
Abstract
This study aimed to determine whether the Korean version of the Berg Balance Scale (BBS) is suitable for assessing the balance ability of patients with spinal cord injury. The results of the Korean version of the BBS were collected from 80 patients with spinal cord injury. The collected data were analyzed using Rasch analysis to determine the suitability of participants and items, item difficulty, rating scale, and separation reliability. Of the 80 participants, 7 were evaluated as unsuitable participants, and 1 of 14 items was judged unsuitable. Item 7 was unfit, “standing unsupported with feet together.” Item 14, “standing on 1 leg,” was the most difficult, and item 3, “sitting unsupported,” was the simplest. The results of the rating scale analysis showed that a four-point scale (0-3 points) was appropriate when administering the Korean version of the BBS to patients with spinal cord injury. The separation reliability for the items was 0.99, and the separation reliability for the participants was 0.97. The reliability and validity of the Korean version of the BBS were verified by applying Rasch analysis to patients with spinal cord injury. Based on the results of this study, the Korean version of the BBS is suitable for evaluating the balance ability of patients with spinal cord injury. It is expected to provide evidence for clinical use.
Highlights
This study verified the validity of the Korean version of the Berg Balance Scale (BBS) for spinal cord injury patients using Rasch analysis.
A four-point rating scale was found to be more suitable than a five-point scale for assessing balance in spinal cord injury patients.
The Korean version of the BBS demonstrated high reliability and sensitivity, making it an effective tool for evaluating balance in clinical settings.
Introduction
Worldwide, more than 15 million individuals suffer from spinal cord injury, and 250 000 to 500 000 individuals suffer from acute spinal cord injury each year due to traffic accidents, falls, and violence, among others. 1 Spinal cord injury causes complete or incomplete loss of motor and sensory functions below the level of the lesion, 2 which can lead to complications including bedsores, joint contractures, osteoporosis, and sexual dysfunction. 3 In addition to the loss of physical function, spinal cord injury affects psychological and social factors, and its permanent sequelae place a significant burden on the healthcare system, family, and community participation. 4
The American Spinal Injury Association Impairment Scale is a scale that classifies spinal cord injury by considering motor and sensory functions by the American Spinal Injury Association (ASIA). Further, it objectively quantifies the degree of spinal cord injury and indicates the status of recovery. 5 The sensory score can be used to check whether tactile and pain sensations are preserved, and sensory preservation below the level of injury is used as a valuable indicator for motor recovery. 6 The motor score is used as an international standard to quantify muscle strength and degree of paralysis after spinal cord injury, 7 and can predict upper limb and hand function, balance ability, and functional mobility ability. 8
The recovery prognosis of spinal cord injury varies depending on whether it is complete or incomplete, and incomplete injury has a better prognosis in terms of functional recovery. 9 Patients with complete spinal cord injury have reduced physical activity compared to before the injury and mainly lead a sedentary lifestyle dependent on a wheelchair, 10 which makes upper body muscle strength, balance ability in a sitting position, and trunk control function essential factors for performing functional activities such as wheelchair propulsion. 11 Conversely, 86% of patients with incomplete spinal cord injury recover walking ability and have the potential to walk. 12 Therefore, balance ability in a standing position is vital in daily functional activities and mobility. 13
Balance is essential for posture control during periodic movement tasks such as sitting or standing upright, walking, and running, including for non-periodic tasks such as starting to walk or performing complex movements. 14 Previous studies have shown that balance ability is necessary to properly maintain one’s body for successful activities of daily living. 15 Balance control is essential for daily activities, and various balance abilities are required depending on the specific task. 16
Factors affecting this balance include various functional aspects such as vision, hearing, proprioception, muscle strength, and endurance. 17 Patients with spinal cord injury have balance problems due to partial or complete loss of somatosensory perception and difficulty in voluntary movement control. 18 Impaired balance makes it difficult to maintain normal posture, which affects the ability to perform activities. 19 Additionally, it is directly related to safety issues such as falls, leading to severe injuries such as fractures, and psychological factors such as depression and anxiety, leading to activity restrictions. 20 This ultimately reduces the ability to participate in productive activities in the community. 13 Therefore, improving postural control and balance ability is essential to improve the function of patients with spinal cord injury, lead an independent life, and promote community participation. Furthermore, the use of assessment tools to apply customized rehabilitation programs aimed at this goal is essential.13,21,22
Currently, in clinical practice, the modified functional reach test (mFRT), timed up and go test (TUG), and Romberg test are used to evaluate patients’ balance with spinal cord injury.23 -25 The mFRT measures the distance the arm is extended forward from a sitting position, which can evaluate dynamic balance ability. 26 The TUG measures the time it takes to walk 3 m on a chair with armrests, return to the chair, and sit down again to measure functional mobility ability. 27 The Romberg Test is an evaluation that observes the degree of posture maintenance by placing both feet together with eyes open or closed. It can confirm static balance according to proprioception. 28 These tools have limitations in evaluating patients with spinal cord injury who show various clinical characteristics depending on the level of injury, 8 and there are time constraints in using all tools to evaluate balance ability.
To address these issues, tools that can evaluate both static and dynamic balance simultaneously are being developed and used.29,30 Among these tools, the Berg Balance Scale stands out as it can comprehensively assess posture maintenance, voluntary movement control, and reflex ability to external factors. It achieves this by incorporating movements commonly performed in daily life. The Berg Balance Scale is widely used in clinical settings. 31 Each item is evaluated from 0 to 4 points according to performance. Moreover, it comprises detailed items that objectively evaluate static and dynamic balance ability in various postures such as sitting, standing, and posture changes. 31 Further, several previous studies have proven the BBS to be a valid assessment tool for posture control, balance, and mobility. Furthermore, it is frequently used to assess balance ability in clinical settings.32 -34
According to previous studies, the inter-rater reliability of the BBS was verified in Spanish spinal cord injury patients. 22 The validity and reliability of the BBS were verified in Swiss spinal cord injury patients. 35 Additionally, a study proved the clinical usefulness of using the BBS to measure the balance ability of patients with spinal cord injury. 23 These research results confirmed that the Berg Balance Scale is a tool that can precisely assess balance ability by considering the functional characteristics of patients with spinal cord injury at each level. There have been studies in Korea that have verified the reliability and validity of assessment tools targeting patients with lower limb amputations and hemiplegia.33,34 However, there is a lack of studies targeting patients with spinal cord injury.
Rasch analysis converts an item’s score system from an ordinal to an interval scale and accurately analyzes the validity of an assessment tool36,37 It is helpful for analyzing repeatedly measured assessment tools to identify clinical changes in the rehabilitation process, such as assessing a patient’s functional status or predicting functional prognosis. 38 Recent domestic and international studies have utilized Rasch analysis to develop or verify new assessment tools. Studies verifying the validity of BBS through Rasch analysis can also be found.39 -42
Therefore, the present study investigated the suitability of the Korean version of BBS to evaluate the balance ability of patients with spinal cord injury. It verified its validity by applying Rasch analysis to analyze the suitability of participants and items, item difficulty, rating scale, and separation reliability.
Methods
Participants
This study was a retrospective study conducted with approval from the Institutional Review Board (IRB) of Kangwon National University (KWNUIRB-2024-06-004-001), granted on September 4, 2024. The requirement for informed consent was waived by the IRB due to the retrospective nature of the study. All procedures performed in this study adhered to the ethical principles outlined in the Declaration of Helsinki, as revised in 2013. The research participants were 80 patients diagnosed with spinal cord injury who were admitted to a rehabilitation hospital in K City. Data collection involved selecting patients who completed the BBS evaluation among those hospitalized from January 2023 to April 2024. The general characteristics of the research participants are shown in Table 1.
General Characteristics of Participants (N = 80).

Instruments
Berg Balance Scale
The BBS, developed by Catherine Berg in 1989, was initially designed to assess the risk of falls in older adults. Since then, it has been widely used to evaluate the physical balance ability of older adults and patients with central nervous system diseases. These include stroke, traumatic brain injury, cerebral palsy, Parkinson’s disease, and dementia. The BBS has the advantages of being inexpensive and time-consuming, including having simple equipment and preparation required for assessment. It comprises 14 assessment items. Each scored on a five-point scale from a minimum of 0 to a maximum of 4 points. A higher score is given when the amount of assistance is less, the task is performed independently, and the total score is 56 points when all items are performed flawlessly. It takes 15 to 20 min to perform all assessment items, and a higher total score indicates a better balance ability of the participant. The inter-rater reliability of the BBS is r = .96, and the construct validity is r = 0.80 to 0.98, showing very high reliability and validity. 43 The Berg Balance Scale-Korean version evaluated on stroke patients showed very high reliability with intra-rater reliability of r = .95 and inter-rater reliability of r = .96. 44
Analysis
This study followed the EQUATOR network’s Rasch Reporting Guideline for Rehabilitation Research (RULER) checklist. The research methods, analysis, and reporting of results were based on the guidelines in the checklist (Appendix 1). 45
The participants’ general characteristics were analyzed by frequency using the SPSS Windows software version 23.0. After collecting the results of the BBS evaluation conducted on patients with spinal cord injury, the collected data were analyzed for the fit and difficulty of the participants and items, the rating scale, and the separation reliability using Winsteps (Winsteps, Chicago, IL, U.S.A.) version 3.80.1.
The items and misfit participants were excluded based on the model fit statistics. If the mean square residual value of the infit index of the item was less than .6 or greater than 1.4 and the Z value was less than −2 or greater than 2, the item was judged as an infit item. If the mean square residual value of the infit index was less than −2 or greater than 2 and the Z value was less than −2 or greater than 2, the subject was judged as an infit subject. 46
The suitability of the rating scale was judged to be an appropriate scale category when the mean square residual of the outfit index was 2.0 or less or the observed average showed a vertical ordering, and when the step calibration interval of the adjacent scale was 1.0 logit or more and 5.0 logit or less. 47 The numerical ordering of the average measurements means that the responses to each item were not concentrated on a specific scale but showed balanced responses. The step calibration means that the average measurement interval between each scale was standardized and corrected. In the case of an inappropriate scale, the scale was reset by integrating it with the previous or subsequent scales to meet the criteria of the rating scale and then analyzed.
Finally, a separation reliability analysis was conducted for the items and participants. The separation reliability of the items is to find out how consistently each item measures what it is intended to measure. Moreover, the separation reliability of the participants is to determine whether the assessment tool can estimate the factor it intends to measure equally even when the subject group changes. The separation reliability for items and participants was judged to be acceptable if the separation reliability coefficient was 0.70 and the separation index was 1.5 or higher, good if the separation reliability coefficient was 0.80. The separation index was 2.0 or higher, and excellent if the separation reliability coefficient was 0.90. The separation index was 3 or higher.36,46
Results
Analysis of the Suitability of Participants and Items
The fit analysis showed that 7 out of 80 participants were unsuitable because the mean autoregressive residual of the internal consistency index was less than −2 or greater than 2, and the z-value was less than -2 or greater than 2. The fit analysis of the items was performed on 73 participants, excluding the 7 participants. The item fit results showed that Item 7 of the 14 items was considered non-conforming: “standing unsupported with feet together” (Table 2).
Item Fit Statistic.

Delete item.
Item Difficulty Analysis
The 13 items of the Berg Balance Scale-Korean version are listed in order of difficulty, except for 1 item that was judged inappropriate (Figure 1). The left side of Figure 1 shows the distribution of participants, and the right side shows the distribution of item difficulty. The higher an item is on the scale, the more difficult it is, and the larger the logit value, and the lower the item is, the smaller the logit value. Thus, item 14, “standing on 1 leg,” is the most challenging item, while item 3, “sitting unsupported,” is the most accessible.

Personal ability or item difficulty map.
Rating Scale Analysis
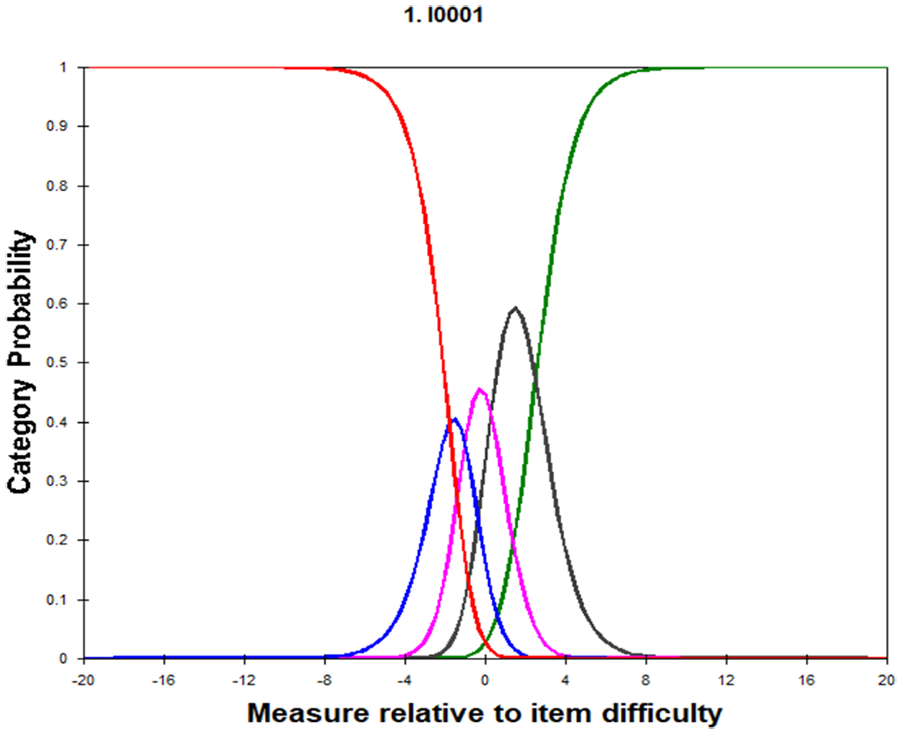
As a result of determining the appropriateness of the rating scale (0-4 points) of the Korean version of BBS, the mean autoregressive residual of the outfit index is less than or equal to 2.0, and the mean measurements are vertically ordered. However, the five-point scale was unsuitable because the step correction interval was analyzed as less than 1.0 logit (Table 2). Therefore, the scale was revised to a four-point scale by combining the 1- and 2-point scales. The results showed that using a four-point scale compared to a five-point scale distinguished responses between each scale (Tables 3 and 4; Figures 2 and 3).
Five-rating Scale Analysis.

Four-rating Scale Analysis.

Category probability curves for 5 category Likert scale.

Category probability curves for 4 category Likert scale.
Separation Reliability
The separation reliability analysis showed that the separation coefficient of the participants was 5.63, the separation reliability was 0.97, and the separation coefficient of the items was 11 (Table 5).
Separation Reliability of Person and Item.

Discussion
Maintaining balance is the basis for performing functional activities in the home and community. 48 Mobility is essential for social participation. 49 Balance ability and trunk control are essential for wheelchair propulsion and walking for patients with spinal cord injuries.11,13 However, patients with spinal cord injury have difficulty in postural control and maintaining balance due to loss of sensory and motor functions below the level of injury, 50 which can lead to limitations in daily life. 26 Therefore, improving balance ability in patients with spinal cord injury is essential for promoting community participation 51 and performing independent daily life.
The goal of rehabilitation for patients with spinal cord injury is to lead a life as independently as possible within limited activities and to return to the community. 52 Improving balance ability can be a goal of rehabilitation for patients with spinal cord injury, 53 and it is vital to use appropriate assessment tools to apply treatment goals that are tailored to individual characteristics depending on the level of injury.
Tools such as mFRT, TUG, and Romberg Test are used to evaluate the balance of patients with spinal cord injury.23 -25 The BBS has the advantage of simultaneously assessing static and dynamic balance and comprises 14 items commonly seen daily. It was developed to evaluate stroke balance ability 31 in clinical practice. It is applied to patients with various diseases. Thus, we intend to measure the balance of patients with spinal cord injury using the Korean version of BBS. This study was conducted to verify the validity of the BBS using Rasch analysis for patients with spinal cord injury.
First, the infit and outfit indices presented in the Rasch analysis were used to verify the 1-dimensional structure. As a result of analyzing the fit between the participants and items, 7 out of 80 participants (11.4%) were found unsuitable. After examining the fit between the items for 73 participants, excluding the 7 participants, the item considered unsuitable in this study was Item 7, “Standing with both feet together without holding them together.” If the mean square residual value of the item fit is high, it means that the item is not homogeneous with other items in the scale, and if the value is low, it means that the item overlaps with other items. 54 The mean square residual value of item 7 was low at −2.8, indicating that it is an inappropriate item as it assesses a similar ability to item 2, “Standing without holding on.” Therefore, it was confirmed that 13 items, except for 1 item, satisfied unidimensionality. The process of reconstruction involves deleting inappropriate items through analyzing the suitability of the assessment tool. This can reduce the time needed by decreasing the number of assessment items and enhance the construct validity. 34
As a result of analyzing the difficulty of the 13 appropriate items, item #14, “Standing on 1 leg,” had the highest with 4.86 logits, followed by item #13, “Standing with 1 foot in front of the other,” with 3.63 logits. Conversely, item #3, “Sitting with the right posture without leaning on the back of a chair,” had the lowest with −8.51 logits, followed by items #4, “Sitting from a standing posture,” and #5, “Moving from chair to chair” with −2.44 logits and −2.23 logits, respectively. As shown in Figure 1, the logit scores are converted according to the difficulty of the items and the individual’s ability and are listed on a graph, allowing for direct comparison. According to previous studies, when the distribution range of the difficulty of the items is similar enough to measure the individual’s ability range, it can be said that the distribution is appropriate. 54 In this study, the difficulty range of the items and the distribution of the participants were appropriate, but the low logit value of Item 3, “Sitting with the right posture without leaning on the back of the chair,” is the same result as the low logit value in previous studies.55,56 This item is the only item that evaluated sitting balance, and the ASIA impairment scale of the participants in this study was mainly distributed in C and D. Therefore, it is thought that this result was obtained because the participants’ balance ability was reasonable compared to the difficulty of the item, and there was no effective differentiation.
In a previous study targeting general older adults, the most challenging evaluation item was “standing on 1 leg,” and the most straightforward item was “sitting in a standing posture.” 56 In a study targeting individuals with a hemiplegic disability, the most challenging item was “standing with 1 foot in front of the other foot,” the most accessible evaluation item was “sitting with the proper posture without leaning on the back of the chair.” 22 In a study of amputation patients, the following items were found to be difficult to assess in the following order: “standing on 1 leg,” “turning 360°,” and “placing alternate foot on step of stool.” 42 This shows that even with the same assessment tool, the difficulty of the assessment items differs depending on the participant’s disability characteristics or functional level and demonstrates the need for a balanced assessment that considers the characteristics of spinal cord injury patients.
As a result of analyzing the rating scale, the outfit index of each scale was 0.96, 0.44, 1.05, 1.81, 0.94, showing values below 2.0, and the average measurement value also showed a sequential increase arrangement of −5.58, −1.48, 0.02, 1.60, and 5.56. However, the step correction interval was analyzed to be below 1.0 logit between the 1-point and 2-point scales. Thus, it was re-modified into a four-point scale that integrated the 1-point and 2-point scales. As a result, the values were utterly separated according to each rating scale score, and the intersection points between the scales were arranged sequentially, showing an appropriate response category probability curve. Unlike previous studies on older adults and hemiplegic patients, which concluded that a 5-point scale was appropriate,22,56 this study determined that a 4-point scale was more appropriate for evaluating patients with spinal cord injury using the Korean version of the BBS. Analyzing the entire scale indicated that further examination of items could enhance evaluation rationality by reducing items with excessively low difficulty to a smaller scale than the 5-point scale, and assigning higher scores to items with high difficulty that are difficult to assess. Therefore, it was determined that a four-point scale is appropriate when administering the Korean version of BBS to patients with spinal cord injury.
Finally, the separation reliability analysis results showed that the subject separation index was 5.63, the separation reliability was 0.97, the item separation index was 11.90, and the separation reliability was 0.99. The construct validity can be estimated through the separation reliability. The concurrent validity can be assessed through the reliability of the subject separation. 57 Generally, a separation reliability coefficient of 0.90 and a separation index of 3 or higher are interpreted as excellent.36,46 The item separation reliability analyzed in this study provide strong evidence supporting the high reliability and sensitivity of the assessment tool. Notably, the high levels of person separation reliability and separation index indicate that the tool can effectively distinguish between individuals with varying levels of ability, thereby enhancing its applicability in clinical settings. These findings suggest that the Korean version of BBS is highly suitable for evaluating balance ability in individuals, reinforcing its clinical utility and relevance. Therefore, when the Korean version of BBS was applied to patients with spinal cord injury in this study, the validity and reliability can be judged high.
This study verified the appropriateness of the items when applying the Korean version of the BBS to patients with spinal cord injury, presented the difficulty level of the items, and verified the validity of the evaluation tool by conducting a rating analysis of the scale. The study’s limitations include its retrospective design, which did not allow for prior sample size calculation or power analysis, and the fact that it targeted only patients with spinal cord injury in a specific region. These factors make it challenging to generalize the results to broader populations. Since the number of participants was small, data collection should be conducted on many people. Additionally, since the prognosis for functional recovery varies depending on the level of neurological damage, stage of recovery, and age of the participants, future research needs to be conducted by identifying differences in the participants’ general characteristics.
Conclusions
This study aimed to determine whether the Korean version of BBS is suitable as a balance ability assessment tool for patients with spinal cord injury by applying Rasch analysis and analyzing the validity of the participants and items, item difficulty, rating scale, and separation reliability. As a result of the Rasch analysis, 7 out of 80 participants were unfit. Item 7 of 14, “Standing with both feet together without holding them together,” was deemed unsuitable. Regarding item difficulty, Item 14, “Standing on 1 leg,” was the most difficult, and Item 3, “Sitting with the right posture without leaning on the back of a chair,” was the most accessible. As a result of the rating scale analysis, a four-point scale was found to be more suitable than a five-point scale, and the reliability of the items and participants was found to be excellent. These results show that the Korean version of BBS is a suitable tool for systematically and objectively assessing the balance ability of patients with spinal cord injury. It also offers evidence for use in clinical settings and provides intervention guidelines based on item difficulty levels. This suggests that tailoring rehabilitation interventions accordingly can improve reliability.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251338928 – Supplemental material for Validity of the Berg Balance Scale in Individuals With Spinal Cord Injury: A Rasch Analysis
Supplemental material, sj-docx-1-inq-10.1177_00469580251338928 for Validity of the Berg Balance Scale in Individuals With Spinal Cord Injury: A Rasch Analysis by Han-Som Kim, Seon-A. Kim and Jong-Sik Jang in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors would like to express their gratitude to all individuals who indirectly contributed to the completion of this study.
Ethical Considerations
Given the retrospective nature of this study, prior consent from the subjects was not required, and it was conducted with the approval of the Institutional Ethics Committee of Kangwon National University (KWNUIRB-2024-06-004-001).
Author Contributions
Han-Som Kim: Conceptualization; Formal analysis; Investigation; Methodology; Writing-original draft. Seon-A Kim: Data curation; Formal analysis; Validation; Writing-original draft. Jong-Sik Jang: Methodology; Project administration; Writing-review & editing.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the first author upon reasonable request. Access to the data is restricted due to ethical considerations and the protection of participant confidentiality.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.