
Abstract
The Saudi Vision aims to empower women in leadership positions, particularly in male-dominated fields. Despite these national reforms, disparities remain. This study aimed to explore women’s status in leadership and administrative positions in the medical imaging field and assess the empowering factors related to women’s leadership and administrative roles. An online cross-sectional questionnaire was distributed to female workers in the medical imaging field at health and academic institutions between December 2021 and October 2022. The questionnaire comprised 3 sections: a) demographics (14 items), b) self-empowerment (38 items), and c) challenges faced by women in the medical imaging field (7 items). All responses were mandatory. Only 18.3% of the 44 female executives had leadership responsibilities, with most of them working in the medical imaging industry (72.7%). Furthermore, 49.6% of Saudi women feel that they cannot advance into administrative jobs. The common challenges faced by women were difficulties in balancing work and life (54.6%), followed by long working hours (52.5%) and societal restrictions (42.1%). The findings revealed no significant association between the mean score for challenges faced by Saudi women and various demographic characteristics (P > .05). This study reveals that many Saudi women in medical imaging and radiology feel constrained in their ability to advance to administrative roles, reflecting deep-rooted cultural barriers that Vision 2030 seeks to address. Significant participation from women younger than 25 revealed an unanticipated yet meaningful influence of Saudi Vision 2030, demonstrating how recent reforms have encouraged younger women to pursue careers and feel empowered to enter the medical imaging profession earlier than previous generations. Addressing challenges requires targeted policy initiatives and reforms. By promoting gender equity and fostering an inclusive work environment, institutions in the healthcare sector can empower women and enhance their career growth.
Highlights
This cross-sectional survey of 240 Saudi women in medical imaging found only 18.3% held leadership or administrative roles, highlighting persistent underrepresentation.
Participants reported high self-esteem (mean 4.26/5) and self-efficacy (mean 4.11/5), indicating strong internal readiness for leadership despite systemic barriers.
The top challenges to advancement were work–life balance (54.6%), long working hours (52.5%), and societal restrictions (42.1%), with no significant variation across demographic groups.
Significant engagement by women under 25 (49.2% of sample) reflects the early impact of Saudi Vision 2030 reforms in empowering younger graduates to enter and aspire within the field.
Saudi Arabian initiatives such as Wusool and Qurrah enabled women to join private sector and ensured job stability.
Introduction
Global development for women has stalled because of the economic and social impacts of the pandemic and geopolitical tensions, with the risk of leaving permanent scars on universal efforts toward empowering women. Empowerment is a combination of power and self-sufficiency, rather than a single process that stimulates individuals to contribute positively to the success of communities. Qualified females remain marginalized in leadership and administrative positions. 1 According to the United Nations Educational, Scientific, and Cultural Organization (UNESCO), the global science records indicated that less than 30% of researchers are female, with 42% in Asia, 30% in Africa, 32% in North America and Western Europe, and 45% in Latin America. 2 In the United States of America (USA), the presence of females in decanal positions (ie, dean, vice dean, senior associate dean, associate dean, and assistant dean) in medical schools is only 15% of the academic leadership population. 3 In Saudi Arabia, only 23.2% of all researchers are female; thus, the number of female researchers is lower than that reported by UNESCO. 4 Women’s political empowerment in Saudi village councils was found to represent only 33% of the total positions; therefore, the councils are dominated by men. 5
Cultural norms heavily influence attitudes toward women’s roles, particularly in the health sector, perpetuating gender disparities. Expectations of altruism over financial gain led to low-paying or unpaid positions, disproportionately affecting women. In collectivist societies like the Middle East and Saudi Arabia, traditional values often limit women’s leadership opportunities. Additional barriers include environmental factors, familial responsibilities, workplace male dominance, and gender inequality. 6 The Saudi 2030 Vision marks a turning point by increasing media attention to the empowerment of women. However, deep-rooted cultural beliefs continue to pose challenges, with resistance stemming from religious convictions and entrenched customs. 7
The interplay between personal and workplace challenges forms a complex matrix, where individual barriers, such as lack of self-motivation and educational attainment 8 are compounded by severe work atmosphere issues, including sexual harassment, 9 lack of a platform for expression, perceived incompetence, and male coworkers’ discomfort with competent women. 10
Evidence indicates that the participation of women in the field of medicine is approximately 50%. 11 In contrast, the role of women in leadership is less owing to reasons such as delayed leadership opportunities, gender inequality, and unequal capabilities. Some female faculty members may have difficulty balancing professional and family responsibilities, leading them to leave their leadership roles in favor of males because of a lack of cooperation and work-life balance. 12 Despite increasing reports of violence and discrimination against women,13,14 empowering women remains a crucial strategy for safeguarding and protecting women from abuse. 15 Addressing core challenges requires raising awareness and implementing policies that promote women’s roles, ensure equal opportunities, and support work-life balance. These measures can enhance leadership skills and drive women’s societal development.
Recent initiatives to enhance women’s participation in the workforce and promote their leadership roles have revealed a complex landscape of progress and challenges. A comparative study of 5 countries highlighted significant disparities: Pakistan and India lag behind in empowering women, 16 whereas Thailand and the Philippines lead the initiatives, with greater flexibility and freedom for women to ascend to leadership positions. 17 Malaysia, while showing promise, offers slightly less flexibility than Thailand. 16 In Saudi Arabia, women’s representation in leadership roles remains notably low, with the country ranking 141st out of 149 on the Global Gender Gap Index in 2018. Despite a remarkable 130% increase in the number of women in the private sector by 2022, their representation in leadership roles remains lower than their progress in education and political empowerment (ranking 127th out of 149). 18
Research from various regions indicates a persistent underrepresentation of women in leadership positions within radiology and medical imaging. In Europe, for example, data gathered by the European Society of Radiology in 2019 revealed that only 20.6% of chair positions were held by women, despite a growing number of female practitioners entering the field. 19 Similarly, in Australia, significant gender disparities in interventional radiology was reported, emphasizing the need for policies that promote gender equity and support women’s career advancement. 20 Research from the United States and Europe consistently shows that women in radiology and medical imaging hold fewer senior administrative and academic positions compared to men, despite having similar qualifications and professional experience.21,22 We believe that specific cultural and societal norms in Saudi Arabia add unique dimensions to these global challenges.
To accelerate progress toward women’s empowerment by 2030, further research is needed to identify and address the barriers that continue to impede their advancement. Women continue to experience discrimination in several areas, including childbirth, marriage, family decisions, and health. Giving women an equal voice in all these decisions might help them become more empowered in society.
The Saudi Arabia Vision initiative promotes the empowerment of women by relaxing the constraints placed on them. Since 2016, this initiative has publicly stated that women should comprise 30% of leadership positions in the Saudi system. 7 The reform of the entire system, including education and healthcare, favors the contributions of women to the advancement of life in the Kingdom. These recent developments offer important lessons for increasing efforts in emerging fields, such as medical imaging in medicine and academia. 23
Previous studies have extensively explored the empowerment of women in various sectors such as education and workplace settings.1,5,24-26 However no study has explored the status of Saudi women in leadership and administrative roles in medical imaging or the factors empowering them. Addressing this gap, our study investigates these roles post-Saudi Vision 2030, identifying empowering factors, unique challenges, and strategies to enhance female empowerment in radiology. This research provides valuable insights into gender dynamics within Saudi Arabia’s evolving medical imaging field.
Methods
Study Design, Setting, Population
This cross-sectional study was conducted using self-designed and validated questionnaires that were administered between December 2021 and October 2022. The target population comprised women working in the medical imaging or radiological science departments at hospitals and universities in Saudi Arabia. Inclusion criteria required participants to be Saudi women aged 18 or older, holding an educational degree at the level of a diploma, bachelor’s degree, master’s degree, or Ph.D. Individuals who did not satisfy these criteria were excluded from this study. Of the 250 responses received, 240 female participants satisfied the inclusion criteria and provided consent for inclusion in the final sample for analysis. Participants who did not meet the inclusion criteria were excluded.
Sample Size Estimation
The sample size was calculated by the online calculator (http://www.raosoft.com/samplesize.html) at a 5% margin of error and 95% confidence interval. The necessary sample size for this study was 218 since we anticipated that there would be 500 women working in the medical imaging or radiological science departments at hospitals and universities in Saudi Arabia. On the other hand, we decided to poll as many respondents as possible to prevent sampling bias therefore we received 250 responses but accepted 240 responses. The remaining 10 respondents were excluded due to incomplete responses or failure to meet eligibility criteria. Since participation was voluntary and anonymous, no specific reasons for non-participation or dropout could be obtained.
Questionnaire Design
A self-designed and validated questionnaire was developed to investigate women’s leadership in medical imaging. The bilingual online surveys, crafted in both English and Arabic by researchers, comprised 3 sections. The first section gathered demographic data and basic information, including region, age, marital status, number of children, education level, sector, hospital size, years of experience, monthly income, leadership position status, and current job roles. The second section addressed 7 domains, with a total of 38 items: self-esteem (4 items), self-efficacy (2 items), economic empowerment (5 items), freedom of mobility (3 items), environmental factors (10 items), institutional factors (7 items), and job empowerment factors (7 items). The final section focused on the challenges faced by women in the medical imaging field and comprised 5 items. Each item was assessed on a 5-point Likert scale ranging from “1” for “strongly disagree” to “5” for “strongly agree.” To ensure the validity and reliability of the survey instrument, we conducted both external and internal consistency assessments. Before the main study, external validity was established through expert review by a panel of specialists in leadership and women’s empowerment, who evaluated the questionnaire for content relevance and clarity. Their feedback was incorporated into the final version The questionnaire was subjected to a pilot study for internal consistency with a random sample of women to assess its validity and reliability. The pilot study yielded a Cronbach’s alpha of (α = .90), indicating high reliability and validity of the instrument. In the main study, the overall mean score for the challenges faced by Saudi women was calculated by averaging the scores for the 5 items related to these challenges, with higher scores indicating greater agreement with their presence. There were no missing data in the final dataset, as the online questionnaire was designed with all questions set as compulsory; participants could not proceed to the next item without completing the previous one.
Data Collection
The data were collected using convenience sampling. The questionnaire was distributed online to the study population via social media platforms and email lists from academic institutions. An electronic link to the questionnaire, created using Google Forms, was distributed to the target population. This process was continued until the required sample size was reached.
Ethics and Consenting
This study was conducted via an online cross-sectional questionnaire, targeting female professionals within the medical imaging field in Saudi Arabia. Given the non-invasive and anonymous nature of the survey, which did not collect any personally identifiable information from participants, the Institutional Review Board (IRB) granted a waiver for written informed consent. Instead, participants provided their consent electronically at the beginning of the survey. This consent procedure ensured that all participants were fully informed about the purpose of the study, the voluntary nature of their participation, the anonymity of their responses, and the academic use of the data collected. This method aligns with ethical guidelines for minimal risk research involving human subjects. This manuscript was prepared in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies. The completed STROBE checklist is provided in the Supplemental Materials. 27
Data Analysis
Data analysis was performed using Statistical Package for the Social Sciences (SPSS) version 27 (SPSS Inc., Chicago, Illinois, USA). Descriptive statistics were calculated, including the frequencies and percentages of categorical variables. Continuous variables were presented as mean values. To assess the associations between variables, Student’s t-test was used for comparisons involving 2 groups, whereas Analysis of Variance (ANOVA) was used for comparisons involving more than 2 groups. All statistical analyses were conducted at a significance level of α = .05.
Results
Geographical Distribution and Basic Characteristics
Most respondents were from Riyadh, comprising 55.4% of the total study sample, and representing the largest group. The next largest group was from the Eastern region, accounting for 13.8% of participants. Regarding years of experience, 60.4% of the respondents (n = 145) reported having 5 years of experience. In terms of age distribution, 49.2% of respondents (n = 118) were under 25 years old, while 18.3% (n = 44) were between 25 and 30 years old. Further details of the geographical distribution are available in Figure 1 and demographic characteristics of the participants are summarized in Table 1.
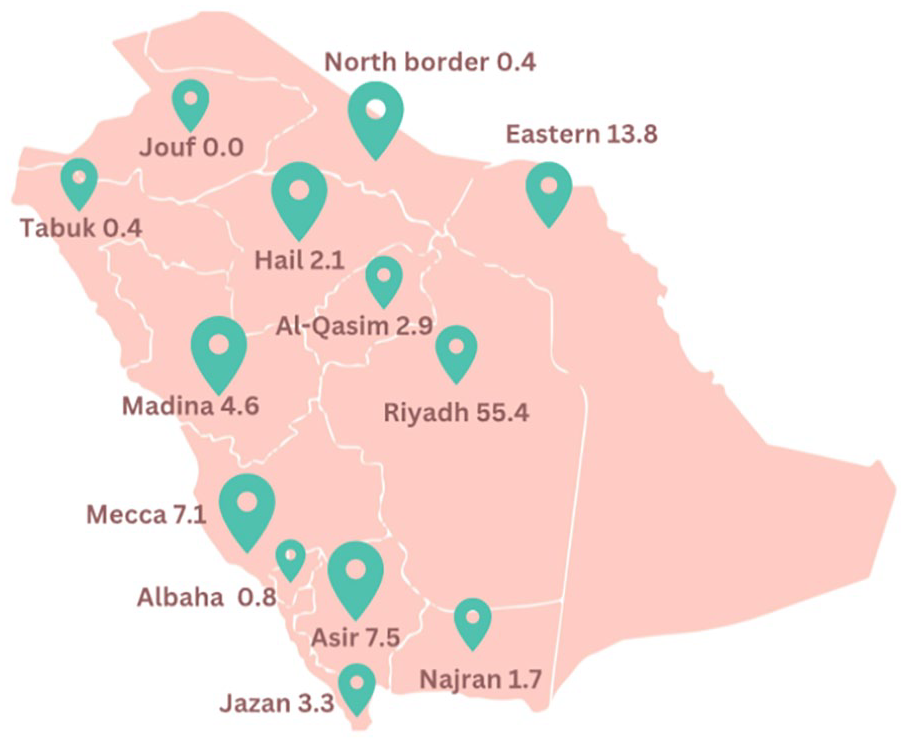
Geographical distribution of participants.
Characteristics of the Participants (n = 240).

The demographic profile of the study sample revealed a significant proportion of single females (n = 125, 52.1%), while (n = 108, 45%) were Married. Within the subgroup of married and divorced women (n = 115, 47.9%), the majority had 1 to 2 children (n = 81, 70.4%). While (n = 33, 28.7%) had 3 to 6 children and a solitary respondent reported more than 7 children (n = 1, <1%). A substantial proportion of the sample reported an annual income of $32 000 or higher (n = 176, 73.3%), representing the most prevalent income bracket. In contrast, a smaller segment of the sample earned between $16 000 and $32 000 annually (n = 38, 15.8%), as shown in Figure 2. In terms of educational attainment, the respondents exhibited a high level of education, with the majority holding undergraduate degrees (n = 181, 75.4%). Additionally, a significant number of participants had achieved master’s degrees (n = 26, 10.8%), while a smaller proportion held PhD degrees (n = 5, 2%), highlighting the educational qualifications of the study population. The education level distribution of the study sample, depicted in Figure 2-top left, highlights the significant representation of the healthcare sector. Most respondents (n = 160, 66.7%) were employed in the government health sector, whereas a smaller proportion (n = 39, 16.3%) were affiliated with the private health sector. The distribution of workplace settings varied notably: 22.1% (n = 44) of the respondents were working in hospitals with a capacity of 100 beds, 14.6% (n = 29) were employed in hospitals with 110 to 150 beds, and a substantial majority (n = 126, 63.3%) were working in larger hospitals with more than 150 beds, as illustrated in Figure 2-left. This distribution highlights the diverse healthcare environments in which participants were situated.
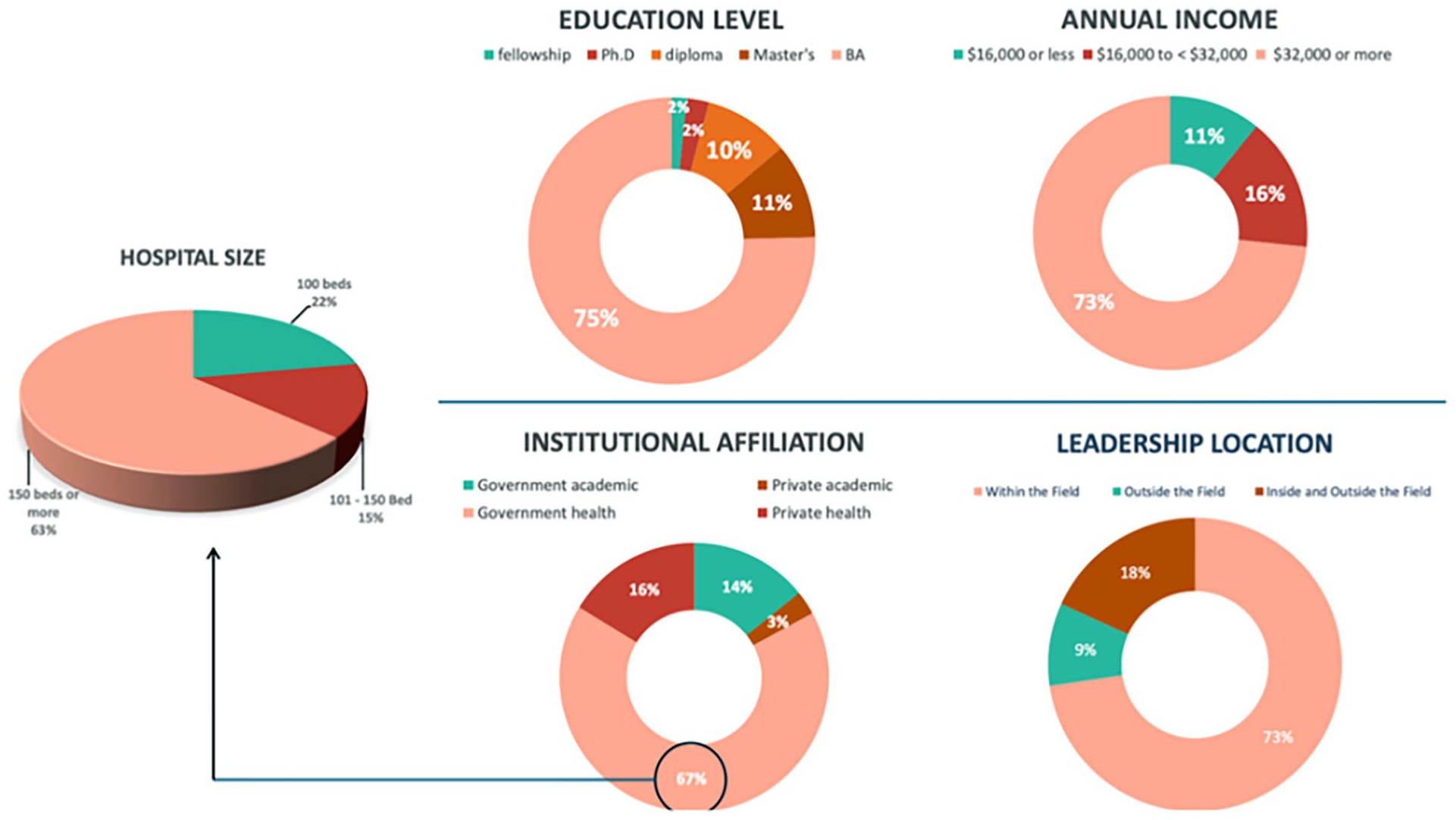
The demographic characteristics of the sample.
The findings revealed that a minority of female participants (n = 44, 18.3%) had held leadership or administrative positions. In contrast, the vast majority (n = 196, 81.7%) did not perform such roles (Figure 3). Within the subset of female leaders, most (n = 32, 72.7%) had served in leadership or administrative roles, particularly in the medical imaging field. A smaller group (n = 8, 18.2%) had held these positions outside the medical imaging field, and only a few (n = 4, 9.1%) had experienced leadership roles both inside and outside of medical imaging. Further analysis of the location of these leadership roles indicated that the majority of these positions were internal to the respondents’ institutions (n = 36, 81.8%), with a smaller fraction (n = 7, 15.9%) leading outside their institutions. Remarkably, only 1 respondent had held a leadership position both inside and outside the institution. This distribution highlights the limited internal leadership roles women undertake in healthcare institutions, particularly in medical imaging.

Female leaders’ data.
Empowerment Factors Related to Self-Esteem
The analysis of self-perception among the respondents revealed a strong sense of self-worth, with 95.8% (n = 230) affirming that they viewed themselves as equally worthy as others. Additionally, a high proportion (85.9%, n = 206) strongly agreed that they were satisfied with themselves, as reflected by a mean score of 4.26 (SD = 0.9). This sentiment extended to their professional roles, where respondents exhibited high self-esteem regarding leadership and administrative positions, achieving an average mean score of 4.29 out of 5.00 (SD = 0.62), indicating strong agreement as measured by the study tool (Table 2). Furthermore, regarding self-efficacy, 80.8% (n = 161.6) of participants either agreed or strongly agreed that they possessed effective management skills that allowed them to overcome challenging situations, yielding a mean score of 4.11 out of 5 (SD = 0.89; Table 2).
Results of Self-Empowerment Dimension of Self-Esteem and Self-Efficacy.

Empowerment Factors Related to Socio-Economic and Freedom Mobility Dimension
In the assessment of empowerment factors related to socioeconomic status and freedom of mobility, most of the study sample responded affirmatively on the Likert scale, with an average agreement score of 3.78 out of 5.00. This score implies general agreement with the economic-related aspects. Notably, the statement “I can have/ask for loans” garnered substantial agreement, with 79.6% (n = 191) of respondents agreeing (average score: 4.04 ± 0.93). Additionally, the statement concerning equality in work-related allowances between men and women also received significant agreement, with 71.3% (n = 171) of respondents affirming (average score: 3.87 ± 1.00). The study found an average agreement level of 3.46/5, aligning with the “I agree” option on the Likert scale. However, variations emerged in mobility-related aspects. Travel within the Kingdom for conferences had strong agreement (70.5%, M = 3.86, SD = 1.065), while travel abroad without restrictions saw lower agreement (52.5%, M = 3.47, SD = 1.203). Additionally, 58.4% disagreed with the freedom to switch jobs within radiology (M = 3.06, SD = 1.273), as shown in Table 3.
Results of Socio-Economical Dimension & Freedom Mobility.

Empowerment Factors Related to Environmental Factors
On the Likert scale, responses to environmental factors overall tended toward neutrality, with an average rating of 2.95 out of 5.00. For instance, less than half of the women in medical imaging, specifically 44.2% (n = 106), agreed that there was equity in the nomination process for funding training courses at work, with an average score of 3.18 (SD = 1.19). Notably, 29.2% (n = 70) remained neutral and 26.7% (n = 64) disagreed with the statement “I find equality between men and women in nominations for courses at work.” Regrettably, a significant proportion of respondents 51.6% (n = 124) did not feel supported by their work environment in terms of recognition of their talent or the provision of resources for professional development. They rated their support for maintaining gifted, hardworking, and intelligent staff at a low 2.52 (SD = 1.2). Similarly, 50.5% (n = 121) rated the availability of a library or resources for updates in the field at 2.66 (SD = 1.3; Table 4).
Results of Environmental Dimension.

Empowerment Factors Related to Institutional Dimension
Regarding the institutional dimension, participant hesitancy was observed, with an average response of 3.32 on a 5-point Likert scale, indicative of a neutral position. The data revealed a pronounced disparity in responses concerning elections and nominations for leadership roles, with a higher proportion of respondents (41.3%, n = 99) expressing disagreement than agreement (33.3%, n = 80) or neutrality (25.4%, n = 61). This disparity caused the overall mean to shift to 3.83, augmented by a standard deviation of 1.3. Conversely, the statement “I feel I belong to my work field” garnered a favorable reception, with 66.7% (n = 160) of participants agreeing, yielding a mean response of 3.63 and a standard deviation of 1.2. The detailed levels of agreement with the other statements are presented in Table 5.
Results of Institutional Dimension.

Empowerment Dimension Related to Job Factors
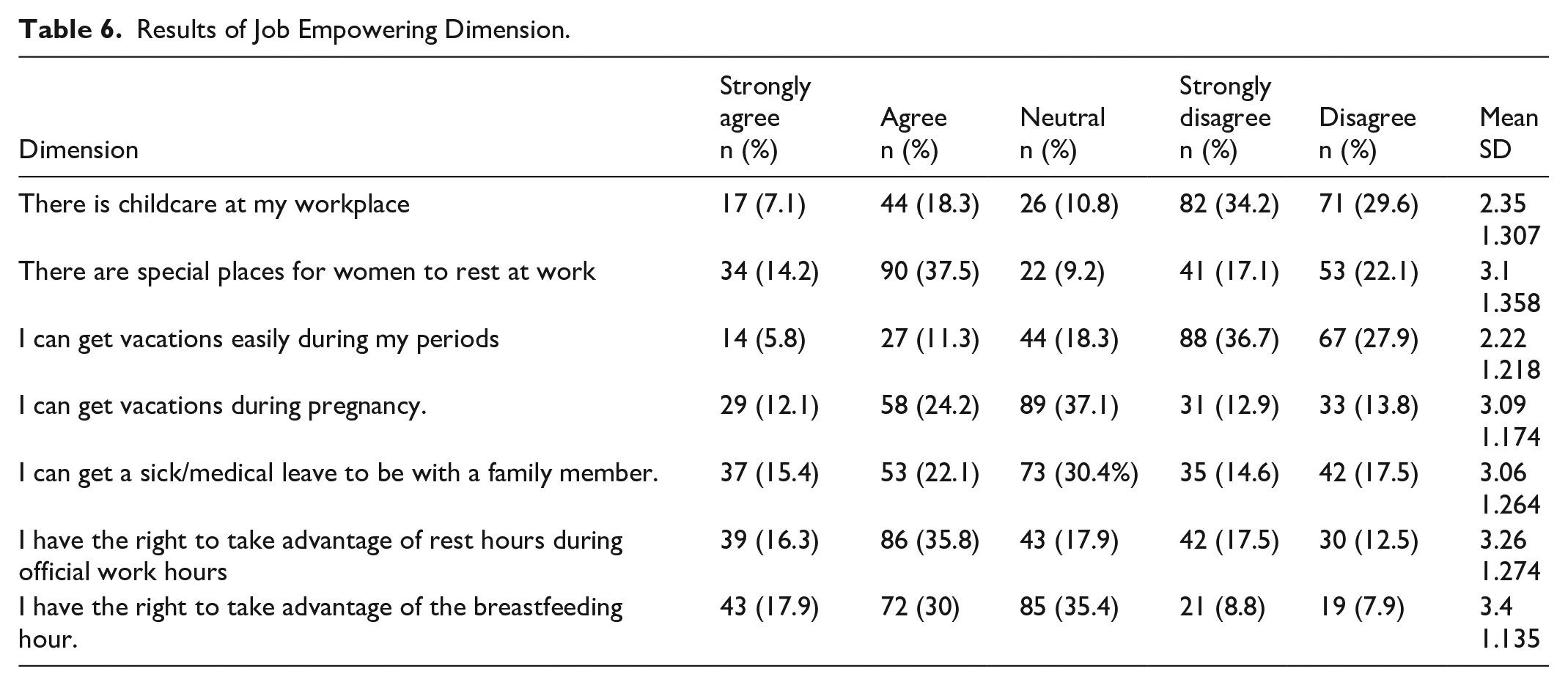
The study sample suggested a neutral position on factors concerning the leadership and administrative roles of women in the workplace, with an average score of 2.92 out of 5.00, falling within the neutral category of the Likert scale (2.61-3.40). Notably, there was a variation in agreement levels regarding workplace situations, with scores ranging from 2.22 to 3.40, straddling the lower and upper neutral bounds of the scale, indicating varying degrees of disagreement to neutrality. This variation is particularly evident in responses to specific statements, such as “It is my right to benefit from the first hour of breastfeeding,” which received the highest neutrality score of 3.40; followed by “It is my right to benefit from comfort hours during official tenure,” scoring 3.18; and “Special places for women to relax during work hours” with agreement of 3.06. Conversely, statements indicating disagreement included “There is childcare provision at my workplace,” which received the lowest agreement at 2.35; and “I can easily obtain leave during my menstrual period,” which scored 2.22, highlighting areas of significant dissent within the study sample regarding specific workplace/job suitability for women (Table 6).
Results of Job Empowering Dimension.
Challenges Facing Women Empowerment
Figure 4 shows that the top challenge for women in this study is work-life balance (54.6%, n = 131), followed by long working hours (52.5%, n = 126). Societal restrictions affected 42.1% (n = 101), while 41.3% (n = 99) struggled with childcare during work. Lastly, 33.4% (n = 80) reported negative attitudes toward women in leadership.

Challenges facing women empowerment.
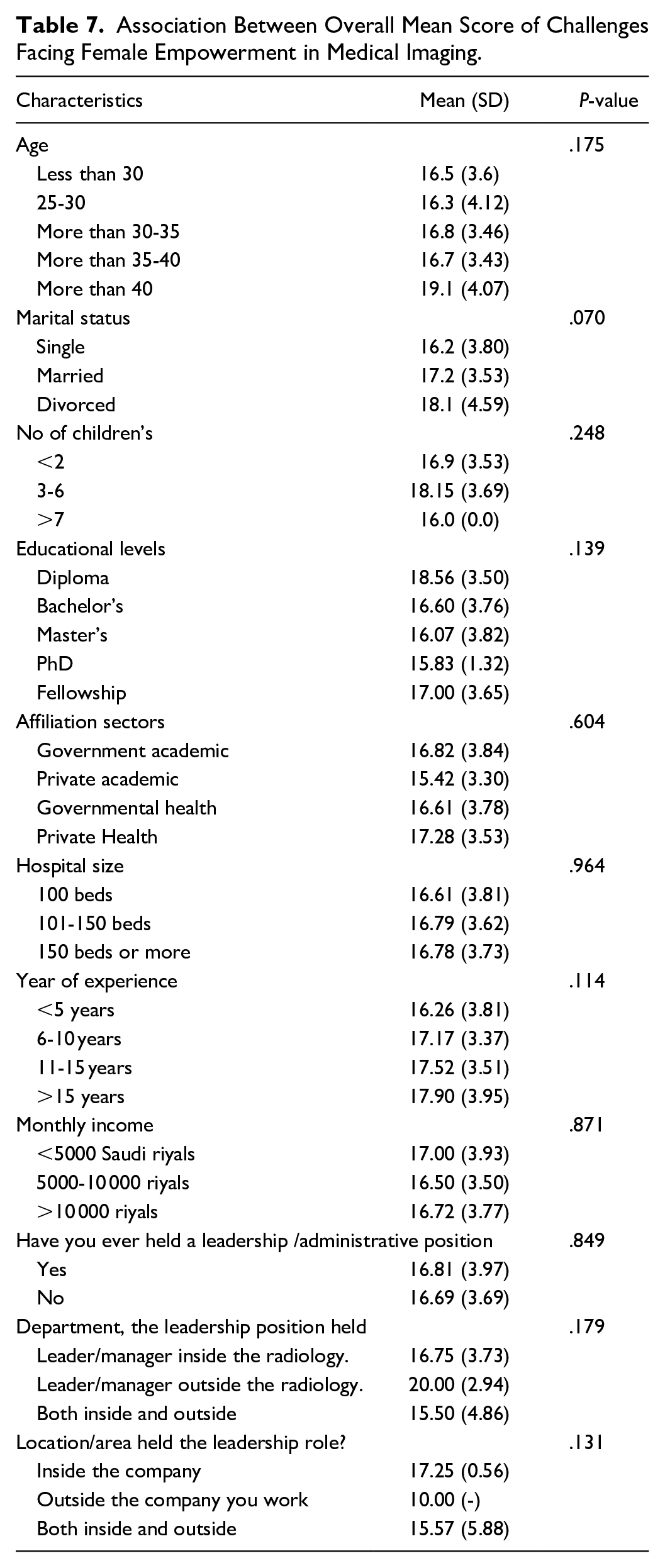
Table 7 shows no significant association was observed between the mean scores of the challenges faced by Saudi women and various demographic characteristics. Notably, women over the age of 40 reported a higher mean score of challenges (19.1 ± 4.07) than their younger counterparts. However, this difference was not statistically significant (P = .175). Similarly, women holding diplomas reported a higher mean score of challenges (18.56 ± 3.50) relative to those with other academic degrees, even though this variation also lacked statistical significance (P = .139). Additionally, women with over 15 years of experience indicated a higher mean score of challenges (17.90 ± 3.95) than those with fewer years of experience, with no significant difference observed (P = .114).
Association Between Overall Mean Score of Challenges Facing Female Empowerment in Medical Imaging.
Discussion
Since the announcement of Saudi Vision 2030, enhancing women’s empowerment has been a key objective, with specific goals, including a 30% increase in women’s participation in the labor market by 2020. This study investigates the status of women in leadership and administrative positions within the field of medical imaging, serving as a microcosm for examining broader global trends and the specific impact of Saudi Vision 2030 on women’s empowerment. Key factors affecting female empowerment and the challenges faced in this sector were assessed. Having an administrative role in the field of medical imaging reflects an empowering status and indicates effective leadership and influence in the field. This enables a role-modeling function for future generations. Unexpectedly, our study revealed that most of the sample (81.7%) had never held leadership or administrative positions. This is supported by research on underrepresented academic women in the field of radiology in the U.S., despite having comparable levels of experience to men.21,22 We know that female representation in nursing within Saudi Arabia is significantly high. 28 Nursing in Saudi Arabia has historically demonstrated high female representation, largely driven by prevailing societal norms favoring women in caregiving roles. But the overall high female representation in nursing within Saudi Arabia might be substantially influenced by foreign workers, primarily from India, the Philippines, and Malaysia, 29 further complicating direct comparisons with medical imaging, where workforce demographics and cultural expectations differ significantly. In medicine, although women represent over half of medical school students and graduates in Saudi Arabia, they account for only approximately one-third of physicians employed by the Ministry of Health. 30 This disparity may partially be explained by the higher levels of burnout experienced by female medical students and practitioners. 31 When evaluating female representation across healthcare fields, direct comparisons between medical imaging and nursing in Saudi Arabia should be approached cautiously due to distinct societal and demographic factors influencing each profession. This underrepresentation of women in healthcare leadership is not unique to Saudi Arabia. Globally, women constitute a significant majority (more than 70%) of the healthcare workforce.32-34 However, they hold a disproportionately small percentage of leadership positions. In the U.S., women account for only 20% of department chairs in academic medicine, and fewer than 18% of radiology journal editorial board members are women. 35 Further findings, increased female representation in journal leadership correlates with greater visibility of women in the field, though progress in attaining top leadership positions is slower. 35 Studies indicate that women occupy only about 25% of senior leadership roles in the healthcare sector in North America . There is significant gender gap in medical imaging as women make up only 25% of radiology residents. 36 The proportion of academic offices held by women ranges from 11% to 40%, reflecting significant variation and uneven access to leadership pathways. Again, female representation on hospital boards of directors stands at just 14%, while only 18% of hospital CEOs are women. Even in top administrative roles, women account for just 38%, indicating that although some progress has been made, substantial gender gaps persist at the highest levels of decision-making. 37 Astute reader can see that women’s representation in healthcare leadership remains limited, with notable disparities across roles.
A significant finding from our research is the youth demographics of our sample, with 67.5% under 30 years, reflecting a surge in female graduates following the Saudi Vision 2030 empowerment initiatives. 38 This upsurge in women’s presence in medical imaging jobs is supported by broader societal and cultural shifts that favor the empowerment of women, underscoring the critical role of macro-level factors, such as government policies. Previous studies showed that micro-level factors such as personal and familial influences affect the empowerment of women. Nevertheless, the macro-level elements (ie, society, culture, organizations, and governmental initiatives) are pivotal for rapid and effective empowerment. This study identified high levels of self-esteem and self-efficacy among participants. This suggests that the respondents valued themselves highly and felt competent at managing stress and maintaining professionalism under pressure. These traits are crucial internal predictors that should be considered when designing empowerment programs to enhance women’s leadership. This alignment of individual capabilities with systemic support highlights a dynamic framework through which women’s leadership can be effectively promoted. 24 These findings suggest that self-esteem and self-efficacy are integral components of programs aimed at fostering female leadership. The significant correlations between these internal factors and leadership efficacy highlight their potential to overcome workplace barriers. Low self-esteem, a notable limitation identified in previous studies, generally results in women avoiding leadership roles and settling for passive participation without decision-making power. Thus, enhancing psychological assets through empowerment initiatives may enable women to assume leadership positions. This approach promises to promote individual empowerment and drive transformative changes across organizational cultures.25,39,40 Despite these positive indicators, the disparities persisted. In our sample, women continued to hold fewer tenured positions and experienced slower career progression than their male counterparts, a trend that persisted despite increased female participation in radiology over the past 40 years. 41 This phenomenon is observed globally, with minimal representation of women on editorial boards and their absence from top editorial roles across various fields. 35
Furthermore, regarding economic aspects within the Saudi context, participants reported equity in wages, promotions, and access to investment opportunities as mandated by the National labor system. 42 This contrasts starkly with the global issue of gender wage gaps, which are frequently unexplained by factors such as seniority or career breaks. 43 The persistent wage gap in academia, exacerbated by the challenges women face when negotiating salaries, underscores the critical international issue of empowerment of women. 44 This aligns with other studies, reinforcing that salary disparities remain a significant barrier to achieving global gender equity.22,45-47 Wage inequality is a global issue with significant repercussions for women’s participation in the workforce, often resulting in reduced job opportunities and limited chances for leadership roles. This pattern is observed universally across various sectors, including the demanding field of radiology, where the stress of the work, combined with insufficient financial compensation, discourages women from pursuing or maintaining leadership roles.22,45 However, this is not the primary deterrent in the Saudi Arabian context, where recent reforms and initiatives have supported an increase in women assuming leadership positions in medical imaging. This divergence highlights the impact of targeted national policies and reforms in addressing some of the universal challenges faced by women in professional environments.
In addition, our study explored the freedom of mobility of Saudi women in medical imaging, a field that was previously constrained. 48 Recent reforms under Saudi Vision 2030, such as the legalization of women’s driving and removal of travel restrictions without a male guardian, have significantly enhanced women’s independence and empowerment. In the historical context described in the book “Gender, Class, Nationality, and Women’s Access to Public Places in Riyadh,” Saudi women encountered numerous obstacles that impeded their empowerment and independence. 49 Several factors have contributed to the historical underrepresentation of women in public spaces, including (a) the prohibition of women’s driving, (b) inadequate public transportation infrastructure, (c) the financial burden of hiring private drivers, and (d) the absence of anti-harassment legislation—factors that collectively restrict women’s mobility and freedom. These barriers significantly limit women’s public engagement and access to opportunities. 49 However, these challenges, deeply ingrained in various facets of their lives, have been addressed through progressive reforms under Saudi Vision 2030. Concerted government efforts have been made to dismantle these barriers, setting a framework to prevent their reoccurrence, marking a definitive step toward a future where such limitations will not persist.
Limited access to transportation intensifies “hidden” barriers that hinder women’s participation in the labor market, restricts their access to essential services such as education and healthcare, and ultimately diminishes their empowerment. These transportation barriers limit physical mobility and contribute to broader socioeconomic disadvantages, hindering progress toward gender equality and empowerment.50,51 The reforms initiated under Saudi Vision 2030 have significantly contributed to the empowerment of women, particularly in terms of freedom of mobility, which is a crucial factor in advancing leadership and administrative roles. The study’s findings revealed an overall positive perception among participants concerning mobility freedom, with an average agreement level of 3.46 on a 5-point Likert scale. This suggests that policy changes have been somehow effective in enhancing women’s mobility rights in the Kingdom. Several obstacles have been resolved, and solutions are still being implemented by the government. Since 2018, significant advancements have been made in the realm of women’s rights in Saudi Arabia. Notably, these include the authorization for women to drive, the issuance of driving licenses, and the swift enactment of harassment laws. The Saudi Human Resources Development Fund introduced the “Wusool” program, which is designed to bolster women’s participation in the workforce. Specifically, by targeting newcomers in the private sector, this initiative addresses transportation barriers that often hinder women’s employment, thereby enhancing job stability. This strategic approach supports women’s entry and retention in the job market and aligns with broader national objectives to empower women economically. This is evidenced by an average score of 3.86, indicating that these changes have fostered greater participation of women in domestic professional development activities. The “Wusool” program provides financial assistance for transportation costs to eligible workers, covering up to 80% of the cost and lasting 24 months. 52 The substantial agreement rate of 70.7% concerning the ease of internal travel for participation in conferences and events indicates the beneficial impact of recent reforms on women’s mobility within the Kingdom. This consensus among participants regarding freedom of mobility corroborates our findings, illustrating the effectiveness of these reforms in enhancing internal mobility and, consequently, creating more professional engagement opportunities for women.
Conversely, the lower agreement level (52.5%) regarding the ability to travel internationally without restrictions suggests that while domestic mobility has improved, international mobility still presents challenges. Although women have technically had the freedom to travel outside the Kingdom without a guardian since 2019, the relatively low level of agreement indicates that additional, less visible barriers that impact their ability to travel remain. This discrepancy warrants further investigation to identify and address the underlying factors contributing to this restraint. A notable disagreement (58.3%) was observed regarding the freedom to transfer between jobs within the medical imaging field, with many respondents feeling restricted by unclear policies. This was reflected in the lower average score of 3.06. This highlights the broader issue of policy transparency and implementation, which affects both domestic job mobility and international travel opportunities for women in this sector. Such policy gaps may hinder physical mobility and could extend to broader workplace dynamics that influence career progression and satisfaction among women.
In addition, despite the high levels of loyalty and passion for their careers and institutions expressed by the participants, a lack of tangible efforts from workplaces to nurture and motivate talented, hardworking female employees has been observed. This disconnect between employee dedication and organizational support further emphasizes the need for comprehensive policies and cultural shifts within workplaces. Studies have confirmed that having talented women in leadership positions benefits final work outcomes and enriches the organization from diverse perspectives.53,54 Nevertheless, the Women in the Workplace 2017 report revealed that although women represent 52% of the U.S. population, they constitute only 20% of leadership roles.55,56 This demonstrates the difficulty women face in reaching the top. In the recruitment process, institutions can implement several strategies to foster gender diversity and empowerment, such as: (a) forming a diverse selection committee that includes prominent female leaders to interview candidates. 57 Our findings highlight a critical gap in workplace support, particularly regarding a lack of nurseries and childcare facilities. A key to enabling the full participation of women in the workplace involves instituting policies that address these gender-specific needs. An intriguing aspect of our findings was that the participants identified a lack of supportive policies for menstrual leave as a significant barrier in the workplace. Menstrual discomfort can affect performance and attendance. 58 However, this is often overlooked in standard workplace policies. 59 The absence of provisions for menstrual leave not only impacts women’s health and well-being but also reflects broader issues of gender sensitivity and inclusivity in organizational policies. Such inclusive policies can support working mothers and contribute to an environment that values workplace flexibility. One illustrative initiative is the “Qurrah” Subsidy Program, launched by the Saudi Child Welfare Authority to assist working mothers by providing childcare while they engage in employment opportunities within the private sector. 60 This explains the increasing number of women entering the medical imaging field. Such programs highlight the importance of supportive measures for female employees to promote continued professional engagement and growth. The effectiveness of these measures is further evidenced by the increasing participation of women in the medical imaging field, as indicated in our study. This trend illustrates the positive impact of targeted institutional policies that recognize and address the unique challenges women face in balancing professional and personal responsibilities.
Another persistent issue is related to long working hours. This issue can significantly limit work-life balance, contributing to burnout and decreased job satisfaction, which are particularly detrimental in high-stress environments such as medical imaging. Furthermore, the lack of development opportunities and the inability to participate in professional gatherings hinder personal and professional growth and limit women’s ability to stay updated with technological and methodological advancements in their field. 61 To mitigate the adverse effects of the identified barriers, participants suggested the implementation of part-time job opportunities and recognition of exemplary employees through monthly awards for the most accomplished worker. Participants also advocated the establishment of programs aimed at fostering the development of women’s skills in management and leadership. This recognition not only rewards merit but also encourages a culture of excellence and motivation among employees. 62 The workplace should also implement comprehensive training and development programs to address issues such as unconscious bias, negotiation techniques, and principles of equity. These interventions are crucial for fostering an environment that supports gender equity and empowers women to reach leadership roles. The underrepresentation of women in leadership positions in our study is partly due to the demographic composition of the sample—49.4% were recent graduates and 60.4% had less than 5 years of work experience. This observation aligns with previous studies that showed a predominance of women in lower-ranking positions as opposed to senior roles.63,64 However, data suggest that men are more likely to ascend to managerial positions more rapidly than women, 65 indicating a potential systemic bias or lack of support mechanisms that facilitate women’s career progression in leadership roles. Furthermore, the literature supports this observation by indicating that women are 18% less likely to be promoted than their male counterparts. 53 To address this imbalance, targeted mentorship programs and leadership training should be specifically designed to empower women and promote gender equity in managerial roles. Without supportive policies, talented employees may fall behind or be unable to reach their full potential in their careers.22,53 Global interventions such as Executive Leadership in Academic Medicine (ELAM) program in the U.S. has been instrumental in preparing women for top leadership roles. 66 These programs focus on mentorship, leadership competencies, networking, and executive coaching. Another leading initiative by Norway, Spain, Iceland, and France who introduced Corporate Board Quotas (CBQs) which mandates a 40% quota for women on corporate and public sector boards, 67 which has directly increased female leadership representation. Australia’s Workplace Gender Equality Agency (WGEA) set an exemplary act that tracks and incentivizes organizations to improve gender equity through annual reports, benchmarking, and certification. 68 While these global initiatives offer promising models for promoting gender equity and increasing female leadership, their long-term success also depends on retaining women in the leadership pipeline, an area where many countries, including Saudi Arabia, continue to face persistent challenges, particularly within academic and healthcare sectors.
Another attribute of underrepresentation in leading positions and advanced ranks is the lack of retention of women, particularly in academia. 69 This phenomenon may be amplified by the scarcity of role models and inadequate mentoring, which discourages women from pursuing leadership or administrative positions. 45 To counteract this trend, a supportive workplace environment should be developed. By implementing robust mentoring programs to nurture the talent of women, organizations can help them realize their full potential and effectively address the “leaky pipeline” issue, which is especially prevalent in the medical field. 46 Another reason is that women miss these opportunities because of familial obligations and societal expectations regarding parenting and domestic responsibilities. 70 We recommend implementing family friendly policies and promoting a culture of work-life integration at the institutional, departmental, and individual levels, tailored to acknowledge and accommodate gender-specific challenges. 71 These enhancements can be achieved through flexible working hours and support systems for employees returning after maternity breaks or leaves. Workforce policies should include provisions for breastfeeding or lactation breaks for new mothers, recognizing that Saudi working women have the right to conditional paid maternity leave for up to 3 years after childbirth. To further support this, women returning to work within 24 months postpartum should be entitled to paid breastfeeding breaks totaling no more than an hour per day. 72
Limitation of the Study
Initially, our study aimed to target Saudi women aged 25 or older, focusing on those likely to have some professional experience and potential leadership roles within the medical imaging field. However, the significant participation from women younger than 25 altered our perspective. This outcome underscores a crucial development in the sector, likely catalyzed by the progressive initiatives under Saudi Vision 2030. The early professional entry and aspirations for leadership roles among this younger cohort highlight a transformative shift in women’s empowerment in Saudi Arabia. This shift has broadened the scope of our study, indicating that Saudi Vision 2030 is fostering a new generation of women who are not only entering the workforce earlier but are also equipped with strong educational backgrounds and empowerment aspirations significantly sooner than previous generations. This study presents several considerations that influence the interpretation of the findings. First, the sample included a significant number of recent graduates who lacked extensive work experience. This characteristic reflects the dynamic changes occurring in Saudi Arabia as part of Vision 2030, which introduced academic programs and employment opportunities previously unavailable to women. Second, the data collection method relied on self-reported online surveys, which, while convenient, may have affected the data reliability. Additionally, the cross-sectional nature of the survey captures only a single moment in time, and combined with the relatively small sample size, limits the ability to generalize these findings to all female medical imaging workers, both in Saudi Arabia and worldwide. This study employed self-reported questionnaire data, which inherently carries a risk of response bias. Participants’ perceptions and personal experiences regarding empowerment and challenges faced could lead to overestimation or underestimation of these barriers. However, this provided valuable firsthand insights into participants’ personal experiences and perceptions of empowerment and barriers. While self-reporting can introduce response bias, it also enables authentic and direct representation of participants’ lived experiences, capturing nuanced views that quantitative measures alone might overlook. Thus, the data offers meaningful and rich perspectives essential for understanding and addressing the real-world challenges faced by Saudi women in the medical imaging field. One limitation of this study is that we did not perform multivariate analysis, which could have adjusted for potential confounding variables such as age, marital status, years of experience, and employment sector. Given the exploratory nature of this research, the focus was primarily on identifying baseline trends and group-level differences. However, future studies should incorporate multivariate approaches, such as logistic regression or multiple linear regression, to better assess the independent effects of various factors on leadership engagement and empowerment outcomes.
Future research should explore the impact, effectiveness, and scope of women’s empowerment in leadership and administrative roles. A systematic longitudinal evaluation of women’s empowerment is imperative to accurately monitor the trajectory of their roles in the medical imaging sector and determine their alignment with Saudi Arabia’s Vision 2030 objectives. This evaluation requires collaboration between various private and government entities to enhance access to comprehensive databases that accurately track the number of women in leadership and administrative positions within the specialty. The duration of tenure in these roles and their impact during this period must also be considered. Access to such data could provide valuable insights into women’s workforce participation, support targeted efforts to improve their representation in these roles, and evaluate the effectiveness of their contributions over time. Adopting diverse recruitment committees, including several prominent women in the hiring process, can help ensure a more equitable selection mechanism. Additionally, initiatives aimed at empowering women should incorporate measures of self-efficacy and self-esteem as predictors of empowerment. Moreover, both macro- and micro-level factors, including societal, cultural, familial, and personal dynamics, must be comprehensively addressed, as they play pivotal roles in facilitating women’s empowerment.
Conclusion
Saudi Vision 2030 has undeniably spurred significant progress in women’s overall workforce participation in Saudi Arabia, a substantial underrepresentation of women persists in leadership roles within the specific field of medical imaging. Such reforms have advanced female profession, evidenced by improved wage equity and access to senior roles. Women remain underrepresented in decision-making positions, highlighting the need for both policy enforcement and cultural shifts. Addressing structural, personal, and familial barriers through initiatives like “Wusool” and family-friendly policies shows promise but requires expansion and evaluation. To strengthen women’s leadership in medical imaging and healthcare, a multi-faceted strategy is essential. Establishing structured mentorship programs, implementing gender quotas, and launching leadership development initiatives that foster self-efficacy and essential management skills. Flexible work arrangements, such as part-time options and childcare support, should be integrated into institutional policies to better support working mothers—particularly those in or aspiring to leadership roles. Equally important is the introduction of inclusive policies that recognize gender-specific needs, such as menstrual and lactation leave, while promoting a culture of recognition through regular awards and amplify visibility of female role models. Addressing unconscious bias through mandatory training and embedding equity principles into institutional frameworks is also vital. Create dedicated platforms and networks for women in medical imaging to connect, share experiences, access resources, and support each other’s professional growth. Lastly, tracking progress through gender-disaggregated data and fostering public-private sector collaboration will ensure the sustainability and effectiveness of these empowerment efforts. Sustainable progress demands a holistic approach combining political, societal, and personal empowerment. Collaboration among government, private sectors, and communities is essential to create inclusive, thriving opportunities for women across professions.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251340172 – Supplemental material for From Self-Efficacy to Disparities in Institutional Support: A Cross-Sectional and Multi-Dimensional Evaluation of Women in Empowerment and Leadership in Radiology Under Vision 2030
Supplemental material, sj-docx-1-inq-10.1177_00469580251340172 for From Self-Efficacy to Disparities in Institutional Support: A Cross-Sectional and Multi-Dimensional Evaluation of Women in Empowerment and Leadership in Radiology Under Vision 2030 by Ashwag Rafea Alruwaili, Alanoud Abdullah Alzahrani, Hajar Abdullah Almater, Lina Abdualaziz Aldibas, Nawal Farah Al anazi, Asma mohammed albanyan and Wadha Alyami in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors extend their appreciation to The Central Research Laboratory/ Research Institute/ Center Supporting Program (RICSP-25-3), King Saud University, Riyadh, Saudi Arabia.
Prince Naif Health Research Center, Investigator support Unit for the language editing service provided
Authors would like to acknowledge and extend our deepest gratitude to the remarkable women who generously participated in this research study. Your voices have added depth to our findings, and we hope that the insights gained from this study will contribute to the betterment of women empowerment all around the world.
Author’s Note
Alanoud Abdullah Alzahrani is now affiliated to Saudi Industrial Development Fund, Riyadh, Saudi Arabia.
Ethical Considerations
The study received approval from the Institutional Review Board (IRB) at King Saud University Medical City (KSU-MC) under the approval number E-21-6532.
Consent to Participate
Participants were informed of the study’s purpose and their rights, and informed consent was obtained through an explicit question in the survey.
Author Contributions
ARA: Conceptualization, Project administration, Methodology (questionnaire design/validation), Writing—review and editing (journal finding and submission). AAA: Writing—original draft (methods section), Writing—review and editing (proposal), Project administration (IRB submission). HAA: Methodology (questionnaire design/validation), Writing—original draft (literature review), Writing—review and editing (proposal). LAA: Formal analysis (statistical analysis), Validation (results interpretation), Writing—review and editing (proposal). NFA: Writing—review and editing (proposal), Project administration (IRB submission). AMA: Writing—original draft (discussion), Methodology (questionnaire final editing). WA: Writing—original draft (discussion).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by The Central Research Laboratory/ Research Institute/ Center Supporting Program (RICSP-25-3), King Saud University, Riyadh, Saudi Arabia
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.