
Abstract
Emergency department (ED) overcrowding and prolonged length of stay (LOS) remain critical issues in healthcare systems. This study compared 4 bed allocation strategies to optimize patient flow and resource utilization in a regional teaching hospital in Taiwan. A discrete-event simulation model was developed using 1 year hospital data from January 2022, including 29 718 ED visits. The following strategies were evaluated: (1) intra-departmental bed sharing, (2) optimized bed allocation, (3) cross-departmental bed lending with 5% capacity, and (4) combined optimization with bed borrowing. The model was validated by t-tests comparing the simulation outputs with actual hospital data. Results: All strategies demonstrated improvement compared to current operations. Of these, Strategy 4, combined optimization with bed borrowing, was the most promising: it maintained stable ED nursing utilization at 45.65% with a 95% confidence interval (CI) of 45.60% to 45.71% while reducing the cases of extended LOS. The rates of ED LOS exceeding 6, 12, and 24 h were 2.48%, 0.38%, and 0.12%, respectively, which is a significant improvement compared with the baseline. Optimization alone contributed to a 20% improvement in extended LOS under Strategy 2, while additional bed-sharing policies further improved performance by 10%. Conclusions: Strategic bed allocation combined with controlled bed-sharing policies achieved a 30% reduction in extended ED LOS without increasing nursing workload. The optimal strategy (Strategy 4) reduced cases of ED LOS exceeding 6 h to 2.48% while maintaining stable nursing utilization at 45.65%, demonstrating the effectiveness of combining optimization with resource sharing in ED patient flow management.
Introduction
Statistics from the Taiwan Ministry of Health and Welfare in 2024 reveal that emergency department (ED) visits have increased by approximately 78% since 2004 even after excluding the effects of the COVID-19 pandemic. 1 This surge combined with the rising elderly population is placing a significant burden on emergency departments’ workload. When hospitals are unable to provide sufficient resources or services to patients, this causes emergency department overcrowding. Previous literature indicates that frequent users of emergency services account for approximately 4% to 8% of ED patients and 18% to 28% of ED visits.2,3 Patients who do not require urgent medical attention may lead to suboptimal utilization of emergency medical resources. During their ED stay, patients undergo examinations and other procedures (such as X-rays, Magnetic Resonance Imaging (MRI), and ultrasound) following consultation with various specialists. The varying time and workload for these procedures create bottlenecks.4,5 After examination, patients are transferred to observation areas to wait for discharge or hospitalization. When inpatient beds are unavailable, patients requiring hospitalization must stay in the observation area, a situation referred to as “access block.” This directly affects the observation duration and ED length of stay (LOS).
The competition for assigning inpatient beds to different medical services is complex. Five common categories of patients compete for inpatient beds include: emergency surgery, patients requiring invasive examination, outpatient arrangement for hospitalization examination or regular treatment, intensive care unit (ICU) transfer to general ward, and emergency hospitalization. 6 The ED LOS for emergency patients in hospitals is influenced by various factors including non-emergency surgical patients, emergency admissions, and hospital bed occupancy rates.7,8 Consequently, the allocation of inpatient beds and associated medical resources in hospitals is intricately linked to the timely admission of emergency patients for hospitalization.9,10
In hospital practice, inpatient beds are allocated to different clinical units. Some smaller units may be assigned fewer beds and larger units may have more resources. Such allocation may result in a lack of organizational flexibility. However, flexibility in bed utilization is a key concept for efficient bed management. Bekker et al 11 explored the issue of flexibility in hospital bed allocation and proposed a strategy to strike a balance between efficiency and professionalism. Their study compared 4 inpatient bed allocation strategies including dedicated beds, sharing beds, hybrid policy, and threshold policy. Xue et al 12 developed optimization models and used computer simulations to determine the optimal bed allocation for different types of patients in an ophthalmology hospital, resulting in recommended bed allocation percentages of 15% for trauma, 16% for cataract in 1 eye, 28% for cataract in both eyes, 11% for glaucoma, and 29% for retina patients. Zhou et al 13 proposed a 2-stage model for public hospital inpatient room allocation and patient scheduling. Their results show that the proposed models and solution approaches effectively balance expected net revenue, average acceptance ratio, average waiting time, and probability of being served within target waiting times.
However, when discussing the allocation of inpatient beds, corresponding supporting measures are necessary. Previous literature has not comprehensively discussed the impact of bed allocation on emergency department congestion. In addition, although many studies have focused on the simulation and optimization of bed allocation,14,15 none have explored whether different bed allocation strategies affect ED LOS during resource conflicts. Therefore, this study bridges these gaps by investigating the consequences of different bed allocation strategies on LOS in emergency departments. The primary goals are to ensure prompt admission of emergency patients and decrease emergency patient waiting times, while maintaining efficient bed allocation across hospital departments.
Materials and Methods
Current Status
The research was conducted at a 946-bed reginal teaching hospital. It is in a rural section of central Taiwan. This hospital aids around 500 000 residents. Taiwan’s Ministry of Health and Welfare lists it as 1 of 46 advanced emergency responsibility hospitals. As a regional teaching hospital, it shows the characteristics of average healthcare providers with moderate dimensions within rural Taiwan. Its bed count and number of services match regional hospitals, which usually offer approximately 800 to 1200 beds. Each year, the hospital’s emergency section manages nearly 30 000 patient encounters. This number matches that of similar regional Taiwanese hospitals in Taiwan. Hospital administrative data were collected from emergency and inpatient departments from Jan 2022 to December 2022. The total number of emergency visits was 29 718. After excluding patients with out-of-hospital cardiac arrest (OHCA), in-hospital cardiac arrest (IHCA), do-not-resuscitate orders (DNR), family requests, and voluntary departures, the analysis focused on the remaining cases, with statistics are presented in Table 1. These exclusions were necessary because the information on these cases was missing and incomplete in the system, which may represent unusual patient flows that would skew the analysis of normal ED operations. Specifically, cardiac arrest cases often bypass standard triage processes and follow specialized resuscitation protocols, while patients with DNR orders or those who left voluntarily represent incomplete ED journeys that would affect length-of-stay calculations.
ED LOS Statistics by Patient Disposition Types in 2022.

Note. Clinic: Patients discharged for outpatient follow-up. Transfer: Patients transferred to other healthcare facilities. Other: Including patients who left against medical advice, expired, or had other dispositions.
OR = operating room.
Among the patients who required admission to the hospital after their visit to the emergency department, 3.14% had a stay in the emergency department for more than 6 h. The ED reported no instances of patients who stayed longer than 48 h. The percentage of patients with a 24-h LOS was 0.03%, with approximately half of these cases requiring transfer to a general ward. According to the National Health Insurance Emergency Quality Improvement Program, 17% of patients sent to emergency responsibility hospitals were not admitted within 6 h. 16 Although the hospital’s 3.14% rate of ED stays exceeding 6 h for hospitalization is relatively low compared to other hospitals, reducing ED overcrowding remains crucial for improving healthcare quality, patient satisfaction, and reducing healthcare workers’ stress levels.
Model Construction
This retrospective study used a system simulation to model the current conditions of the facility to explore how inpatient bed allocation strategies affect ED LOS. The simulation model was developed using Simul8 software, a discrete-event simulation platform that is widely used in the healthcare environment. This software has been adopted in numerous studies to examine hospital resource allocation and patient flow optimization.17 -19 These studies demonstrated its reliability in accurately representing complex healthcare systems and predicting the impact of operational changes. Using emergency and inpatient data from January 2022 to December 2022, we performed a t-test to validate the model and ensure its alignment with real-world conditions. After validation, the bed allocation strategies were explored. The simulation results of these strategies are obtained, followed by a discussion of the outcomes.
There are some core elements in system simulation: resources are the entities that provide services and include doctors, nurses, equipment, and beds. Events are activities that occur at a time point, including the arrival of patients, the start of treatment, and the end of treatment. Entities are objects that move within the system. In this study, they represented all patients. Queues are places in which entities wait for resources. They represent waiting for patients to receive treatment or wait for beds. The model also needs to set parameters, such as patient arrival times and treatment times. These elements were used to construct a model for this study. The simulation period was set to 1 year with a warm-up period of 1 month to achieve steady-state conditions. We conducted 30 replications to ensure statistical reliability. This approach follows standard practice in healthcare simulation studies where system stability rather than parameter estimation is the primary concern. 20 The confidence intervals reported in our results represent the variability across these simulation runs, each using different random number seeds but identical structural parameters. To clarify the model structure, Figure 1 presents a visual flow diagram of patient pathways and decision points in the simulation.

Patient flow in the simulation model.
Regarding staffing parameters, there were 7 nurses in the ED. The workload related to direct and indirect care encompasses approximately 40% to 50% of the total tasks executed during work. The model does not address cost or productivity. Therefore, nursing utilization rate was defined as the proportion of total working time spent on direct and indirect patient care activities.
The model follows a standard ED process flow. During the operation process, all patients entering the ED receive triaging. The patients were categorized by medical staff based on their disease severity into 2 categories: high-risk critical cases and general emergencies, categorized as Level 1 to 2 and Level 3 to 5. Regardless of the category, the medical team first makes a diagnosis to see whether emergency surgery is required; if necessary, the patient will be directly taken to the operation theater, and if not, the high-risk critical patients will be examined in general, whereas the general emergency patients will be referred for treatment to the relevant specialty. Non-surgical patients will then undergo basic examinations, laboratory tests, and imaging studies, such as X-rays and MRI; related tests will be repeated if necessary. The patient shall be sent for various examinations as ordered by the physicians until such time after all the concerned examinations are realized, when the assessment of the needs of intensive care in the General Observation Area is referred either to the pediatric observation area or the specialty areas concerned with the condition. Finally, it will be a proper time for the actual process discharge to occur because it is with respect to an orderly condition. This interconnected process ensures that patients receive the most appropriate treatment based on their urgency and medical needs while also maintaining the efficient operation of the emergency department. After constructing the framework of the emergency department and its processes using Simul8, the actual patient visit data and treatment times for each station from 2022 were imported into the model. The detailed parameter setting is shown in Appendix.
Model Validation
As shown in Table 2, a one-sample t-test was used to validate whether the rate of ED LOS in the simulation model differed significantly from the actual conditions. The actual rates of ED LOS in 2022 for ED patients with LOS exceeding 6, 12, and 24 h were 2.80%, 0.42%, and 0.03%, respectively. The corresponding rates in the model for ED patients with LOS exceeding 6, 12, and 24 h were 2.62%, 0.47%, and 0.18%, respectively. The test results showed no significant differences, thus confirming that the system simulation model used in this study accurately reflected the actual conditions of the field.
Model t-Test.

S.E. = standard deviation.
Strategy Design
The simulation for average bed usage for each department utilizing inpatient data from the year 2022 was realized in a general hospital setting; for example, gastroenterology uses 33 beds. Unlimited bed use was also simulated for all of these departments in cases where unlimited bed resources could be allocated; this may become gastroenterology using a maximum of 58 beds (Table 3). We then investigated bed allocation strategies to reduce LOS in the emergency department.
Department’ Bed Allocation & Simulation Result.

Note. Unit: Beds.
MG = gastroenterology; MN = neurology; Mn = nephrology; MP = pulmonology; SL = thoracic surgery; SS = general surgery; SC = cardiac surgery.
The bed management in the simulation system consisted of 4 allocation strategies. The first strategy is that intra-departmental bed-sharing systems were set up separately for the Internal Medicine divisions and surgical divisions. In Strategy 1, there was no bed reallocation among departments. Instead, when a specialty reaches its bed allocation limit, patients are admitted to other departments within the same division. The second strategy is to reconfigure the number of beds in the respective departments using an optimization algorithm. The third strategy is a departmental bed-lending policy, where 5% of beds, rounded to the nearest integer, are lent from each specialty within their division. Fourth, it extends the bed-lending policy further into an optimized allocation while keeping these pools separate in each division.
The model is tested 30 times for each strategy. The objective was to minimize the number of patients with an ED LOS of ≥6 h. The objective function and constraints are as follows.
Minimize: Σ(ED stay ≥ 6 h)
Subject to:
OTMG + OTMN + OTMn + OTMP = 158
OTSL + OTSS + OTSC = 101
33 ≤ OTMG ≤ 58
19 ≤ OTMN ≤ 34
9 ≤ OTMn ≤ 32
30 ≤ OTMP ≤ 55
2 ≤ OTSL ≤ 8
73 ≤ OTSS ≤ 97
0 ≤ OTSC ≤ 3
where:
OTMG = Optimized number of beds in Gastroenterology
OTMN = Optimized number of beds in Neurology
OTMn = Optimized number of beds in Nephrology
OTMP = Optimized number of beds in Pulmonology
OTSL = Optimized number of beds in Thoracic Surgery
OTSS = Optimized number of beds in General Surgery
OTSC = Optimized number of beds in Cardiac Surgery
Results
We evaluated 4 bed allocation strategies across 7 departments within the Internal Medicine and Surgery Division, comparing their impacts on ED LOS. Tables 4 and 5 summarize the key statistics for each strategy. For Strategy 1, an ED nursing utilization rate of 45.65% was exhibited, with patients experiencing extended LOS as follows: 2.48% exceeding 6 h, 0.37% exceeding 12 h, and 0.12% exceeding 24 h. Strategy 2, which implemented optimized bed allocation, slightly shifted the average ED nursing utilization rate to 45.66%. However, this strategy showed slightly higher extended LOS metrics: 2.56% stayed longer than 6 h, 0.43% longer than 12 h, and 0.14% longer than 24 h. Strategy 3 introduced cross-departmental bed sharing (14 beds, representing 5.4% of the total capacity) while maintaining existing bed allocation, yielding an overall ED nursing utilization rate of 45.71%. The extended LOS metrics were similar to those in Strategy 1, where 2.49% of patients had LOS greater than 6 h, 0.37% greater than 12 h, and 0.12% greater than 24 h. Strategy 4 combined optimal bed allocation with bed borrowing, utilizing 13 beds, or 5.0% of the total capacity for sharing among departments. The ED nursing utilization rate was 45.65% in this strategy. The extended LOS metrics remained stable, with 2.48% staying longer than 6 h, 0.38% longer than 12 h, and 0.12% longer than 24 h.
The Result of Simulated Bed Allocation.
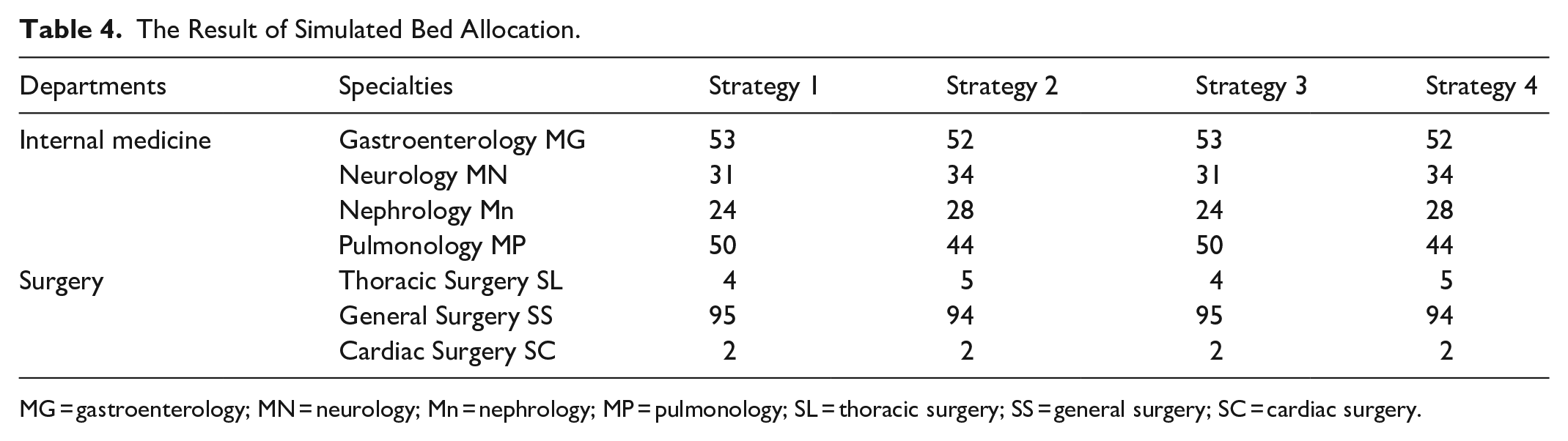
MG = gastroenterology; MN = neurology; Mn = nephrology; MP = pulmonology; SL = thoracic surgery; SS = general surgery; SC = cardiac surgery.
The Result of Simulated Metrics.
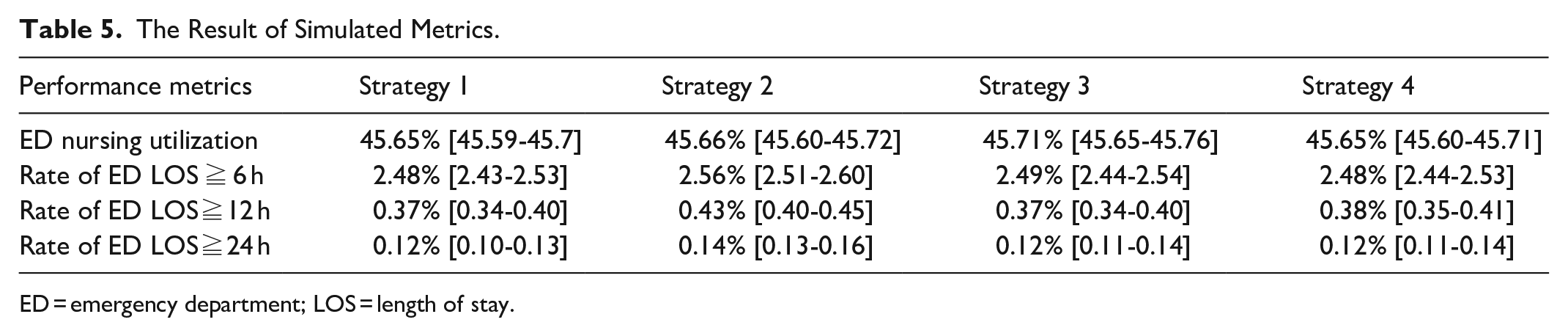
ED = emergency department; LOS = length of stay.
Figure 2 shows a comparison between the simulated current state and the results of the strategy implementation. Improvement rates were calculated as the percentage reduction in the extended LOS metrics compared with the current state. For example, the current simulated rate of ED LOS exceeding 6 h was 2.80%, strategy 1 reduced this metric to 2.48%, and the improvement rate was [(2.62-2.48)/2.62] × 100% = 5.34%. All strategies showed significant improvements compared with the current state. The clinical significance of these improvements should be considered alongside the statistical significance, as even small reductions in extended LOS can meaningfully impact patient experience and ED operations.

Improvement rates of extended length of stay metrics under different strategies.
Discussions
This study had several key findings. First, none of the 4 strategies significantly changed the average utilization by ED nursing staff. Second, the low metrics of patients experiencing ED LOS greater than 6, 12, and 24 h, with no patients staying longer than 48 h, indicate minimal impact on the overall workload of ED nurses who were responsible for the care of patients waiting for inpatient beds. Finally, all 4 strategies appeared in a far better shape compared to the present one, in particular, a tremendous decrease in the share of patients who stay in the ED for more than 12 and 24 h. However, borrowing and sharing strategies resulted in more than two-fold higher rates of ED LOS of more than 6 h compared with an optimal bed allocation strategy. Furthermore, these methods resulted in close to a 10% higher rate of ED LOS exceeding 12 and 24 h compared to the optimal bed allocation model, indicating that resource- and bed-sharing capabilities are effective approaches for improving ED patient flow.
Our results showed that although all strategies improved the current state, the most promising approach to address ED congestion without increasing nursing workload (45.65%, 95% CI: 45.60-45.71) significantly involved integrating optimal bed allocation with bed borrowing (Strategy 4). If we only optimize the beds between departments without considering external resources, such as borrowing, Strategy 2 would be the best choice, and it still shows an improvement of approximately 20% in the current LOS. These findings help to develop important knowledge regarding the effect of flexible resource allocation to deal with overcrowding in the ED, which is an important challenge for the modern healthcare system.
The stability of ED nursing utilization rates (approximately 45.7%) across all 4 strategies represents a significant finding that merits careful consideration. Jin et al believed that due to fluctuations in bed occupancy rates and nursing demand levels, the required nursing staff may vary greatly from day to day. This makes traditional “fixed scheduling” staffing systems inefficient, costly, and potentially unsafe. Therefore, an on-call mode was designed, and the study also found that, compared to fixed scheduling, the on-call mode had lower annual costs. 21 However, this method may not necessarily apply to Taiwan’s high-pressure, high-demand medical environment. Our results suggest that strategic bed management can improve patient flow without an additional burden on nursing staff. This difference might be attributed to our integrated approach, which considers both department-specific needs and cross-departmental resource-sharing. This finding aligns with Izady et al’s 22 research, where they also found through reconfiguring hospital beds can improve inpatient service efficiency. The demand for effective medical management, especially in the allocation of specialized beds, is very important. 23
Particularly noteworthy is the substantial reduction in extended LOS cases achieved through Strategy 4. The combination of optimal bed allocation with controlled bed borrowing (utilizing 5% of the total capacity) demonstrated that even modest cross-departmental resource sharing can yield meaningful improvements. Although Strategy 2 does not perform as well as Strategy 4, its advantage lies in its simplicity. This finding aligns with Tsai et al’s 24 research, which emphasized the importance of balanced resource utilization in managing ED congestion. However, their study focused on evaluating the effect of suppressing daily variations in the ED by adjusting the number of empty beds per day. Our study concentrated on reallocating the beds assigned to each department.
Our findings contribute to the growing body of literature on healthcare operation management in several ways. Previous studies have demonstrated that a slight increase in bed numbers could reduce the patient waiting time 25 and designed a new queue system for better bed allocation. 26 However, beds are not managed by a single department. When allocating bed resources to satisfy ED patient needs, it is difficult to identify the most appropriate department that can share it. We challenge the traditional department-centric bed management approach by demonstrating that controlled resource sharing can benefit both the ED and inpatient departments. Second, the results support the theoretical framework regarding the relationship between resource flexibility and system efficiency in healthcare settings. 27
All these strategies could also be implemented in practical terms to consider organizational dynamics. Bed borrowing and bedsharing mechanisms clearly require a protocol, communication system, and interdepartmental cooperation if they are to work. Some of the key considerations, especially in implementing the proposed bed allocation strategies, are the establishment of explicit criteria for bed borrowing, with defined triggers and protocols for resource sharing, robust information systems that can monitor bed availability and ensure timely communication among departments, and staff training and engagement that are critical to successful implementation, given that resistance to change is a frequent obstacle in healthcare settings. Our findings suggest that as little as 5% sharing may yield significant benefits, which can ease the transition for hospitals and may be more tolerable to the department.
This study was conducted in a 946-bed regional teaching hospital located in rural central Taiwan, which is one of the nation’s 46 primary emergency responsibility hospitals. While this specific context may limit the direct generalizability to all hospital settings, the principles of resource optimization and flexible bed allocation are broadly applicable. Hospitals with similar bed capacities and departmental structures, particularly those in the Asia-Pacific region with comparable healthcare systems, may find our strategies particularly relevant.
A 3.14% rate of ED LOS exceeding 6 h for hospitalization should be considered a notable problem in the context of Taiwan’s healthcare system. According to the Taiwan Healthcare Indicator Series (THIS), reducing the ED LOS is a key performance indicator for hospital accreditation. The selected hospital’s ED LOS was relatively good compared to some international benchmarks. In comparison to other developed countries such as the United States, Bouda Abdulai et al’s 28 study points out that 32% of ED patients need to wait more than 6 h. Kalen’s 29 study indicates that more than 16% will wait for more than 8 h. There still remains room for improvement in Taiwan’s high-efficiency healthcare system. This is particularly important given the country’s aging population and the 78% increase in ED visits since 2004, as noted in the introduction. Furthermore, the clinical impact of extended ED stays on patient outcomes, staff workload, and system capacity makes addressing this issue a priority regardless of its comparative standing.
Overall, the findings of this study have several practical implications for ED management. The proposed bed-sharing system can be implemented with minimal structural changes. The 5% bed-lending policy provides a concrete starting point for hospitals. The combined strategy offers a balanced approach between optimization and practical constraints. The stable nursing utilization rate suggests that the changes do not increase staff burden.
This study has several limitations that should be considered. First, our simulation model assumed bed transfer under ideal conditions, and thus might not capture the full range of conditions that exist in reality, such as staffing constraints and seasonal fluctuations in the volume of patients. Second, the study was conducted within 1 hospital, and thus may not allow generalization of our findings to diverse healthcare settings. Third, the impact of bed sharing on specialty-specific care quality and patient outcomes was not measured directly.
Conclusion
This study demonstrated that combining optimal bed allocation with controlled bed-sharing policies can effectively reduce ED LOS while maintaining operational stability. In addition, the operational stability is preserved. The optimal strategy achieved a 30% reduction in extended ED LOS, stable nursing utilization of 45.65%, and a significant decrease in prolonged stay cases, suggesting that hospitals can enhance emergency patient flow via planned resource handling. Further studies should examine the implementation of these approaches at various medical facilities and assess their viability.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251335799 – Supplemental material for Optimizing Emergency Department Patient Flow Through Bed Allocation Strategies: A Discrete-Event Simulation Study
Supplemental material, sj-docx-1-inq-10.1177_00469580251335799 for Optimizing Emergency Department Patient Flow Through Bed Allocation Strategies: A Discrete-Event Simulation Study by Sen-Tian Wang, Shao-Jen Weng, Ting-Yu Yeh, Chih-Hao Chen and Yao-Te Tsai in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Appendix
Simulation Model Parameter Setting.

| Parameter type | Description | Value/setting |
|---|---|---|
| Arrival Time | The patient enters the ED | Empirical data |
| Triage Staff | Emergency triage personnel | 3 Staff |
| Specialty Clinics | Emergency treatment units (internal medicine, surgery, pediatrics, etc.) | 1 Staff per specialty |
| Examination Resources | Examination capacity for patient level 1 to 5 | 1 Staff per triage level |
| Laboratory Resources | Laboratory capacity for patient level 1 to 5 | 1 Staff per triage level |
| Imaging Equipment | X-ray | 1 Unit, uniform (5,15) min |
| MRI | 1 Unit, exponential (20) min | |
| Other examinations | 1 Unit, average (10) min | |
| Emergency Observation | Pediatric observation area | 10 Beds |
| General observation area | 40 Beds |
ED = emergency department; MRI = magnetic resonance imaging.
Acknowledgements
None.
Ethical Considerations
This research did not require IRB approval because it does not involve in any human participants or personal data.
Consent to Participate
The data was collected based on administrative process. Informed consent is not applicable.
Author Contributions
S.T.W. and S.J.W. conceptualized and designed the study; T.Y.Y. and C.H.C. conducted data analysis and interpretation; Y.T.T drafted the manuscript; All authors reviewed and edited the manuscript for intellectual content. All authors have read and approved the final version of the manuscript.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Chang Bing Show Chwan Memorial Hospital (grant number: BRD-111005).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.