
Abstract
Consanguineous marriages are known to increase the risk of autosomal recessive genetic disorder. In this study we aimed to examine the perspective and attitudes of parents with 1 or more affected children by an AR disease toward consanguineous marriages. A total of 285 parents completed a self-administered survey. The participants belonged to 2 groups: a clinical sample defined as consanguineous parents with at least 1 child affected by an AR genetic disease, while the community sample were non-consanguineous parents. The questionnaire was about the subjects’ attitudes toward consanguinity and was divided into 2 parts: sociocultural and health attitudes. The clinical sample showed positive sociocultural views toward consanguineous marriages compared to the community sample as they had statistically significant differences regarding the belief it decreases divorce, general support of consanguinity in general and more specifically encouragement of their children to marry a relative. Regarding health attitudes, statistically significant differences were found between the 2 groups in 6 out of 7 examined variables. Despite the well-known associated reproductive and genetic risks of consanguinity, consanguineous subjects continue to support and positively view such marriages.
Keywords
Highlight
● Consanguinity and Child With Autosomal Recessive Disease.
Introduction
Consanguineous marriage is widely practiced in Arab and Middle Eastern countries, with some of the highest rates globally. 1 The prevalence of consanguinity in the Middle East and North Africa (MENA) region is estimated to range between 25% and 60%, with a preference for first-cousin marriages, leading to a high incidence of autosomal recessive (AR) disorders in the region. The association between consanguinity and the prevalence of AR diseases is well-documented.1 -7 Many Arab societies remain tribal, with a limited number of ancestral lineages, resulting in a significant burden of certain genetic disorders confined to specific tribal groups or families. 2
Despite the well-documented risk of an increased incidence of inherited autosomal recessive (AR) disorders, as well as the high prevalence of certain genetic conditions among specific tribes, endogamy and consanguineous marriages remain widely practiced and highly regarded in the MENA region due to various socio-cultural factors. These factors include the preservation of family structure and property, the facilitation of marital arrangements, improved relations with in-laws, reduced risk of undisclosed financial or health issues, and the belief that such unions promote marital stability. 1 In the United Arab Emirates, despite the numerous challenges that women face, many participants continued to uphold the practice of consanguineous marriage. 8 Similarly, data from Saudi Arabia indicate that consanguineous marriages remain prevalent, even among individuals aware of the heightened risk of genetic disorders in their offspring. 9
In Kuwait, consanguinity remains prevalent, as evidenced by 2 studies conducted in the last decade using data from the preceding 3 decades, despite its well-documented adverse reproductive health consequences.10,11 The earliest study found that nearly half of married couples in Kuwait were consanguineous, 11 while the most recent study reported a slight decline, yet consanguineous marriages still accounted for 46% of unions. 10 Recent research has further examined the association between consanguinity and the increased prevalence of certain inherited genetic disorders in Kuwait, including mitochondrial diseases,12,13 inborn errors of immunity,14,15 classic homocystinuria (OMIM number 236200), congenital malformations,16,17 primary ciliary dyskinesia (OMIM numbers 244400 and 612444), 18 retinitis pigmentosa (OMIM numbers 617460 and 613660), 19 and hyperoxaluria type 1 (OMIM number 259900). 20
The major aim of this study is to examine the sociocultural and health perspective and attitudes of parents with 1 or more affected children by an AR disease toward consanguineous marriages. To reach our aim, we compared the responses of this group with those of non-consanguineous married couples in the community.
Methods
Subjects
A total of 285 parents were invited to participate in this study during February 2022. The sample was divided into 2 groups: a clinical sample consisting of parents attending various hospital clinics and a community sample. The clinical sample included 150 consanguineous parents from different families who attended outpatient clinics in Kuwait for inborn errors of immunity, inborn errors of metabolism, or hematologic diseases and had at least 1 child diagnosed with an autosomal recessive (AR) disease. Of these 150 subjects, 128 (85.3%) responded to the questionnaire (53 males [41.4%] and 75 females [58.6%]). The respondents’ children were affected by inborn errors of immunity (n = 32), hematologic diseases (n = 34), or inborn errors of metabolism (n = 62). The participants’ ages ranged from 24 to 60 years (mean [M] = 39.71; standard deviation [SD] = 8.56).
The second group consisted of 154 respondents from the community, recruited outside clinical settings (49 males [31.8%] and 105 females [68.2%]). Their ages ranged from 30 to 73 years (M = 42.47; SD = 12.94). All were married to non-relatives. The control group was selected from outside the clinic to align with the study’s primary objective. Respondents in both groups included either couples or individual spouses. The study’s aims were explained to all participants.
Variables
A self-administered survey (Supplemental Files) was developed by a clinical immunologist (WA), a medical anthropologist (YA), and a medical geneticist (SB). It included 2 major sections. The first section included demographic and personal data (11 questions), such as sex, governorate, age, education level (6 categories), family income (8 categories), year of marriage, age at marriage, and number of children. Also, the respondents were asked to determine the degree of consanguinity with their spouses. It was divided into 9 categories: first cousins on the father’s brother’s side, father’s sister’s side, mother’s brother’s side, or mother’s sister’s side; double cousins through the father’s brother and the mother’s sister or the mother’s brother and the father’s sister; second cousins; third cousins; and non-consanguineous.
The second section of the questionnaire was about the subjects’ attitudes toward consanguinity and was divided into 2 parts. The second section of the questionnaire (11 questions) was about the subjects’ sociocultural and health attitudes toward consanguinity. Five colleagues in related fields reviewed the questionnaire for validity. The questionnaire was tested for reliability in a pilot study of 32 subjects during a 2-week period.
Sociocultural Attitudes
This section explored sociocultural attitudes toward consanguinity and collected 6 data points: the frequency of consanguineous marriage in the community (“common,” “uncommon,” or “do not know”), whether consanguinity is increasing in the society (“increasing,” “decreasing,” “no change,” or “do not know”), whether consanguinity decreases divorce in the society (“agree,” “disagree,” or “do not know”), whether participants support consanguinity (“agree,” “disagree,” and “neutral”), how participants would react if their child decided to marry a relative (“encourage him or her,” “advise against,” or “does not affect the decision to allow the child to marry”), how common consanguinity was among participants’ families (“common,” “middle,” “uncommon,” or “do not know”), and whether it is important to discuss consanguinity before marriage (“agree,” “disagree,” or “do not know”).
Health Attitudes
This section examined health attitudes toward consanguinity and collected 6 data points: whether the participant thought the death of a child could be caused by genetic disease (“yes” or “no”), whether there is a relationship between consanguinity and abortion (“agree,” “disagree,” or “do not know”), whether consanguinity increases genetic defects in children (“agree,” “disagree,” or “do not know”), whether the participant’s child’s health problem was caused by (“consanguinity,” “unrelated to consanguinity,” or “do not know”), whether a 25% chance that the participant’s fetus would inherit a recessive disease is an acceptable possibility (“agree,” “disagree,” or “do not know”), whether the participant would consider prenatal testing if there were a chance of passing on a recessive disease (“yes,” “no,” or “do not know”), and whether the participant considered marriage pretests a good practice (“yes,” “no,” or “do not know”).
Five colleagues in related fields reviewed the questionnaire for validity. The questionnaire was tested for reliability in a pilot study of 32 subjects during a 2-week period.
Five faculty members from the Department of Sociology and Social Work at Kuwait University reviewed the questionnaire to ensure its validity. The study was approved by The Research and Ethics Committee of the Ministry of Health in Kuwait, and by the Kuwait University Health Sciences Center Ethical Committee, in accordance with the Declaration of Helsinki and informed written consent was obtained from all participants (Ref.: VDR/EC/3544).
Statistical Procedures
Statistical Package for Social Sciences (Version 25) was used for data entry and analysis. Descriptive and inferential statistics were used. Chi-square test was used to examine the difference in percentages between the clinical and outside samples’ sociocultural and health attitudes toward consanguinity. Student t-test was used to examine the differences between clinical and outside respondents’ age at marriage, the total number of children, number of affected children by the same disease in the family, and number of children’s deaths caused by genetic diseases. Finally, the Pearson correlation test was used to examine the relationship between the rate of consanguinity in the respondents’ families and some social and health variables.
Results
Table 1 presents the frequencies and percentages of the degree of blood relation among respondents from the clinics.
The Clinical Respondents’ Degrees of Consanguinity.

The data show that the majority of respondents were married to their first cousins (78.1%). Additionally, 64.8% of the clinical sample married a first cousin, distributed as follows: 21.1% paternal uncle’s side, 7.8% paternal aunt’s side, 15.8% maternal uncle’s side, and 20.3% maternal aunt’s side. Moreover, 13.1% of the clinical sample were married to double cousins, with 9.4% on the paternal uncle and maternal aunt’s side, and 3.9% on the maternal uncle and paternal aunt’s side. The percentages of participants married to second and third cousins were 10.2% and 11.7%, respectively.
The study examined the sociocultural and health attitudes of the clinical sample and compared them with those of the community sample regarding consanguineous marriage and perceptions of consanguinity.
Significant differences were found between the 2 groups. Generally, parents in the clinical sample held a more favorable sociocultural view of consanguineous marriage within society. Most clinical respondents (68.8%) believed consanguinity is common in Kuwait, compared to only 14.9% of the community sample who considered it uncommon.
Regarding perceptions of consanguinity prevalence, significant differences were observed between the clinical and community samples. Among the clinical respondents, 26.6% believed consanguinity is increasing in society, while 21.6% believed it is not. In contrast, 20.8% of the community sample believed consanguinity is increasing, whereas 39.0% thought it is decreasing.
Nearly half of the clinical sample (51.6%) agreed that consanguinity reduces divorce rates, with none disagreeing, while 48.4% were uncertain. Comparatively, 43.8% of the community sample agreed that consanguinity decreases divorce, while 26.8% disagreed, and 29.4% were uncertain.
When asked if they support consanguinity in general, significant differences emerged between the 2 samples: 18.0% of the clinical sample supported consanguinity compared to 8.4% of the community sample. Furthermore, 20.3% of the clinical respondents reported that they would encourage their children to marry a relative, compared to 12.4% of the community respondents.
The data indicated that 87.5% of the clinical sample stated that consanguinity is common within their family, compared to only 20.8% of the community sample. Finally, only 39.8% of the clinical respondents considered it important to discuss consanguinity with their children before marriage, compared to 72.7% of the community respondents.
Significant differences between the 2 samples were found across 6 of the 7 examined variables (Table 2).
Comparison Between the Clinic and Community Samples Regarding the Consanguinity and Their Attitudes and Perspectives Toward Sociocultural and Health Issues.

Of the clinical respondents, 75.8% believed that a child could die due to a genetic disease, compared to 94.1% of the community respondents.
Regarding the relationship between consanguinity and reproductive loss, 33.6% of the clinical sample agreed, while none disagreed, and 66.4% were uncertain. In contrast, 30.7% of the community respondents agreed, 24.2% disagreed, and 45.1% were uncertain.
While most respondents agreed that consanguinity increases genetic defects in children, significant differences were found: 81.3% of the clinical sample agreed, with none disagreeing, whereas 77.9% of the community respondents agreed, while 24.2% disagreed.
Among the clinical respondents, 75.0% believed that children’s health problems could be attributed to consanguinity, compared to only 9.5% of the community respondents.
Respondents were asked whether they would find it acceptable to have a child with a 25% chance of being affected by a recessive genetic disorder if both parents carried a common pathogenic variant. In the clinical sample, 43.0% disagreed with this possibility, compared to only 18.3% of the community respondents.
Regarding prenatal testing, 33.6% of the clinical respondents said they would consider it if there was a 25% chance that the fetus would be affected, compared to 72.7% of the community respondents.
The only variable that showed no significant differences between the 2 samples was the perception of premarital carrier screening for common inherited genetic disorders. Most respondents (96.1% of the clinical sample and 94.8% of the community sample) considered premarital carrier screening a beneficial practice.
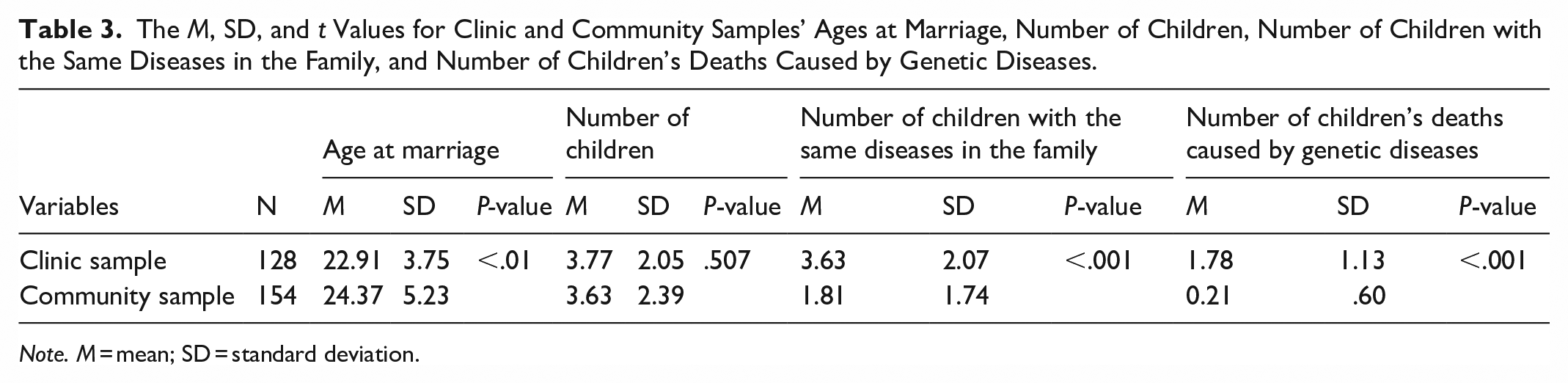
Several additional variables were analyzed to assess differences between individuals who married relatives and those who did not. These included age at marriage, number of children, number of children with the same diseases in the family, and number of children’s deaths due to genetic diseases.
Data revealed significant differences between consanguineous and non-consanguineous couples in terms of age at marriage, number of children with the same diseases in the family, and number of children’s deaths caused by genetic diseases. No significant differences were found in the total number of children. Consanguineous couples visiting the clinic tended to marry at a younger age, have a higher number of children affected by similar genetic conditions within the family, and were more likely to experience child loss due to genetic diseases compared to non-consanguineous families (Table 3).
The M, SD, and t Values for Clinic and Community Samples’ Ages at Marriage, Number of Children, Number of Children with the Same Diseases in the Family, and Number of Children’s Deaths Caused by Genetic Diseases.
Note. M = mean; SD = standard deviation.
Table 4 presents the relationship between the rate of consanguinity within respondents’ families and factors such as education, income, number of affected individuals in the family, and the number of children’s deaths due to genetic diseases.
The Relationship Between the Rate of Consanguinity in the Respondents’ Family and Some Social and Health Variables.

No relationship was found between the rate of consanguinity within a respondent’s family and family income. However, the results indicated an inverse relationship between consanguinity rate and education level. Conversely, a higher rate of consanguinity within families was associated with a greater number of individuals affected by the same genetic diseases and a higher rate of child mortality due to genetic conditions.
Discussion
Our data indicate that first-cousin marriage is the most commonly practiced form of consanguineous marriage among parents with at least 1 child affected by an inherited autosomal recessive (AR) genetic disease (78.1%), consistent with findings from previous studies.1,10,11,20 Most clinical respondents with affected children were married to close relatives. Within the clinical sample, 10.2% were married to second cousins, while 11.7% were married to third cousins. Despite the negative health impact on their affected children, clinical respondents maintained positive perspectives toward consanguinity. Compared to non-consanguineous couples, clinical respondents were more likely to perceive consanguinity as both common and increasing in society. A regional study found that individuals married to relatives and those with a high frequency of consanguineous marriages within their families exhibited significantly higher attitude scores in favor of such unions.21,22
Regarding family stability, clinical respondents were more supportive of consanguinity, believing it reduces the divorce rate in society. They felt that families would be more stable when couples are relatives, as this would lower divorce rates, though statistical evidence remains lacking. This belief was also reflected in a previous study conducted in Kuwait, where consanguineous spouses reported a higher degree of family stability compared to non-consanguineous families. 10 Similar findings have been observed in studies from other cultural contexts. 23
Despite their children’s inherited genetic diseases, clinical respondents indicated that consanguinity fosters family stability, and they were more likely to encourage their children to marry relatives. Additionally, clinical respondents were less inclined than non-consanguineous respondents to discuss consanguineous marriage with their children before marriage. Overall, the clinical sample viewed consanguinity positively from a sociocultural perspective.
Interestingly, clinical respondents believed that consanguinity could lead to the death of their children due to inherited genetic conditions, with an increased risk of reproductive wastage compared to the community respondents. However, they were also less inclined to consider prenatal testing than the community sample. Regarding awareness of the likelihood of passing genetic diseases to their children, the clinical sample was less likely to accept this possibility compared to the outsider respondents. These findings suggest that parents may struggle to acknowledge a hereditary explanation for genetic disorders, particularly if not all their children are affected. This perspective aligns with findings from a consanguinity study conducted in Saudi Arabia, where consanguineous families often attributed illness to religious or folk beliefs rather than genetic inheritance. 24
Increasing number of couples who are seeking premarital counseling in communities with high levels of consanguineous marriages, because of growing public awareness to prevent the occurrence of inherited genetic diseases in their offspring. 25 The results of this study showed that non-consanguineous couples are seeking more counseling compared with consanguineous partners. This might explain the strong belief of pursuing consanguineous marriage despite the increased risk of passing on inherited AR genetic disorders to their offspring. Such families prioritize their social lives and family ties to other potential health consequences in their future children. Consanguineous couples in our study got married at a younger age, which has been observed in other studies as well.10,26 This could be explained by the arranged marriage by the couple’s parents or families, not the spouses themselves. The older a person is, the more autonomy he could get in the marital process and choosing a partner outside the family circle. Our data showed that the number of affected individuals with the same disease in the family and the number of children’s deaths caused by genetic disorders are related to society’s high degree of consanguinity. In addition, this may also relate to the person’s level of education which can affect marital choices favoring consanguinity (Table 4), in parallel with the findings of a Saudi study, in which people with a lower level of education had a negative view toward consanguinity. 22 Such association has been supported by other studies from different cultures.10,27 -30
It is important to recognize the limitation of this study. The clinical sample was mainly made up of parents who attended outpatient clinics, which may have resulted in selection bias. However, the inclusion of both clinical and community samples broadens the diversity of participants. Additionally, the results may not be applicable to families with varied genetic origins due to the focus on consanguineous parents whose children have been diagnosed with autosomal recessive (AR) illnesses. To improve the findings’ external validity, future research should take into account more extensive recruitment tactics and longer data collection times. Also, the fact that the sample was limited to parents who were hired in February 2022 may have limited how broadly the results can be applied to other time periods.
Conclusions
The high level of inbreeding and rising consanguinity rates contribute to the high prevalence of inherited autosomal recessive (AR) genetic disorders in the MENA region, leading to significant morbidity and mortality. Nevertheless, consanguineous marriage remains widely practiced and highly favored in the region. Despite its well-documented reproductive risks, consanguineous couples perceive such marriages as beneficial, with advantages outweighing the potential health consequences.
It is important to note that this study was limited to parents with at least 1 child affected by an AR disease, compared to non-consanguineous families from the community. Given the continued prevalence of consanguinity in the MENA region, implementing and promoting national-level premarital carrier screening programs is a critical preventive measure to reduce infant morbidity and mortality. Further research is needed to explore the relationship between consanguinity and AR disorders in relation to variables such as ethnicity, geographic region, social group, and religious background.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580251366872 – Supplemental material for Attitudes of Parents With a Child With Autosomal Recessive Disease Toward Consanguinity
Supplemental material, sj-pdf-1-inq-10.1177_00469580251366872 for Attitudes of Parents With a Child With Autosomal Recessive Disease Toward Consanguinity by Yagoub Al-Kandari, Shaker Bahzad, Dina Ramadan, Hind Alsharhan, Mohammad Hussain and Waleed Al-Herz in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-2-inq-10.1177_00469580251366872 – Supplemental material for Attitudes of Parents With a Child With Autosomal Recessive Disease Toward Consanguinity
Supplemental material, sj-pdf-2-inq-10.1177_00469580251366872 for Attitudes of Parents With a Child With Autosomal Recessive Disease Toward Consanguinity by Yagoub Al-Kandari, Shaker Bahzad, Dina Ramadan, Hind Alsharhan, Mohammad Hussain and Waleed Al-Herz in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We would like to thank all participants for completing the survey
Ethical Considerations
The study was approved by The Research and Ethics Committee of the Ministry of Health in Kuwait, and by the Kuwait University Health Sciences Center Ethical Committee, in accordance with the Declaration of Helsinki.
Consent to Participate
Informed written consent was obtained from all participants (Ref.: VDR/EC/3544).
Author Contributions
YA: development of the research questionnaire, data analysis, and writing the first manuscript draft, SB: development of the research questionnaire and subjects enrollment, DR and HA: subjects enrollment, MH: development of the research questionnaire and data entry, and WA: development of the research concept, development of the research questionnaire, and subjects enrollment. All coauthors approved the submitted manuscript.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.