
Abstract
Poverty eradication and good health and well-being are at the core of Sustainable Development Goals (SDGs) concerns. As illness greatly contributes to poverty, addressing health poverty is crucial to combat the broader issue. Global poverty reduction (PR) efforts currently face significant challenges. Remarkably, China accelerated its poverty alleviation efforts in 2015 with the implementation of the Health Poverty Alleviation Project. However, existing knowledge about China’s health PR policies is scattered across the literature, which impedes a comprehensive understanding among researchers and practitioners. This study seeks to bridge knowledge gap as input for further research by synthesizing relevant policies and literature. It reviews China’s 12 policies on health PR since 2015, analyzes the governance logic and key governance initiatives for health PR, and assesses the effectiveness of governance in this area by reviewing 27 pieces of literature. Most studies show that China’s policies to alleviate health poverty have enhanced PR. China initially established a nationwide, systematic, and coordinated health poverty governance system, which demonstrated good PR effects. These insights offer valuable lessons for the global poverty reduction agenda, such as accurate identification of the poor, systematic implementation of health PR, and sustained promotion of health PR. We hope that these efforts will help some nations or regions optimize their PR initiatives and advance the cause of eradicating poverty worldwide.
Keywords
Poverty eradication and health promotion constitute crucial components of the SDGs. Disease exacerbates poverty conditions, while poverty restricts access to essential healthcare services, ultimately forming a vicious cycle of disease-poverty. At present, the global PR cause is confronted with significant challenges, and addressing health poverty is of vital importance for the realization of the SDGs.
This narrative review systematically examines China’s health PR policies and the published literature. It comprehensively collates the major policy measures of China’s health PR, evaluates their implementation effectiveness, and focuses on discussing the experiences and deficiencies of these measures.
The research findings indicate that China’s health PR policies have achieved favorable outcomes. They have provided valuable experiences for the global health PR undertaking, such as the need for accurate identification of the poor, systematic implementation of health PR, and sustained promotion of health PR.
Introduction
Poverty poses a grave challenge to society and represents the greatest obstacle to the realization and enjoyment of human rights. Eliminating poverty is the dream of humanity. Whether through the United Nations (UN) Millennium Development Goals (MDGs) or the UN Sustainable Development Goals (SDGs), eradicating poverty has always been a primary issue of global concern. Through the years, worldwide poverty reduction (PR) efforts have achieved significant results. In 2015, the number of people living in extreme poverty worldwide fell from 1.9 billion in 1990 to 836 million, successfully achieving the MDG of reducing absolute poverty by half in 2015 compared with the 1990 level. 1 Between 2010 and 2019, the proportion of workers living in extreme poverty worldwide decreased by half, from 14.3% to 7.1%. 2 However, the rate of PR has since slowed and been exacerbated by widening global inequality, stagnant economic growth, and increasing food shortages, owing to a combination of factors such as the impact of the COVID-19 pandemic, recurrent regional conflicts, climate crises, and ecological degradation. 3 According to the SDGs Report published by the UN in 2022, 93 million people worldwide were living in extreme poverty in 2020, with the number of people living in poverty rising rather than falling. 4 Rural poverty was even more severe, with 80% of the planet’s poor living in rural areas, 5 and populations in developing countries suffering to a large extent.
The poverty–health nexus has become a key focus of current policy formulation, and health has been recognized as central to PR and socio-economic development. 6 Health is a fundamental human right, a prerequisite for the existence and effectiveness of human capital (HC), and a basic guarantee for the sound functioning of the family and social economy. Health problems place a heavy burden on individuals and families in terms of poverty.7,8 Health risks directly affect household finances by generating unanticipated costs. 9 When health risks persist, household medical expenses increase, incomes decline, and savings are depleted—even to the point of the afflicted borrowing or selling property to cope, which leads to catastrophic health expenditures. 10 In addition, health risks have an indirect impact on household income through their effect on individual and household behavior and the amount of time spent working.11,12 Health risk shocks may not only lead to incapacitation, loss of time spent working, and reduced household income but may also crowd out household investment in production, lower investment in the HC of children, undermine households’ income-generating capacity, and catapult households into chronic poverty.13,14 Families become vulnerable to a vicious circle of “poverty and illness” when they are chronically affected by reduced income and increased costs due to health shocks. 15
The improvement of health status can reduce medical expenditures and effectively increase individual productivity and hours spent working, which in turn may increase income to prevent poverty. 16 Economic growth reinforces the health of the population and the accumulation of HC. 17 Therefore, the prevention of poverty due to disease is an important task in promoting sustainable PR. Accordingly, substantial health PR efforts have been made worldwide, especially in developing countries, such as the free healthcare policy for the poor in Uganda, 18 health card program in Indonesia, 19 conditional transfer program for the poor in Georgia, 20 and Rashtriya Swasthya Bima Yojana healthcare program in India, 21 dedicated to the governance of health poverty. Similarly, China implemented a special project to combat health poverty—the Health Poverty Alleviation Project (HPAP)—in 2015. In February 2021, China announced that it had completed the task of eradicating absolute poverty and achieved the PR goals of the UN 2030 Agenda for Sustainable Development, 10 years ahead of schedule. 22 Nevertheless, health is a long-term concern, and the phenomenon of “poverty caused (returned) by illness” still requires attention. Therefore, summarizing China’s health PR policies and implementation effects is important to consolidate the achievements of health poverty alleviation efforts. Furthermore, at a time when global PR is facing major challenges, it is crucial for the development of global PR to analyze China’s health PR policies and implementation effects. Hence, this narrative review explored the following questions: What specific health policies have been implemented in China to reduce poverty since 2015? How effective have these policies been? By answering these questions, we endeavor to provide valuable insights for PR in developing countries in an effort to contribute to global PR.
Methods
As a narrative review, this study primarily synthesized policy experiences and the implementation effectiveness of health PR in China through a review of the relevant policies and literature.
Definition of Health Poverty
Prior to the literature search, we first defined health poverty for conducting research. Health poverty stems from multidimensional poverty for which no unified concept exists, and scholars mostly conceptualize it based on the loss of opportunity, capability deprivation, and risk shocks.23 -27 Generalizing previous studies, we conclude that health poverty refers to individuals or family members who gradually lose the ability to withstand risky shocks while defending against health risks. This phenomenon leads to low health levels, increased expenditure, decreased income and savings, insufficient investments in human resources, deprivation of the ability to generate income, and eventually, a state of poverty. Health poverty not only increases the economic burden but also results in reduced individual viability, a lack of family HC, insufficient incentives for long-term development, and ultimately, a vicious cycle of disease–poverty chains (Figure 1).

The cycle of disease-poverty.
Search Strategy
An online search of the related policy documents and academic literature was conducted, covering the period 2015 to 2023. Policy documents containing the search terms (“poverty” OR “health poverty”) AND (“against” OR “alleviation” OR “solve” OR “prevent”) were searched on the official websites of the Chinese government, National Health Commission, and National Health Insurance Bureau. Academic literature was searched on China National Knowledge Infrastructure and PubMed. Boolean phrases such as “OR” and “AND” were used with the following keywords: “poverty,” “poor,” “financial burden,” “financial vulnerability,” “catastrophic health expenditure,” “health,” “healthcare,” “medical,” “illness,” “diseases,” “health insurance,” “health assistance,” “health resources,” “health fiscal expenditures,” “health policies,” “medical security,” “medical insurance,” “medical assistance,” “medical resources,” “medical fiscal expenditures,” and “health investment.” The titles and abstracts were screened.
Eligibility Criteria
To be included in the literature review, policy documents must be officially published and related to health PR. Specifically for academic literature, studies whose (1) target area is China or somewhere within China and whose (2) study data include post-2015 data were selected. Thirty-nine documents comprising 12 government policies and 27 academic articles were included for analysis and result synthesis.
Results
Policies for Reducing Health Poverty in China
China has long committed to lowering poverty. In 2015, the central government issued the “Decision on Winning the Battle Against Poverty,” 28 which instigated a decisive mode of poverty eradication in China and proposed for the first time the implementation of the HPAP. The HPAP takes health poverty governance as an important element of the overall eradication of poverty and emphasizes that impoverished populations must enjoy basic medical and healthcare services and obtain medical security and medical assistance to fight poverty and prevent poverty arising from illnesses. Within this framework, the central government published in 2016 a special document providing guidance on the governance of health poverty. This document additionally offers opinions on the implementation of projects to alleviate health poverty and clarifies the key tasks of the HPAP to guide efforts to lower health poverty. 29 Subsequently, the central government promulgated a series of health policies that comprehensively promote the development of health PR, including the “Three ‘A Batch’ Action Plan for Health Poverty Alleviation Project,” 30 “Three-Year Action Plan for Health Poverty Alleviation,” 31 “Three-Year Action Plan for Medical Security Poverty Alleviation,” 32 “Implementation Opinions on Consolidating and Expanding the Achievements of Health Poverty Alleviation and Effectively Linking It with Rural Revitalization,” 33 and “Implementation Opinions on Consolidating and Expanding the Achievements of Poverty Alleviation through Medical Security and Effective Linking with the Rural Revitalization Strategy.” 34 Table 1 lists the main health poverty-alleviation policy documents released by the central government since 2015 along with their main content. Sorting through these policies, we found that China’s health PR policies cover three broad areas: (1) accurately identifying an impoverished population, (2) improving the level of medical security for an impoverished population, and (3) optimizing the allocation of health resources and improving the medical capacity and public health services (PHS) in poverty-stricken areas.
China’s Main Policies to Alleviate Health Poverty Since 2015.

Accurately Identifying Impoverished Populations
The central government proposed establishing an accurate working mechanism to mitigate poverty, which requires accurately identifying impoverished populations, coordinating projects, using funds, measuring households, assigning people to villages, and achieving poverty eradication. Impoverished households are identified through farmer applications, democratic evaluations, public announcements, and step-by-step reviews under government guidance at the township level. The entire process is publicly supervised to ensure fairness and justice. Consequently, 98.99 million poor people in China were identified, and electronic information files on the poor were established nationwide. 35 The policy lays the foundation for realizing precise health support for poor people through a refined management of the poor population and precise allocation of resources to alleviate poverty. 36
Improving the Level of Medical Security
China’s programmatic document on health poverty alleviation—”Guiding Opinions on the Implementation of Health Poverty Alleviation Projects”—proposes raising the level of medical security and reducing the burden of medical expenses on the rural poor by raising the reimbursement rate for hospitalization costs, lowering the starting point for major illness insurance, raising the rate of reimbursement for major illness insurance, and increasing the level of medical assistance. Simultaneously, it proposes setting up a mechanism for linking basic medical insurance, major illness insurance, and medical assistance systems to bring synergy and complementarities into play and create a synergy of protection. The policies include the “Implementation Plan for the Three-Year Action on Poverty Alleviation through Medical Security (2018-2020),” “Work Plan for Solving the Outstanding Problems of Providing Basic Medical Security for the Poor,” “Guiding Opinions on Resolutely Completing the Hard Tasks of Poverty Alleviation through Medical Security,” “Notice on Winning the Battle of Poverty Alleviation through Medical Security of High Quality,” “Implementation Opinions on Consolidating and Expanding the Achievements of Poverty Alleviation through Medical Security and Effective Linking with the Rural Revitalization Strategy.”
The aforementioned policies concretely detail relevant objectives and measures, summarized as follows: (1) Achieve 100% coverage of the rural poor using basic medical insurance, major disease insurance, and medical assistance; (2) Fully implement the basic medical insurance treatment policy and raise the overall level of medical security to gradually fill the gap between urban and rural areas; (3) Increase the tilt of major disease insurance by lowering its starting point for the rural poor by 50%, increasing the payment ratio by 5 percentage points, and gradually raising and abolishing the payment ceiling; and (4) Improve the ability of medical assistance to provide basic support and ensure that the annual medical assistance for rural impoverished populations covers no less than 70% of their out-of-pocket hospitalization expenses within the policy-defined scope, under the annual assistance limit. Meanwhile, the tilt assistance for special difficulties has been further increased.
Optimizing the Allocation of Health Resources
The “Guiding Opinions on the Implementation of the Health Poverty Alleviation Project” states that in impoverished areas, it is necessary to strengthen the construction of medical and healthcare service systems, standardize county-level hospitals, township health centers, and village health offices, accelerate the improvement of the network of PHS, and intensify support for building the capacity of professional public health institutions in terms of disease prevention and control (P&C) as well as maternity and child healthcare. Since then, a series of policies—such as the “Three ‘A Batch’ Action Plan for Health Poverty Alleviation Project,” “Three-Year Action Plan for Alleviating Health Poverty,” and “Implementation Opinions on Consolidating and Expanding the Achievements of Health Poverty Alleviation and Effective Linking with Rural Revitalization” has been issued to further clarify the relevant objectives and measures. These are summarized in the following areas.
(1) Increase government healthcare spending (GHS). To this end, central financial authorities maximize the transfer of funds and planning and construction projects for healthcare in poor areas.
(2) Strengthen the construction of the medical and health service systems in poverty-stricken areas and comprehensively improve facility conditions: This plan encompasses one county-level public hospital (including a traditional Chinese medicine hospital) in each poverty-stricken county, one government-run health center in each township, and one health center room in each administrative village. In keeping with this plan, each specialized department of every county hospital will have at least one qualified practicing physician; in each township health center, at least one qualified practicing (assistant) physician or general practitioner; and in each village health center, at least one qualified rural doctor or practicing (assistant) physician.
(3) Compensate for the shortcomings of the public health service system. This is done by strengthening the construction of disease P&C institutions, enhancing the infrastructure conditions of disease control institutions, strengthening the staffing of primary medical and healthcare institutions with child healthcare practitioners, implementing effective management of contracted services for chronic diseases, reinforcing the construction of maternal and child healthcare institutions at the county level, and carrying out actions to promote maternal and child health in impoverished areas.
Effectiveness of China’s Policies to Reduce Health Poverty
Since the HPAP was implemented in 2015, numerous scholars have conducted evaluation studies on such policies. Based on the chief policy categories of the HPAP, we present an overview of the relevant studies from two perspectives: (1) medical security and (2) health resource allocation (RA; see Table 2 for the specific research situation of the relevant scholars).
Specific Studies on the Effectiveness of Chinese Health PR Policies by Relevant Scholars.

Medical Security and PR
Basic Medical Insurance and PR
Scholars have explored the PR effects of basic health insurance in terms of income poverty, relative poverty, poverty vulnerability, and poverty risk resilience. In terms of income poverty, the targeted medical insurance showed a significant income-enhancing and poverty-reducing effect, particularly expanding the proportion of subsidized premiums and the share of reimbursement for hospitalization with a largely significant positive effect. 37 As for relative poverty, the rural medical insurance system significantly and robustly reduced the probability of rural residents falling into relative poverty. 38 Regarding vulnerability to poverty, participation in a new rural cooperative medical insurance and basic medical insurance for urban and rural residents, access to basic medical reimbursement, and higher levels of reimbursement significantly reduced residents’ vulnerability to poverty, with a greater effect on absolute poverty.39 -41 Regarding the ability to resist poverty risk, urban and rural residents’ health insurance significantly enhanced the health level of individuals and their ability to resist such risk. This insurance could play a significant role in alleviating poverty due to illness for the migrant population and for families who are exposed to the risk of major illness. 42
Major Illness Insurance and PR
As a supplement to basic medical insurance, the objective of major medical insurance is to further lower catastrophic medical costs grounded in basic medical insurance and to provide secondary compensation for the medical services needed by families that have already incurred catastrophic medical expenditures. 43 This has reduced the impact of health risk shocks on a family’s financial situation and ultimately mitigated the effects of poverty caused by illness. On the one hand, major illness insurance significantly lowered the probability of absolute poverty by directly lowering families’ economic burden through reduced medical expenses. On the other hand, by increasing the labor force participation of families, the impact on economic income was avoided due to the shock of major illnesses that lead to a patient’s complete inability to work. 44
Medical Assistance and PR
Medical assistance is an important part of the medical security system, 45 a special social assistance system implemented by the government to respond to and solve the basic medical problems of the poor, and helping the poor is the first principle of medical assistance. 46 Medical assistance, as the last safety net in the medical security system, is becoming increasingly crucial in alleviating the burden of disease on poor families. 47 Medical assistance effectively reduces poverty by directly minimizing the financial burden of medical care on the poor. Several studies have shown that medical assistance can significantly reduce the medical expenses of disadvantaged groups, especially catastrophic health expenditures, effectively alleviate the burden of medical costs on impoverished individuals, and reduce the incidence of poverty.48,49
While most studies on medical security and PR present positive outcomes, some show that medical security has a limited effect on PR and even exacerbates poverty. They propose that the implementation of major medical insurance policies can improve regional poverty, but core variables such as actual reimbursement ratios do not significantly mitigate regional poverty. 50 Medical insurance, especially urban and rural residents’ medical insurance, does not improve the health equity of rural residents. Instead, it may widen the degree of health inequality between urban and rural areas, and, based on the “pro-poor” nature of health inequality and the severity of aging, it may lead to a “health inequality–health poverty” trap. 51
Health RA and PR
GHS and PR
Numerous studies have evaluated the poverty-reducing effects of GHS, and some studies have shown that GHS has a significant PR effect. GHS can improve the health of household members, increase the supply of labor for households, expand the proportion of household employment, help households lower their healthcare costs, increase household wage income, and alleviate household poverty by influencing the supply of and demand for healthcare services. It can not only reduce the incidence and depth of health poverty but also reduce the vulnerability of households to poverty and increase their ability to withstand health risks.52 -54
Medical RA and PR
Medical RA is the basis for people’s enjoyment of healthcare services and may impact poverty through fairness, and fair medical RA can effectively reduce poverty due to healthcare expenditures.55,56 Graded diagnosis and treatment are beneficial for improving the efficiency of medical RA in underdeveloped areas, as this mitigates the shortage of medical services and provides a productive pathway for alleviating health poverty. 57 The number of resources such as primary medical institutions, medical technicians, and primary beds available for patients have a significant positive effect on reducing health poverty.55,56 The equalizing medical services have a significant effect on PR, especially on alleviating the relative poverty of rural migrant workers, and have spatial spillovers. 58 Medical RA impacts poverty by releasing the health needs of the population. The higher the medical PR in a neighboring area, the lower the incidence of poverty in that area. 59
Public Health RA and PR
PHS enhance the living environment of urban and rural residents, effectively carry out disease P&C, help reduce residents’ direct spending on healthcare, and lower the indirect costs of transportation, accommodations, and unemployment due to seeking medical advice. 60 Simultaneously, PHS increase residents’ health capital, promote the accumulation of healthy HC, improve individual survivability, and thereby increase the labor income and mitigate the relative poverty of rural households.61,62 Zhou et al 63 found that improvements in PHS had the greatest impact on mitigating multidimensional poverty for migrant workers in Western China, the younger generation, and female migrant workers.
Discussion
China has long emphasized the governance of health poverty and in 2015 began to implement the HPAP, systematically and sustainably advancing PR by accurately identifying the poor, raising the level of medical security, and strengthening the allocation of medical and healthcare resources, as discussed below.
(1) Accurate identification of the poor: Accurately identifying people living in poverty to implement targeted support initiatives that help them escape extreme poverty is a major challenge faced by the international community. World Bank researchers confirmed that while pro-poor programs are an important policy tool for eradicating poverty, the selection of appropriate beneficiaries faces significant challenges. 64 Alatas et al 65 found that the chief reason for this difficulty is that poor people are concentrated in rural areas where the income of the rural population comes primarily from agriculture and the informal employment sector. This makes it difficult to target the poor using a methodology based on household income accounting, which in turn makes it difficult to effectively use funds for alleviating poverty. In addition, community elites are easily siphoning poverty alleviation funds; as such, the poor are not the ultimate beneficiaries. 64 The Chinese government has done much work to accurately identify the poor and the beneficiaries of its policies through top-down policy guidance from the government to residents, and bottom-up application evaluations from residents to the government, ultimately determining who is impoverished and establishing a database to keep track of them. This process ensures accurate information, comprehensive coverage, and fairness, with the intent that all local people recognize the final beneficiaries. Simultaneously, the database vertically connects various levels of organizations and governments such as families, administrative villages, townships, counties, cities, provinces, and countries, and horizontally covers numerous government departments, educational institutions, healthcare, banks, and other organizations to achieve a smooth flow of information and dismantle information barriers. In addition, the database is dynamically updated annually according to the current situation, which significantly improves the accuracy of identifying the beneficiaries.
(2) Improved medical security: Medical security is a key policy tool for lowering poverty; it protects people from financial hardship due to illness and works in two main ways. First, medical security directly reduces individual out-of-pocket health costs, eases the financial burden of healthcare, 66 and improves access to healthcare. Second, it indirectly improves health 67 and increases the labor supply68,69 or reduces the healthcare burden and promotes non-medical consumption expenditures (eg, education and training expenses). 70 This in turn increases income and lowers poverty. 71 Driven by the HPAP, China’s medical security system has further improved, with the level of medical security for the population, especially the poor, significantly raised, and the effectiveness of reducing poverty significantly enhanced. 72 By the end of 2019, the policy for alleviating poverty through medical insurance had benefited 200 million poor person-times and helped 4.18 million people—who were poor due to illness—escape poverty. 73
(3) Optimized allocation of health resources: The health resources enjoyed by populations in relatively impoverished areas are insufficient, resulting in medical and health service needs not being fully met. 74 As a vital part of social resources, the allocation and usage efficiency of health resources among regions and populations affect the extent to which people are deprived of social resources. According to Amartya Sen’s feasible ability theory and Townsend’s social deprivation theory, addressing health poverty requires paying attention to the allocation and usage efficiency of health resources. GHS, as a means of social redistribution, is used to ensure that urban and rural residents have access to the most basic and effective medical care and PHS. Since the implementation of the HPAP, China has promoted progress in health PR by strengthening investments in the capacity to supply health services to solve the problem of difficult access to healthcare, and by increasing investments in the demand side to address the issue of expensive access to healthcare. Optimizing the allocation of rural medical resources is an important aspect of the HPAP. Following the implementation of the HPAP, the allocation of medical resources in China’s rural regions has greatly improved. As of October 2020, each of the nation’s 832 impoverished counties had at least one county-level public hospital, and each township and administrative village had a health center and village clinic, respectively, staffed by qualified doctors. 75 Optimizing the allocation of rural medical resources lies primarily in meeting the medical and healthcare service needs of rural residents by narrowing the inequality between urban and rural medical resources and promoting the sinking of high-quality medical resources, thereby resolving the problem of difficult, expensive access to medical care and advancing health and PR. In addition, China’s approach to PR by optimizing the allocation of public health resources involves reinforcing health promotion and education, improving health-record and chronic-disease management, and comprehensively preventing and controlling key infectious and endemic diseases so as to improve the health literacy and health level of rural residents, in addition to preventing poverty caused by illness.
(4) Systematic implementation of health PR: The HPAP covers almost all aspects of healthcare and not just reinforces one aspect or implements assistance. While improving basic medical insurance, it has bolstered major disease insurance and medical assistance. While strengthening medical RA and upgrading the capacity of medical services, the HPAP has also increased the allocation of public health resources and upgraded its capacity for health promotion as well as disease P&C. In addition to improving medical security, the HPAP has enhanced the allocation of health resources and synergies with other areas.
(5) Sustained promotion of health PR: Although China announced in February 2021 that it had fully eradicated poverty in 2020, the policies of the HPAP did not end but continue to be implemented as an important element of the rural revitalization strategy. Since 2020, relevant policies have not weakened but instead, reinforced some aspects of the HPAP. For example, in the area of medical assistance, efforts to provide assistance to the poor have been further strengthened by abolishing the deductible for residents who are entitled to basic living allowances and groups that are most vulnerable, and by implementing the dynamic management of information on medical assistance recipients so that those who meet the conditions are promptly included in the scope of the assistance. In the area of major illness insurance, in 2021, China further improved medical security for the poor for major diseases, reduced the starting standard for major disease insurance by 50% for those who are poor due to illness, increased the percentage of payment by 5 percentage points, and eliminated the maximum payment limit.
In summary, the governance of health poverty in China is a targeted effort to deal with the mechanism of health poverty, as illustrated in Figure 2, which shows the logic of governance.
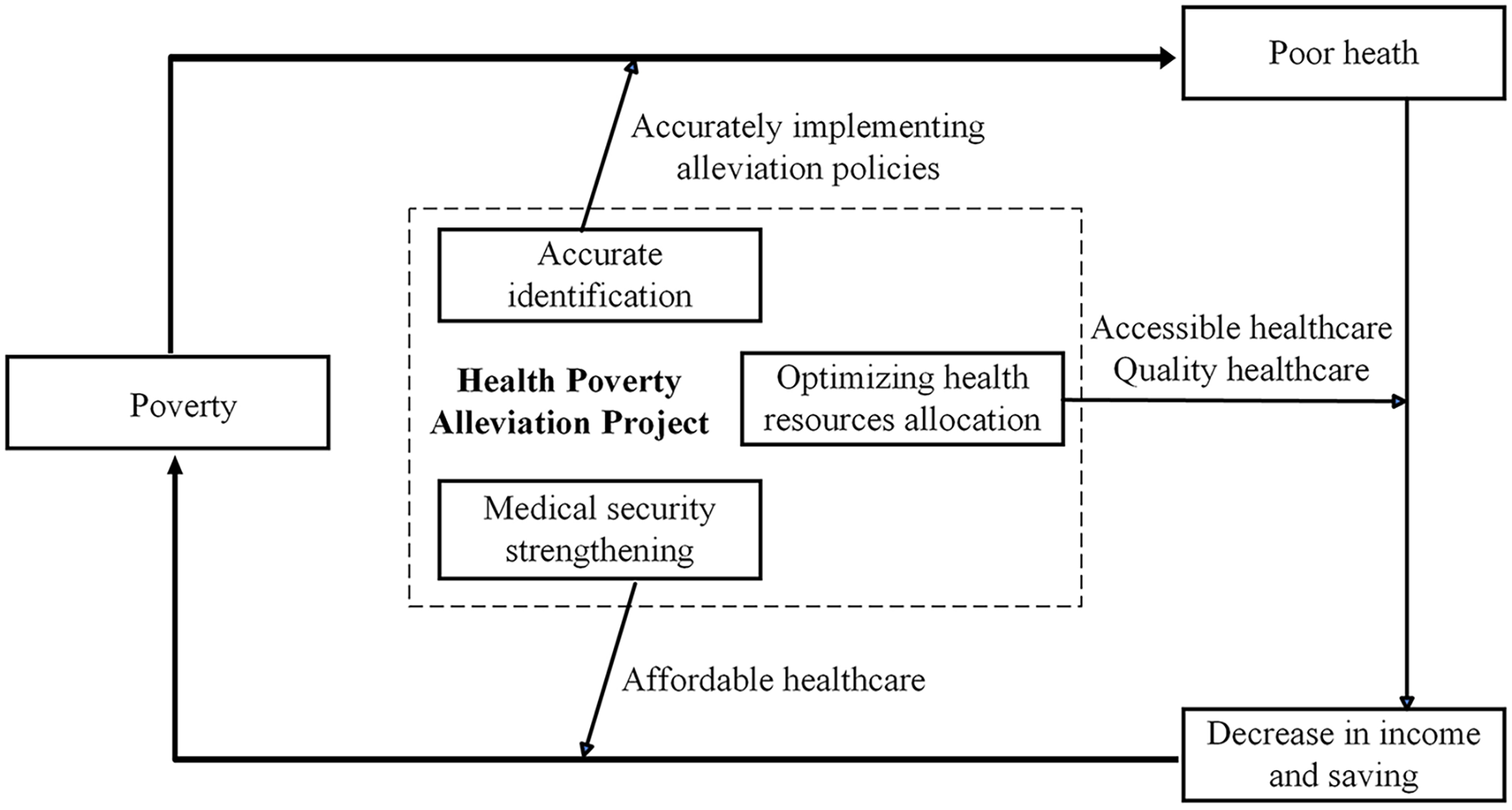
The logic of health poverty governance in China.
Many scholars have conducted empirical studies from multiple angles to evaluate the effectiveness of health PR in China, using different data and various methods. Most studies have found better PR effects in both medical security and health RA, while a few present less-positive outcomes. Here, we focus on three points discussed below.
(1) Although policies to alleviate health poverty have had a positive effect on PR, this does not mean that they do not have shortcomings. For example, in promoting urban–rural health equality in China, challenges arise such as the uneven distribution of medical resources, coupled with the restrictions set by medical insurance (eg, the deductible, limit line, and reimbursement ratio), which may lead high-income earners to obtain more and better-quality medical services owing to their ability to pay, and thus exacerbate health inequality. 76 Rural residents are mostly engaged in manual labor, which is highly dependent on health, and with the reality of aging, which is particularly prominent in rural areas, 77 health inequality is more likely to cause rural residents to fall into a vicious cycle of the health poverty trap. Therefore, the health inequality–poverty trap brought about by medical insurance policies must be highlighted and the necessary steps must be taken to deal with it.
(2) Although the Chinese government has implemented a series of health policies to mitigate poverty, which has improved access to medical and healthcare services for residents in impoverished rural areas, some effectiveness remains unremarkable. For instance, although the nationwide coverage of contracted family doctors exceeded 85% in 2017, the implementation outcomes of the family doctor system were not promising. 78 There is an artificially inflated rate of contracting family doctors across different regions, with low awareness and usage rates among residents regarding these services. 79 This is also why it is difficult for residents in poor areas to obtain normalized protection. Hence, it is necessary to pay close attention to similar policies, to carry out timely evaluations of policy effects, and to make the necessary adjustments and optimization to successfully promote health and mitigate poverty.
(3) Review limitations: First, as a product of Chinese society and national conditions, these policies might not be suitable for all countries and regions and thus, must be optimized based on local realities. Second, regarding the evaluation of policy effects, we only assessed two aspects: (1) medical security and (2) health RA. The perspective and dimension of the evaluation may be incomplete; for example, we did not examine the mitigation of poverty through nutrition and through health education. As such, our conclusions may be more representative if the coverage could be expanded in future studies.
Conclusion
This review is the first to summarize and evaluate China’s health PR policies and effectiveness since 2015. On the whole, most studies show that China’s policies to alleviate health poverty have promoted the development of PR. China has initially established a nationwide, systematic, and coordinated health poverty governance system that has demonstrated good PR effects. The study findings offer valuable lessons for the global PR agenda, such as the need for accurate identification of the poor, systematic implementation of health PR, and sustained promotion of health PR. In future studies, these health PR policies should be continuously promoted and appropriately updated and adjusted according to the circumstances surrounding poverty to advance the sustainable development of health PR and contribute further to global PR.
Footnotes
Acknowledgements
We would like to thank all the employees who participated in the study.
Author Contributions
Concept and design: JL, TZ, XW, JP; Data acquisition and analysis: JL, TZ, ZL, LC; Interpretation of data: JL, TZ; Drafting of the manuscript: JL, TZ; Critical revision of the manuscript: JL, TZ, XW, JP. All authors gave final approval and agreed to be accountable for all aspects of the work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by National Health Commission Healthy China initiative Project (Grant No. JKZGJBGG2317).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data availability is not applicable to this article as no new data were created or analyzed in this study.