
Abstract
Advance Directives (ADs) are essential in end-of-life care, enabling individuals to retain autonomy when they can no longer make decisions. However, data on ADs prevalence and influencing factors in different populations (acutely ill, chronically ill, and general) remain limited globally. This review aims to assess the prevalence of ADs in acute and chronic care settings and the general population and identify factors influencing their completion. A systematic review was conducted using PubMed, Scopus and Cochrane Library databases for English-language studies on ADs prevalence up to December 2023. The Joanna Briggs Institute Critical Appraisal Tool was adopted for bias assessment, and information on potential moderating factors—such as age, gender, income, education, marital status, capacity for self-determination and cancer diagnosis—was collected. Analysis involved a random-effects meta-analysis, subgroup evaluations and meta-regressions, with multimodel inference for multivariate assessment. Out of 239 studies covering 8.9 million people, 73.6% were from North America and 18% from Europe. The estimated global ADs prevalence was 0.26 [95% CI: 0.23-0.30], with higher rates among chronically ill individuals and the general population. Positive associations with ADs completion were found for age, education level and white ethnicity, while male gender showed a negative association. Key influencing factors were white ethnicity, education and cancer diagnosis. These findings suggest that ADs completion remains low, relatively unchanged over time, and potentially unequal, especially among non-white, less-educated and non-cancer patients. Increased efforts to raise ADs prevalence are needed, particularly in underrepresented groups.
Keywords
Advance Directives (ADs) are crucial for ensuring self-determination when decision-making capacity is lost. Despite systematic reviews on ADs in specific settings or on a national basis, there is limited knowledge about their prevalence among patients in acute or chronic care facilities and the general population. Additionally, the factors influencing ADs completion need further exploration.
The majority of the data on advanced directives completion originates from North America and Europe. This study’s meta-analysis estimates the global prevalence of ADs at 0.26. Influential factors include white ethnicity, educational level and the presence of oncologic disease.
Interventions aiming at increasing the prevalence of ADs are crucial, particularly among non-white ethnic groups, less educated populations and patients with non-oncologic conditions.
Introduction
Life and death are inextricably linked, with their relationship being influenced by cultures, religions, science, medicine, values, beliefs and laws, thus making end-of-life (EOL) care approach still tricky to discuss even in our days. 1 This is especially true in response to the increased sophistication and prevalence of advanced medical technology that, despite bringing many benefits on one side, could result in the prolongation of a possibly unqualified life on the other. 2
Since the Universal Declaration of Human Rights in 1948, science and medicine have transitioned towards a patient-centred vision, promoting an active approach to the choices for their health, even if with substantial variability in constitutional laws and healthcare systems worldwide. 3
The wind of change and the discussion on the ownership of EOL decisions started in the US more than 50 years ago, but it was only in 1990 with the Patient Self-Determination Act that individuals’ rights on this topic began to be recognised. In the rest of the world, legislation started later, around the new millennium: in Australia, the first law was enacted 1998; in the UK, in 2005 and in Japan, in 2017.
However, some Asian, African, and Central American countries have little to no data reported on the topic, while others have a law on EOL care but no electronic national registry of people who have effectively written their wishes. 4
Advance Directives (ADs) are legal documents where a person specifies the actions that can or cannot be taken for their health if they are no longer able to make decisions for themselves. 5 They mostly take the form of a living will or a health care proxy or surrogate (the agent the person in charge of the ADs notifies as the one to make decisions for them when no longer able on their own, also called Durable Power Of Attorney or Enduring Guardian). Therefore, ADs preserve individual autonomy and self-determination when the capacity to make decisions is lost. Moreover, ADs have been significant in reducing hospitalisations and unwanted invasive procedures, increasing the use of hospice and palliative care, ensuring concordance between patients’ end-of-life wishes and the care provided, and ameliorating the caregivers’ stress.6,7
Although some systematic reviews have examined ADs on a national scale or within specific settings,8 -11 there is limited overall knowledge about the prevalence of ADs completion among patients affected by acute or chronic diseases, as well as within the general population. Additionally, exploring the factors that influence ADs completion is crucial for enhancing patient care, shaping effective policies, and potentially aligning end-of-life care with patients’ values and preferences.
Methods
This report is part of a larger systematic review project structured within the CoCoPop (Condition, Context, Population) framework, 12 aiming to investigate the prevalence and moderators of ADs, advance care planning (ACP) and do not resuscitate (DNR) orders among different populations and settings (https://www.crd.york.ac.uk/PROSPERO/view/CRD42024513137). The results concerning the prevalence and moderators of ADs are presented in this paper. The PRISMA 2020 checklist 13 was followed for reporting.
Three main populations were investigated: general unselected community individuals, acutely ill patients, and chronically ill patients (both oncologic and non-oncologic).
The settings were classified as community, outpatient offices, prehospital emergency medical services (EMS), Emergency Departments (ED), hospital wards, intensive care unit (ICU), nursing home/elderly home (NH/EH) and palliative care (PC).
The prespecified moderators investigated were median age, gender (proportion of men), white ethnicity (proportion of white individuals), income (median income), education (proportion of individuals with at least a college degree), continent, oncologic disease (proportion of patients with an oncologic diagnosis), marital status (proportion of individuals married or engaged) and self-determination capacity.
Study Selection and Data Extraction
PubMed, Scopus, and Cochrane Library databases were searched from inception up to December 31, 2023 (Supplemental Material).
We considered only English language prospective, retrospective cohort studies, cross-sectional surveys and randomised controlled trials (RCTs) that reported on the prevalence of ADs. In the case of RCTs or pre-post interventional studies, we recorded only the prevalence observed in the control or pre-intervention arm.
Advance Directives were defined from the Bioethics Thesaurus as any declaration made by patients, in advance of a situation where they may be incompetent to decide about their own care, stating their treatment preferences or authorising a third party to make decisions for them.
Two reviewers, blinded to each other’s assessment, independently evaluated the studies using the Rayyan software 14 as primary storage support. Discrepancies were resolved through review, and in case of persistent disagreement, a senior reviewer was involved for the final decision.
Data extraction was also performed by 2 reviewers using a Microsoft Excel® spreadsheet. The extracted information included article characteristics, population characteristics, prevalence of ADs and potential moderating factors. For grouped continuous data, such as age classes, the midpoint of each interval was multiplied by the frequencies of the corresponding classes and the sum of the products was divided by the total number of values to estimate the mean.
Risk of Bias Assessment
The Joanna Briggs Institute (JBI) critical appraisal tool for prevalence reporting 15 was applied to all the included studies. For consistent evaluation, a negative discrepancy between actual and ideal sample size 16 was considered inadequate. Additionally, self-reported methods for collecting ADs information were considered less reliable compared to methods that utilised healthcare or administrative records.
Statistical Analysis
A random-effects proportion meta-analysis model was built, including subgroup analysis for the populations and settings investigated. The meta-analysis was conducted by adopting the inverse variance method and the logit transformation with continuity correction. Confidence intervals for individual studies were calculated through the Clopper-Pearson method. 17 Heterogeneity was expressed with the I 2 statistic. Orchard plots and bubble plots were generated for data visualisation.
Influence analysis was carried out through the leave-one-out method and involved the exploration of both the variation of the meta-analytic estimate, Baujat plot as well as studentized deleted residuals and Cook’s distances.
The moderator analysis was conducted using univariate meta-regressions to explore various potential moderator variables across all the studies included.
Variables reported in less than 20 studies were excluded from moderator analysis.
Before proceeding to multivariable modelling, potential correlations among the continuous candidate moderators were studied using Spearman’s rank correlation coefficient. In case of highly correlated variables (Spearman’s Rho > 0.8), only one variable was kept in the analysis.
A multivariable meta-regression model was built through a multi-model inference, which determines the most fitting combination of predictors and identifies the most critical predictors across the constructed model. Furthermore, multimodel coefficients aggregated across all models in which they appear can be displayed. Predictor importance is reported in a scale from 0 to 1 and, by convention, variables scoring 0.8 or higher are considered highly influential.
The corrected Akaike Information Criterion (cAIC) was used for model selection.
To investigate the robustness of the multimodel results to potential bias due to missing variable data, a sensitivity analysis was performed by running the multimodel inference again on a complete dataset where missing data were imputed through a random forests algorithm.
All the analyses were carried out in R 4.3.2, 18 using the packages ‘meta’, 19 ‘metafor’, ‘dmetar’, 20 ‘orchaRd’ 21 and ‘missForest’. 22
Reporting Bias
Meta-analyses of proportions aim to depict the prevalence including observational and non-comparative information about an event. This inherently precludes the testing of statistical significance for their findings, consequently, classical statistical tests used for reporting bias detection such as Egger’s test are not recommended for prevalence meta-analyses. 23
However, doi plots and Luis Furuya–Kanamori (LFK) index were recently discussed as instruments to objectively verify the presence of reporting bias also in the case of prevalence studies, in case of a priori expectation of positive or negative reporting bias. 24
For the purposes of this systematic review, the main concern of the Authors was a positive reporting bias (higher prevalence studies being more likely to be published), therefore, an LFK index > 1 would have been considered as an indicator of reporting bias.
Doi graphs and LFK index were calculated with the ‘metasens’ 25 package for R.
Certainty of Evidence
Despite there is currently no available guideline for rating the evidence from epidemiological studies, the main items of the GRADE methodology can be used as points of discussion. 26
Results
A total of 2374 studies resulted from searching the 3 databases, which were screened by title and abstract, after removal of duplicates. Ultimately, considering also hand-search, 535 articles were reviewed in full. Among these, 239 articles providing prevalence data for ADs among 8 914 842 individuals were finally included in the meta-analysis (Figure 1).

PRISMA flowchart.
The general characteristics of the included studies are summarised in Table 1, while detailed descriptions of each individual study are available in Supplemental Table 1.
General Characteristics of the Included Studies.

Note. k = number of studies; EMS = emergency medical services; IQR = interquartile range.
Most of the included studies focused on patients affected by chronic conditions (k = 140, 58.6%), with the most frequent settings being nursing homes/elderly homes (k = 68, 28.5%) and community settings (k = 59, 24.7%).
Almost all the studies were conducted in high-income countries (k = 230, 96.2%), predominantly from North America (k = 176, 73.6%) or Europe (k = 43, 18%), globally encompassing a period from 1984 to 2023.
Sample sizes were similar across the explored populations, while the chronic population showed a higher median age and a lower proportion of men and married or engaged individuals.
Missingness Distribution and Risk of Bias
Figure 2A illustrates the distribution of variable missingness among the explored populations. Globally, the variables with more missing data across the studies were education (k = 85), oncologic aetiology (k = 92), and marital status (k = 93).

Distribution of missingness across the extracted variables, risk of bias of included the studies according to the JBI critical appraisal tool. Abbreviations: JBI – Joanna Briggs Institute. A: Variables available for data extraction. B: Risk of bias assessment (JBI Critical appraisal tool).
Data about income were available in 21 studies; however, the variety of techniques used for reporting prevented the possibility of comparisons. Therefore, this variable was excluded from the candidate moderators included in the meta-regressions.
The risk of bias for prevalence assessment, evaluated with the JBI critical appraisal tool, was generally low, with 90.7% of the studies (k = 217) satisfying at least 7 of the 9 items of the tool (Figure 2B). The most critical limitations were the small sample size in 31% (k = 74) of the included studies and the methods used for ADs detection, with self-reporting methods adopted in 45% of studies (k = 107). Since self-reporting can introduce recall bias and small sample sizes are more prone to sampling bias, a non-pre-planned subgroup analysis was conducted to determine if the detection methods or sample size significantly influenced the meta-analysis results (Supplemental Figures 1 and 2). Neither the use of self-reported methods nor sample size showed a significant association with different estimates (P = .386 and P = .358).
Table 2 displays the global meta-analytic synthesis, subgroup analyses and the univariate meta-regressions, while Figure 3 provides a graphical visualisation of the relationships found.
Meta-Analysis Results, Subgroup Analyses, Univariate Moderators’ Meta-Regressions.

Note. k = number of studies; n = number of patients involved; EMS = emergency medical services; CI = confidence interval.
p <0.05.

Univariate meta-regressions. Panel (A) shows the subgroup analysis for acutely ill, chronically ill, and general population. The other panels show the bubble plots relative to the moderators: year of publication (B), education (C), white ethnicity (D), median age (E), male sex (F), oncologic disease (G), and marital status (H).
The global meta-analytic estimate of the prevalence of ADs was 0.26 [95% CI: 0.23-0.30], with a prediction interval ranging from 0.02 to 0.85. Subgroup analyses revealed significantly lower proportions in the acute population [0.16, 95% CI: 0.12-0.22], rather than the chronic [0.28, 95% CI: 0.24-0.34, P = .002] or general population [0.32, 95% CI: 0.25-0.40, P = .002].
Regarding the investigated settings, the ED [0.17, 95% CI: 0.09-0.29, P = .047] and prehospital EMS [0.07, 95% CI: 0.06-0.09, P = .007] showed significantly lower proportions of ADs (Supplemental Figure 3).
No significant differences were found among continents (Supplemental Figure 4) and different self-determination capacity statuses (Supplemental Figure 5).
Subgroup meta-analytic estimates for single countries are depicted in Supplemental Figure 6.
Univariate meta-regressions showed no significant effects for the year of publication (P = .107), the proportion of oncologic patients in the sample (P = .147), and the proportion of married or engaged individuals (P = .712).
However, age [OR: 1.02, 95% CI: 1.002-1.03, P = .023], the proportion of individuals with a college degree or higher [OR: 4.27, 95% CI: 1.43-12.76, P = .009], and the proportion of individuals of white ethnicity [OR: 4.09, 95% CI: 1.75-9.59, P = .001] were positively associated with the proportion of ADs.
Conversely, the proportion of men in the sample [OR: 0.30, 95% CI: 0.10-0.86, P = .025] was negatively associated with ADs prevalence.
Observed heterogeneity was very high, and each of the continuous moderators explored in univariate analyses had little explanatory power globally, with ethnicity and education being 2 variables with higher R 2 values (6.77% and 6.23%, respectively), while the remainder accounted for less than 3% variability each.
Influence Analysis
Influence analysis revealed 2 influential studies,27,28 Supplemental Figures 7 and 8 show the Baujat plot and the other results of influence analysis.
However, the results obtained from refitting the meta-analysis with the leave-one-out method (Supplemental Figure 9) and dropping the 2 influential studies together showed an unmodified prevalence of ADs.
Multivariate Meta-Regression Modelling and Sensitivity Analysis
Correlation analysis (Supplemental Figure 10) highlighted a strong correlation between the proportion of oncologic patients and the proportion of patients married or engaged (Spearman’s rho = .89). Therefore, the latter variable was excluded from model building.
Additionally, the variable for self-determination capability was omitted from the multivariable model building because all the studies involving incapable patients also included patients with chronic conditions.
The predictor importance in multimodel inference was assessed based on 256 models fitted and evaluated using cAIC.
The most influential variables were education, white ethnicity and the proportion of oncologic patients.
The sensitivity analysis, involving multimodel inference fitted on random forest-imputed missing data, confirmed the significance of education level and ethnicity as influential factors. Additionally, this analysis included the variables continent, population and age (Figure 4).

Multimodel inference results.
Table 3 shows the multimodel inference weighted coefficients for both the complete and imputed studies. Education level was the only variable retaining statistical significance in the multivariate modelling of the complete studies. It also remained among the most influential factors in the model considering the imputed variables.
Multimodel inference weighed coefficients.

Note. OR = odds ratio; CI = confidence interval.
p <0.05.
Reporting Bias
The doi plot (Supplemental Figure 11), built on logit-transformed proportions, showed a left-skewed distribution and an LFK index value of −4.31, thus disconfirming concerns regarding positive reporting bias.
Discussion
This systematic review examined the prevalence of ADs among various groups, including the general population, acutely ill patients and chronically ill patients, along with their moderators. The key findings are: (a) Studies on ADs predominantly originated from high-income countries, especially the US. (b) The global proportion of individuals with recorded ADs is 0.26, with significant heterogeneity among studies. Higher proportions were observed among chronically ill patients and the general population compared to acutely ill patients. (c) Univariate moderator analysis identified several factors positively associated with ADs prevalence: median age of the sample, prevalence of oncologic illness, level of education and white ethnicity. Conversely, male sex was negatively associated with ADs prevalence. Multimodel inference analysis, along with sensitivity analysis, highlighted education and white ethnicity as the most influential moderators.
Overall, these findings suggest that, despite the widely advocated importance of ADs completion 29 and active research on promotion in this field during the last decades, 30 the overall proportion of ADs completions remains low, static over time, and possibly unequal.
The mechanisms underlying these results are probably an intricate milieu of cultural, socio-economic, legal, religious, healthcare and personal aspects that are difficult to synthesise and weigh, potentially explaining the extremely high heterogeneity reported among studies, even within the same countries.
A more nuanced interpretation of the findings requires acknowledging how legal and cultural frameworks influence ADs completion. Countries differ widely in their legal infrastructure, from comprehensive legislative support to near-complete legal absence or poor enforcement elsewhere. 31 Yet even legal provision does not guarantee implementation. 32 Cultural norms also shape attitudes towards autonomy and death: in many Asian societies, for instance, family-centred decision-making has a higher weight in ADs-related decisions.33,34 In Pakistan, religious beliefs, cultural sensitivities around death, and low legal literacy were found to inhibit both conversations and documentation of end-of-life preferences. 34 These legal-cultural dynamics contribute to regional disparities and must be factored into global interpretations of ADs prevalence.35,36
Globally, significant differences were found across acutely ill, chronically ill, and general population groups in ADs completion, with the individuals in the latter 2 showing a higher prevalence of ADs.
Ageing is a risk factor for major, chronic, progressive and debilitating diseases; however, despite age differences observed among the populations studied, with an older median age in general and chronic populations, other aspects other than age could contribute to the decision to complete ADs.
In particular, the nature of chronic illness seems to have a rather strong influence, with oncologic conditions being associated with a higher prevalence of recorded ADs, this could be due to deeper social perception of the implications of most of the oncologic diseases, as well as more inclusive diagnostic-therapeutic pathways which encompass a reflection about end-of-life wishes. 37
This difference is also reflected in lower palliative care access for patients affected by non-oncologic diseases, which has been progressively pointed out in recent years.38,39
Another critical point is the reporting of similar proportions of ADs between self-determination capable and non-capable patients, underlying the risk of losing the possibility to know precious information when it’s needed to make choices.
Still, in recent years, discussion has developed around the controversy of precedent autonomy as the justification for advanced dementia directives that complicates the decisional process around patients who lose very early self-determination due to their primary illness. 40
Gender disparity towards a lower completion of ADs emerged from univariate meta-regressions, however, multimodel inference reduced the importance of this variable, probably because women tend to outlive men and be older at the end of life. Nonetheless, the inverse relation between male proportion and ADs completion could be explained by the different cultural norms and approaches between men and women regarding their caregiver status, and economic possibilities, consistent with other literature. 41
Finally, the most influential factors which emerged even after multivariate adjustment were white ethnicity and education.
Racial disparities in healthcare are still widely spread, and they also affect the EOL care. 42 Black people or other ethnic minorities in the US are less likely to have completed ADs. This could be explained by a different approach in the discussion of treatment decisions with healthcare providers due to inaccessibility of care and mistrust of the healthcare system, greater preferences for life-sustaining treatments, religious and spiritual beliefs, language barriers and discomfort to speak of EOL preferences with family members43 -46.
Education disparities are widely associated with disparities in access to healthcare,47,48 underlying the pivotal role of instruction in allowing individuals to make informed decisions and self-determination.
Of note, despite the impossibility of modelling an income variable, income information could have partly been captured from both the ethnic and education variables and could have contributed to their weight in analyses.
Our reported prevalence is slightly lower compared to those obtained from previous nation-based systematic reviews conducted in the last decade in the US 8 and Germany, 9 the larger geographical areas considered rather than single countries and the language restriction for paper selection could have contributed to this.
Limitations
Several limitations should be considered when evaluating the results of this study.
First, legal aspects may vary profoundly across the different countries from which data were extracted and could have had a role in modifying the reported prevalences.
Second, we assumed that the same moderator would similarly affect the prevalence of ADs in the different countries, populations, and settings explored, despite their baseline cultural, religious, and socioeconomic differences. In practice, the weight of single factors could have varied in different situations.
Third, the inclusion of a very large timespan could have encompassed social and legal modifications even within the single countries explored.
Fourth, most of the data collected in this work came from the US, while other areas of the globe are almost not represented. Therefore, the results should be interpreted as a picture of Western cultures. Moreover, the exclusion of non-English literature could have introduced language bias, especially for Asian estimates.
Finally, despite the number of studies collected, some studies reporting ADs could have been missed due to the variety of terms used in the literature.
Certainty of Evidence
The GRADE ratings are summarised in Table 4.
GRADE Evaluation of Confidence in Findings.
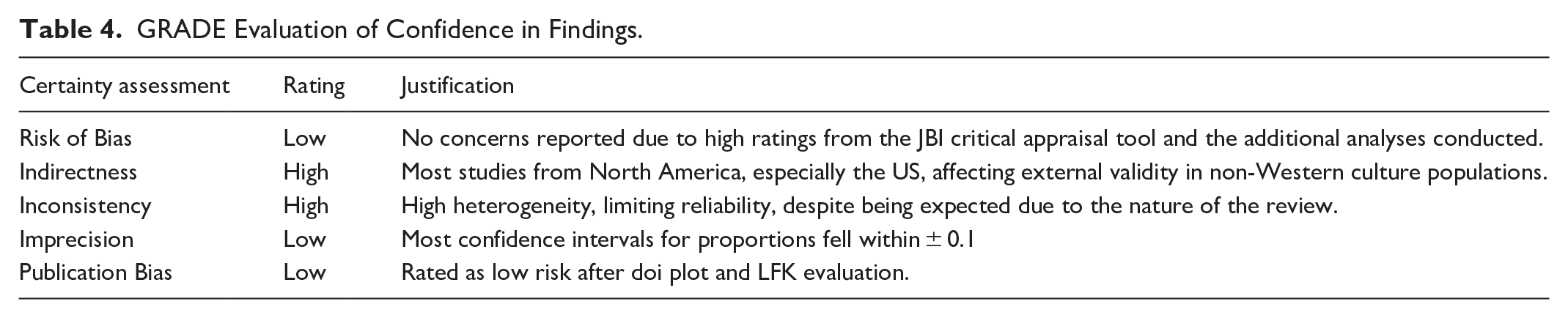
Most of the studies included came from North America, especially the US, conditioning the external validity of the results, especially in non-Western-culture populations, therefore, indirectness was rated at high risk.
Overall, no concerns were reported regarding the risk of bias of the included studies due to the globally high ratings obtained from the included studies concerning the JBI critical appraisal tool.
Also, reporting bias was rated as low risk after the doi plot and LFK evaluation.
Apart from income data, coherence in variables reporting allowed meta-analysis of a significant number of studies and most of the confidence intervals for proportions fell within ± 0.1, therefore, imprecision was rated as low risk.
Finally, heterogeneity was rated as high risk and was the most important aspect limiting the reliability of the results, despite this being expected due to the nature of this systematic review 23 and the variety of possible residual unmeasured confounders.
Future Perspectives
Based on the reported findings, possible interventions should focus on both information and ease of access and completion of ADs.
First, early school information programmes could create the basis for more informed adults and back transfer to their families the importance of reflecting on their own end-of-life wills and the instruments to have them respected.
Recently, courses enhancing discussion about death and dying dedicated to children up to the age of 8 are being developed 49 but there is still a lack of information about their long-term effectiveness.
Physicians, in particular primary care physicians, could be another active source of information and discussion about end-of-life preferences, and have been proven to be effective in increasing ADs completion. 50
However, despite the literature generally indicating a positive attitude towards the concept of ADs that increases with increasing experience with their use, several barriers are reported, ranging from legal problems, cultural and religious obstacles to discussion, to family influence. 51
Unfortunately, a recent survey in Belgium demonstrated a still low involvement of general practitioners in ADs completion. 52
Also, based on the results reported, information on end-of-life instruments should be especially fostered in patients affected from chronic non-oncologic diseases.
Finally, a redesign of less complex ADs documents and a simplification of the general process of ADs completion could have a positive influence on the least-educated sections of the population and reduce the logistical, time-consuming barriers. 53
Conclusions
Despite half a century having passed since their first introduction, the global prevalence of ADs remains low across the populations and settings explored. Moderator analysis suggests non-white ethnicities, less educated segments of society and patients suffering from non-oncologic diseases are the most important targets of information campaigns.
Different points in life trajectories and different figures, such as teachers and general practitioners, could serve as vehicles to increase population awareness and competition for documents.
Supplemental Material
sj-docx-12-inq-10.1177_00469580251344161 – Supplemental material for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-12-inq-10.1177_00469580251344161 for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis by Danila Valenti, Giulia Bortolotti, Federico Moro, Silvia Cardini, Silvia Cavagna, Marco Tartaglione, Davide Allegri, Fabrizio Moggia, Federico Semeraro and Lorenzo Gamberini in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-13-inq-10.1177_00469580251344161 – Supplemental material for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-13-inq-10.1177_00469580251344161 for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis by Danila Valenti, Giulia Bortolotti, Federico Moro, Silvia Cardini, Silvia Cavagna, Marco Tartaglione, Davide Allegri, Fabrizio Moggia, Federico Semeraro and Lorenzo Gamberini in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-14-inq-10.1177_00469580251344161 – Supplemental material for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-14-inq-10.1177_00469580251344161 for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis by Danila Valenti, Giulia Bortolotti, Federico Moro, Silvia Cardini, Silvia Cavagna, Marco Tartaglione, Davide Allegri, Fabrizio Moggia, Federico Semeraro and Lorenzo Gamberini in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-15-inq-10.1177_00469580251344161 – Supplemental material for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-15-inq-10.1177_00469580251344161 for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis by Danila Valenti, Giulia Bortolotti, Federico Moro, Silvia Cardini, Silvia Cavagna, Marco Tartaglione, Davide Allegri, Fabrizio Moggia, Federico Semeraro and Lorenzo Gamberini in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-jpeg-9-inq-10.1177_00469580251344161 – Supplemental material for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis
Supplemental material, sj-jpeg-9-inq-10.1177_00469580251344161 for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis by Danila Valenti, Giulia Bortolotti, Federico Moro, Silvia Cardini, Silvia Cavagna, Marco Tartaglione, Davide Allegri, Fabrizio Moggia, Federico Semeraro and Lorenzo Gamberini in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-jpg-1-inq-10.1177_00469580251344161 – Supplemental material for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis
Supplemental material, sj-jpg-1-inq-10.1177_00469580251344161 for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis by Danila Valenti, Giulia Bortolotti, Federico Moro, Silvia Cardini, Silvia Cavagna, Marco Tartaglione, Davide Allegri, Fabrizio Moggia, Federico Semeraro and Lorenzo Gamberini in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-jpg-10-inq-10.1177_00469580251344161 – Supplemental material for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis
Supplemental material, sj-jpg-10-inq-10.1177_00469580251344161 for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis by Danila Valenti, Giulia Bortolotti, Federico Moro, Silvia Cardini, Silvia Cavagna, Marco Tartaglione, Davide Allegri, Fabrizio Moggia, Federico Semeraro and Lorenzo Gamberini in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-jpg-11-inq-10.1177_00469580251344161 – Supplemental material for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis
Supplemental material, sj-jpg-11-inq-10.1177_00469580251344161 for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis by Danila Valenti, Giulia Bortolotti, Federico Moro, Silvia Cardini, Silvia Cavagna, Marco Tartaglione, Davide Allegri, Fabrizio Moggia, Federico Semeraro and Lorenzo Gamberini in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-jpg-2-inq-10.1177_00469580251344161 – Supplemental material for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis
Supplemental material, sj-jpg-2-inq-10.1177_00469580251344161 for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis by Danila Valenti, Giulia Bortolotti, Federico Moro, Silvia Cardini, Silvia Cavagna, Marco Tartaglione, Davide Allegri, Fabrizio Moggia, Federico Semeraro and Lorenzo Gamberini in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-jpg-3-inq-10.1177_00469580251344161 – Supplemental material for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis
Supplemental material, sj-jpg-3-inq-10.1177_00469580251344161 for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis by Danila Valenti, Giulia Bortolotti, Federico Moro, Silvia Cardini, Silvia Cavagna, Marco Tartaglione, Davide Allegri, Fabrizio Moggia, Federico Semeraro and Lorenzo Gamberini in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-jpg-4-inq-10.1177_00469580251344161 – Supplemental material for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis
Supplemental material, sj-jpg-4-inq-10.1177_00469580251344161 for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis by Danila Valenti, Giulia Bortolotti, Federico Moro, Silvia Cardini, Silvia Cavagna, Marco Tartaglione, Davide Allegri, Fabrizio Moggia, Federico Semeraro and Lorenzo Gamberini in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-jpg-5-inq-10.1177_00469580251344161 – Supplemental material for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis
Supplemental material, sj-jpg-5-inq-10.1177_00469580251344161 for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis by Danila Valenti, Giulia Bortolotti, Federico Moro, Silvia Cardini, Silvia Cavagna, Marco Tartaglione, Davide Allegri, Fabrizio Moggia, Federico Semeraro and Lorenzo Gamberini in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-jpg-6-inq-10.1177_00469580251344161 – Supplemental material for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis
Supplemental material, sj-jpg-6-inq-10.1177_00469580251344161 for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis by Danila Valenti, Giulia Bortolotti, Federico Moro, Silvia Cardini, Silvia Cavagna, Marco Tartaglione, Davide Allegri, Fabrizio Moggia, Federico Semeraro and Lorenzo Gamberini in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-jpg-7-inq-10.1177_00469580251344161 – Supplemental material for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis
Supplemental material, sj-jpg-7-inq-10.1177_00469580251344161 for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis by Danila Valenti, Giulia Bortolotti, Federico Moro, Silvia Cardini, Silvia Cavagna, Marco Tartaglione, Davide Allegri, Fabrizio Moggia, Federico Semeraro and Lorenzo Gamberini in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-jpg-8-inq-10.1177_00469580251344161 – Supplemental material for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis
Supplemental material, sj-jpg-8-inq-10.1177_00469580251344161 for The Prevalence of Advance Directives and Its Moderators Among Community People, Acutely and Chronically Ill Patients: A Systematic Review and Meta-Analysis by Danila Valenti, Giulia Bortolotti, Federico Moro, Silvia Cardini, Silvia Cavagna, Marco Tartaglione, Davide Allegri, Fabrizio Moggia, Federico Semeraro and Lorenzo Gamberini in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Author Contributions
Danila Valenti – Conceptualisation, Funding Acquisition, Supervision.
Giulia Bortolotti – Conceptualisation, Data curation, Investigation, Writing – Original Draft.
Federico Moro – Methodology, Data curation, Investigation.
Silvia Cardini – Data curation, Investigation.
Silvia Cavagna – Data curation, Investigation.
Marco Tartaglione – Data curation, Investigation.
Davide Allegri – Formal analysis.
Fabrizio Moggia – Conceptualisation.
Federico Semeraro – Writing – review & editing.
Lorenzo Gamberini – Methodology, Formal analysis, Visualisation, Project Administration, Writing – Original draft.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Publication costs are covered with funds from the Palliative Care Network, Bologna Local Health Agency, Bologna, Italy. No other fundings were received for this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All the data used to perform the meta-analysis is available within the Supplemental Materials
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.