt Consumption.

Table 5 presents findings related to knowledge on salt content in common food products whereby most respondents were aware of the high salt content of food products sold in the market. Most respondents are aware in regards to type of food with lower salt content, for example: white rice, papaya, green tea. However, more than half of the respondents (2350, 53.4%) answered wrongly and unaware of the hidden salt content in certain commonly consumed food such as bread.
Knowledge on Salt Content in Different Types of Food.

Attitude on Salt Intake
In general, assessment on attitude towards salt intake (Table 6) shows more than half of the respondents depicts a positive attitude towards importance of salt reduction. Most of the respondents, 75.6% (3326) agreed on being worried about serious health problems due to intake of high salt content food and 52.7% (2319) agreed being concerned for salt content in foods they consume. Even though 66.7% (2933) of the respondents agreed on limiting the amount of salt intake is important to health, however only 43.3% (1906) agreed being confident to control their daily salt intake with 33.7% agreed to the feeling being pressured to practice healthy eating.
Attitudes on Salt Intake.

Perceptual Beliefs About Salt Intake
Table 7 presents respondents’ perceptual beliefs regarding salt intake, revealing several concerning misconceptions that may influence unhealthy dietary behaviours. Majority of respondents 72.9% (3207) agreed food taste can be enhanced by adding salt and sauces while cooking, indicating strong reliability towards salt intake to ensure taste and food palatability. Around 43.0% (1890) believed that salt intake can be neutralized by drinking more water whereas 40.2% (1769) agreed certain types of salt (Rock, Kosher, Himalaya Salt) contain less sodium than normal salt and believe these are healthier salt options.
Perceptual Beliefs About Salt Intake.

Salt Related Label Reading Practice
Table 8 presents salt-related label reading practices among respondents prior to purchasing food products. Only 13.9% (n = 611) reported always checking for labels such as “No Added Salt” or “Low/Reduced Sodium,” while 48.9% (n = 2153) did so occasionally, and 37.2% (n = 1636) reported never. Similarly, 45.7% (n = 2011) occasionally read the sodium content on food labels, whereas 42.7% never did. When it came to purchasing low-salt food products, only 10.6% (n = 465) reported doing so consistently, 46.5% (n = 2046) occasionally, and 42.9% (n = 1889) reported never.
Food Label Reading Practices.

Salt Intake Practices
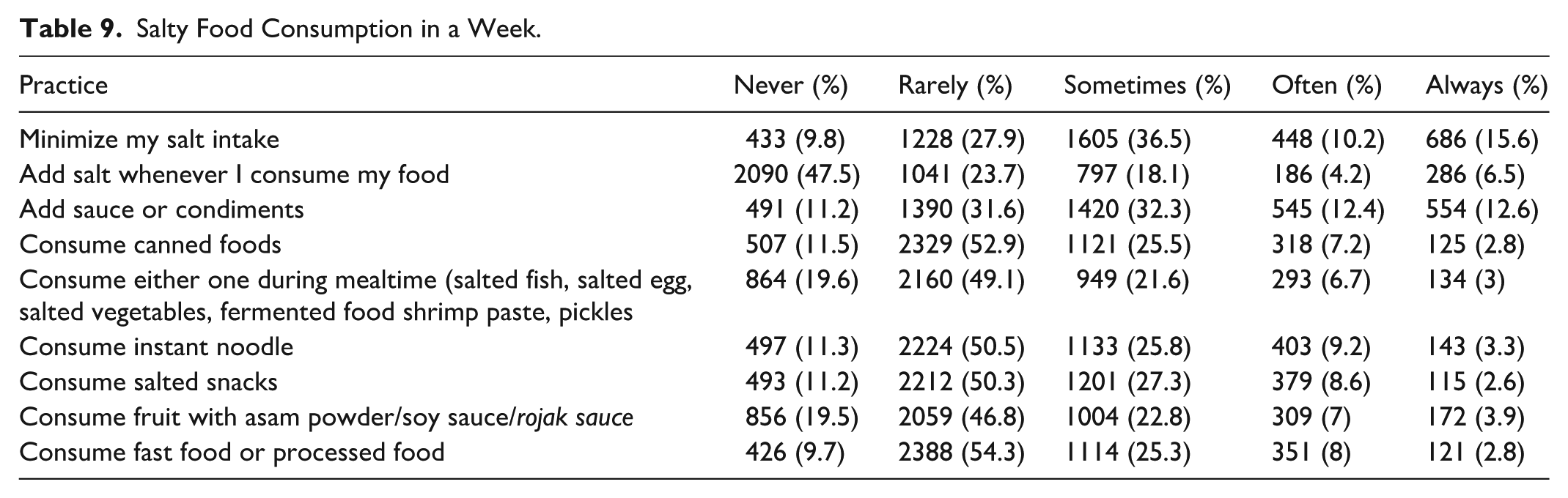
Table 9 presents the salt intake practices of the respondents. Overall, the majority reported making a conscious effort to reduce their salt consumption. Nearly half (47.5%, n = 2090) stated they never add salt at the table, while 75.1% (n = 3301) reported either never, rarely, or only occasionally adding sauces or condiments during food preparation or before eating. Regarding processed or canned food consumption, 52.9% (n = 2329) indicated they rarely consume such items. Similarly, foods commonly eaten in Malaysia such as salted fish, pickled vegetables, and other fermented items were reportedly consumed rarely by 49.1% (n = 2160) of respondents. In addition, 54.3% (n = 2388) reported rarely consuming fast food on a weekly basis.
Salty Food Consumption in a Week.
Association of Salt Intake Practices with Knowledge, Attitude, Beliefs, and Label Reading Pertaining to Salt
Table 10 presents the association of salt intake practices with knowledge, attitude, beliefs, and salt related label reading behaviour. Multivariate analysis showed that there are 3 predicting factors related to salty food consumption which are attitudes, perceptual beliefs, and salt related label reading behaviour. The odds ratio results showed attitude, perceptual beliefs, and label reading practice about salt increase by 2.259, 1.521, and 1.463 times respectively to salt intake practices.
Association with Salty Food Consumption.
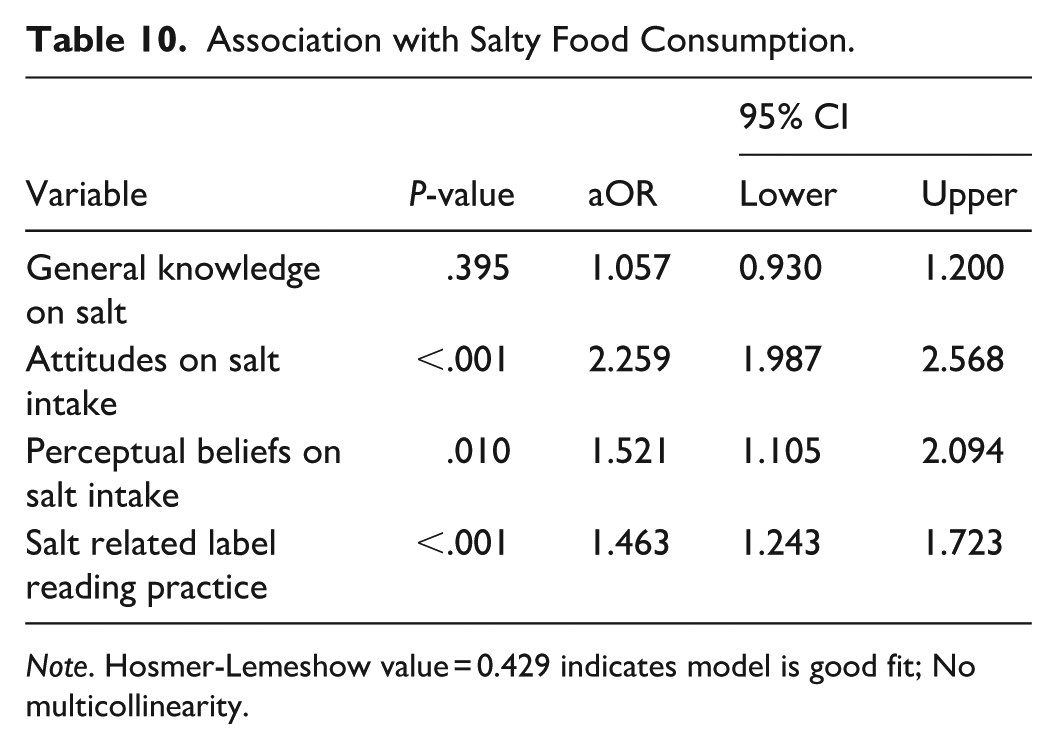
Note. Hosmer-Lemeshow value = 0.429 indicates model is good fit; No multicollinearity.
Discussion
This study explored Malaysian adult’s knowledge, attitudes, beliefs, and practices related to salt consumption. Understanding these dimensions is vital, as they directly influence dietary behaviours and long-term health outcomes. Study findings show nearly 70% of participants were unable to correctly associate salt with sodium, a finding consistent with studies from New Zealand and UAE.16,17 This fundamental knowledge gap may contribute to poor dietary decisions, particularly regarding processed foods where sodium is often hidden. 18 Although most respondents recognized the prominent health risks of excessive salt intake such as hypertension and cardiovascular diseases, fewer were aware of its links to the less commonly discussed health conditions like osteoporosis, asthma, gastric, cancer, consistent with findings reported in Costa Rica. 19
A significant proportion of respondents were also unaware of the WHO recommended daily salt intake level, reflecting previous Malaysian findings. 5 While participants could generally identify high salt foods like processed and fermented food products, many overlooked staple items such as bread, which contribute substantially to daily sodium intake. Therefore, it can be deduced that although respondents were generally able to identify foods typically associated with high salt content, they were unaware of the presence of hidden salt in commonly consumed items that lack a perceptibly salty taste. Similar gaps in awareness have been noted in Turkey and other countries, where salt content in staple foods is under recognized.20,21 Unlike salt, the taste of sugar is more readily detectable, enabling consumers to detect sweetness and make immediate adjustments to their intake. Whereas salt is often embedded in recipes and ready-made foods; cereals, sauces, and processed meats that may not taste salty making it difficult for individuals to monitor their intake. Thus, reformulating commonly consumed products has shown to be an effective population level strategy to reduce sodium consumption. 22
In terms of perceptions, many participants believed that low salt food lacks flavour and it’s necessary for salt or flavour enhancers to be added for palatable meals. This perception underscores the cultural significance of salt in Malaysian cuisine, where traditional cooking methods commonly incorporate salt for flavour enhancement, food preservation, and marination. Dishes such as soy-based gravies, salted fish, pickled vegetables, and fermented products are dietary staples and similar cultural based dietary choices are observed across other Asian populations, where salt is deeply embedded in traditional cooking practices.23 -25 Additionally, the study uncovered several common misconceptions, including the belief that drinking more water can neutralize salt intake, and that Himalaya, Kosher, or Rock salts are healthier alternatives to regular table salt and these findings were parallel to similar studies conducted in Singapore and other high income countries,24,25 emphasizing the need for targeted education to address inaccurate assumptions. Thus, to improve intervention outcomes, it is essential to move beyond general awareness campaigns and consider nuanced change to traditional food practices and flavour preferences. Context specific strategies, such as the Communication for Behavioural Impact – Salt Reduction (COMBI-SR) intervention implemented among culturally diverse community with high rates of hypertension demonstrated effectiveness. The intervention addressed key barriers of socioeconomic constraints in accessing healthier salt alternatives and deeply rooted cultural dietary habits. This was achieved by reformulating familiar dishes, engaging local stakeholders, and delivering health messages aligned with cultural norms. 26 Similarly, study among individuals of African descent in the UK highlighted the absence of culturally tailored messaging and the limited availability of low-salt options hindered salt-reduction efforts, further emphasizing the importance of culturally grounded approaches. 27
This study also found many respondents expressed concern about health risks associated with excessive salt intake and were generally supportive towards efforts to reduce salt consumption. However, this was accompanied by negative perceptions of low sodium diets, particularly in terms of taste. This ambivalence reflects patterns observed in both local and international studies, whereby willingness to reduce salt often coexists with dissatisfaction towards the blandness often associated with reduced-salt foods.28,29
In terms of practices, although most respondents reported avoiding added salt at the table, many still regularly used high-sodium sauces and condiments during cooking. This suggests an incomplete understanding of where most of the dietary salt comes from. 30 While consumption of canned and processed foods was relatively low, traditional high-sodium items such as salted fish and fermented vegetables were consumed weekly, reflecting strong cultural dietary patterns across Asia.31,32 Similarly, in countries like Brazil, India, and China, discretionary salt use and condiments account for over half of total sodium intake.33,34 These findings suggest that a lack of confidence in managing salt intake, limited awareness of sodium content in commonly consumed foods, and the perceived difficulty of making dietary changes represent key psychological and behavioural barriers that are consistent with broader literature on health behaviour change.35,36
This study also revealed limited engagement in salt related label reading, with approximately half of the respondents rarely checking sodium content. Barriers included small font size, time constraints, and limited nutritional literacy. Similar challenges have been reported in Brazil and China,37 -40 underscoring the need for clearer labelling and targeted public education to support informed decision making.
In addition, the study examined predictors of salt related behaviour, identifying key factors that influence individuals’ dietary choices and salt intake. Attitudes, beliefs and salt related label reading behaviour were significantly associated with salt reducing practices, aligning with findings from a study among healthy and hypertensive Turkish adults, which reported lower salt intake was linked to greater health awareness, motivation driven by health considerations, and regular use of nutrition labels. 41 While beliefs about disease risk and perceived health benefits encourage dietary change, however perceived barriers like taste and cultural norms, low self-efficacy, fatalistic attitudes, negative outcome expectations often hinder the translation of intention into sustained behaviour. 20
Notably, knowledge alone did not significantly predict salt reduction behaviours aligning evidence from India and Malaysia, where awareness of health risks did not necessarily lead to behaviour change.15,42 While some studies report positive effects of knowledge on food choices, 41 broader reviews suggest knowledge is insufficient on its own to shift dietary behaviours at the population level.43,44 These studies underscore the importance of addressing not only knowledge gaps but also deeply held beliefs and perceived barriers when designing effective salt reduction interventions. These studies underscore the importance of addressing not only knowledge gaps but also deeply held beliefs and perceived barriers when designing effective salt-reduction interventions. The findings emphasize the need for behaviour change strategies that go beyond knowledge provision by addressing cognitive and emotional barriers, while also considering critical sociocultural, economic, and environmental influences in the design of future salt-reduction interventions.
Limitations
The reliance on self-reported questionnaires introduces potential recall bias, particularly in capturing detailed dietary intake and salt-related behaviours, thereby limiting the accuracy of estimated salt consumption. In addition, while this study examined individuals’ knowledge of salt intake, it did not investigate how this knowledge was acquired. This represents a significant limitation, as understanding the sources of information such as media, educational institutions, or healthcare providers is crucial for designing targeted and effective public health interventions. Future research should explore these knowledge pathways, as addressing misinformation, especially on social media, or stemming from cultural beliefs, requires context-specific and platform-sensitive communication strategies.
Conclusion
This study offers valuable insights into the knowledge, attitudes, beliefs, and practices towards salt consumption among Malaysian adults. While there is general awareness of the health risks associated with excessive salt intake and positive attitude towards reduction efforts, significant gaps persist in the public’s understanding, particularly regarding hidden sources of sodium, recommended intake levels, and the broader health consequences of high salt consumption. Although most respondents’ express willingness to reduce their salt intake, cultural preferences for salty flavours, traditional cooking methods, and prevailing misconceptions about healthier salts alternatives, such as Himalayan or rock salt, continue to pose barriers. These beliefs, often passed down through generations or reinforced by marketing, can undermine behaviour change.
Therefore, efforts to reduce dietary salt intake must go beyond knowledge dissemination and address deep-rooted cultural beliefs and taste preferences. Future interventions must be culturally tailored, incorporating community engagement, culturally relevant messaging, and local food practices. Integrating behaviour change strategies with respect for cultural norms will be essential in translating awareness into sustainable dietary improvements. Multi-sectoral strategies combining health promotion, behavioural insights, and food policy reforms are crucial to shift both perception and practice towards healthier salt consumption. Health communication campaigns should be tailored to local cultural contexts and emphasize practical alternatives. Educational interventions must go beyond awareness by equipping individuals with the skills to read and interpret nutrition labels effectively, empowering informed food choices. In parallel, regulatory approaches such as front-of-pack labelling, mandatory food reformulation, and locally driven community programmes are essential to support sustainable, population-wide shifts in salt-related behaviours.
Footnotes
Acknowledgements
The authors would like to extend heartfelt appreciation to the Director General of Health Malaysia for his permission to publish this paper and the National Institutes of Health, Ministry of Health Malaysia for funding this research project. We would like to extend our gratitude as well to the original author of the Chinese Health Literacy Scale for Low Salt Consumption, Dr. Patsy Chau (School of Nursing, The University of Hong Kong) forgranting the permission to use the tool, Dr. Shubash Shander Ganapathy (Institut for Public Health, Ministry of Health Malaysia) and other expert panel members who had provided valuable comments to the development of the adapted instrument, research team members, and all participants who had participated in this study.
ORCID iDs
Ethical Considerations
The study was registered under National Medical Research Register, Ministry of Health Malaysia and was approved by Medical Research and Ethics Committee (MREC) Ministry of Health Malaysia (NMRR ID-22-00689-JLC).
Consent to Participant
The research team also obtained written consent from participants via informed consent form prior to data collection.
Authors Contributions
KP, AAA, HM, TSMY, MK, MA, and MZJ participated in study design and data collection. KP, AAA, MK involved in data analysis. KP, AAA drafted the initial manuscript with significant contribution from TSMY, MA, MZJ & MK. All authors had participated, read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research and publication of this article was funded by the Ministry of Health Malaysia via the National Institutes of Health Malaysia research grant under the research registration number NMRR ID-22-00689-JLC. The funder is also a stakeholder of the study but did not participate in the study process.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data set is available from the corresponding author upon reasonable request.