
Abstract
The success of telehealth programs to guide clinicians to perform sexual assault medical forensic examinations relies on clinicians’ positive attitudes toward telehealth services, though no validated tools to measure these variables exist. This study aims to report validity and reliability of a novel tool with two scales: Positive Beliefs and Acceptance scales for hospital nurse clinicians at sites initiating the Texas Teleforensic Remote Assistance Center (Tex-TRAC). An analysis of pre-post cross-sectional data of hospital nurse clinicians (N = 121) trained in the use of Tex-TRAC telehealth technology at seven participating hospitals in Texas from July 2022 to May 2023 was performed. The Kaiser-Meyer-Olkin (KMO) measure of sampling adequacy and Bartlett’s test of Sphericity sample size analysis were performed. Exploratory Factor Analysis (EFA) was applied for validity and internal consistency reliability Cronbach alpha (α) values were described for two scales: Positive Beliefs and Acceptance scales. Positive Beliefs scale has a KMO value of 0.810 and Barlett’s test of sphericity (χ2 (6) = 380.47, P < .001). Acceptance scale has a KMO value of 0.832 and Barlett’s test of sphericity (χ2 (28) = 432.19, P < .001). After Promax Oblique rotation, the final four-item Positive Beliefs scale had α = .894; the final five-item Acceptance scale had α = .876. Validity and reliability of both scales demonstrated potential usefulness for future telehealth interventions engaging Sexual Assault Nurse Examiners. Continued use of these scales could provide additional information that can be leveraged in training curriculum of similar telehealth programs like Tex-TRAC.
Keywords
What do we already know about this topic?
There were tools that assess the different aspects of hospital nurse clinicians.
The research makes a meaningful contribution of a novel tool with two scales: Hospital nurse clinicians’ Positive Beliefs and Acceptance scales. These scales are important to understand the hospital nurse clinicians’ positive attitudes toward the services that use telehealth technology and acceptance of telehealth technology. This study adds the existing literature by examining the validity and reliability of the tool that has potential to use with the hospital nurse clinicians in other projects that use telehealth technology.
The current study demonstrated that the tool is valid and reliable to assess the hospital nurse clinicians’ positive attitudes and acceptance on telehealth technology. This suggests that the tool has potential to apply in other telehealth projects.
Introduction
Approximately one in five women and one in 14 men in the United States report experiencing attempted or completed rape at some point in their lifetimes. 1 Despite these alarming statistics, very few sexual assault survivors seek medical treatment in the emergency department (ED). These sexual assault survivors still face many challenges, including further psychological distress caused by healthcare providers with limited training in providing trauma-informed, patient-centered sexual assault medical forensic examinations. 2 Sexual assault nurse examiners (SANEs) have become the gold standard in providing Sexual Assault Forensic Examinations (SAFEs) when sexual assault survivors present for treatment. However, many EDs lack 24-hour access to experienced SANEs. Telehealth programs for SAFE have become an increasingly utilized strategy to increase access to high-quality SAFEs when a hospital has no SANE on staff or contract or the SANE is not very experienced. Access to SANEs via telehealth can provide real-time guidance to hospital nurse clinicians in order to perform SAFEs.3-5 However, the success of telehealth programs depends on clinicians’ positive attitudes (ie, positive beliefs and acceptance) regarding the technology. 6 While a handful of studies to date have examined clinicians’ attitudes toward telehealth for SAFEs, no standardized measures of hospital nurse clinicians’ positive beliefs and acceptance have been validated. A validated standardized measure would help compare baseline differences in hospital clinicians’ attitudes across different sites for tailored training aimed at increasing positive attitudes toward telehealth assisted SAFEs.
In a large state with a wide rural area such as Texas, SANEs are largely limited to urban areas, leaving much of the 78% of Texas counties designated as rural, with limited access to SANEs. 7 In 2013, Texas passed legislation requiring all healthcare facilities with EDs to treat presenting sexual assault survivors who do not want to transfer to a facility with forensic nurses available (known as a “sexual assault forensic exam (SAFE)-ready facility”). 8 However, Davis et al 9 found hospital personnel still preferred to transfer sexual assault survivors to SAFE-ready facilities, sometimes 50 or more miles away, due to their reluctance to have a non-SANE clinicians with minimal forensic exam training to conduct a SAFE. Transferring patients poses several challenges, such as (1) the patient might not present to the referred facility, especially if the initial response was not trauma-informed;8,9 (2) added travel time poses additional safety and health risks;10,11 (3) additional emergency room charges; (4) time-sensitive prophylactic medications may be delayed; 12 and (5) evidence may be lost or contaminated. 13 At the same time, treating sexual assault survivors at the presenting site is optimal, but only if care is high-quality, patient-centered, and trauma-informed. In 2017, the Texas legislature updated the definition of SAFE-ready facility to include a forensic nurse providing guidance to a local clinician via telehealth.
Telehealth technology is a promising practice to increase access to high quality clinical and forensic management including SAFEs in rural areas, thus preventing transfers. Clinicians’ attitudes toward and acceptance of telehealth programs have been demonstrated to be critical to the success of the telehealth programs and it is likely the case with the telehealth for SAFEs.6,14,15 Systematic evaluation of clinicians’ attitudes early in the process can mitigate barriers to improve access to quality care. 16 Despite the existence of tools that demonstrated nurse clinicians attitudes and acceptance of telehealth programs for other health areas, there are no validated tools that can be applied to hospital nurse clinicians.
The purpose of this study was to examine the validity and reliability of a novel tool with two scales: Positive Beliefs toward and Acceptance of using Texas Teleforensic Remote Assistance Center (Tex-TRAC) telehealth technology which connects hospital ED clinicians to expert SANEs via telehealth (referred to as TeleSANEs). 17 To our knowledge, this is the first study that tests the validity and reliability of scales to measure hospital nurse clinicians’ attitudes towards the a TeleSANE telehealth platform.
Methodology
Study Setting
Cross-sectional data were collected from July 2022 to January 2024 using an online-delivered pre-post survey instrument during the delivery of the initial Forensic and CART training for the hospital nurse clinicians of Tex-TRAC program. 17 Partnering Tex-TRAC hospital nurse clinicians participated in the Tex-TRAC Forensic and CART Training at their respective rural and underserved hospitals. The training was conducted by Tex-TRAC staff and training modules included a Tex-TRAC program overview (ie, about the Tex-TRAC program components including its goals, and objectives, activities), sexual assault, trauma-informed care, and hands-on skills training for using the Tex-TRAC telehealth technology equipment. To validate the questionnaire, cross-sectional pre-survey responses from the training participants (N = 121) at partnering ED hospitals in Texas were used. This study was approved by the Institutional Review Board of Texas A&M University (IRB2019-1227F) which was renewed on February 2, 2025.
Study Design and Procedures
The evaluation team developed a questionnaire based on a survey used in Kaldeweide 18 to measure the uptake of eHealth technology among healthcare providers, adapting it to align with the Tex-TRAC TeleSANE telehealth program. The questionnaire for the present study included 34 questions (Supplemental Table 1) which asked participants about previous forensic nursing education (ie, prior training on SAFEs), type of previous forensic training (ie, 2-hour basic evidence collection training course, 6-hour Tex-TRAC Forensic and CART training, 40-hour Sexual Assault Nurse Examiner course), knowledge about conducting a SAFE, and positive beliefs and acceptance towards general use of telehealth as well as the Tex-TRAC telehealth technology. This study focuses on two main areas of interest: hospital clinicians’ Positive Beliefs and Acceptance of the Tex-TRAC telehealth technology.
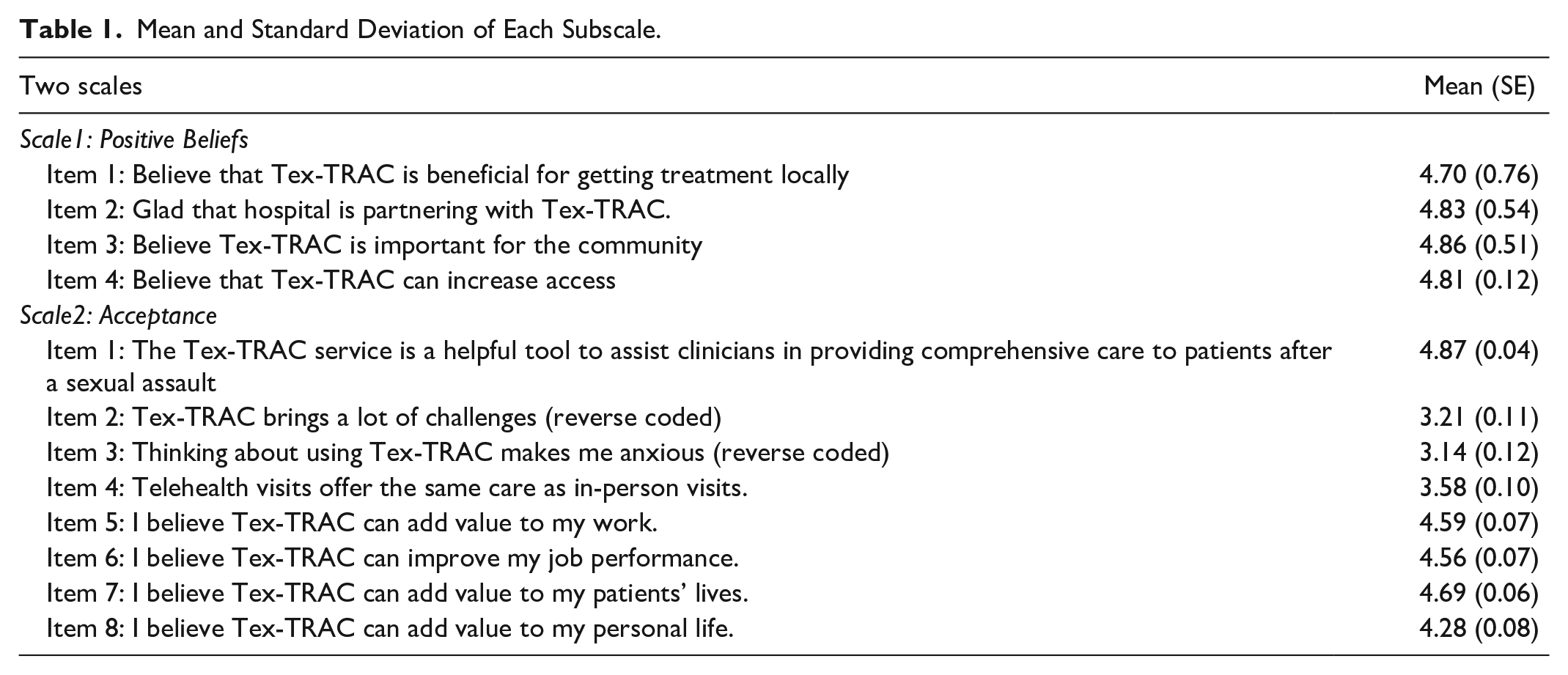
The Positive Beliefs scale contains four items, and the Acceptance scale has eight items (Table 1). Responses for both scales were rated on a 5-point Likert scale (Strongly Disagree = 1, Disagree = 2, Neither Agree nor Disagree = 3, Strongly Agree = 4, Strongly Disagree = 5). The composite scores for the four-item Positive Beliefs scale ranged from 6 to 20 and the eight-item Acceptance scale ranged from 8 to 36.
Mean and Standard Deviation of Each Subscale.
Inclusion/Exclusion Criteria
This study used a convenience sample of hospital nurse clinicians completing the Tex-TRAC Forensic and CART Training. Consent was obtained maintaining anonymity through a question at the end of the survey: “This survey data is anonymous and cannot be linked back to you. Do you consent to the project team using the data you submit for research purposes?” This study only includes participants responses of “yes.”
Data Description
Data collection occurred as pre- and post-training surveys; we excluded post-training surveys if the pre-training survey was not completed. Data was downloaded in CSV format from Qualtrics 19 and exported into Stata version 18.0. 20 Data was cleaned for detailed analyses by checking for missing variables, describing study variables, and recoding as needed. Response rates of items were also assessed (Supplemental Tables 2 and 3).
Sample Size Determination
Sample size was considered using different approaches during analysis. A large body of research supports the use of two common approaches for sample size: calculation on the subject-to-item ratio of 5:1 to 10:1 or using absolute. 21 Our item ratio for the Positive Beliefs scale is 10:4 with minimum required sample size should be 40, whereas the item-ratio for Acceptance scale is 10:8 with minimum required samples size should be 80. We also performed sample size estimation calculations recommended by Vanderziela et al, 22 which is based on the following formula.

In the above formula, n denotes the estimated sample size,
To confirm the above two methods, we performed the Kaiser Meyer Olkin (KMO) measure of sampling adequacy test and Bartlett’s test of sphericity, an objective test that assessed the factorability of the correlation matrix.23-25 A KMO’s measure of at least 0.50 is considered necessary to perform sampling adequacy (Supplemental Table 4).23-25
Statistical Analysis
Participants rated each item in the scale on a 5-point Likert scale (Strongly Disagree = 1, Disagree = 2, Neither Agree nor Disagree = 3, Strongly Agree = 4, Strongly Disagree = 5). Two questions in the Acceptance subscale were reverse scored (items 2 and 3) in analyses. We described the values of mean and standard errors (SE) of each item and reported the number of factors retained, uniqueness value, and internal consistency reliability. 26 For deciding the factors to be maintained, we used more than one criterion., that is, Kaiser criterion27,28 and Scree plot. 29 Kaiser’s criterion applied the eigenvalues >1 to retain the factor.
To measure construct validity, we performed Exploratory Factor Analysis using Principal Factor Analysis method separately for each item. We applied the Oblique Varimax (oblique) rotation method, which allows factors to be correlated. 30 The oblique Promax rotation represents how variables are weighted for each factor. The variables with eigenvalues greater than zero (after rotation) are retained.
We reported internal consistency reliability with Cronbach Alpha.31,32 Previous scholars have recommended an acceptable Cronbach Alpha’s as .70; however, for the psychometric properties of scales, the preferred cut-off Alpha values for the reliability are .80 for good or .95 for excellence, respectively.32-34 We used the Enhancing Quality and Transparency of Health Research (EQUATOR) guideline: Specifically, “Strengthening the Reporting of Observational Studies in Epidemiology (STOBE)” 35 checklist (Supplemental Table 5).
Handling of Missing Values
We determined missingness > 5% and reported as relevant.36,37
Results
All clinicians completing the surveys were hospital nurses. The means and Standard Errors (SE) of both scales analyzed in this study can be found in Table 1. The response rates for each item included in each scale ranged from 99% to 100% (Supplemental Tables 2 and 3), with a total of 121 completed surveys, thus meeting the sample size criterion.23-25,38,39 The results from the KMO measure of sampling adequacy and Bartlett’s test of sphericity illustrated that our sample size for each question was adequate to perform factor analysis. The result of KMO measure of sampling for the Positive Beliefs scale (four items) was 0.810 and for the Acceptance scale (eight items) was 0.813, showing both questions had adequate samples (ie, KMO ratios >0.5). The results from KMO measure of sampling adequacy and Bartlett’s test of sphericity showed the sample sizes were adequate for each scale, and the items were assumed to be intercorrelated, P < .001. KMO measures >0.80 are considered good or excellent, and <0.50 are considered inadequate (Supplemental Table 4). All study questions had adequate sample sizes for factor analyses.23,24
Exploratory Factor Analysis
The results of EFA after factor rotation for both the Positive Beliefs scale and Acceptance scale are presented. The results from the EFA of Positive Beliefs scale showed only one factor (factor 1) had eigenvalues >1, whereas results from the EFA of Acceptance scale showed four factors (factor 1 to 4) positive eigenvalues 40 (Table 2).
Results of Exploratory Factor Analysis (EFA) for Both Scales.

Note. 1. For positive belief scale, we need to run EFA only one time as all the items have good uniqueness values. So, our model keeps all four items.
For acceptance scale, we need to run EFA for three times dropping items that have uniqueness scales >0.6, considering those items were not well explained by the factors. And thus, our final model of acceptance scale maintains only five items (Item 1, 5, 6, 7, 8).
Denote the uniqueness value is acceptable (i.e., <0.6). Only positive factor values are reported.
A Scree test was performed to plot the eigenvalues for visual observation, and in the scree plot of the Positive Beliefs scale (Figure 1), the “elbow joint” indicates the cut-off number of factors for consideration. Results indicate the first factor explains the major portion of the variance in the Positive Beliefs scale. Similarly, the first two factors of Acceptance scale were retained as the eigenvalue is greater than 1 (Figure 2). After applying Promax oblique rotations, all the items under Positive Beliefs scale showed good uniqueness value (i.e., <0.6) 41 (Figure 1 and Table 2). Therefore, we retained all four items.

Scree plot of eigenvalues after factor loading of Positive Beliefs scale.

Initial scree plot of eigenvalue after factor loading of acceptance scale.
On the other hand, after Promax rotation was applied for the Acceptance scale, one of the items (item 4) had a uniqueness value of 0.72. Therefore, we dropped item 4, and repeated analyses. This time, we observed that the retained factor is 1 and the uniqueness value for items 2 and 3 was high at 0.87 and 0.91 respectively. Therefore, we dropped those two items, after checking with the scree plot to determine the factors to be retained (Figure 3), and EFA with Promax rotation was performed again. This time, all the remaining items (items 1, 5, 6, 7, 8) showed acceptable uniqueness values. Thus, providing a final five-item Acceptance scale.

Scree plot of eigenvalue after factor loading of acceptance scale (after dropping item 4 which has uniqueness value >0.6).
Internal Consistency Reliability
The results from internal consistency reliability for the four-item Positive Beliefs scale demonstrated a good Cronbach’s alpha coefficient (α = .832), an acceptable level for a novel scale. Results from the internal consistency reliability of the five-item Acceptance scale also showed a good Cronbach’s alpha coefficient (α = .876). The final models for both the Positive Beliefs and Acceptance scales are shown in Table 3.
Description of Items Included in the Final Scales.

Note. Responses were 5-point Likert scale (strongly disagree = 1, somewhat disagree = 2, neither agree nor disagree = 3, somewhat agree = 4, strongly agree = 5).
Discussion
This study examined the validity and reliability of a novel tool used with hospital nurse clinicians to measure attitude towards Tex-TRAC telehealth technology, specifically the two scales of Positive Beliefs and Acceptance. These scales were used during the training of hospital clinicians prior to using the Tex-TRAC telehealth technology to provide 24/7 access to an expert SANE in order to address the needs of rural and underserved sexual assault survivors in rural Texas hospital emergency departments. The sample size is adequate for performing factor analysis. Specifically, in our study, 121 hospital nurse clinicians completed and consented for the survey, which was sufficient to proceed with the factor analysis based on the KMO sampling adequacy test and Bartlett’s test of sphericity. 23 Our methods were consistent with a study done by De Winter et al, 42 which found that a sample size as small as 12 is adequate if there is as high as 0.90. Also, we are confident that the sample was sufficient to perform the factor analysis as the results from KMO showed sampling adequacy.
In our analysis, we retained four factors for the Positive Beliefs scale after the first rotation. However, for the Acceptance scale, only five items were retained after three rotations. Both final scales of the novel tool showed a good alpha value, it can be assumed that these scales are valid and reliable to apply in new or current program similar to the Tex-TRAC program either in Texas or other states. Understanding the clinicians’ beliefs towards and acceptance of telehealth technology could be useful to provide insight regarding retention, which subsequently could lead to increased access to high quality care for sexual assault survivors. 16
As per our results from the EFA analysis of the Positive Beliefs scale, we retained only one factor with eigenvalue greater than 1 and all four items with uniqueness values <0.6. 41 In the Acceptance scale, we observed from the factor loading five items had uniqueness values <0.6 as we retained the items with a uniqueness value <0.6 as they were well explained by the retained factor.
Overall, the present study’s internal consistency reliability of two scales showed a high Cronbach’s alpha value, suggesting homogeneity, that is, the items measure the same underlying construct, of these scales. In many fields that assess attitude, Cronbach’s alpha is widely used. 43 However, some might argue a very high Cronbach alpha may be due to items which are not very well related to each. 31
When implementing innovative interventions, the belief and acceptance of the users, in our case hospital nurse clinicians, are important for participant retention and program sustainability. Our findings support a prior finding by Wade et al, in which the clinicians’ acceptance of telehealth services is critical in the future use, expansion of services, and sustainability. 6 Because hospital nurse clinicians are interacting with traumatized patients while using the innovative Tex-TRAC telehealth technology, ensuring their Positive Beliefs and Acceptance of the program is critical. Moreover, a study by Allison et al 44 found that having access to a TeleSANE could improve the confidence and self-efficacy of hospital clinicians using telehealth technology especially providing forensic medical examination for sexual assault survivors. Using scales that are valid and reliable to measure their Positive Beliefs and Acceptance is important for the quality of assessment and results. With no prior validated tools to assess Positive Beliefs and Acceptance of hospital nurse clinicians using a TeleSANE telehealth technology, our findings suggest a potential tool for future use in similar TeleSANE programs providing services to sexual assault survivors. Also, prior literature revealed a high turnover rate among SANEs and clinicians due to many factors including satisfaction, positive attitude, and acceptance,45-47 indicating these are important factors for retention and subsequently for increasing healthcare access for sexual assault survivors. Since our current tool did not include the measure for job satisfaction and intention to stay in the sexual assault field, further research is warranted in this regard. 48 Nevertheless, our final scales in the tool showed good validity and reliability, highlighting its potential for use in other geographically rural areas throughout the U.S., specifically rural and underserved areas lacking immediate access to SANEs, and a telehealth intervention could increase access to immediate care. 49
Limitations
This is the first known tool that has been validated for use to examine hospital nurse clinicians’ Positive Beliefs and Acceptance toward the use of a TeleSANE telehealth technology in a systematic manner. A particular strength of the final developed tool was the high Cronbach Alpha value for the scales. However, there were some limitations. As the Cronbach Alpha does not indicate the stability or consistency of the test over time, nor indicate the stability and consistency of the test of the different test formats, it might be helpful to test the tool using a different format (i.e., paper-based survey). As in other studies that have self-reported responses, social desirability bias is a possibility which may lead to spurious correlations between variables. In addition, the current study presents the results validating a tool that was completed by hospital clinicians, especially nurses, who serve sexual assault survivors. Therefore, caution might be needed when or if applying to clinicians who provide services for other patients (i.e., non-traumatized patients), or other types of clinicians, when implementing a telehealth program. Moreover, our scales are meant to be used with hospital nurse clinicians, and did not include other important factors such as other staff members including hospitals administrators, 50 budget allocation, and feasibility of telecommunication in the particular geographic areas. Finally, we acknowledge that retention of the nurse clinicians and sustainability of the program requires more than two aspects (i.e., hospital clinicians’ Positive Beliefs and Acceptance); future research is recommended to consider other factors such as satisfaction, working environment, and support system.46,47
Conclusion
Hospital nurse clinicians’ Positive Beliefs and Acceptance of a TeleSANE telehealth technology for real-time technical/clinical support to perform sexual assault medical forensic examinations on survivors in rural and underserved communities is critical to the success and sustainability of such programs. While the tool was not meant to measure the comprehensive aspects (such as retention and sustainability), for further utilization among hospital clinicians, our findings confirmed that this is a valid and reliable tool, capturing hospital nurse clinicians’ attitudes using Positive Beliefs and Acceptance scales while having acceptable construct validity and internal consistency reliability. This tool can be used confidently to collect similar training at sites that plan to use a TeleSANE telehealth technology. Results can be used to adapt training to address hospital nurse clinicians’ attitudes in real time to mitigate barriers to TeleSANE telehealth technology uptake. The use of the Tex-TRAC’s TeleSANE telehealth technology will be sustained only when hospital nurse clinicians believe it is beneficial to the community and only when they accept the use of the telehealth technology.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251332790 – Supplemental material for Valid and Reliable Attitude Scales for Measuring Clinician’s Attitudes Towards Telehealth Assisted Sexual Assault Forensic Exams: Using a Pre-Post Survey
Supplemental material, sj-docx-1-inq-10.1177_00469580251332790 for Valid and Reliable Attitude Scales for Measuring Clinician’s Attitudes Towards Telehealth Assisted Sexual Assault Forensic Exams: Using a Pre-Post Survey by Wah Wah Myint, Heather R. Clark, Kim Zemanek, PhD, Kayce Ward, MSN, Stacey A. Mitchell, DNP and Nancy R. Downing, PhD in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-1-inq-10.1177_00469580251332790 – Supplemental material for Valid and Reliable Attitude Scales for Measuring Clinician’s Attitudes Towards Telehealth Assisted Sexual Assault Forensic Exams: Using a Pre-Post Survey
Supplemental material, sj-pdf-1-inq-10.1177_00469580251332790 for Valid and Reliable Attitude Scales for Measuring Clinician’s Attitudes Towards Telehealth Assisted Sexual Assault Forensic Exams: Using a Pre-Post Survey by Wah Wah Myint, Heather R. Clark, Kim Zemanek, PhD, Kayce Ward, MSN, Stacey A. Mitchell, DNP and Nancy R. Downing, PhD in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Ethical Considerations
This study was approved by the Institutional Review Board of Texas A&M University (IRB2019-1227F) on March 24, 2022, with renewal approval on February 5, 2025.
Consent to Participate
We collected de-identifiable participant data. Also, the participants were asked if consented to use their de-identifiable data.
Author Contributions
WWM: A lead author, conceptualization, data analysis, preparation of draft, and final manuscripts. HRC: Co_author. Guided the structure of the article, regularly reviewed, and provided suggestions from time to time, critically reviewed and edited draft and final manuscripts. KZ: Co_authors. Reviewed critically and edited the draft and final manuscripts. SM: Co_authors. Reviewed critically and edited the draft and final manuscripts. KW: Co-author: Verified the data and reviewed critically the final manuscript. NRD: Co_author: Reviewed critically, edited drafts and final manuscripts, and provided the suggestions from time to time.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Tex-TRAC was supported by grant number 2019-V3-GX-K019, awarded by the Office for Victims of Crime, Office of Justice Programs, U.S. Department of Justice. Tex-TRAC is also supported through an agreement with the Texas Attorney General’s Office in response to Senate Bill 71, establishing a statewide telehealth center for sexual assault medical forensic examinations. The opinions, findings, and conclusions or recommendations expressed by the Tex-TRAC team are those of the contributors and do not necessarily represent the official position or policies of the U.S. Department of Justice or the Texas OAG.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.