
Abstract
This study aims to develop a scale for patient evaluation of health literate health care organizations (PEHLHO) tailored to the Chinese context, addressing deficiencies in existing tools. It also examines the relationships between PEHLHO, communicative health literacy (CHL), and enhancement of perceived health literacy (EPHL) in major Chinese cities. This includes their correlation with perceived service quality (PSQ) and perceived a community with shared future for doctor-patient (PCSF) to improve healthcare service quality and patient experiences in China. A PEHLHO Scale was developed using focus group discussions and the Delphi method, with other scales adapted from existing instruments. This cross-sectional study was conducted through an online survey administered in major cities from February 17, 2024, to March 4, 2024, which included Shanghai, Chengdu, Guangzhou, Beijing, Wuhan, Xuzhou, Nanjing, Suzhou across China. A total of 6411 questionnaires were collected. Following quality control standards, the remaining sample of 5206 valid responses met the minimum recommended size for structural equation modeling. Data analysis was performed using SPSS and AMOS software. Exploratory factor analysis of the PEHLHO Scale revealed 3 factors: health education, involvement in diagnosis and treatment, and convenient services. All scales showed good validity and reliability. Informing patients about service fees received the lowest score. A Structural-Process-Outcome model confirmed that PEHLHO positively influences PCSF and PSQ, with CHL and EPHL as mediators. This model was validated in additional cities, demonstrating good generalizability. Enhancing patient health literacy should focus on systemic changes. Establishing health literate health organizations (HLHOs) can improve CHL, doctor-patient communication, and patient health literacy, ultimately optimizing healthcare service quality and doctor-patient relationships. Promoting (HLHOs) in China has significant potential and importance.
Keywords
Highlights
A novel Patient Evaluation Scale for Health Literate Health Organizations (PEHLHO) was developed using Delphi and focus group methods, tailored to the Chinese healthcare system.
The PEHLHO scale consists of three validated dimensions-Health Education, Involvement in Diagnosis and Treatment, and Convenient Services-demonstrating strong psychometric properties.
A Structural-Process-Outcome model revealed that PEHLHO may positively influence patients’ perceived service quality (PSQ) and perceived a community with shared future for doctor-patient (PCSF), mediated by communicative health literacy (CHL) and enhanced perceived health literacy (EPHL).
This study offers a new theoretical framework integrating structural, cognitive, and relational dimensions of healthcare quality, advancing the evaluation of organizational health literacy.
Promoting Health Literate Health Organizations may serve as a strategic approach to improving doctor-patient communication, strengthening health literacy, and achieving high-quality development in China’s healthcare system.
Introduction
Background
Most healthcare organizations focus on treating diseases rather than promoting health literacy. 1 Until recently the interest in health literacy was primarily concentrated in the United States and Canada, but over the past decade, it has become increasingly internationalized. 2 Since the concept of health literacy was introduced in 2005 in China, there has been a comprehensive effort to enhance the study and promotion of health literacy. 3 Health literacy is a comprehensive reflection of economic and social development, influenced by political, economic, educational, social, cultural, and health development levels. 4 Despite significant progress in improving health literacy in China over the past decade, by 2020, only about one-fourth of the population possessed basic health knowledge and skills. 3 Therefore, studying health literacy among the Chinese population holds significant practical importance.
Earlier definitions of health literacy focused on individuals’ ability to gather and process health information to make good decisions about health care and the individuals’ ability to use the information to promote and maintain good health. However, the concept of health literacy should consider that an individual’s health literacy varies dynamically in different contexts and environments. 5 Even if individuals have sufficient health literacy, they may struggle to access, understand, and apply health information and services in unfamiliar environments and during medical consultations filled with professional terminology, to make health decisions. 6 The responsibility for understanding and using services and information should shift from individuals to organizations. 7 The concept of health literacy has been expanded to encompass the functions of interaction between healthcare providers, healthcare systems, and patients. 8 Health literate health care organizations (HLHO) are proposed and defined as organizations that facilitate public to navigate, understand, and use information and services to care for their health.6,9 Therefore, compared to research solely focusing on individual health literacy, in-depth exploration of HLHO plays a more significant role in universally improving patient health literacy levels from a systemic perspective.
“Healthy People 2030” proposes definitions for both individual health literacy and organizational health literacy, collectively forming a comprehensive concept of health literacy. 10 The personal health literacy of patients is greatly influenced by healthcare institutions and their services. 11 In 2012, 10 attributes most relevant to HLHOs were identified. 6 These attributes focus on providing health information, training employees in health communication, addressing health literacy issues through specific leadership activities, and assessing whether the organizational environment is suitable for patients with different levels of health literacy. 12 Improving individual health literacy not only leads to better health outcomes but also reduces healthcare costs,3,13,14 thus saving resources to improve population-level health status.15,16 Therefore, a patient-centered service model must incorporate health literacy.
However, existing healthcare organization assessment tools for health literacy have certain limitations, such as lengthy items, 17 limited measurement dimensions, 18 direct translation versions that are not fully applicable to the Chinese cultural environment,19,20 and a lack of broader validation. 20 Few have undergone systematic adaptation and validation in Chinese cultural and clinical contexts. In addition, the study of HLHOs remains in its infancy in China. Therefore, to develop a new scientifically and practically applicable evaluation tool tailored to the Chinese context by combining the core attributes of health Literacy healthcare organizations and drawing on theoretical achievements from previous research,1,6,18,20 our research team employed CiteSpace for visual analysis to explore the current status and development trends of HLHOs in the preliminary phase of this project. Based on these findings, we conducted focus group discussions to initially construct a set of indicators for such institutions. Building on this foundation, the present study established the indicator weights through 3 rounds of the Delphi method combined with the Analytic Hierarchy Process (AHP), ultimately developing the new Chinese patient evaluation of health literate health care organizations scale (PEHLHO). Simultaneously, focusing on PEHLHO, communicative health literacy (CHL), and enhancement of perceived health literacy (EPHL) as core variables, this research would conduct surveys in 5 representative major cities across the eastern, western, southern, northern, and central regions of China. It would establish the relationship between these variables and the patient’s perceived service quality (PSQ) and perceived a community with shared future for doctor-patient (PCSF). Furthermore, validation would be conducted in 3 cities in the eastern province where the research team is located. The aim was to provide more precise and effective theoretical support and practical guidance for enhancing healthcare service quality and optimizing patient experiences in China.
Theoretical Framework
The Structure-Process-Outcome (SPO) model is widely applied and effective in evaluating healthcare service quality. 21 As is shown in Figure 1, the Structure refers to the attributes of the environment in which services are provided, including facilities and equipment, human resources and policies. The Process refers to the attributes of diagnostic and treatment activities (such as completeness, continuity, and functional quality). 22 The inherent linear interaction of the SPO model elucidates the state of the structure, process, and outcomes of the research object or the logical relationship among the three. 23 In research, the structure dimension can be used to analyze whether healthcare institutions support the practice of organizational health literacy. For example, whether healthcare institutions provide health information and services that are easy for patients to understand and use, and whether they have healthcare professionals with good health literacy. Secondly, the process dimension can understand the efficiency and quality of healthcare institutions in implementing organizational health literacy. Finally, the outcome dimension can evaluate the actual impact of organizational health literacy practices on healthcare service quality and doctor-patient relationships to verify the effectiveness of organizational health literacy practices. This study will adopt the SPO model to construct a structural equation model, to delve into the impact of organizational health literacy on healthcare service quality and doctor-patient relationships, and their related mechanisms.

The structure-process-outcome model.
Hypothesis Formulation
To better understand how PEHLHO, CHL, and EPHL improve healthcare service quality and patient experiences in China, this study proposes several hypotheses grounded in existing literature and theoretical frameworks. Specifically, the relationships between PEHLHO, CHL, and EPHL in major Chinese cities were examined, including their correlation with PSQ and PCSF.
The purpose of organizational health literacy is to enhance patient engagement in the health care process, improve the navigation system of healthcare, and enhance communication skills. 12 Research has demonstrated a significant correlation between the evaluation results of Health Literacy healthcare organizations and patients’ perceptions of the adequacy of information provided by hospitals. 19 When patients perceive that healthcare institutions are improving their health literacy levels, they may feel satisfied with the quality of services and communication from the healthcare institution. This satisfaction enhances patients’ confidence in seeking medical care and makes them more willing to engage in proactive communication with their doctors. Furthermore, the quality service provided by healthcare institutions make patients feel respected and cared for, thus they are more willing to actively express their health needs and concerns. Thirdly, by optimizing communication processes, providing clear and understandable health education, and encouraging patient involvement in treatment decisions, healthcare institutions can help patients improve their communication skills with doctors, thereby enhancing patients’ sense of participation and autonomy in the diagnosis and treatment process. Therefore, we proposed Hypothesis 1 (H1): PEHLHO is positively associated with CHL.
Building upon the role of PEHLHO in enhancing CHL, it is also important to explore its influence on patients’ PSQ, which refers to patients’ evaluation of physicians’ professional abilities, service attitudes, and treatment outcomes. Bopp has categorized healthcare quality into technical quality provided by healthcare providers and functional quality perceived by patients (healthcare consumers), considering the latter as more important in assessing healthcare quality than the former. 24 Healthcare institutions promoting enhancement of health literacy will facilitate the improvement of healthcare quality. 25 HLHOs aim to enhance patient access to information and services, making them more understandable and accessible.17,26 Enhancing organizational health literacy helps eliminate barriers and improve healthcare services for everyone. 27 When the PEHLHO is high, it indicates patients’ positive evaluation of physicians’ excellent performance in communication, health education, and other aspects. Therefore, we proposed Hypothesis 2 (H2): PEHLHO is positively correlated with PSQ.
Beyond improving patients’ PSQ, PEHLHO may also contribute to fostering a stronger relational bond between doctors and patients, namely PCSF. It represents a sublimation of the doctor-patient relationship. PCSF means that both doctors and patients share a consistent understanding of the disease, work together in coping with the disease, and jointly bear the responsibility for the treatment outcomes. 28 Enhancing patients’ health literacy levels seems to be a prerequisite for fostering the PCSF. In patient-centered healthcare models, health literacy is a fundamental element that empowers patients, enhances their participation, and activates them.29,30 When patients feel the doctor’s concern and understanding, they may trust the doctor. Environments with health literacy may help strengthen patients’ trust in doctors and the healthcare system. 31 Additionally, adjusting communication methods based on patients’ health literacy levels can enable patients to better participate in medical decisions. 32 Patients’ active participation can also enhance doctors’ attention to and sense of responsibility for patients’ conditions. Therefore, we proposed Hypothesis 3 (H3): PEHLHO is positively correlated with PCSF.
While PEHLHO may shape patients’ CHL, PSQ, and PCSF, the role of CHL itself in empowering health management deserves equal attention. It reflects patients’ confidence and ease in communicating with doctors. 32 Patients with higher CHL are more likely to ask questions, express opinions, and articulate their needs, 32 thereby obtaining more comprehensive and personalized medical advice and information. Conversely, patients with low literacy are less likely to ask questions to healthcare professionals, which may affect their ability to understand their medical conditions and treatments. 33 Additionally, doctors encouraging patient participation can increase the involvement of patients with sufficient functional health literacy. 34 Therefore, high CHL not only helps patients understand their medical condition and treatment plans but also enhances their self-management capabilities. Therefore, we proposed Hypothesis 4 (H4): Patients’ CHL is positively correlated with EPHL.
Alongside empowering patients’ health literacy, CHL may also serve as a key determinant in forming patients’ PSQ. Patients heavily rely on communication with healthcare professionals to understand and manage their health issues. 35 Patients with high CHL tend to have a more positive perception of medical services, thereby enhancing PSQ. Secondly, patients with high CHL are more likely to actively participate in medical decision-making, thus enhancing the perception of service quality. Additionally, patient health literacy appears to be a key factor in enhancing management skills that improve healthcare quality and increase healthcare professionals’ sense of responsibility and belonging. 25 Patients’ positive communication attitudes enable doctors better understand patients’ situations comprehensively and devise more precise treatment plans. Therefore, we proposed Hypothesis 5a (H5a): CHL is positively correlated with PSQ and Hypothesis 5b (H5b): CHL mediates the relationship between PEHLHO and PSQ.
As CHL may improve patients’ PSQ, the ensuing enhancement in physician–patient interactions contributes to the emergence of a novel relational paradigm—transforming the traditional provider–recipient model into a collaborative partnership characterized by shared decision-making and joint risk responsibility. Healthcare communication and patient engagement in healthcare are considered decisive factors in health literacy.2,36 Patients with high levels of CHL can increase trust in doctors and confidence in treatment plans, actively participate in treatment decisions, and strengthen cooperation with doctors. Secondly, through communication, patients acknowledge the collaborative relationship between doctors and patients, understand and accept the limitations of medicine, and jointly face the challenges of the disease. These factors together contribute to patients’ profound perception of PCSF. Lubasch et al 37 has argued that health literacy-sensitive communication is not only an important dimension of organizational health literacy but also has the potential to improve the doctor-patient relationships. Additionally, healthcare institutions play a crucial role in enhancing patient health literacy and promoting harmonious doctor-patient relationships. Doctors and patients are not just traditional roles of treatment providers and recipients but also partners in the healthcare process. The establishment of HLHOs will promote patients’ CHL, thereby enhancing their perception of PCSF. Therefore, we proposed Hypothesis 6a (H6a): Patients’ CHL is positively correlated with PCSF and Hypothesis 6b (H6b): CHL mediates the relationship between PEHLHO and PCSF.
Notably, CHL not only directly influences PSQ and PCSF, but may also indirectly enhance them by improving EPHL. Frosch and Elwyn 38 have proposed a “unified” vision of health literacy that emphasizes patient engagement to support patient-centered and responsive healthcare. This vision places health literacy within a broader context of participatory medical activities. 39 Patients with higher health literacy are more likely to understand and accept explanations and guidance from doctors, and are more likely to actively participate in treatment decisions, thus better appreciating the professionalism and care of doctors. Furthermore, by communicating in a “health literate” way addressing patients’ needs, health professionals can play a critical role in taking the patients’ health literacy into account and strengthening their health literacy. 32 Improving patients’ CHL may enhance their health literacy, thereby increasing their PSQ. Therefore, we proposed Hypothesis 7a (H7a): EPHL is positively correlated with PSQ and Hypothesis 7b (H7b) EPHL mediates the relationship between CHL and PSQ.
The enhancement of PSQ through EPHL represents only 1 facet of health literacy’s impact. More fundamentally, as a core tenet of PCSF, shared decision-making requires patients and providers to co-create understanding through improved health literacy. Making appropriate health decisions is not solely the responsibility of patients but requires shared responsibility with healthcare professionals. 40 Patients with higher health literacy are more likely to actively participate in treatment decisions, thereby experiencing the power of unity between doctors and patients more deeply. Furthermore, patients with higher health literacy better understand doctors’ diagnoses and treatment recommendations and are aware of the limitations of modern medical technology, thus establishing a closer and more trusting relationship. Research has showed that the higher the level of patient health literacy, the higher the trust in doctors and the healthcare system. 31 Additionally, patients’ CHL enhances their perception of PCSF by increasing their health literacy. Therefore, we proposed Hypothesis 8a (H8a): EPHL is positively correlated with PCSF and Hypothesis 8b (H8b): EPHL mediates the relationship between CHL and PCSF.
Methods
Questionnaire Composition
The self-designed questionnaire included items on age, gender, marital status, educational background, and the type of hospital visited most recently within the past 3 months. The scales included PEHLHO, CHL, EPHL, PCSF, and PSQ. The tool for PEHLHO was determined through rigorous focus group interviews and the Delphi method. The remaining scales were adopted from mature scales in previous literature. In addition to the questionnaire introduction and informed consent form, the questionnaire also provides special instructions for certain statements: (1) All responses should be based on the most recent medical visit within the past 3 months; (2) “My doctor” or “doctor” refers to the attending physician who treated me during this visit; (3) “Hospital” refers to the medical institution where the most recent medical visit took place. A general knowledge question was inserted into the questionnaire for participants to answer, in order to assess their response attitude and reduce common method bias. All scales used a five-point Likert scale (1-5), unless otherwise specified, with the options being: strongly disagree, disagree, uncertain, agree, and strongly agree.
Questionnaire Survey and Patient Involvement
In the preliminary phase of this project, our research team employed CiteSpace for visual analysis to explore the current status and development trends of HLHOs. Based on these findings, we conducted focus group discussions to initially construct a set of indicators for such institutions. Building on this foundation, the present study established the indicator weights through 3 rounds of the Delphi method combined with the AHP, ultimately developing the PEHLHO scale. Other scales were sourced from English literature. Prior to conducting the pilot survey, the research team translated the scale items into Chinese and modified them to adapt to the reading and comprehension habits of the Chinese population without altering the semantic meaning.
The pilot survey was conducted by the research team from February 13, 2024, to February 16, 2024. The research team made improvements based on the issues identified during the pilot survey to form the official survey questionnaire. The official survey was conducted by the research team from February 21, 2024, to March 4, 2024 through convenient sampling method online. Convenience sampling is a non-probability sampling method where data is collected from an easily accessible and available group of people. 41 In this study, convenience sampling was employed for several practical reasons. As exploratory research, it allows for the quick collection of preliminary data, which is essential for informing more rigorous future research. Additionally, due to resource constraints in terms of time, budget, and manpower, convenience sampling provides an efficient and cost-effective solution. 41 To compensate for the insufficient sample size in previous studies, 1 the research team distributed questionnaires online through Questionnaire Star (https://www.wjx.cn) to representative large cities in China. 42 The representative large cities included Shanghai (Eastern), Chengdu (Western), Guangzhou (Southern), Beijing (Northern), and Wuhan (Central). A total of 4018 questionnaires were collected. Additionally, this study selected 3 representative cities in Jiangsu Province (the province where the research team is located): Suzhou (Southern), Nanjing (Central), and Xuzhou (Northern) to validate the model again. A total of 2393 questionnaires were collected. Respondents were informed that they could voluntarily fill out the questionnaire, and all information provided would be kept confidential. Before answering the questionnaire, respondents were required to confirm their informed consent. The survey targeted individuals who had visited a hospital for medical treatment within the past 3 months. It is suggested that the ratio of the number of items to the sample size should be approximately between 1:5 and 1:10 when conducting factor analysis. 43 The total items in the questionnaire was 30. Therefore, the sample size in this study was deemed adequate for model construction.
This study was conducted in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines to ensure comprehensive and transparent reporting. 44 The STROBE checklist was completed and is provided as a Supplemental File.
Quality Control
The VIP feature of Questionnaire Star was utilized to establish rules (respondent’s city, minimum completion time, common sense question judgment, and selection of “informed consent”) to assist in screening out invalid questionnaires. Questionnaires from respondents whose cities were not among the specified cities were marked as invalid responses. Questionnaires with insufficient completion time were also marked as invalid responses. Questionnaires from respondents whose identities did not match (when the respondent selected “No” to the question “Have you visited a hospital for treatment of a newly developed illness in the past six months?”) were marked as invalid responses. Questionnaires with incorrect answers to the common-sense question (“What is the phone number for calling an ambulance?”) were marked as invalid responses. Respondents who selected “No” to the “informed consent” option had their survey automatically terminated. Additionally, manual verification was conducted to check for duplicate responses. Based on the filled-in personal identification code (first letter of the name + last 4 digits of the phone number), IP address, city, gender, age, and educational background, it was determined whether multiple responses came from the same person.
According to quality control standards, the Questionnaire Star system automatically eliminated 750 invalid questionnaires (668 questionnaires with a completion time of less than 200 s; 1 questionnaire with participant identity mismatch; and 81 questionnaires with incorrect answers to the general knowledge question). Additionally, 4 duplicate questionnaires were manually identified, resulting in a total of 754 invalid questionnaires. The remaining valid questionnaires totaled 3264, yielding an effective response rate of 81.23%. Furthermore, for the questionnaires distributed in 3 representative cities (Suzhou, Nanjing, and Xuzhou) in the southern, central, and northern regions of Jiangsu Province (the province where the research team is based) for hypothesis model validation, the Questionnaire Star system automatically eliminated 447 invalid questionnaires (364 questionnaires with a completion time of less than 200 s; 2 questionnaires with participant identity mismatch; and 81 questionnaires with incorrect answers to the general knowledge question). An additional 4 duplicate questionnaires were manually identified, resulting in a total of 451 invalid questionnaires. The remaining valid questionnaires totaled 1942, yielding an effective response rate of 81.15%.
A post hoc power analysis, conducted using G*Power (Version 3.1) as recommended by Balkin and Sheperis,45,46 revealed that the current sample size had a statistical power of 1.00 for detecting a small effect size of 0.15. 47 This was based on a Type I error rate of α = .05 and the number of predictors included in the regression models.
Measurement Scales
Patient Evaluation of Health Literate Health Care Organizations Scale (PEHLHOS)
Organizational health literacy (OHL) refers to the ability of health organizations to provide services and information that are easy to find, understand, and use for patients, helping them make decisions, and eliminating existing barriers.6,16 Farmanova et al 48 suggest that OHL has to acquire a new meaning and stretch beyond improving navigation, understanding, and use of information. Drawing on theoretical achievements and scales from previous studies,1,6,12,18 -20,26 this research, through multiple rounds of focus group interviews and 2 rounds of Delphi method, aims to construct a set of scientifically and practically applicable evaluation indicators for PEHLHO adapted to the Chinese context.
The Delphi method is a structured expert consultation technique that typically involves multiple rounds of anonymous questionnaires to collect expert opinions and gradually achieve consensus. 49 In this study, we employed a 2-round Delphi method, inviting 37 and 23 experts from various medical institutions and government agencies to provide consultations in each round. These experts primarily engage in research in the fields of clinical medicine, nursing, and public administration. After each round of surveys, we summarized and revised the feedback results to optimize the entries and ensure consensus among the experts.
To ensure the scientific rigor and reliability of the Delphi results, we implemented the following measures: (1) Expert Selection: Experts were selected based on predefined criteria, including professional background, work experience, and academic qualifications; (2) Anonymity and Multi-Round Feedback Mechanism: Anonymity was maintained throughout the consultation process to avoid inter-expert influence and promote independent judgment. After each round, the feedback was analyzed and the indicators were revised and optimized to gradually reach consensus; (3) Quantitative Evaluation: A quantitative assessment was used to measure expert participation and consensus. The response rate exceeded 70%, indicating high engagement. The authority coefficient (Cr), derived from the judgment basis (Ca), and familiarity degree (Cs), was used to assess the reliability of expert opinions, with Cr ≥ 0.70 indicating reliable expert input. The consistency and coordination of expert ratings were evaluated using the coefficient of variation (CV) and Kendall’s W. A significant W value (P < .05) indicated that expert opinions had reached consensus. Indicator Screening Criteria: Only entries with an importance score mean ≥ 4.50 and CV ≤ 0.25 were retained, and final adjustments were made based on experts’ qualitative feedback.
The final evaluation tool consists of a total of 11 questions, such as, “During the doctor-patient communication process, my doctor provided health education at an appropriate pace, with clear pronunciation and a gentle tone,” “During this visit, my doctor developed a follow-up plan for me to evaluate the treatment effectiveness,” “The online medical service platform provided by the hospital during this visit (such as appointment scheduling, payment, and accessing test reports) facilitated my medical treatment experience.” The evaluation tool is composed of 3 dimensions: “Health Education,” “Participation in Diagnosis and Treatment,” and “Convenient Services.” These items were assessed using a 5-point Likert scale with reverse scoring, where the options were sorted in sequence: Strongly agree (5 point), Agree (4 points), Uncertain (3 points), Disagree (2 points), and Strongly disagree (1 points). A higher total score across all items indicates a more favorable PEHLHO. After EFA and CFA, the Kaiser-Meyer-Olkin (KMO) for PEHLHOS was 0.920, respectively. The Cronbach’s α for them was 0.930, with CR of 0.900, 0.865, 0.887, and AVE of 0.645, 0.684, 0.723, respectively. Additionally, it had good discriminant validity and model fit.
Communicative Health Literacy Scale (CHLS)
This study adopted a 6-item short form of communicative health literacy (COM-HL) developed by Finbråten et al. 32 The scale exhibited a good single-dimensional structure. Personal health literacy is conditional and contextual.50,51 To better aid respondents in recalling their medical visits, this study added a situational prefix “During this medical visit. . .” before each item. These items were assessed using a 5-point Likert scale with reverse scoring, where the options were sorted in sequence: Strongly agree (5 point), Agree (4 points), Uncertain (3 points), Disagree (2 points), and Strongly disagree (1 points). The total score of CHLS ranges from 6 to 30, with higher total scores indicating stronger CHL. After EFA and CFA, the KMO for CHLS was 0.892, respectively. The Cronbach’s α for them was .904, with CR of .904, and AVE of .611. Additionally, it had good discriminant validity and model fit.
Enhancement of Perceived Health Literacy Scale (EPHLS)
This study utilized the subscale “Having Sufficient Information to Manage Health” from the health literacy questionnaire (HLQ) developed by Osborne et al. 52 To better facilitate respondents in recalling their medical visits, this study added a situational prefix “Through this medical visit. . .” before each item. Additionally, the language of the items was appropriately adjusted to suit the understanding of the Chinese population. Therefore, this variable was redefined as “Enhancement of Perceived Health Literacy.” These items were assessed using a 5-point Likert scale with reverse scoring, where the options were sorted in sequence: Strongly agree (5 point), Agree (4 points), Uncertain (3 points), Disagree (2 points), and Strongly disagree (1 points). The total score of EPHLS ranges from 4 to 20, with higher total scores indicating stronger EPHL. After EFA and CFA, the KMO for EPHLS was 0.803, respectively. The Cronbach’s α for them was .899, with CR of .903, and AVE of .700. Additionally, it had good discriminant validity and model fit.
Perceived a Community with Shared Future for Doctor-Patient Scale (PCSFS)
The PCSFS used in this study was developed by our research team previously. 28 The scale has demonstrated good validity and reliability. To enhance respondents’ recall of their medical visits, this study added a situational prefix “Through this medical visit. . .” before each item. These items were assessed using a 5-point Likert scale with reverse scoring, where the options were sorted in sequence: Strongly agree (5 point), Agree (4 points), Uncertain (3 points), Disagree (2 points), and Strongly disagree (1 points). The total score of PCSFS ranges from 3 to 15, with higher total scores indicating stronger PCSF. After EFA and CFA, the KMO for PCSFS was 0.742, respectively. The Cronbach’s α for them was .870, with CR of .872, and AVE of .695. Additionally, it had good discriminant validity and model fit.
Perceived Service Quality Scale (PSQS)
The perceived service quality scale used in this study was adapted from a short-form version of The perceived service quality scale (pSQ-SF6). 53 The pSQ-SF6 has demonstrated acceptable psychometric properties. To enhance respondents’ recall of their medical visits, this study added a situational prefix “During this medical visit. . .” before each item. For example, “During this medical visit, I believe this doctor possesses good professional competence.” These items were assessed using a 5-point Likert scale with reverse scoring, where the options were sorted in sequence: Strongly agree (5 point), Agree (4 points), Uncertain (3 points), Disagree (2 points), and Strongly disagree (1 points). The total score of CHLS ranges from 6 to 30, with higher total scores indicating stronger PSQ. After EFA and CFA, the KMO for PSQS was 0.879, respectively. The Cronbach’s α for them was .922, with CR of .924, and AVE of .671. Additionally, it had good discriminant validity and model fit.
Statistical Analysis
This study used SPSS 26.0 to conduct EFA, reliability analysis, descriptive analysis, and correlation analysis. Additionally, AMOS 24.0 was employed for CFA and to construct the structural equation model (SEM) to test the research hypotheses. Prior to analyzing the data, P-P plots, Q-Q plots to assess the normality of continuous variables.
Considering that the scale items included contextual language or rephrased statements, all scales need to undergo exploratory factor analysis and confirmatory factor analysis. In this study, 1632 sample were used for EFA and 1632 sample for CFA. This study first employed principal component analysis and varimax rotation to extract factors. An eigenvalue greater than 1 was used as the extraction criterion for the exploratory factor analysis. A KMO value greater than 0.6 and a significant result (P < .05) from Bartlett’s test of sphericity indicated that the data were suitable for factor analysis.54,55 The acceptable threshold for communality was set at 0.4. 56 The cumulative variance explained by the extracted factors was expected to exceed 50%. 57 After rotation, factor loadings were considered acceptable if they exceeded 0.4. 58 Through AMOS 24.0, CFA was conducted using the maximum likelihood estimation method to assess 3 aspects of construct validity: structural validity, convergent validity, and discriminant validity. Common indicators of structural validity included the root mean square error of approximation (RMSEA), standardized root mean square residual (SRMR), and goodness of fit index (GFI) and adjusted goodness-of-fit index (AGFI). Convergent validity was evaluated through factor loadings and composite reliability (CR), with standardized factor loadings required to be greater than 0.4 59 and CR values exceeding 0.6. 60 Discriminant validity was assessed using the average variance extracted (AVE), with acceptable values set at greater than 0.5. 61 Reliability analysis was examined to assess the internal consistency among scale items. Cronbach’s α over .7 was considered acceptable 62 and corrected item-total correlations (CITC) were expected to exceed 0.4. 63 In addition, this study conducted a Harman’s single-factor test to assess common method bias. If the variance explained by the first common factor was less than 50%, it was considered that no significant common method bias existed. 64
Through maximum likelihood estimation, structural equation modeling (SEM) was conducted through AMOS 24.0 to analyze the effects of individual indicators on the overall construct and the relationships between individual indicators. The evaluation of the model primarily focuses on assessing whether the fit is ideal. A smaller ratio of chi-square to degrees of freedom (χ²/df) indicates a higher model fit. GFI greater than 0.9 indicates good model fit. 65 As the number of parameters increases, the AGFI approaches 1, which is favorable for achieving ideal fit. Typically, an AGFI of 0.9 is used as a criterion for judgment. 65 A smaller value of SRMR indicates higher model fit. SRMR < 0.08 is generally considered an acceptable fit standard. 66 A larger value of root mean square error of approximation (RMSEA) indicates lower fit between the hypothesized model and the data. 66
Results
Reliability and Validity Analysis
Validity Analysis
The wording of each scale was modified according to the application scenarios of this study, thus exploratory factor analysis was conducted using maximum variance rotation method. The KMO values of all scales were greater than 0.7, indicating suitability for factor analysis. Except for the PEHLHO scale, factor extraction for other scales was based on the principle of eigenvalues greater than 1, resulting in the extraction of a single common factor. The cumulative variance explained by each scale ranged from 60.193% to 79.861%, reaching an ideal level. For the PEHLHO scale, fixed factor number of 3 was employed for factor analysis, resulting in a cumulative variance explained by the 3 common factors of 60.193% (Table 1). Overall, all scale structures were deemed reasonable, capable of effectively explaining latent factors (Table 1). Convergent and discriminant validity of all scales were examined using AMOS 24.0. The CFA of the 3-factor structure of the PEHLHOS has been shown in Figure 2. The results showed that the AVE for each scale ranged from 0.645 to 0.723, all exceeding 0.5, indicating good convergent validity (Table 2). To assess discriminant validity, we also performed the Heterotrait-Monotrait Ratio of Correlations (HTMT) analysis. All HTMT values were below the recommended threshold of 0.85, indicating satisfactory discriminant validity (Table 3). Additionally, indices such as SRMR, GFI, CFI, Incremental Fit Index (IFI), Relative Fit Index (RFI), and Normed Fit Index (NFI) all met relevant standards. Notably, the PCSF was confirmed as a saturated model. In summary, all scales demonstrated good validity (Table 4).
Exploratory Factor Analysis of Each Scale. a

PEHLHO = Patient Evaluation of Health Literate Health Care Organizations; CHL = Communicative Health Literacy; EPHL = Enhancement of Perceived Health Literacy; PCSF = Perceived a Community with Shared Future for doctor-patient; PSQ = Perceived Service Quality.
Convergent Validity of All Scales. a

PEHLHO = Patient Evaluation of Health Literate Health Care Organizations; CHL = Communicative Health Literacy; EPHL = Enhancement of Perceived Health Literacy; PCSF = Perceived a Community with Shared Future for doctor-patient; PSQ = Perceived Service Quality.

Confirmatory factor analysis of the 3-factor structure of the PEHLHO.a
Discriminant Validity Analysis of All Scales. a

PEHLHO (F1, F2, F3) = Patient Evaluation of Health Literate Health Care Organizations; CHL = Communicative Health Literacy; EPHL = Enhancement of Perceived Health Literacy; PCSF = Perceived a Community with Shared Future for doctor-patient; PSQ = Perceived Service Quality.
Confirmatory Factor Analysis for a Multi-factor Model. a

PEHLHO (F1, F2, F3) = Patient Evaluation of Health Literate Health Care Organizations; CHL = Communicative Health Literacy; EPHL = Enhancement of Perceived Health Literacy; PCSF = Perceived a Community with Shared Future for doctor-patient; PSQ = Perceived Service Quality.
Reliability Analysis
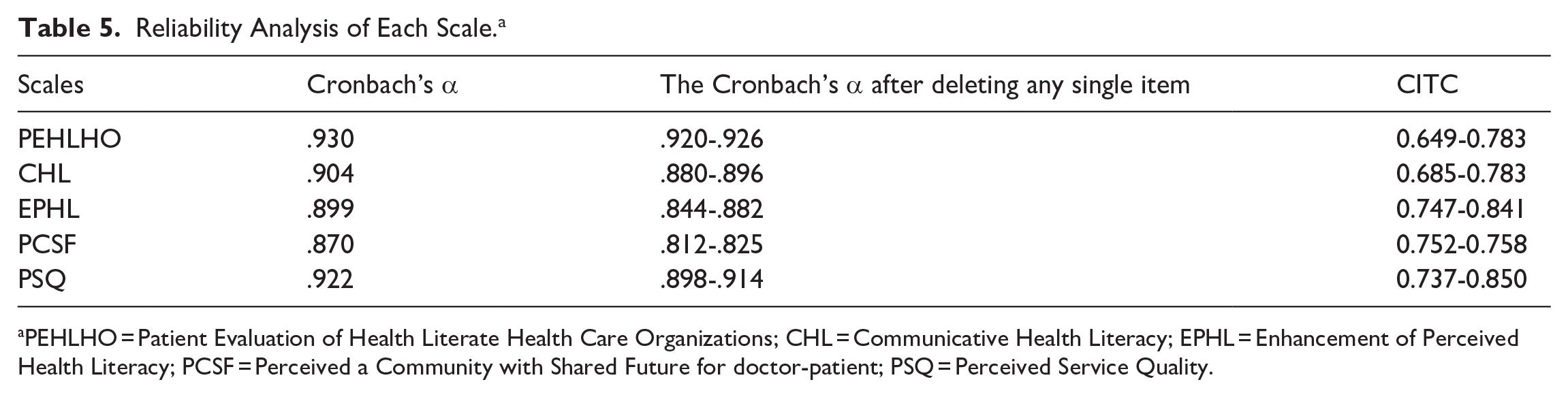
The Cronbach’s α coefficients of each scale ranged from .870 to .930, indicating good internal consistency within the scales. The changes in Cronbach’s α remained within an acceptable range even after deleting any item. Additionally, the composite reliability (CR) values of each scale were all greater than 0.6, reflecting their good composite reliability. In conclusion, the scales demonstrate good reliability (Table 5).
Reliability Analysis of Each Scale. a
PEHLHO = Patient Evaluation of Health Literate Health Care Organizations; CHL = Communicative Health Literacy; EPHL = Enhancement of Perceived Health Literacy; PCSF = Perceived a Community with Shared Future for doctor-patient; PSQ = Perceived Service Quality.
Common Method Bias
All variables were loaded into exploratory factor analysis to determine the number of factors required to explain the variance of the variables. 67 The results showed that the first principal component explained only 39.057%, which was below the recommended threshold of 50%, 68 indicating that no significant common method bias exists in the data.
Descriptive Analysis
Basic Demographic Information Statistics
The average age of participants was 36.09 ± 9.15 years, indicating that participants’ ages were predominantly concentrated between 30 and 45 years old. The majority of participants registered for general appointments (47.1%) and specialist appointments (44.3%), suggesting that most participants opt for routine outpatient care. County public hospitals (32.5%) and township health centers or community health service centers (24.8%) were the primary types of hospitals visited. The distribution of gender showed a slight predominance of female patients (52.9%), while the majority of participants were married (71.5%). Participants’ education levels were mainly concentrated at the level of junior college or below (46.9%) and undergraduate (46.9%), indicating that they predominantly had a moderate or lower level of education (Table 6).
Demographic characteristics of participants.

PEHLHO Scale Item Score Description
Through descriptive analysis of items in the PEHLHO scale, the item “During this doctor-patient communication, my doctor provided me with guidance on self-health management at home (eg, medication, exercise, nutrition, etc.).” received the highest average score (M ± SD: 3.75 ± 1.142), followed by the item “In this doctor-patient communication, the content of my health education from my doctor was easy to understand.” with the second highest average score (M ± SD: 3.74 ± 1.090). The item “During the doctor-patient communication, my doctor encouraged me to participate in the formulation of the treatment plan.” received the lowest average score (M ± SD: 2.59 ± 1.022; Table 7).
Descriptive Analysis of PEHLHO Scale Items. a

PEHLHO: Patient Evaluation of Health Literate Health Care Organizations.
Correlation Analysis
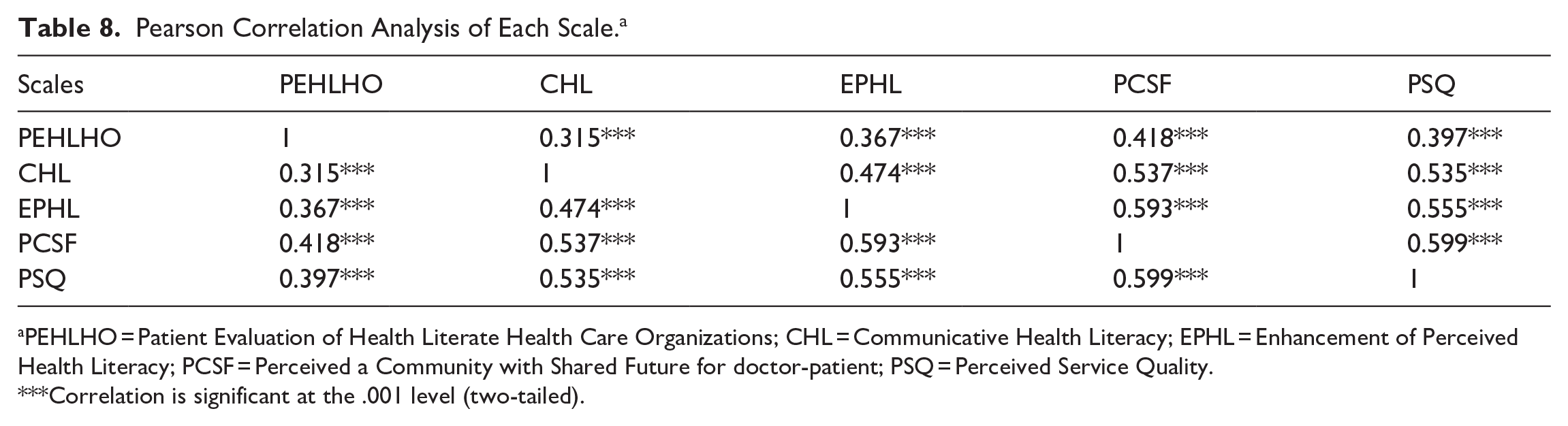
Through QQ plots, histograms, and the Kolmogorov-Smirnov test, it was determined that all data distributions are normal. Therefore, Pearson correlation analysis revealed significant positive correlations between all variables, with all showing significant differences (P < .001). The correlation coefficients ranged from .315 to .599. Specifically, there was a significant association between PCSF and PSQ (r = .599, P < .001). EPHL was closely related to PCSF (r = .593, P < .001). Furthermore, EPHL was also closely related to PSQ (r = .555, P < .001). CHL was closely related to PCSF (r = .537, P < .001) and PSQ (r = .535, P < .001; Table 8).
Pearson Correlation Analysis of Each Scale. a
PEHLHO = Patient Evaluation of Health Literate Health Care Organizations; CHL = Communicative Health Literacy; EPHL = Enhancement of Perceived Health Literacy; PCSF = Perceived a Community with Shared Future for doctor-patient; PSQ = Perceived Service Quality.
Correlation is significant at the .001 level (two-tailed).
Model Construction
Following the initial structural equation modeling (SEM) path diagram created using AMOS, the fit indices, unstandardized path coefficients, and standardized path coefficients were obtained. The CMIN/DF (Chi-square degrees of freedom ratio) 11.479, which exceeds the ideal standard of 2. However, considering the sample size of 3264 in this study, this may be the reason for the relatively high value. The SRMR (Standardized Root Mean Square Residual) is 0.037, lower than the standard of 0.08. The RMSEA (Root Mean Square Error of Approximation) is 0.057, also below the standard of 0.08. GFI (Goodness of Fit Index) is 0.912, AGFI (Adjusted Goodness of Fit Index) is 0.896, NNFI (Non-Normed Fit Index, also known as TLI) is 0.937, and CFI (Comparative Fit Index) is 0.943, all meeting the standard of 0.9, indicating that the overall fit of the structural equation model is ideal (Table 9). The standardized coefficients of each path are acceptable and statistically significant. Among them, CHL and EPHL have the highest standardized path coefficient (β = .424, P < .001; Table 10). Specifically, CHL acts as a mediator between PEHLHO and PSQ, as well as between PEHLHO and PCSF. EPHL mediates between CHL and PSQ, as well as between CHL and PCSF. Moreover, EPHL serves as a mediator between PEHLHO and PSQ, and between PEHLHO and PCSF (Figure 3).
Initial Model Fitting Statistics.

Standardized Coefficients in Initial Structural Equation Model. a

PEHLHO = Patient Evaluation of Health Literate Health Care Organizations; CHL = Communicative Health Literacy; EPHL = Enhancement of Perceived Health Literacy; PCSF = Perceived a Community with Shared Future for doctor-patient; PSQ = Perceived Service Quality.

Path diagram of structural equation model.*
Validation of the Model with a Small Sample Size
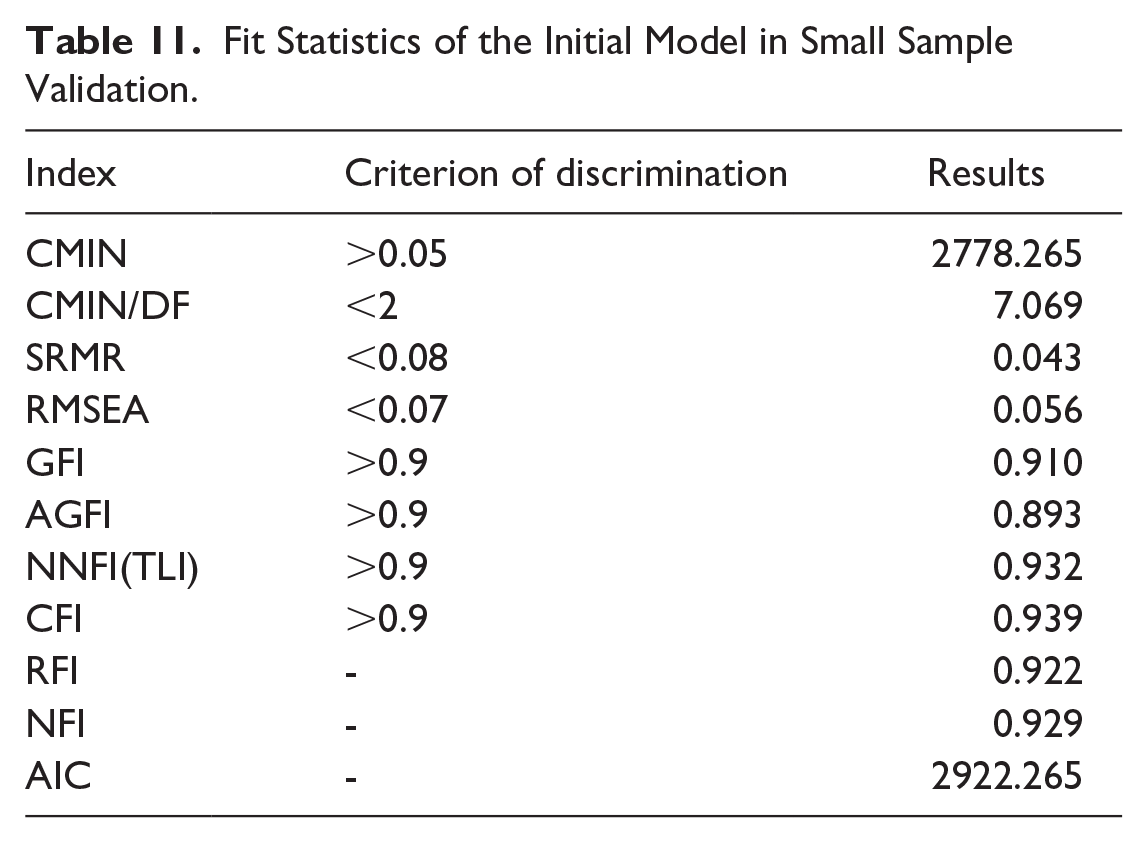
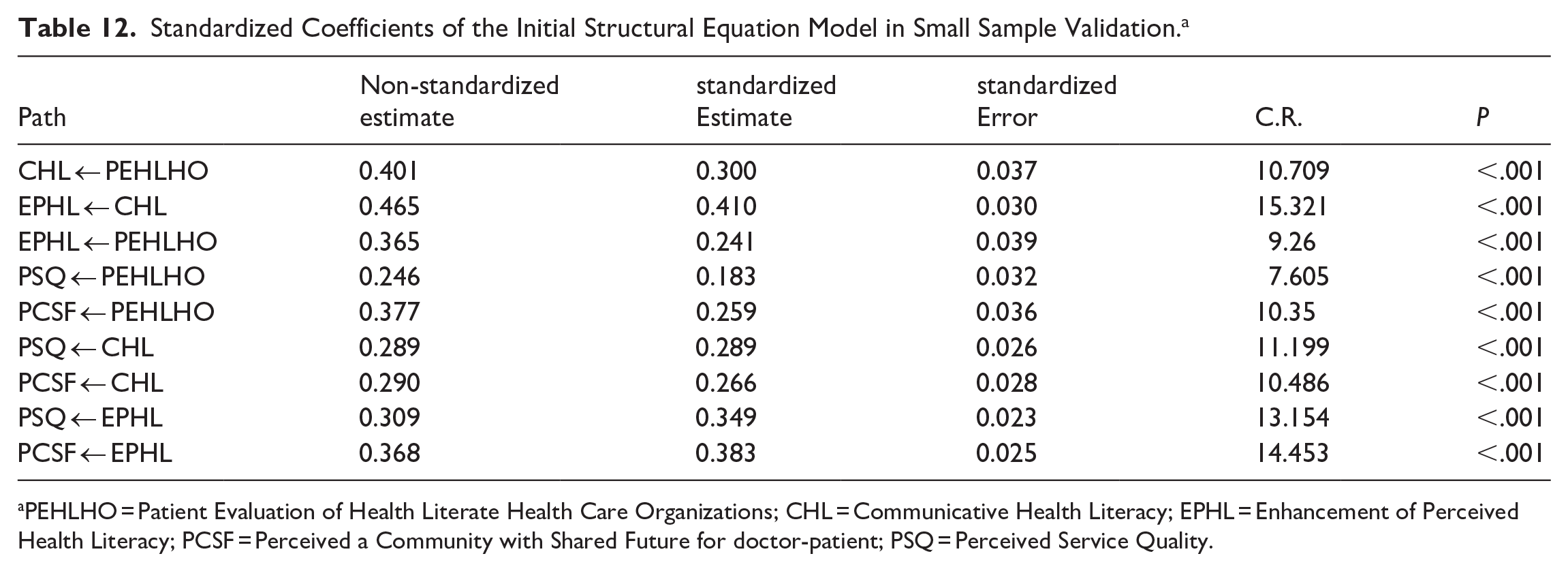
Validation of the structural equation model was conducted using a sample of 1942 participants from Jiangsu Province. The results of the study indicated that the model fit was satisfactory, with a CMIN/DF ratio of 7.069, consistent with the explanations provided earlier (Table 11). Furthermore, the proportions of the standardized coefficients for each path in the model with the small sample were similar to those of the established model. Overall, the model demonstrated good generalizability (Table 12).
Fit Statistics of the Initial Model in Small Sample Validation.
Standardized Coefficients of the Initial Structural Equation Model in Small Sample Validation. a
PEHLHO = Patient Evaluation of Health Literate Health Care Organizations; CHL = Communicative Health Literacy; EPHL = Enhancement of Perceived Health Literacy; PCSF = Perceived a Community with Shared Future for doctor-patient; PSQ = Perceived Service Quality.
Discussion
A HLHO must be capable of assisting individuals in accessing, comprehending, and utilizing services and information in the best possible manner, regardless of their literacy levels. 69 This study has innovatively constructed a HLHOs evaluation system in China and, for the first time, developed a PEHLHO-PSQ/PCSF model. In this study, the PEHLHO scale includes 3 dimensions: health education, accessibility of services in diagnosis and treatment, and accessibility of services. This scale demonstrates good reliability and validity. Transparent disclosure the service fees to patients is one of the 10 attributes of a HLHO. 6 By understanding the service fees, patients can better grasp their health status and medical needs, thereby making informed health decisions. However, in this study, this score for transparency in service fees was the lowest. The SPO model was applied in this study to construct the PEHLHO—PSQ/PCSF framework. The results of this study indicate that PEHLHO may positively influence PCSF and PSQ, while CHL and EPHL play mediating roles in this process. At the same time, CHL and EPHL may also positively influence PCSF and PSQ.
Under the positive influence of PEHLHO, CHL and EPHL come into play. In many cases, individual health literacy can develop as organizational health literacy improves.70,71 Organizational health literacy can be considered the “how-to-implement” of patient-centered care, 48 the strategy and the catalyst for building supportive culture, supportive systems, policies and practices, and an effective workforce. 72 The health education, diagnostic support, and convenient services provided by medical institutions enhance patients’ communication abilities with healthcare providers, thereby promoting understanding of physician advice and treatment plans. Simultaneously, the organizational environment can compensate for patients’ limited health literacy. 73 Besides physical environment support, HLHOs also exert indirect influence through healthcare personnel on patients. Improving healthcare professionals’ and organizations’ understanding of health literacy is a key factor in helping individuals achieve positive health outcomes. 10 With these efforts, patients’ perceived health literacy continues to improve, enabling them to have a deeper understanding of their health status and actively participate in the treatment and health management process.
PEHLHO may positively influence PCSF and PSQ. In this process, CHL and EPHL play an intermediary role. Organizational health literacy is considered a significant determinant of patient satisfaction and engagement. 74 When patients hold positive evaluations of medical institutions in terms of organizational health literacy, they often have better understanding and management of their health conditions, thus enhancing trust and cooperation with the medical institution. This enhanced trust and cooperation contribute to building closer doctor-patient relationships. Medical institutions committed to implementing best practices in health literacy are expected to enhance the overall quality of healthcare services. 25 The more positively patients evaluate health literacy medical organizations, the more they perceive the services provided by the medical institution as professional, effective, and humane. With increasing PEHLHO, their perceptions of service quality also correspondingly improve. 25 Furthermore, improvements in organizational health literacy not only help address patient health literacy issues but also lead to better health outcomes for them. 75 These positive outcomes will further promote the harmonious development of doctor-patient relationships and the continuous improvement of service quality.
CHL and EPHL may positively influence PCSF and PSQ. Patient-physician communication is a key determinant of good doctor-patient relationships. 76 As CHL and patient health literacy improve, communication between patients and physicians becomes smoother, and patient participation in decision-making becomes more active. This conducive communication environment enables patients to better understand the health information and advice provided by doctors, thereby enhancing their confidence in treatment and compliance. Additionally, health literacy-sensitive communication, supported by physicians, influences patient empowerment. 18 When patients perceive more understanding and support from doctors during communication, they are more inclined to view doctors and medical institutions as partners in facing illness and pursuing health together. The establishment of such a partnership not only contributes to improving the quality of medical services but also deepens trust and cooperation between patients and doctors. This trust and cooperation are at the core of PCSF.
In summary, the establishment of HLHOs not only improves doctor-patient relationships and enhances the quality of medical services but also lays the foundation for building a more harmonious and efficient healthcare system. However, implementing organizational health literacy faces numerous challenges, such as lack of time and funding, 77 and cultural change.78 -80 Promoting organizational health literacy practices requires multiple, simultaneous, and thorough changes. 48 Scholars suggest 3 steps to promote organizational health literacy practices to facilitate organizational change: (1) Encourage leadership to promote health literacy; (2) Develop a vision for health literacy transformation and effectively communicate it throughout the organization; (3) Provide training and education for all staff to ensure a smooth transition. 80 Some scholars propose that a healthcare system level effort is needed a systemic approach to enhance communication practices and standards, verbal/written communication skills, and patient knowledge and engagement, and that there is a need for the healthcare system to consider health literacy as an organizational priority, that is, be responsive. 12 In China, the promotion of HLHOs has not been fully implemented. Organizational health literacy culture should be integrated as part of management’s efforts to improve service quality. 25 This study suggests that promoting HLHOs in China should be included in development strategies, strengthened with policy guidance and financial support, enhanced through cross-departmental cooperation and resource integration, and leveraged with modern technology to improve promotion effectiveness.
Theoretical Implications
This study utilized various methods such as the Delphi method, focus group interviews, and on-site surveys to compile a new evaluation scale for HLHOs in China. This scale encompasses multiple dimensions and indicators, enabling a more comprehensive and systematic assessment of the service capabilities and levels of medical institutions in terms of health literacy. Secondly, based on the SPO model, a model for PEHLHO-PSQ/PCSF was constructed, revealing the inherent connections among these aspects. By combining quantitative and qualitative research methods, this study provides a new theoretical framework for assessing and optimizing the service quality of medical institutions.
Practical Implications
The evaluation system for HLHOs developed in this study provides specific directions and pathways for improvement for medical institutions. By assessing medical institutions across the dimensions of health education, participation in diagnosis and treatment, and convenient services, medical institutions can clearly understand their shortcomings in providing services and information that are easy to access, understand, and use. Subsequently, they can formulate targeted improvement measures. This will help medical institutions enhance patient satisfaction and trust, improve doctor-patient relationships, and simultaneously enhance the quality and efficiency of medical services.
Limitations
This study is a cross-sectional study, which poses certain limitations in causal inference. However, the study effectively validated the evaluation scale for PEHLHO, a process that covered 5 representative cities in China and underwent additional validation in 3 other cities, ensuring the cultural adaptability of the scale in China. Moreover, based on this scale, the study constructed a model for PEHLHO-PSQ/PCSF, which exhibited high stability. This provides a solid theoretical foundation for future causal inference studies. Furthermore, in constructing the aforementioned model, the study primarily utilized quantitative analysis methods, which rely more on previous literature and scale item inferences when explaining causality. However, to ensure the accuracy and reliability of the study, focus group interviews and the Delphi method were employed in compiling the evaluation scale for patient assessments of HLHOs. These methods provided more solid empirical evidence during implementation, aiding in better interpretation of the relevant results. Lastly, to cover a wider range of representative cities, the study employed online questionnaire surveys. Despite implementing strict quality control standards, there may be biases in the survey respondents due to the unique nature of online communities. This aspect requires attention and improvement in future research endeavors.
Conclusion
Patients’ positive evaluations of HLHOs have a positive impact on PCSF and PSQ, with CHL and EPHL playing an intermediary role in this process. Enhancing organizational health literacy can effectively strengthen the ability of medical institutions to provide easily understandable information and accessible services to patients, improve patients’ health literacy levels, optimize doctor-patient communication, enhance service quality, and improve doctor-patient relationships. Promoting HLHOs in China can become an important pathway for the high-quality development of healthcare.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251351178 – Supplemental material for The Construction Level of Health Literate Health Organizations and Its Impact on Patients’ Health Literacy: Based on Self-Determination Theory and Structural Equation Modeling
Supplemental material, sj-docx-1-inq-10.1177_00469580251351178 for The Construction Level of Health Literate Health Organizations and Its Impact on Patients’ Health Literacy: Based on Self-Determination Theory and Structural Equation Modeling by Renjie Lu, Jing Zhou, Jiaying Ge, Xiyang Xia, Chao Lei, Shenyu Zhao, Dan Shen, Xiaoyu Wang, Jiaqian Chang, Yang Chen and Lingmin Hu in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580251351178 – Supplemental material for The Construction Level of Health Literate Health Organizations and Its Impact on Patients’ Health Literacy: Based on Self-Determination Theory and Structural Equation Modeling
Supplemental material, sj-docx-2-inq-10.1177_00469580251351178 for The Construction Level of Health Literate Health Organizations and Its Impact on Patients’ Health Literacy: Based on Self-Determination Theory and Structural Equation Modeling by Renjie Lu, Jing Zhou, Jiaying Ge, Xiyang Xia, Chao Lei, Shenyu Zhao, Dan Shen, Xiaoyu Wang, Jiaqian Chang, Yang Chen and Lingmin Hu in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
Not applicable.
Ethical Considerations
The study was approved by the ethics committee of Changzhou Maternity and Child Health Care Hospital (No. 2023[26]) in 2023.
Consent to Participate
All participants’ informed consent was obtained online before the survey.
Author Contributions
Renjie Lu: Conceptualization, Methodology, Investigation, Formal Analysis, Funding Acquisition, Writing-Original Draft, Writing -Review & Editing. Jing Zhou: Data Curation, Writing-Original Draft, Writing -Review & Editing, Validation. Jiaying Ge: Visualization, Writing-Original Draft, Writing -Review & Editing. Xiyang Xia: Writing -Review & Editing. Chao Lei: Investigation, Writing -Review & Editing. Shenyu Zhao: Writing -Review & Editing. Dan Shen: Writing -Review & Editing. Xiaoyu Wang: Writing -Review & Editing. Jiaqian Chang: Writing -Review & Editing. Yang Chen: Conceptualization, Methodology, Validation, Supervision. Lingmin Hu: Conceptualization, Methodology, Funding Acquisition, Supervision.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Hospital Management innovation research project of Jiangsu Hospital Association in 2023 [JSYGY-3-2023-247], and Open Research Fund Program of Changzhou Institute for Advanced Study of Public Health, Nanjing Medical University [CPHS202303], and research program on policy of traditional Chinese medicine for deepening reform of healthcare system in 2024 of the Monitoring and Statistical Research Center of the National Administration of Traditional Chinese Medicine [YGZXKT2024124], and the Science and Technology Major Project of Changzhou Municipal Health Commission [ZD202323], and Top Talent of Changzhou “The 14th Five-Year Plan” High-Level Health Talents Training Project [2022CZBJ084], and Changzhou Maternal and Child Health Hospital 2024 scientific research project [HL202407].
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that there is no conflict of interest.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy restrictions.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.