
Abstract
Introduction:
The Age-Friendly Health Systems initiative (AFHS) was developed to spread principles of high-quality care for older adults using the 4Ms Framework: What Matters, Medications, Mentation and Mobility. In 2020, the Veterans Health Affairs (VA) set a goal to become an AFHS, given nearly half of Veterans are over aged 65.
Methods:
This quality improvement study followed the Model for Improvement which guided a series of Plan Do Study Act (PDSA) cycles to implement and spread the AFHS model within the VA, as measured by clinical sites receiving AFHS recognition from the Institute for Healthcare Improvement (IHI). A national AFHS Steering Committee was formed, followed by a 4Ms note template and dashboard. VA ran 3 AFHS Action Communities which included synchronous training sessions and coaching calls in 4Ms care. IHI recognition was tracked over 5 years for VA sites. The Standards for Quality Improvement Reporting Excellence 2.0 guidelines (SQuIRE) were used.
Results:
From 2020 to 2025, 455 VA care settings earned Level 1 recognition from IHI at 138/139 (99%) of VA parent facilities. 268/455 (59%) sites have gone on to achieve Level 2 recognition. 66% of Level 1 sites are ambulatory, 7% are acute care, and 24% are nursing homes. Since 2022 when the VA AFHS note template was implemented, 163 000 unique Veterans have been recorded as having been reached with 4Ms care, of whom 71% reside in urban areas, 23% are aged 85 and older, and 59% are aged 65 to 84.
Conclusion:
The VA implemented the AFHS initiative at nearly all VA parent facilities over 5 years, spreading the 4Ms model of Age-Friendly care across geographic and care settings. Further study is needed on the clinical impact of and optimal implementation strategies for AFHS. The VA experience offers a promising model for health systems seeking to implement AFHS.
Highlight
The Department of Veterans Affairs successfully implemented the Age-Friendly Health Systems iniative across all VA parent medical centers across 5 years, offering a promising model for spreading high quality geriatrics care focused on the 4Ms of Mobility, Mentation, Medications and What Matters.
Introduction
As the population ages, the healthcare system must adapt to meet the needs of our aging population; in particular, the Veterans Health Affairs system serves an increasingly old Veteran population, with nearly half of Veterans over aged 65.1,2 Older Veterans have unique needs and are more likely than younger Veterans to experience polypharmacy, disability, cognitive impairment, mobility limitations and/or multimorbidity. 3 The Age-Friendly Health Systems Initiative (AFHS), developed in 2018 by the Institute for Healthcare Improvement (IHI) in partnership with the John A. Hartford Foundation, seeks to integrate best practices in geriatric care using the memorable 4Ms framework: What Matters, Medications, Mentation, and Mobility (Figure 1). 4 Each of these pillars is based on evidence generated from successful care models that improved outcomes for older adults, 5 meant to help clinicians across care settings assess older patients for any limitations and “act on” the findings to align care with goals. 4 For example, the “What Matters” domain refers to eliciting what matters to an older adult both for current and advance care planning, while for “Medications” teams should identify potentially high risk medications and optimize polypharmacy as appropriate. For “Mentation” or “Mind,” clinicians should focus on screening for delirium, dementia, and/or depression, and for “Mobility” teams should identify ways to support function and reduce the risk of falls. 6 Once a clinical setting demonstrates that it has a system to “assess and act on” each M, it can apply for AFHS recognition from the IHI as a participant (Level 1); once a setting has implemented the 4Ms for at least 3 months, it can apply for Level 2 recognition, known as “Committed to Care Excellence.” 7

An image from a VA public-facing website inviting veterans to talk to their care teams about age-friendly care. 8
Since its launch, AFHS has spread to thousands of care settings across the United States and beyond 9 and the 4Ms have become a shared language for Geriatric care and workforce training.10-12 In 2020, the Veterans Health Affairs (VA)’s Office of Geriatrics and Extended Care (GEC) joined the Age-Friendly Health Systems movement 4 to advance VA’s goal to provide the best care to the nation’s aging Veteran population, seeking to improve care for older Veterans and help them age in place when possible. 1 The VA’s enrollment in AFHS builds on a long legacy of innovation in Geriatric care, including the creation of the Geriatric Research, Education, and Clinical Centers (GRECCs), which serve as centers of excellence and engines of innovation in the care of older Veterans. 3 GRECCs typically collaborate with GEC to implement clinical innovations, and in the case of AFHS several GRECC leaders served as early AFHS adopters in VA and leaders in the AFHS Steering Committee (including author AWS).
Understanding the VA’s experience with implementing AFHS is important for several reasons. First, the VA population continues to age, so information about the implementation of AFHS is essential to guide future initiatives to support this high-needs population. Next, the VA anticipates running a “State of the Art” conference on the future of Age-Friendly research, so a clear context of the current state is critical to inform next steps of AFHS implementation, research and evaluation. 13 And finally, as other large health systems seek to “scale and spread” AFHS, the VA’s experience may offer a possible model and experience. Several large health systems, such as CVS Minute Clinic, have also engaged with AFHS, 14 but more evidence is needed about how to scale the 4Ms within large integrated health systems. Although an increasing number of papers have been written about AFHS within the VA, most have provided theoretical overviews on the importance of this approach,1,3,15,16 offered single-setting implementation or evaluation studies,17,18 or focused on interventions related to 1 of the 4Ms but not the set.19-22 Recent studies offer reviews of implementation strategies, but are limited by setting, 23 or not specifically focused on the VA. 24 Table 1 offers example of emerging evidence from the VA’s AFHS initiative and illustrates the need for a paper to detail the first years of implementation of AFHS within the VA. This manuscript aims to close these gaps in the literature by describing the implementation of the AFHS as a quality improvement initiative within the national VA health system, including the approach and results from the first 5 years, and discussion of lessons learned and future directions for AFHS within the VA and beyond.
Select Publications on the Age-Friendly Health Systems Initiative within the VA, Listed by Clinical Setting.
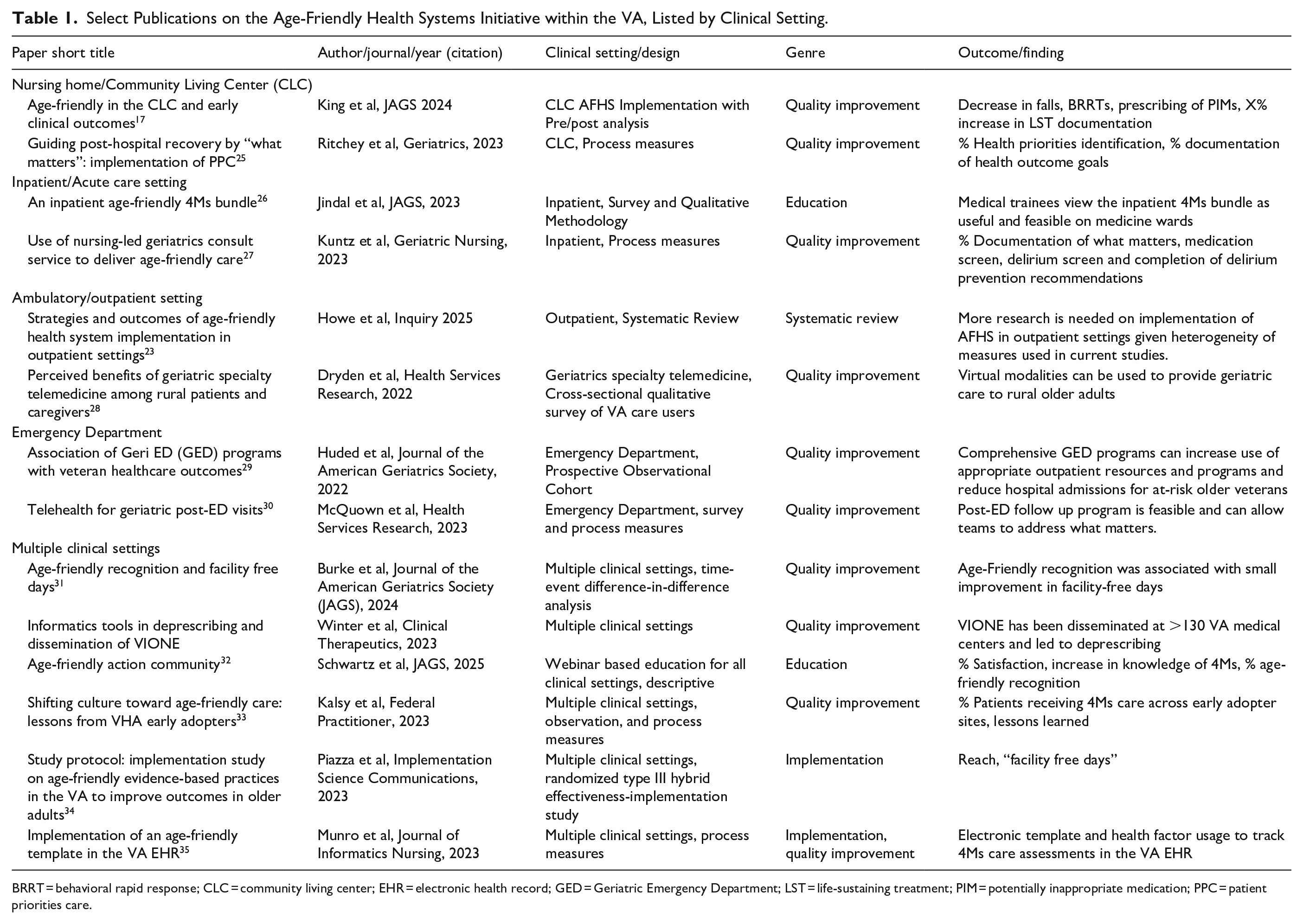
BRRT = behavioral rapid response; CLC = community living center; EHR = electronic health record; GED = Geriatric Emergency Department; LST = life-sustaining treatment; PIM = potentially inappropriate medication; PPC = patient priorities care.
Methods
This paper uses the SQUIRE 2.0 (Standards for Quality Improvement Reporting Excellence) reporting guidelines 36 to describe the implementation of AFHS within the VA. This study was considered quality improvement for operations purposes, and thus exempt from further institutional review board oversight per Veterans Health Administration (VHA) Program Guide 1200. 37
The VA Office of Geriatrics and Extended Care, which set the goal for the VA to become the largest health system to be recognized as Age-Friendly and to implement AFHS across multiple clinical settings, took into consideration multiple contextual factors. The contextual factors which were considered include the VA being an integrated health care system with ability for high quality communication across facilities, having a centralized electronic health record system, and understanding that the delivery of Age-Friendly care is part of the VA mission of providing high quality care to Veterans as a High Reliability Organization. 38 The Model for Improvement was the framework that guided VA implementation of AFHS, with its emphasis on forming a team, setting aims, establishing measures, and then selecting and testing changes before implementation and spreading them.39,40
In 2020, GEC formed a dedicated central office team to work with VA sites to implement AFHS, which included a program lead (KW), programmatic assistants, and an implementation science expert from the VA Office of Innovation detailed to GEC to the guide implementation. The VA AFHS team formed a partnership with IHI and the John A. Hartford Foundation to support implementation of AFHS within the VA. The intervention in this study was the implementation of AFHS throughout the VA through a combination of test of changes known as Plan-Do-Study-Act (PDSA) cycles, described below, designed to achieve goals of implementing AFHS within the VA. 1 To measure success of implementation, the team planned to use the number of clinical settings through the VA recognized by the IHI (Level 1 recognition, Participant level recognition and/or Level 2 recognition, Committed to Care Excellence), which was measured monthly throughout the intervention through recognition information provided to GEC by IHI. Recognition from IHI was considered to be an external measure of meaningful 4Ms implementation, assessed by IHI through a formal process that involves submission of “Care Description Worksheets” that detail the particular settings approach to AFHS implementation, 7 including the teams’ listing of evidence based screening tools and clinical approaches to address each of the 4Ms in their particular care setting. Because AFHS implementation and recognition were not required of VA teams, the study team hypothesized that without intervention, a significant increase in VA teams receiving AFHS recognition from IHI would not be seen. The study hypothesized that a multifactorial intervention including creating a leadership team, developing training materials and creating infrastructure to track 4Ms implementation would lead to an increase in numbers of clinical teams receiving AFHS recognition from IHI. Since the VA set a goal to spread AFHS within the VA nationally and advertised this opportunity broadly through VA communication channels, the study lacked a comparison group of teams who were not invited to participate in AFHS.
Figure 2 illustrates the timeline of PDSA cycles for implementation of AFHS within the VA, along with a run chart including AFHS recognition numbers from IHI. Although the VA AFHS team assessed individual aspects of the intervention through mixed methods approaches, such as assessing the VA educational efforts through quantitative and qualitative assessments described elsewhere, 32 this study measured the success of the overall AFHS implementation through completed AFHS recognitions from IHI. The study team anticipated that recognitions would increase with time, as more VA teams had the opportunity to participate in VA AFHS trainings and gain access to VA AFHS resources, described below.

Run chart and timeline of VA age-friendly PDSA cycles and level 1, AFHS recognition of VA care settings by IHI (as of 3/1/2025).
The first step in the Model for Improvement is forming a team, and this was among the first PDSA cycles conducted in the national implementation of AFHS within the VA. The GEC AFHS team sought out VA early adopters of AFHS, by communicating with IHI to identify VA teams who had participated in IHI trainings on AFHS, known as “Age-Friendly Action Communities.” 9 An Age-Friendly Action Community involves several months of webinars and coaching calls about the 4Ms, designed to help teams adopt the principles of AFHS and complete the steps to recognition from IHI.7,32 The first VA clinical teams enrolled in an Age-Friendly Action Community led by the IHI in March 2020, and tended to be led by clinicians already engaged in Geriatric care, such as Geriatrics Clinics, which are either primary care or multidisciplinary consult clinics, and Community Living Centers (CLCs, which are VA skilled nursing facilities that typically include both long term care and short term rehabilitation wards). 1 Several of these early adopters were invited to join the inaugural VA Age-Friendly National Steering Committee, formed in July of 2021. The Steering Committee members were invited to serve 2-year terms, with the possibility of renewal, and the AFHS team intentionally sought Steering Committee representation from different health professions, including physicians from different specialties including geriatrics, primary care, hospital medicine, spinal cord injury, and more, as well as nurses, pharmacists, social workers, psychologists, physical therapists, and more. The Steering Committee members also represented a broad array of geographic regions across the VA as well as different care settings and service lines such as primary care, nursing home, and hospital medicine. Together, the GEC Age-Friendly team and the VA Age-Friendly National Steering Committee identified key drivers of implementation at the facility level and then planned for scale up and spread across VA facilities.
While the Steering Committee was initially aware of many sites implementing AFHS within the VA, they lacked a formal mechanism to track sites in progress, prior to receiving recognition from IHI. In fall 2022, a subcommittee of the Steering Committee developed a national electronic health record (EHR) note template to track implementation of 4Ms care. 35 The template allows teams to document 4Ms care in a variety of settings, such as whether and how Mentation was addressed, for example, and laid the foundation for the national VA Age-Friendly 4Ms Dashboard, launched in fall 2023. The VA AFHS dashboard, an online tool that draws data from the completed AFHS note templates, can be used to track local implementation of AFHS and supports teams to gather data for Level 2, Committed to Care Excellence recognition from IHI, which requires counts of older adults reached by 4Ms care. Additionally, the dashboard allows for continuous process improvement and nationally, helps leaders understand the implementation, reach and impact of 4Ms care throughout the VA health care system.
The national VA Age-Friendly 4Ms Dashboard includes several data visualizations for completed 4Ms assessments, allowing teams to filter the data by facility, care settings/location, and timeframe (fiscal year/month). Any staff member in VA can request access to the dashboard and with the correct permissions, can drill down to see Veteran-level data to understand which individual Veterans have received 1, 2, 3, or all 4Ms within a specific timeframe. Additionally, teams can see which other care settings/locations across VA are documenting 4Ms care using the national 4Ms EHR template, creating opportunities for synergy and collaboration. By regularly reviewing the dashboard data, teams can identify opportunities to improve their processes and to identify outcomes that matter to the older Veterans they serve.
The next PDSA cycles involved creating an online community and conducting trainings on AFHS within the VA. An online “Community of Practice” for VA AFHS was created via Microsoft Teams, which allowed for dissemination of new AFHS tools and resources as well as celebration of teams earning AFHS recognition from IHI. A Sharepoint site was developed to host VA specific AFHS tools, such as guidance on forming interprofessional AFHS teams for local leadership and implementation, a list of publications relevant for VA AFHS, and VA-specific adaptations of IHI AFHS resources. 41
In fall of 2022, VA launched its first VA-specific Age-Friendly Action Community, intended to help VA teams adopt Age-Friendly approaches across care settings. 32 The Action Community provided 7 months of synchronous online webinars focused on each of the 4Ms, which featured clinical experts on each topic as well as interprofessional teams highlighting case examples of implementing the 4Ms. Over 150 teams participated in the first VA AFHS Action Community, contributing to a steady growth of AFHS recognitions, described elsewhere. 32 VA hosted its second Age-Friendly Action Community from January to July 2024. Over 440 teams enrolled, representing over 1000 clinicians from 129 VA facilities in 48 out of 50 states. During that same time, in March 2024, the VA Under Secretary for Health (USH) signed memorandums of understanding with IHI and The John A. Hartford Foundation, formalizing VA’s partnership with these organizations, recognizing the shared goal of advancing Age-Friendly care for Veterans.
The next step in implementing AFHS took place in June 2023, when VA hosted an Age-Friendly Summit to bring together nearly 100 leaders and champions to accelerate adoption of the 4Ms, document key lessons learned from early adopters, and develop a 5-year plan moving forward. Day 1 of the Summit focused on building connections through gathering individual insights, initiating collective conversations, and building network support among attendees. Day 2 challenged attendees to identify priorities and creative approaches to scale up and spread AFHS in VA. Three key themes underscored essential next steps in the movement, focusing on (1) Veteran Experience, (2) Engagement, and (3) Evaluation. These themes were then shaped into actions, milestones, and measures for fiscal year (FY) 2024 to 2028, to be tracked and enacted by the Steering Committee and GEC AFHS team. Milestones to be tracked included number of unique Veterans reached by 4Ms care, number of teams achieving Level 1 and Level 2 AFHS recognition from IHI, and % of parent VA medical centers (each of which may contain multiple VA health settings) with an AFHS recognized site.
In 2024 several VA teams joined IHI’s “scale up and spread collaborative” which focused on parent VAs and other non-VA medical centers with 3 or more clinical sites with AFHS recognition. Finally, VA hosted its third Age-Friendly Action Community from January to July 2025, with over 500 teams enrolled.
Results
From March 2020 when the VA committed to becoming an Age-Friendly Health System, to March of 2025, a total of 455 VA care settings have earned at least AFHS Level 1, Participant recognition from IHI at 138/139 (99%) of VA parent facilities. Figure 2 summarizes key milestones and PDSA cycles in the VA’s AFHS journey and provides a run chart demonstrating the growth in AFHS Level 1 recognition of VA care settings through March 1, 2025. Figure 3 illustrates the geographic spread of AFHS within the VA.

Geographic distribution of VA sites with Age-Friendly recognition from IHI, as of March 2025. 42
As of March 1, 2025, a total of 268/455 (59%) VA clinical sites have also gone on to achieve AFHS Level 2 recognition from IHI, known as Committed to Care Excellence. Of the 455 care settings with AFHS Level 1 recognition, 66% are ambulatory settings (including Home Based Primary Care), 7% are acute care settings, 24% are CLCs, and 3% are emergency departments and urgent care. 43
Since September 2022, when the VA AFHS note template was implemented, a total of 163 000 unique Veterans have been recorded as having been reached with 4Ms care (as of 3/31/2025). About 71% of these Veterans reside in urban areas, 28% in rural areas and 1% in highly rural areas. Of the Veterans reached with 4Ms care, 23% are aged 85 and older, 59% are ages 65 to 84, 12% are ages 45 to 64, and 5% are less than 45 years old. Vietnam-era Veterans make up 61% of those reached with 4Ms care.
The number of recognitions continued to rise steadily over the course of the observed period. Over 1000 teams have participated in a VA Age-Friendly Action Community, though it was not possible to determine which of these teams may have participated more than once or with different team members. Recognition numbers do not reflect teams that may have Care Description worksheets in progress or under review by IHI. Because the VA AFHS intervention was voluntary for teams, no additional costs were associated with the intervention, beyond the cost of the GEC staff involved in AFHS and the time spent by Steering Committee and clinical team members on a voluntary basis.
Discussion
VA has rapidly implemented AFHS nationally, spreading the 4Ms framework to over 455 care settings at 99% of VA parent medical centers, with broad geographic distribution. Despite being first introduced at the height of the COVID-19 pandemic in March of 2020, the AFHS initiative has been spread largely through the voluntary efforts of VA clinicians and teams engaged with the AFHS movement. 1 Hundreds of teams have participated in the VA Action Communities, and team enrollment has increased with each subsequent Action Community. The VA AFHS note template and dashboard track the growing adoption of 4Ms care across care settings, and recognition numbers from the IHI continue to climb and increase in geographic distribution. The Veterans reached by the 4Ms according to the AFHS dashboard older than the general VA population, with 82% aged 65 and above, compared to 49% of the general Veteran population who are aged 65 and above. 2
To our knowledge, this is the first manuscript to report on the implementation and spread of AFHS within a large national health system that spans multiple care settings. While other papers have detailed the spread of AFHS, these have typically only been reported in 1 type of clinical setting (ie, – convenient care clinic) 14 or individual sites 33 or settings. 17 This paper closes a gap by demonstrating the spread of AFHS recognition through multiple PDSA cycles designed to engage interprofessional teams across care settings and across the country.
Strengths of this project include the multifaceted nature of the intervention, which included development of both educational and community building approaches (Steering Committee, Action Community, online Community of Practice) as well as informatics infrastructure (note template, dashboard) to implement AFHS. Other strengths include multiple sources of data, including internal VA data such as the 4Ms Dashboard and external VA data such as IHI Age-Friendly recognitions. Early data from other studies suggests strong engagement from VA clinicians and team members, with potential for significant cost savings and system impact, though further study is needed.17,31,44 Because AFHS can build on and provide synergy with existing VA initiatives within a specific M domain, 15 team members already engaged with 1 aspect of Geriatric care and/or 1 of the 4Ms may be willing to engage to extend their efforts to other M domains and pursue AFHS recognition of those efforts.1,3,17
Several aspects of the Model for Improvement have helped to shape the journey of many VA teams, including getting started with small tests of change on a local level, and leveraging storytelling to demonstrate the value of Age-Friendly care for Veterans. 45 Nationally, it has been important to provide multiple opportunities for learning and engaging with AFHS, reinforcing the purpose of the movement and demonstrating how AFHS aligns with VA health care priorities. Annual communications plan including regular update emails and an annual “State of Age Friendly” virtual call have helped to engage various stakeholders, sharing information about AFHS recognition with the VA and sharing examples of evidence-based practices and innovations to promote 4Ms care within the VA. 5 Figure 4 illustrates these pillars for scaling and spreading AFHS within the VA. Perhaps most importantly, a unified vision has guided VA across all levels of the organization: to become an integrated Age-Friendly Health System ready to provide person-centered care for all Veterans as they age. 15

Strategies for scaling and spreading age-friendly health systems within the VA.
Limitations of this work include the unique nature of the VA care setting, which may impact its generalizability to other health systems. For example, the VA tends to have more male patients, patients with higher comorbidities and an older average age than in the general population.2,3 Another limitation includes the lack of information about the frequency of completion and fidelity of the 4Ms note template at capturing clinical practice, 35 which could lead to under or over estimating the number of Veterans reached by 4Ms care. Further, it is not known to what degree achievement of IHI recognition corelates with changes to care pathways or clinical outcomes, through studies of individual sites offer promising early results.17,46 This study lacked a comparison group, through future studies could look at clinical outcomes in groups that did and did not achieve AFHS recognition, as early data suggests clinical impacts associated with AFHS recognition. 31 However, despite these limitations, this study offers measures of AFHS uptake that require a more structured self-report through the note template and IHI Care Description worksheets, which suggest both an internal and external evidence of spread.
Additionally, although the initial scope and scale of AFHS dissemination within the VA over the past 5 years has been rapid, further study is needed to under barriers, facilitators and impact of AFHS implementation in different care settings and regions. For example, the national dashboard can shed light on the degree to which AFHS transformation is reaching older adults across demographic groups to ensure all Veterans receive Age-Friendly care, and to identify areas of low uptake or uneven reach to specific patient populations, sequentially combining quantitative inquiry at the dashboard level with qualitative inquiry at sites where implementation lags to explore barriers. 47
As VA scales up and spreads 4Ms care to reach more Veterans, opportunities are emerging for evaluation, research, education, and clinical innovation projects to related to the 4Ms, both individually and as a set. Evaluation efforts include studying implementation strategies and clinical outcomes, such as the impact on person-centered outcome measures that matter to Veterans.16,34 Future education efforts include developing asynchronous online training modules focused on Age-Friendly care for interprofessional teams and health professions trainees, which could be used to onboard new team members into AFHS approaches to care. 48 VA clinical innovation efforts in AFHS 42 include 4Ms bundles for hospital teams, 26 4Ms dashboards for outpatient teams18,26 as well as efforts focused on What Matters communication strategies19,25 and safe medication optimization. 49 Other future directions for VA’s AFHS initiative include continuous improvement of the VA-specific AFHS toolkit of resources as well as ongoing education for staff. As of spring 2025, planning is underway for an Age-Friendly State of the Art (SOTA) Conference. 13 The SOTA will bring together Age-Friendly experts and champions to identify what is known and what additional evidence is needed to support 4Ms implementation, sustainment, measurement, and research within the VA.
Ongoing work is planned to continue to study clinically meaningful outcomes16,17 such as days at home and avoidance or delay of nursing home placement. There is also a need to develop more patient facing communication that captures the voice of the Veteran, such as new videos on communicating about What Matters. 50 Increasing collaboration among other potentially related VA programs such as Whole Health, a primary care program which focuses on Veterans’ goals across the lifespan,18,51 and other programs that focus on 1M domain will also strengthen the ongoing implementation of AFHS within the VA.1,15 A remaining question is the sustainability of relying on a primarily voluntary approach top AFHS implementation, and what level of ongoing professional support is needed from the GEC national program office. The VA’s integrated national health system offers an ideal setting to test different implementation strategies for AFHS within large health systems, informed by implementation science frameworks.
Conclusion
In conclusion, this paper demonstrates that the first 5 years of Age-Friendly Health Systems initiative within the VA have resulted in significant spread of the 4Ms, reaching hundreds of teams and thousands of Veterans over a broad geographic area and multiple care settings. However, much work remains to continue to spread and study AFHS within the VA, an urgent priority given the aging Veteran population who deserve person-centered care focused on what matters to them.1,3 The early results of AFHS implementation in the VA offer a promising model for implementing Age-Friendly care within a large health care system.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251366883 – Supplemental material for Implementation of the Age-Friendly Health Systems Initiative in the Department of Veterans Affairs: 5 Years of Improving Quality for Older Veterans
Supplemental material, sj-docx-1-inq-10.1177_00469580251366883 for Implementation of the Age-Friendly Health Systems Initiative in the Department of Veterans Affairs: 5 Years of Improving Quality for Older Veterans by Andrea Wershof Schwartz, Shivani K. Jindal, Kimberly A. Wozneak and Robert E. Burke in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors wish to acknowledge the John A. Hartford Foundation and the Institute for Healthcare Improvement for their partnership in the Age-Friendly Health Systems movement. The authors would also like to thank their colleagues in the Veterans Health Administration, and in particular the staff in GEC and members of the VA Age-Friendly Health Systems Steering Committee, for their dedication to the care of Veterans.
Author Contributions
All authors contributed to data collection, drafting and revising the article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: VA received funding for the Age-Friendly Health System Action Communities from The John A. Hartford Foundation and the IHI through the Foundation for Atlanta Veterans Education and Research (FAVER) and the Birmingham/Atlanta Geriatric Research Education and Clinical Center (GRECC) at the Atlanta VA Healthcare System. This material is based upon the work supported by the Department of Veterans Affairs, Veterans Health Administration, Office of Geriatrics and Extended Care, and the New England Geriatric Research Education and Clinical Center. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the Department of Veterans Affairs or the United States government.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AWS and SKJ report serving as faculty for the Institute for Healthcare Improvement. KW served as the VA Age-Friendly Lead, and AWS, BB, and SKJ served on the VA AFHS Steering Committee. The other authors report no actual or potential conflicts of interest regarding this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.