
Abstract
With rising life expectancy, older adults’ dependency on children for care increases, though the level of support varies based on children’s individual capabilities. In multi-child households, highly educated offspring are often considered to prioritize personal utility, opting to substitute caregiving with financial assistance. However, as parental health declines, their support evolves to stronger reciprocal motivations. Employing a fixed-effects model clustered at the family level and data from the 2018 China Family Panel Studies, this study analyzes intergenerational support within multi-child households, specifically examining how parental health mediates support from highly educated offspring to older adults across urban and rural contexts. Findings highlight the substantial impact of 2 dimensions of parental health on intergenerational support patterns, with highly educated children in urban and rural areas exhibiting different responses. In urban settings, highly educated children tend to provide less caregiving support, increasing their involvement only in response to severe parental depression. In contrast, children of rural areas face greater expectations of reciprocity, offering both financial and caregiving support when their parents’ health deteriorates. This study once again provides empirical support for the health benefits of parental investment in children’s education. Moreover, these findings offer insights for formulating public policies aimed at addressing inequalities in care for older individuals.
Keywords
In multi-child households, the assumption that highly educated offspring prefer providing financial assistance over caregiving overlooks the fact that they often utilize their resources to support their parents’ well-being, especially during critical periods of health decline. Nevertheless, existing literature offers limited insight into how parental health moderates the relationship between children’s education and the support they provide in multi-child households, and almost no research has addressed this issue in China.
This study is the first in China to explore how intergenerational support patterns among highly educated offspring vary according to the health conditions of older parents in multi-child households, emphasizing urban-rural differences and 2 dimensions of parental health.
The findings deepen our understanding of how highly educated offspring respond to parental health and offer insights for developing public policies to address disparities in care for older people.
Introduction
With the general increase in life expectancy, reliance on children for informal care will intensify, compelling countries worldwide to depend more on this form of support. 1 In Chinese society, caregiving practices for older adults are deeply rooted in a profound cultural legacy, reflecting a longstanding obligation that reinforces strong, supportive familial bonds. This characteristic stems from the limitations of China’s social security system and the enduring, millennia-old family traditions that continue to shape care norms. While substantial research exists on vertical intergenerational parent-child relationships, there is a notable lack of studies on the horizontal division of care within multi-offspring households. 2
In the limited literature on care divisions within multi-child families, studies have highlighted strategic decision-making regarding the allocation of caregiving responsibilities and potential conflicts arising from these dynamics.3 -6 Notably, the relationship between children’s education and parental care provision patterns has garnered considerable attention from scholars as an important facet of caregiving allocation. Despite some differing opinions, researchers generally agree that parents tend to receive daily care from co-residing children with lower educational attainment, as these children often face fewer geographic and professional constraints. In contrast, children with higher educational attainment—typically college-educated—are often engaged in stable yet demanding jobs and live farther away, making them more likely to provide financial assistance rather than direct caregiving.7 -10 The mainstream explanation for this phenomenon is the rational choice theory,11,12 which posits that the family functions as a unit seeking to maximize collective benefits. In this arrangement, the most educated children tend to evade the responsibility of direct caregiving support, opting instead for the more convenient financial assistance, which is less time- and emotion-intensive. This portrayal fails to capture the dynamic reality in which highly educated children actively leverage their assets to enhance parental well-being—especially during critical periods of health decline—as research indicates they offer multifaceted support, including health-related information and financial assistance.13 -15
A more nuanced examination of how children’s individual endowments shape the division of intergenerational support is necessary, with particular attention to the mediating role of parental health in care dynamics. In families with multiple children, caregiving roles are adapted based on various factors, including the characteristics of both parents and children. 16 Parental health emerges as a critical factor when analyzing the internal dynamics of familial care. There is limited literature on how parents’ health influences the relationship between children’s education and the support they provide in multi-child households, and almost no research has addressed this issue in China. In a rapidly modernizing society characterized by pronounced urban–rural disparities and a heavy reliance on adult children for caregiving, exploring how highly educated children in China respond to variation in parental health—as evidenced by their diverse support patterns—will offer valuable new insights for this research field.
This study is the first in China to explore how intergenerational support patterns among highly educated offspring vary based on the health conditions of older parents in multi-child households, with a focus on urban-rural differences and 2 dimensions of parental health. Analyzing variations in intergenerational support provided by higher educated offspring under varying parental health conditions strengthens empirical evidence for the health benefits of parental investment in children’s education. Additionally, comparing urban and rural support patterns in response to parental health sheds light on how modernization shapes intergenerational relationships. These findings also deepen our understanding of how higher educated offspring responds to parental health and provide insights for developing public policies to address disparities in care for older people.
Theoretical Framework and Literature Review
Rational Choice Theory
The rational choice theory serves as a prominent framework adopted by researchers to analyze parental support in multi-child families. Its core premise is that individuals aim to make rational decisions to maximize their benefits.17,18 Consequently, the distribution of parental support responsibilities among adult children is shaped by the opportunity costs associated with providing care. These perceived costs arise from factors such as each child’s proximity to the parent and competing obligations (eg, employment, marriage, and childcare), which implicitly raise the costs of caregiving.3,16
Education is closely related to an individual’s occupational status and serves as an effective indicator for measuring opportunity costs. Children with higher educational attainment experience both increased opportunity costs and unique advantages when it comes to caring for their parents. On one hand, the cost of providing caregiving is higher for these individuals due to heightened time constraints and potential income loss, making them less likely to provide in-person caregiving. In particular, the physical and time demands of being present with their parents have intensified amidst rapid urbanization.19,20 On the other hand, they often possess greater financial resources, allowing them to offer financial assistance to their parents as a substitute for caregiving support. 21 In contrast, offspring with lower educational attainment tend to contribute more directly to their parents’ day-to-day caregiving. With fewer career-related time constraints, these individuals are often more available to provide in-person caregiving support. This dynamic is particularly evident in rural areas, where highly educated offspring often relocate in pursuit of educational or employment opportunities far from home.
In rational cooperative family decision-making, support roles are allocated according to offspring attributes: caregiving, with higher time demands, is typically assigned to less-educated offspring due to their lower opportunity costs, whereas highly educated offspring tend to provide financial support, thereby highlighting the inherent trade-off between caregiving and financial assistance. Studies on caregiving divisions within multi-child families support this rationale. Lei et al found that Chinese parents are more likely to reside with offspring who have lower educational attainment, 22 while Liu and Hu demonstrated that those with lower education are more likely to assume caregiving roles, 23 confirming the rational choice theory. Ma and Wen further revealed that younger, healthier parents tend to live with more educated offspring, while older or less healthy parents cohabit with less educated offspring, particularly in rural areas. 24
Reciprocity Theory
Intergenerational support is a complex process, shaped by motivations grounded in altruistic, exchange, and normative theories. 16 Influenced by Confucian family values, Chinese parents often make excessive investments in their children’s upbringing, fostering a sense of obligation among highly educated children to reciprocate their parents. 25 Researchers who advocate the reciprocal viewpoint contend that children’s provision of intergenerational support is primarily a reaction to their parents’ needs, 26 particularly heightened during periods of health decline. Prior research revealed that children intensify their support when their parents experience deteriorating health or when they encounter challenges in performing activities of daily living (ADLs) and instrumental activities of daily living (IADLs).27 -29 Moreover, Reyes and Shang suggested that parents and children are inclined to maintain or reduce geographical distances between them as a response to the parents’ declining health. 30
Presently, few studies have examined the correlation between offspring’s educational attainment and their responsiveness to caregiving of older people. Patterson investigated the connection between educational attainment and attitudes toward providing Instrumental Activities of Daily Living (IADL) care, 31 finding that individuals with a bachelor’s degree are more inclined to offer comprehensive family IADL support, including caregiving and financial assistance. This aligns with previous research by Li and Jin, 2 which noted an increased reliance on higher-achieving children during parental health decline, and Fingerman et al observed that these offspring often provide greater benefits. 32 Additionally, despite the higher caregiving costs associated with highly educated offspring, the greater parental investment during the early stages of life places these children under greater moral pressure to reciprocate.32,33
However, the impact of children’s education on parental health is more commonly explored. These children face greater pressure to reciprocate and possess greater resources and skills for managing health issues. This includes accessing and spreading health knowledge,34 -36 promoting parents’ health behaviors, 37 and enhancing parents’ psychological states. 13 Their focus on their parents’ health often translates into tangible assistance in day-to-day life. 38 Additionally, offspring with higher levels of education typically have greater financial resources, enabling them to cover their parents’ extensive medical and care expenses.
Greater pressure to reciprocate, combined with the superior advantage of high-achieving offspring, leads to more attentive care for their parents’ health. This attentiveness plays a pivotal role in shaping intergenerational interactions and influences the processes of intergenerational support. As the health conditions of parents evolve, the division of parental support—initially established based on rational choice when parents are healthy—tends to yield to intergenerational reciprocity. Consequently, when the health of parents is considered, offspring with higher education levels are more inclined to provide increased levels of both caregiving and financial support. Based on the rational choice and reciprocity theory, divergent perspectives on the behavior of highly educated offspring lead us to the following hypotheses.
Hypothesis 1a: When accounting for parental health factors, offspring with higher education levels are consistently less likely to provide caregiving support and more likely to offer financial assistance than their less-educated siblings.
Hypothesis 1b: When accounting for parental health factors, offspring with higher education levels are likely to provide similar or even greater levels of caregiving support and financial assistance than their less-educated siblings.
Urban-Rural Disparities
Modernization theory suggests that technological and economic progress erodes traditional values. Rising individual wealth and the expansion of social security further diminish reliance on family support. Moreover, an increased societal emphasis on personal independence diverts attention from family obligations, raising concerns about the decline of filial piety and the viability of informal caregiving. This trend is evident in reduced intergenerational co-residence and diminished obligations to assist older parents in more developed regions, 22 mirroring broader societal shifts toward modern, individualized lifestyles.
Due to historical reasons, urban and rural areas are at distinctly different stages of modernization, a divergence largely shaped by the household registration (Hukou) system. This system allocates social resources in a way that grants urban residents greater access to employment, housing, education, pension insurance, and healthcare, thereby reinforcing China’s urban-rural divide. 39 The unequal distribution of welfare resources has led to higher levels of modernization in urban populations, resulting in significant urban–rural disparities in the health and economic conditions of older parents. These disparities, in turn, influence intergenerational relationships and shape children’s responses to parental health conditions.
In urban areas, where Western influences are strong, parents often require less support from their children due to improved economic conditions and access to market-based care services. In contrast, rural regions—characterized by more adverse economic conditions and a lack of formal care systems—are more dependent on the informal caregiving provided by their children. Moreover, urban environments, with their distinct employment patterns and health risks compared to rural areas, shape distinct responses to both mental health and functional status challenges. Mental health awareness is notably higher in urban areas, 40 while rural parents, often engaged in long-term strenuous labor, tend to prioritize functional status, making them more sensitive to immediate challenges in daily functioning.
Furthermore, in rural areas, children with higher education levels represent a distinct group of upwardly mobile individuals. They have successfully navigated systemic disadvantages imposed by the household registration system, including limited educational resources and impoverished environments, which restrict opportunities for development. 41 The families’ exceptional efforts to facilitate their upward mobility impose significant pressure on highly educated offspring in rural settings, increasing the demand for both caregiving and financial support for their parents. However, the physical distance between highly educated rural offspring and their parents’ residence poses significant challenges in providing consistent support. Considering rural-urban disparities and the mental and functional health of parents, as well as 2 forms of intergenerational support, we propose the following hypotheses.
Hypothesis 2a: Highly educated children in urban and rural areas place varying emphasis on their parents’ mental health and functional status.
Hypothesis 2b: Highly educated children in urban and rural areas differ in their likelihood of providing both caregiving and financial support to their parents.
Data and Method
Data
This study utilizes data from the China Family Panel Studies (CFPS), 42 conducted by Peking University’s China Social Science Survey Center. CFPS utilizes multi-stage, probability proportional to size (PPS) sampling to collect individual, family, and community data across 25 provinces, covering 95% of China’s population, reflecting socioeconomic, educational, demographic, and health dynamics. Biennial follow-ups track the 2010 CFPS participants, with data from the 2012 to 2020 follow-up waves; however, due to significant missing values in key variables, the 2020 data was excluded, and this analysis focuses on the 2018 sample for its recency. Samples are included only if they contain complete data on key aspects of parent-child relationships. Furthermore, to minimize bias associated with co-residing adult children, the analysis was confined to families where every adult child lived separately from their parents. Additionally, we excluded only children and those under 20 who are economically dependent, while ensuring that each household includes at least 2 adult children. The final sample consists of 3135 parents (756 urban and 2379 rural) and 8671 children (2000 from urban parents and 6671 from rural parents).
Methods
Many researchers use fixed-effects models to examine intergenerational interactions in multi-child families by nesting children within their parents.3,22 -24,43 The fixed-effects model addresses omitted variable bias by utilizing information from at least 2 individuals within the same group. It eliminates all time-invariant features from the estimation equation, whether measured or not. 44 In our analysis, some unmeasured family characteristics, such as parenting atmosphere, upbringing environment, and genetic factors, influence both the level of child education and the provision of intergenerational support. Nesting children within parents enables control for unmeasured family characteristics and facilitates the analysis of child-specific effects. The equation for the fixed-effects model is as follows:

Here, i represents parents, j represents individual children,
One significant drawback of the fixed-effects model is its inability to study characteristics that vary between groups but remain constant within individuals in those groups. The random-effects model does not have this limitation, but it requires unobserved effects to be independent of other variables, 43 which is often difficult to satisfy. In addition to the fixed-effects model, this study employs the random-effects model to verify the results. However, the comparison of the coefficients between the fixed-effects and random-effects models did not pass the Hausman test. Pooled OLS estimation produced similar results. This study follows the relevant EQUATOR guidelines for cross-sectional studies.
Measures
The core variables in this study include parental support variables, the educational attainment of offspring, and parental health indicators. Echoing the previous discussion on the ‘financial assistance substituting caregiving support’, parental support variables, based on parents’ self-reports, include 2 indicators: caregiving support, reflecting the frequency of care provided by children, and financial assistance, representing the monthly financial support given to parents, log-transformed for analysis. Caregiving support is encoded from 1 to 7, where ‘no caregiving’ is coded as 1, and codes 2 to 7 correspond to caregiving frequencies of ‘once every few months’, ‘once a month’, ‘2-3 times a month’, ‘1-2 times a week’, ‘3-4 times a week’ and ‘almost every day’, respectively. A higher numerical value indicates a higher frequency of caregiving support. Treating this categorical variable as continuous simplifies the interpretation of results in a fixed-effects model, and this approach is also observed in similar research.18,30 The educational attainment of offspring is categorized into 3 groups: junior high school or less, high school, and associate degree or higher, with the ‘junior high school or less’ group serving as the reference category.
Parental health indicators encompass both mental health and functional status. For mental health, the CFPS uses the 8-item version of the CES-D, including mood, loneliness, and sadness, coded from 1 to 4, with scores summed across the 8 items. A higher total score indicates a deeper level of depression. The reliability of the depression scale is α = 0.79. Functional status indicators use an adapted Nagi scale, assess parents’ mobility and functional limitations, encompassing 7 categories: outdoor activities, eating, kitchen tasks, using public transport, shopping, laundry, and cleaning. Each activity is coded as 1 or 0 (0 indicating the ability to perform the activity and 1 indicating an inability), with scores summed. The reliability of the functional ability scale is α = 0.83. A higher total score indicates lower functional capability. Control variables encompass the children’s age, gender, marital status, individual Hukou, whether they are the oldest or youngest, and whether parents provide household assistance.
Results
Descriptive Analyses
Table 1 presents a descriptive comparison of urban and rural differences in the characteristics of parents and their children. The upper half of Table 1 summarizes the overall characteristics of children, comparing all indicators between urban and rural groups as classified by parental Hukou status. Among the pooled sample, the percentage of those who have completed high school is 15%, while those with associate degree or higher is 14%. There is a significant urban-rural educational disparity: children with parents holding urban Hukou have an educational level well above the average, with 26% having completed high school and 28% having associate degree or higher. In contrast, children with parents holding rural Hukou fall below the average, with 12% having completed high school and 9% having associate degree or higher.
Urban-Rural Comparison of Parental and Offspring Characteristics.

Note. Continuous variables are presented as means, while categorical variables are presented as proportions.
The study finds that the average age of all children is 42.64 years, with 91% being married and 31% holding urban Hukou. A total of 17% of these children have previously received household assistance from their parents. The average score for care frequency, coded from 1 to 7, is 1.73, below the mean, largely due to living separately. The average financial assistance provided is 164.14 yuan. Differences exist between children of parents with different Hukou regarding age, individual Hukou status, family ranking, receiving parental assistance, and frequency of caregiving support. Urban children provide higher financial and caregiving support, which may correlate with better economic conditions in cities and closer living proximity.
The lower section of Table 1 describes parental characteristics. On average, parents are nearly 69 years old with 4.73 years of education. The average score for parental depression is close to 14, slightly below the median of 16. The average score for functional ability is 0.49, indicating generally adequate functional capacity. Comparing urban and rural settings, urban parents are found to be older, more educated, and have significantly better mental and physical health than their rural counterparts.
Urban Parents’ Health Moderating the Relationship Between Child Education and Parental Support
Table 2 presents the associations between the educational attainment of children in urban families and their caregiving and financial support to parents, controlling for family-level characteristics with a fixed-effects model. The results in Table 2 reveal that, in models M1 and M2 which do not include parental health status, children with education levels of associate degree or higher are more likely to provide financial assistance to their parents compared to those with junior high school or less, though the impact of education on caregiving support frequency is not significant. Upon including parental depression and functional ability in M3, the effect of higher education on caregiving frequency becomes significantly negative, and the interaction term between higher education and parental depression is significantly positive. This suggests that highly educated urban children, who typically provide care less frequently, may increase their caregiving in response to parental depression symptoms. This finding, partially contradicting rational choice theory, indicates that these children are particularly concerned with their parents’ mental health and increase caregiving frequency when it deteriorates. The caregiving support frequency of highly educated children exceeds that of their less educated counterparts when parental depression scores exceed 14 (0.065 * 14 − 0.879 > 0). Besides, the interaction between parental functional ability and children’s education is also positive in M3, but not significant, potentially due to the more apparent nature of decline in functional ability, which easily draws attention from all children.
Fixed-Effects Models of Urban Parents’ Health Moderating the Relationship Between Child Education and Parental Support.

Note. Values in parentheses represent standard errors.
P < .05. **P < .01. ***P < .001.
After controlling for the interaction between parental health indicators and education in M4, the effect of children’s higher education on financial assistance becomes non-significant. Meanwhile, the interaction terms for an associate degree or higher with depression and functional ability are positive, though not statistically significant. Incorporating parental health indicators alters the relationship between urban children’s education and the 2 forms of parental support, only partially supports Hypothesis 1a. The changes in primary effects and interaction terms highlight the distinct dynamics of urban areas, where highly educated children prioritize caregiving in response to parental depression, reflecting the progressive attitudes and affluence typical of urban environments.
The association of other child variables with intergenerational support yields notable findings. Parental household assistance positively correlates with caregiving support, suggesting that parental assistance prompts filial care behaviors, as identified by Xu. 46 As children age, their intergenerational support for parents declines, likely due to the increasing demands of their own nuclear families. Those in intact marriages tend to increase financial assistance to parents while reducing caregiving support, although these effects are not statistically significant. Meanwhile, individuals with urban Hukou tend to provide less caregiving support but more financial assistance, a pattern that aligns with rational choice theory and reflects the typically high economic status of non-agricultural children. It should be noted that Table 2 focuses on children of urban parents, and rural household children are a minority in this sample. Additionally, sons provide less caregiving and financial support compared to daughters, aligning with current trends of daughters’ active role in parental support activities, as noted by Gruijters. 47 Eldest children increase caregiving support and decrease financial assistance for parents, although these results are not significant. The association between youngest children and parental support is similarly non-significant.
Rural Parents’ Health Moderating the Relationship Between Child Education and Parental Support
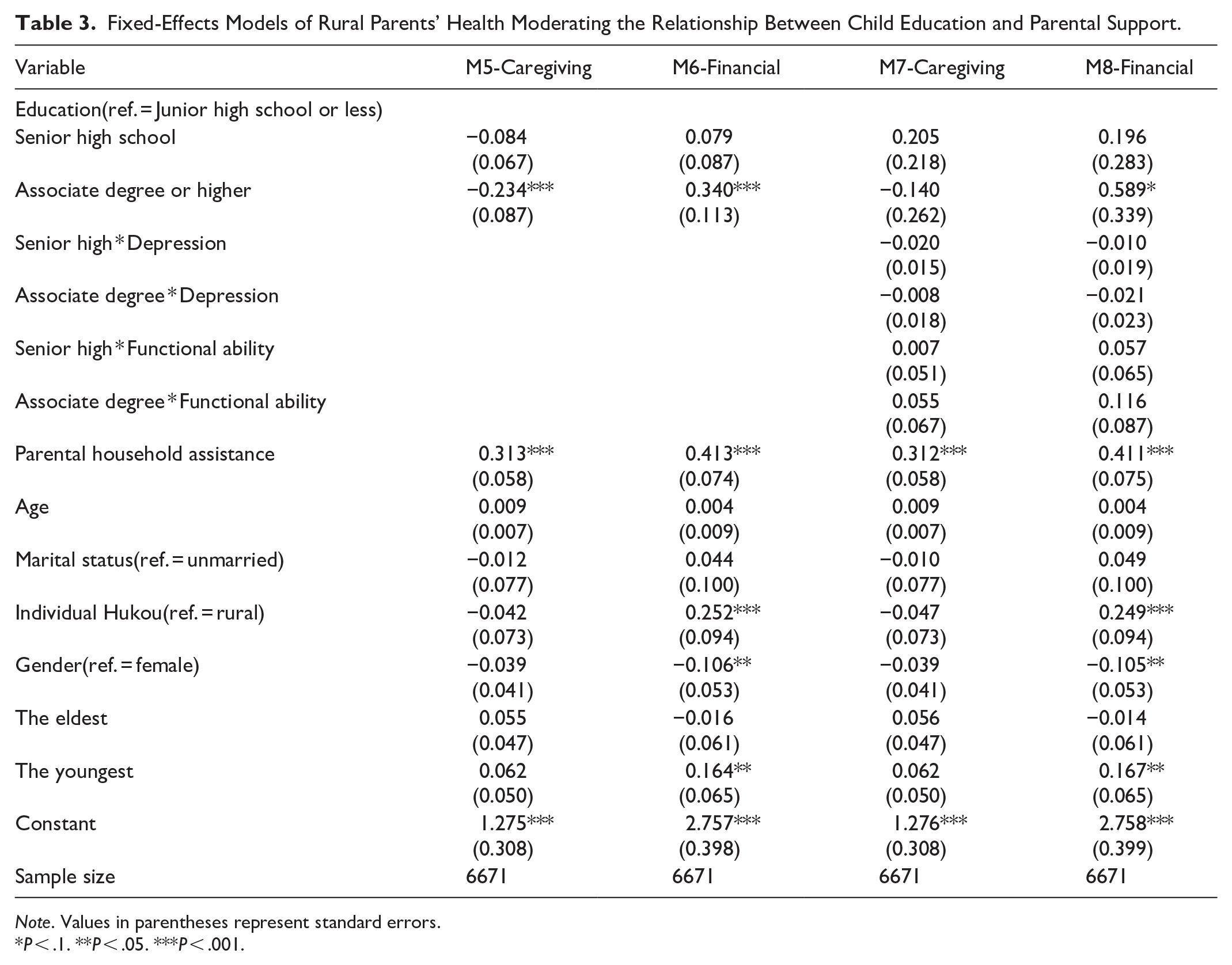
Table 3 presents the associations between the educational attainment of children in rural families and their caregiving and financial support to parents, controlling for family-level characteristics with a fixed-effects model. The results show that in models M5 and M6, which do not account for parental health status, children with education levels of associate degree or higher significantly increase financial assistance and decrease caregiving support compared to those with junior high school or less, fully aligning with rational choice theory. Upon including parental depression and functional ability in M7, the primary negative effect of caregiving support for higher-educated children remains but becomes non-significant, and the interaction terms with parental depression and functional ability are also not significant. Nevertheless, highly educated children from rural areas continue to provide significantly greater financial support than their less educated counterparts in M8. Children from rural areas with higher education levels are more likely than their less-educated counterparts to respond to poor parental health by providing greater financial assistance while maintaining comparable levels of caregiving support. This behavior supports Hypothesis 1b, which predicts that higher-educated offspring provide similar or even greater levels of caregiving and financial support when considering parental health. Furthermore, extending this perspective, highly educated rural offspring provide more comprehensive support to their parents compared to their urban counterparts, aligning with Hypothesis 2b.
Fixed-Effects Models of Rural Parents’ Health Moderating the Relationship Between Child Education and Parental Support.
Note. Values in parentheses represent standard errors.
P < .1. **P < .05. ***P < .001.
Among children from rural areas with higher education, the interaction between the depression indicator and children’s higher education is consistently negative and non-significant. This contrasts with urban samples, as the greater emphasis on parents’ psychological well-being in urban areas may lead to heightened concern among children for their parents’ mental health. Additionally, although the interaction between functional ability and education is not significant in rural samples, its consistently positive direction implies that the physically strenuous nature of rural work may lead highly educated rural children to be particularly attentive to their parents’ functional status. Altogether, urban children and children living in rural areas respond differently to various dimensions of parental health: urban children prioritize mental health, while the latter focus more on functional status, align with Hypothesis 2a.
Figure 1 presents the main effect of higher education and its interaction with parental health on support provided to parents, highlighting 2 key ‘health dimension-parental support pairs’ that best illustrate urban-rural contrasts: depression-caregiving support and functional ability-financial assistance relationships. The top panel shows that urban children with higher education increasingly provide caregiving support as their parents’ depression symptoms worsen, whereas children of rural areas exhibit less concern for their parents’ mental health. The bottom panel demonstrates that a decline in parental functional ability correlates with increased financial support from children, with children of rural areas consistently offering more financial assistance than their urban counterparts.

Presents the main effect of higher education and its interaction with parental health on support provided to parents, differentiated by urban and rural areas. The top image illustrates the main effect of higher education and its interaction with parents’ depression scores on the frequency of caregiving provided, based on estimates from Model 3 in Table 2 and Model 7 in Table 3 (yurban = 0.065x − 0.879; yrural = −0.008x − 0.140; x represents the depression score, while yurban and yrural indicate different levels of caregiving provided). The bottom image depicts the main effect of higher education and its interaction with parents’ functional ability on the financial assistance provided, based on estimates from Model 4 in Table 2 and Model 8 in Table 3 (yurban = 0.133x − 0.023; yrural = 0.116x + 0.589; x represents the functional ability score, while yurban and yrural indicate different levels of financial assistance provided).
The relationship between other control variables of children from rural areas and intergenerational support suggests that parental household assistance not only increases the frequency of caregiving but is also positively associated with financial assistance. Children from rural areas with non-agricultural Hukou offer significantly more financial support but less caregiving. The challenging process of obtaining urban Hukou produces effects comparable to those of higher education. In addition, the roles of age, birth order, marital status, and gender among children from rural areas closely resemble those observed among their urban counterparts. Due to data limitations, our model omits key variables emphasized in prior research, particularly geographic proximity, which is strongly linked to intergenerational support. Prior studies indicate that higher educational attainment among children is often linked to greater geographic distance from parents, reducing caregiving support (eg, Reyes and Shang, 2023) and increasing financial assistance (eg, Liang et al., 2023). The absence of the proximity variable may lead to an underestimation of caregiving support and an overestimation of financial contributions.
Discussion
While informal caregiving by children is common, in societies with underdeveloped public welfare systems like China, parents often invest heavily in their children’s education with the expectation of reciprocal care in old age. This expectation varies between urban and rural areas, as rapid urbanization widens disparities in both socioeconomic levels and cognitive perceptions. This study employs fixed-effects model to analyze the relationship between children’s individual endowments and their provision of financial and caregiving support in response to parental health, within a social context marked by pronounced urban–rural disparities. It specifically examines how parental mental health and functional status conditions influence intergenerational support patterns among highly educated children. The results highlight the crucial moderating role of parental health in shaping intergenerational support dynamics, with distinct patterns emerging between urban and rural settings.
In the urban sample, highly educated children initially offer less caregiving support, increasing their involvement only as parental depression worsens. Furthermore, once health indicators are accounted for, the previously significant financial assistance becomes non-significant. In contrast, the rural sample shows a different pattern: although highly educated children initially seem to reduce caregiving, once parental health is considered, highly educated children provide caregiving at levels comparable to their less educated counterparts while consistently offering more financial assistance. While these variations in intergenerational support of highly educated children reflect a practical calculation of caregiving costs, they also highlight the role of reciprocity, with higher education potentially reshaping parental support perceptions toward parental health.
From the way educated children adapt their support patterns to parental health, it appears that they are more attentive and sensitive to their parents’ health. This underscores the significant value of investing in children’s education as a strategy for enhancing the well-being of older adults in countries with limited public welfare systems. Furthermore, the findings challenge the static view of caregiving arrangements presented by the rational choice theory, instead supporting the notion that intergenerational exchanges are flexible and adapt to parental needs and children’s strengths. Similar conclusions are drawn by Fingerman et al, Li and Jin, and Vergauwen and Mortelmans, 48 highlighting a more dynamic and responsive interaction between educated children and their aging parents.
Besides, variations in parental support between urban and rural offspring highlight the influence of modernization on intergenerational relationships. The differing stages of modernization in urban and rural areas shape the behavior of highly educated children in multi-child households, reflecting individual actions influenced by diverse economic conditions, health perceptions, and pressures of reciprocity. Consequently, we observe that highly educated urban children and children living in rural areas respond differently to 2 aspects of their parents’ health, leading to distinct patterns of parental support. Urban, highly educated offspring generally adopt a more rational caregiving approach, facing less pressure for financial support and showing greater sensitivity to their parents’ mental health needs. In contrast, rural offspring may face stronger expectations of reciprocity and may therefore be less driven by rational calculation, 49 leading them to offer more comprehensive support as their parents’ health declines.
It’s important to acknowledge that variations in children’s education and responsiveness to parental health can exacerbate disparities in older adults’ access to caregiving resources. 50 To mitigate these inequalities, community-based programs that support families from diverse socio-economic backgrounds are essential. Furthermore, there must be increased emphasis on mental health awareness for older individuals and their children in rural areas, ensuring a more holistic well-being for rural older adults. Moreover, attention must be given to the challenges faced by highly educated children in balancing parental support responsibilities with their careers, providing them with greater support to fulfill their caregiving duties. Such initiatives will contribute to a more just and inclusive caregiving environment.
The limitations of this article include the following: First, intergenerational support decisions are based on the overall family circumstances, yet key information is often missing. For instance, the data typically report only one parent’s health status, parental support is based on self-reports, and factors such as the use of market-based care services are not considered. Future analyses should take a more comprehensive view of family situations. Second, the differences in depression symptoms between urban and rural areas suggest that varying health indicators significantly influence how offspring perceive and respond to their parents’ conditions, potentially leading to different levels of intergenerational support. 37 Thus, it is essential to include variables reflecting offspring’s perceptions of their parents’ health to better analyze their responses. Lastly, a more detailed longitudinal dataset is needed to fully understand how parental health impacts children’s support. This dataset should include variables such as the residential distance between parents and each child, the caregiving responsibilities of adult children for their own young children, and the changes in these factors over time, along with longitudinal data on parental health and the care provided by children. This is especially important in multi-child families, where caregiving adjustments are made dynamically. Addressing these research gaps will clarify the processes and outcomes of sibling-based division of intergenerational support.
Conclusion
This article examines how highly educated offspring provide financial and caregiving support in response to parental health, revealing urban–rural disparities and variations across distinct dimensions of parental health. The conclusions of this study can inform public policy development to reduce inequalities in the care of older adults. When formulating family support policies, it is essential to consider how factors such as children’s education influence the care provided to older parents facing health challenges. Policies should prioritize the protection of older adults who lack sufficient support from their children, rather than solely focusing on low-income families with older adults in poor health. Future research should longitudinally explore the relationship between family care and overall parental well-being, as well as its evolving interaction with external factors such as the formal care market.
Footnotes
Ethical Considerations
This study was approved by the Peking University Biomedical Ethics Committee at Peking University (Approval No. IRB00001052-14010).
Consent to Participate
Written informed consent was obtained from all participants (or their legal guardians) prior to enrollment in the study. The data are de-identified by removing all personal identifiers using standard anonymization procedures.
Consent for Publication
All authors have read and approved the final manuscript and give their consent for its publication.
Author Contributions
LL led the data analysis. CJY and ZLH participated in the data analysis. LJX designed the study and wrote the manuscript. LJX, LL, and ZLH participated in the revision of the manuscript. All authors have read and approved the final manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was financially supported by the Ministry of Education’s Major Research Project in Philosophy and Social Sciences of China, “Research on Reconstructing the Family Doctor Service Model in the Context of Regional Healthcare” (Project No. 20JZD027), and the Three-Year Action Plan for the Development of Shanghai’s Public Health System (2023–2025), Key Discipline Construction Project (GWVI-11.1-47, GWVI-11.1-44, GWVI-5), China.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.