
Abstract
Planning for end-of-life and associated decision-making is one of global significance as it impacts the quality of care in palliative care settings, including ensuring that personal preferences are honoured. It is a priority for the Australian health system to use Advance Care Planning (ACP) as it is an effective tool for individuals and their families to make their personal preferences known and implemented. The aim of this project was to evaluate the longer-term impact of the Palliative Care Western Australia (PCWA) ACP workshops. Semi-structured, open-ended questions were used to collect data from 21 participants. Reflexive thematic analysis was used to analyse the data. Three themes emerged: (1) Finding the words, (2) Finding the people and (3) Finding the way. The workshops enabled individuals to complete their Advance Health Directives (AHD) correctly, substitute decision-makers to gain confidence in enacting the AHD for their loved ones, and healthcare professionals to provide seamless, person-centred care.
Introduction
The importance of planning for the end-of-life (EOL) and associated decision-making is one of national 1 ) and international. 2 It is clear from previous research that planning for care and specifically aiding decision-making near the EOL has a significant impact on the quality-of-care provision, including ensuring that personal preferences are honoured.3,4 It is a priority therefore for the Australian health system that Advance Care Planning (ACP) be used as an effective tool for individuals and their families to have their personal choices and preferences known and implemented. 5
Palliative Care Western Australia (PCWA) has led the way in educating Western Australians from all backgrounds in understanding ACP and supporting individuals and carers to document those plans appropriately. PCWA is a not-for-profit peak body in Western Australia (WA) representing palliative care providers and professionals whose aim is quality of life for all. This is achieved by raising awareness and understanding of palliative care in the community and improving access to palliative care services. Secondly, it encourages, recognises, and rewards excellence in palliative care delivery, and thirdly, acts as the bridge between the government and the palliative care sector. 6 The major focus of the community education strategy over the last 10 years has been on delivering free interactive community workshops throughout metropolitan and regional WA. ACP workshops were promoted through the Local Government Authorities and newspapers. The workshop agenda included what was involved in ACP, exploring individual’s priorities for EOL, having EOL conversations, what palliative care was all about and how to complete the Advance Health Directive (AHD) and Enduring Power of Guardianship (EPG). Workshop participants were offered the ACP resource pack, the same could also be accessed online. Following 2 h of face-to-face group interactive meetings facilitated by a qualified workshop facilitator, participants were offered (and many took the offer) a 1-h, one-on-one follow-up visit by PCWA ACP dedicated Counsellors to assist with accurately completing the AHD document. Previous evaluations of the ACP workshops have shown the powerful impact of these sessions. They have revealed statistically significant rates of improvement in understanding ACPs and completion of ACP documentation. 7 Furthermore, there are many satisfied participants who have found the workshops invaluable, and there is a growing demand for participating in the PCWA ACP workshops (Workshops). 8
It is known that patients and carers gain knowledge and understanding from the workshops. 8 Many, if not most participants, translate that knowledge into formal ACP documentation which occurs up to several months after attending a workshop. 7 The question which remains is that: with the documents completed, utilising the support of workshops and Counsellors, and with confidence built in EOL decision-making and advocacy, what happens when the time comes to enact the ACPs?
The Australian Institute of Health and Welfare (AIHW) estimates that nearly half (47%) of Australians live with chronic conditions. Four out of every 5 persons aged over 65 have 1 or more chronic conditions and 20% of the total Australian population live with 2 or more chronic diseases. 9 Furthermore, 70% of all Australians say they wish to die at home, yet less than 15% of all deaths in Australia occur at home. 10 For those wanting to die at home or to have their wishes respected in hospital, hospice, or residential aged care, the AHD is the most secure way to guide their care according to personal preferences. The workshops are aimed at creating awareness and empowering individuals to make their EOL care preferences and decisions known and documented. Additionally, they encourage the dissemination of this information, not only to loved ones, but also to health professionals and carers so they can be cared for according to their wishes. This is the longer-term impact of the workshops on participants’ lives going forward.
Evaluation Question
What is the longer-term impact of Palliative Care WA Advance Care Planning Workshops?
Methods
This qualitative evaluation of the longer-term impact of the PCWA ACP workshops was conducted in Western Australia from April to October 2024. In this study, longer-term is defined as how information gained from workshops impacted participants’ lives going forward. The study followed the appropriate EQUATOR guidelines 11 designed for qualitative inquiries.
Ethics Approval
This study received approval from an Institutional Human Research Ethics Committee in April 2024.
Sampling
To evaluate the longer-term impact, potential participants were emailed from the list of attendees at the workshops between 2018 and 2024. PCWA contacted attendees with information about the study, inviting potential participants to contact the evaluation team directly. Information about the study was also published in the regular PCWA e-newsletter with contact information for the research team. From the responses, we recruited the following 3 groups:
a. Individuals who attended the workshop/s for personal benefit.
b. Family members or significant others who enacted an AHD on behalf of a loved one.
c. Healthcare professionals who attended a workshop and had also cared for patients and/or family members with and without an AHD.
Data Collection
Qualitative telephone and online interviews were undertaken by a female professor (DP), experienced qualitative research and 2 female PhD candidates (GP and EG). Each interview took between 15 and 30 min. Interviews conducted online were transcribed by Microsoft Teams and then corrected by the interviewer. Each participant attended the interview un-accompanied. Telephone interviews were audio recorded and transcribed verbatim using NVivo software. Three telephone interviews were not audio recorded, and the interviewer made detailed field notes during and after the interview. Some participants also provided written information which was included as data. Basic demographic information was gathered for all 3 participant groups during the interview. All data were entered and managed using NVivo software. Participants’ interview questions were arranged according to each group; individuals, family/substitute decision-makers, and healthcare professionals.
For individual participants attending the workshops for personal benefit, the interview topics included:
General impressions of the workshop and its usefulness and adequacy in preparing for EOL decision-making and care.
The feeling of confidence to put the concepts and knowledge gained into practice.
For family members/substitute decision-makers the topics included:
Telling the story of using ACP as part of the care of the family member.
Helpfulness of attending the workshop in making decisions on behalf of a family member.
Confidence in enacting the ACP as a substitute decision-maker.
What would or could be done differently if given another opportunity to make decisions on behalf of someone?
For healthcare professionals and care staff associated with EOL care the topics included:
Describing the care of the person with the ACP.
Experience of caring for someone who had documented/ made known their decisions, preferences and values (compared with those who did not).
The interview guides were pilot tested on the first 3 participants, one from each category and reviewed and did not require modification. Data saturation 12 was reached after conducting 16 interviews. Nevertheless, 5 additional interviews were conducted to ensure clarity of the themes.
Data Analysis
Two types of analysis were planned. The first line of analysis took a conventional approach to the coding and analysis of the interviews, permitting the identification of concepts and themes across all participants. Each transcript was coded by 2 team members before discussing and reaching consensus at regular 4-member team DP, GP, EG and PB (a male Masters student) meetings. A reflexive thematic approach to the analysis was used, as described by Braun and Clarke.13,14
In the second line of analysis, we aimed to create case studies to assess the longer-term impact of AHDs and the experience of their influence during episodes of care towards the EOL for all involved, including the substitute decision-maker, various family members and connected health professionals and carers. It was hoped this would provide a unique view of how the longer-term outcomes of the workshops had developed. However, despite referrals from substitute decision-makers to the General Practitioners (GPs) who had provided care at the EOL, no GPs returned the phone call or email invitations. The reason for non-response is not known. With the data collected, the second analysis approach was adjusted to reconstruct the impact stories from 2 perspectives: the substitute decision-maker, and the health professional.
Both types of analysis followed a rigorous process to minimise bias and ensure all voices were heard from the data. Following the transcription and cleaning, each interview transcript was read by all members of the evaluation team. Line-by-line coding was conducted for each transcript by 2 team members and then discussed at the regular team meetings. Identification of clusters of codes and development of themes was achieved through discussion at meetings.
Recruitment
Invitations to participate in the workshop evaluation were sent by PCWA to former attendees of the workshops. A total of 1256 emails were sent with 52 bounce-backs. Sixty individuals called by phone, 2 responders agreed to participate, and they were asked to contact the evaluation team, 30 of these individuals either declined or had a phone number that was no longer in service. A voicemail and/or text message was left for the remaining 28. Invitations were also included in 3 mail-outs to the PCWA e-news list of 1336 people with 6 bounce-backs. Would-be participants were advised to contact the evaluation team directly to express their interest. Following PCWA’s invitation, 57 potential participants contacted the evaluation team. Information and consent forms were sent to the 57 by email and post. Twenty-one signed consents were received, 3 decided not to participate after reading the information letter, and 26 did not respond. Figure 1 demonstrates the distribution of responses and Figure 2 provides the description of participants.

Response to invitation.
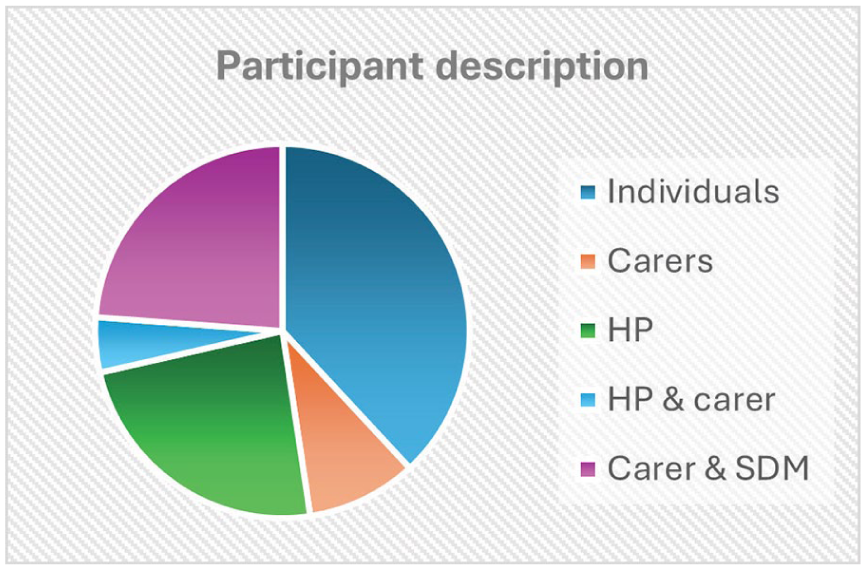
Participant description.
Table 1 further illustrates the limited information we took on participants’ background information.
Participant Profiles.

Note. I = individual; HP = health professional; C = carer; SDM = substitute decision-maker.
Individuals who attended the workshop/s for personal benefit and significant others who cared or enacted an AHD on behalf of a loved one, were generally older compared to healthcare professionals. Only 1 participant was from culturally and linguistically diverse (CaLD) background.
Findings
Previous evaluations of the workshops found that workshops were beneficial in assisting individuals to document their EOL preferences in the immediate and medium term. This current evaluation focused on the longer-term impact of the workshops. Although the workshops have been conducted for over a decade, there was still an element of needing information about ACP. Some themes cut across all 3 participant groups. These themes related to the need for information and the significance of attending a workshop. The themes identified were: (1) Finding words, (2) Finding people and (3) Finding the way.
Themes
Finding the Words
Individuals
The first theme that emerged came from all participant groups who had attended an ACP workshop. Individuals, substitute decision-makers and healthcare professionals found it difficult to talk about issues related to ACP and preparing an AHD. Finding the words to convey their preferences within the AHD was a challenge to individuals as they prepared their documentation. They often found that the words they used to indicate their preferences when completing the AHD were insufficient. Finding the words to start conversations with family and the GP was something the workshop was beneficial for. Before attending the workshop, participants were unaware of what words to use in ACP conversations, they just didn’t know how to talk about what they wanted. For instance, individuals stated that they did not want to ‘be a vegetable’ but did not know the words to write down on the form. The following examples from individuals who attended a workshop illustrate the point.
We wanted to find a way to say, if there was a major problem we want the pain to be relieved entirely even if that shortened our lives. Finding the right way to say things was really difficult. (P13) Well, if I’m going to be a vegetable, I don’t want to be resuscitated. But you can’t actually write that in a document. So how do you say that and get the meaning across, but be clear enough for other people to make proper decisions? (P11)
One participant self-identified as neurodivergent, stated that they had attended 3 workshops and found it very helpful on each occasion. However, they had been unable to complete the AHD even with one-on-one support because they felt overwhelmed by the amount of written information. They suggested that a video could be made to record preferences and decisions as an official alternative to a written document. Finding the words for this participant meant finding a different way to share their decisions.
Substitute Decision-Makers
Substitute decision-makers had concerns that they could misinterpret the message in the AHD which would lead to not fulfilling the individual’s preferences. Therefore, it was vital to get the right words that would accurately convey the preferences.
He [her brother] lived independently, but he would not want people to call an ambulance because he was really worried about the action they would take. When he went on a trip . . ., he got a tattoo on his chest that said ‘do not resuscitate’ because he wanted it to be crystal clear to people. I think having had lots of conversations with him, if we just walked in and we’re just dealing with a piece of paper, it would be much harder than if you’ve had lots of conversations (P20)
Healthcare Professionals
Healthcare professionals, whose work involved helping their patients understand the AHD document and how to complete it, found that they needed to know appropriate words to converse with their patients. The workshops provided them with what was required to support patients who were receiving palliative/EOL care.
. . . it was from having attended the workshop that gave us the conversation, gave us the narrative to actually realise, that there was a discussion to be had. (P10) I learnt a few of those [words] on how to get the conversations with patients. Yes, that [ACP workshop] helped me. (P 21)
Finding the People
“Finding the people” describes the problems associated with discussing plans with substitute decision-makers and how attending the workshop helped. In addition to finding the words to clearly and accurately communicate their preferences on the AHD, there was an element of finding people to entrust with the responsibility of decision-making on their behalf when that was needed. Because the documents themselves talk about so many things that you would never have thought of, and the workshops prepare you for filling in the documents. Then you realise it’s no good just to say, “Oh the kids know what I want”, because they don’t and really, this whole process is important to make sure that you can really have a conversation with the kids. (P 11)
When people consented to become a substitute decision-makers, they wanted to be sure they knew what the individual’s preferences were. The workshop gave them the confidence they felt they needed to ensure they made decisions that honoured the individual’s preferences.
. . .and so, when you are making a decision, you know, in the instance of my brother where we absolutely knew he didn’t want to be kept alive for the sake of keeping alive. But you just have to be confident because you are dealing with someone’s life or death. (P20) I need to know what she wants now – you can’t un-revive someone if you do the wrong thing. (P13)
One individual felt that blood relatives were not always the best people to entrust future EOL decision-making responsibilities. At times, they were friends or people from a community group such as a church, as illustrated by this participant.
My next step is to go to church, . . . I’m hoping to sit down with them and ask them to take over the care of me [make decisions]. And they know what I want. (P14)
The workshops helped participants think about the details and gave them the words and confidence to talk to the people they chose to speak on their behalf. This newfound confidence enabled them to find a way to discuss advance care planning. They also gained new ideas about how to communicate with their families through interactions with other workshop participants.
Family Relationships
Substitute decision-makers reported that the workshops gave them skills as decision-makers to carry out their responsibilities. They acknowledged that sometimes, family members may not agree with decisions made on behalf of the individual, but the skills acquired at the workshops gave them confidence to advocate for the individual.
There’ll be a family member who’s not accepting of what’s happening. . . in the majority, yes, the conversations can be hard. PCWA has helped in skilling me to handle such situations and it’s very helpful (P10)
Healthcare professionals also reported having difficulties in providing care when there was no substitute decision-maker appointed and no AHD in place, compared to when there was a completed AHD.
If that discussion hasn’t occurred . . . it is very difficult. . . if they want to die at home, which most of our clients do, and we know that and we’re very clear [through the AHD] on that, then we can do our best to make that happen. (P18)
Participants recognised the potential for family disagreements because of decisions made by a substitute decision-maker. The workshops highlighted the importance of having conversations with their family members. Others recalled negative experiences resulting from not having conversations with family members about their preferences and felt that an AHD if not discussed, had the potential to fracture familial relationships.
And I guess the third bit is making sure you then have the conversations with family. There are always circumstances outside of the control or situations so, they need an understanding . . .to avoid family conflicts. (P20)
Finding the Way
The impact of attending the workshops was far-reaching in communities where participants lived. They took every opportunity to talk to people around them about how the workshops helped them learn and understand the value of a well-documented AHD. It was evident that attending the workshops resulted in something that became an ongoing conversation for participants. Once their voice had been strengthened by participating in the workshops and, realising the benefits of completing an AHD, one could not help but, advocate for it by talking to family, friends, neighbours and even in parliament.
My name is . . . and I feel it is important to share my experiences, as regards Palliative Care and how we need to share our wishes, about our health care and final moments. (part of speech delivered in Parliament) (P 8)
Healthcare professionals were particularly interested in completed AHDs because they were guided on how to care for the person. They found it easier to provide EOL care to a person who had an AHD in place, especially within indigenous communities, although this was also true with other communities. The benefits of attending the workshops were also profound among healthcare professionals who advocated for the provision of workshops by liaising with PCWA to deliver training for residents within retirement villages.
Participant 11, president of the residents committee at the retirement village where he and his wife live, said, ‘I have organised for PCWA to come and run a workshop. It turned out to be very, very popular and in fact, so many people signed up that they ran 2 workshops’. (field notes, June 10, 2024).
Enacting the AHD
Substitute decision-makers also expressed confidence to enact the AHD knowing that they were acting to ensure the person’s values were respected and carried out. They also realised that it was not as difficult as they thought to follow someone’s wishes when they were documented. It gave them confidence that they were doing what the person wanted, therefore, they felt like a weight had been lifted off their shoulders.
. . .If there is an AHD, that helps us, because we can always go back to the document and see what the patient wants. But when there is no document, it is a whole complex process. (P21).
Another benefit of documenting preferences following attendance at the workshop was that completing the AHD helped families maintain relationships that may otherwise have been broken due to differing viewpoints about how to proceed with their loved one’s care.
And my son said to me, just as well he did that [completed AHD] because he said I would have fought him going at that stage. And so, I would have had cause to have a dispute with my sons, which I certainly wouldn’t have wanted to do. (P8)
Case Studies
Table 2 below presents the stories from each of the participant groups about the benefit of attending ACP workshops and the impact the workshops had on care delivery.
Case Studies of the Impact of Attending PCWA ACP Workshops.

Discussion
The purpose of this evaluation was to understand the longer-term impact of the PCWA ACP workshops and of having an AHD. To achieve that goal, the evaluation recruited and interviewed end-users of the workshops; individuals, primary carers, substitute decision-makers, and healthcare professionals. All of whom had attended community workshops led by PCWA but had different experiences according to their roles. The groups were interviewed to solicit information, not just about the benefits of the workshops in providing skills and information to the participants about the importance of ACP and preparing an AHD, but also how workshop participants utilised the gained skills and information going forward.
Data analysis in the evaluation of the long-term impact of workshops strongly suggests that participants found the workshops informative, beneficial, and consistent with previous evaluations7,8 and studies about ACP in the community 15 The workshops enabled participants to gain insight not only into how to complete an AHD and other relevant documents such as the Enduring Power of Attorney (EPA) and EPG, but also how to have crucial conversations with family. Such workshops have the ability to provide an atmosphere for building confidence to discuss EOL matters.16,17 Studies also show that attending ACP workshops facilitates a change in attitude towards ACP and that, through interaction with other participants, they provide a good learning atmosphere. 17 The workshops provided by PCWA certainly demonstrate the ability to change attitudes, boosting the confidence of individuals, carers, substitute decision-makers and healthcare professionals. EOL is not an easy topic, 18 but PCWA has brought the WA community together to think and talk about something which is often perceived as a taboo subject.
Finding the words to communicate preferences in an AHD and share those preferences with family can be challenging. But when individuals felt confident that they had effectively conveyed their preferences, a sense of peace was attained which has been noted in previous research. 19 One participant, whilst finding the workshop invaluable, had such difficulty in finding the words that she had suggested it would be helpful to video record her AHD. It should be noted that a person can express their EOL preferences in any format, including a video. These formats have legal standing (under common law), although would not be afforded the same legislative weight as a written AHD (which falls under statutory law). This could be reinforced in the workshops. However, it was clear from this evaluation findings that the value to the community provided by the workshops was immeasurable, as many participants shared the information with others.
The ripple effect of ordinary people sharing the positive outcomes of the workshops with their families, neighbours and even in parliament is evidence of the impact workshops had on participants. Studies such as Ref., 19 acknowledged the benefits of ACP discussions but conceded that with a lack of engagement from family/significant others, these conversations could be hampered. It is important therefore, to note that PCWA incorporates the ‘cards’ activity which many participants find useful in learning how to start a conversation. The cards activity involves using cue cards on palliative and EOL subjects, intended to help open conversations. These cards can be downloaded from the PCWA website. It was these skills and communication strategies imparted by PCWA that enabled participants to talk about the topic of ACP with people in their communities. While workshop participants were keen to advocate for the need to engage with ACP, the absence of GPs who are the primary providers of healthcare in this study, confirms the findings of previous studies. GPs have maintained their limited involvement in helping patients with the AHDs. Previous studies found that GPs did not actively promote and assist their patients with AHDs because of decisional conflict and ethical dilemmas when it comes to enacting the document, 20 insufficient time to assist patients 21 and having inadequate knowledge about AHD.21,22
Previous evaluations,7,8 have not followed up with substitute decision-makers or healthcare professionals to understand the impact of having an AHD when it comes to enacting the preferences on behalf of a loved one. The data clearly shows the positive impact completing the document has on the person carrying the responsibilities of decision-making. Participants who had experienced the death of a loved one, both with and without an AHD, there was a stark difference in personal grief and the risk of family fracture.
When combined with participation in the workshops, the evaluation found the substitute decision-makers had more confidence in their knowledge and ability to assert the preferences of their loved one. This empowering experience helped them, even as they reflected on a sad and difficult time. They felt comforted that they had done the best for their loved one which was a positive and life-affirming feeling even in their grief.
Strengths and Limitations of the Evaluation
Recruiting for the evaluation proved difficult as seen by the proportion of participants when compared with contacts. This was also found in the last evaluation 8 which may indicate that those that participated in the study were positively inclined towards the workshops thus, creating a bias in participant recruitment. Evaluation of the longer-term impact of the workshops for individuals is by its very nature difficult as they are only fully known after the person has passed away and the AHD has been. Yet it is these long-term consequences that have such importance for the health of those involved in EOL decision-making and care. The strengths of this evaluation are that individuals who attended workshops, carers and substitute decision-makers and healthcare professionals were represented, and their voices were heard. There was a lack of engagement however from GPs despite being invited after a referral from a substitute decision-maker. GPs are also key in ensuring individuals complete AHDs in a timely manner and key in enacting the AHD when required. 23 Future long-term impact evaluations of the workshops may benefit from a prospective approach which would enable engagement with all those involved at the time. Although there was no participation by GPs in this study, the findings provide practical insights for practice, particularly in raising awareness of ACP and AHD, advocating for EOL decision-making and improving the quality of life and care in alignment with individual’s wishes. Additionally, the evaluation findings have the potential to influence and provides a valuable foundation for future cross-regional and cross-cultural research.
Recommendations
Evaluation participants were keen for the workshops to continue because of the benefits they received from attending. The following were recommendations by participants:
PCWA workshops need to be scaled up to offer the service to more Western Australians.
Expand individualised service to help more people complete the documents.
Reinforce in the workshops the alternate methods for recording AHD, and the online resources available.
Offering GP’s tailored workshops to enable incorporating ACP discussions and documentation in primary health care.
The evaluating team recommended that PCWA consider a longitudinal prospective study of the workshops’ impact. This type of study would enable investigation of the relationship between outcomes and exposure to the workshops.
Conclusion
This evaluation was undertaken to look at the long-term impact of the PCWA ACP workshops. Analysis revealed that participants considered the workshops to be important for individuals, families and communities in Western Australia. All participants supported PCWA continuing to offer the workshops as they were invaluable. Past workshop attendees were very keen for people in their communities to learn about and complete the AHD forms for themselves, as demonstrated when they encouraged family members and friends to attend subsequent workshops.
Supplemental Material
sj-docx-2-inq-10.1177_00469580251371891 – Supplemental material for Advancing Person-Centred Care Through Palliative Care WA’s ACP Workshops: The Longer-Term Impact
Supplemental material, sj-docx-2-inq-10.1177_00469580251371891 for Advancing Person-Centred Care Through Palliative Care WA’s ACP Workshops: The Longer-Term Impact by Gertrude G. Phiri, Emma Gunner, Philip Bafile and Davina Porock in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-1-inq-10.1177_00469580251371891 – Supplemental material for Advancing Person-Centred Care Through Palliative Care WA’s ACP Workshops: The Longer-Term Impact
Supplemental material, sj-pdf-1-inq-10.1177_00469580251371891 for Advancing Person-Centred Care Through Palliative Care WA’s ACP Workshops: The Longer-Term Impact by Gertrude G. Phiri, Emma Gunner, Philip Bafile and Davina Porock in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We would like to thank Sabena Lund and the staff at Palliative Care WA for their help and support in the recruitment of participants.
Ethical Considerations
The Human Research Ethics Committee at Edith Cowan University approved our interviews (approval: 2024-05155-POROCK) in April 2024.
Consent to Participate
Informed written consent was obtained from all individual participants included in the study before starting interviews.
Author Contributions
Gertrude G. Phiri: Conceptualisation, methodology, data collection, data analysis and writing original draft. Emma Gunner: Data collection, data analysis, reviewing original draft and editing. Philip Bafile: Data analysis, reviewing original draft and editing. Davina Porock: Original conception, methodology, supervision of the work, data collection, reviewing and editing of the original draft.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the evaluation of PCWA’s Advance Care Planning Workshops and subsequent report has been provided by the WA Department of Health. An independent evaluation is a requirement of the Health Department’s Sustainable End of Life and Palliative Care Peak Body Services contract with PCWA.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The Research Team do not intend to re-use the data.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.