
Abstract
This research compared healthcare services utilization among older persons living in urban and rural Vietnam and determined the key factors contributing to their differences. A nationally representative sample of 3,049 older Vietnamese people in 2019 was used with multivariate logistic regressions and Poisson regressions to identify factors influencing the probability and frequency of service utilization. The standard concentration index (CI) and Erreygers concentration index (EI) were applied to measure the differences. The extension of the Oaxaca-Blinder decomposition was used to examine the rural-urban differences in healthcare services utilization and quantify factors contributing to the differences. CIs and EIs were relatively small and nearly zero, meaning that both inpatient service utilization and outpatient service utilization were equally distributed across all household wealth quintiles, regardless of their residence of living. Oaxaca-Blinder decomposition analysis results revealed statistically significant differences between rural and urban older persons in outpatient service utilization, in terms of its probability and frequency. Rural persons had 4.9% lower in the probability of outpatient services utilization than their urban counterparts. Similarly, rural residents had 3.033 times lower in the frequency of outpatient services utilization than urban residents. The use of health insurance during medical treatments and poor health status were two significant determinants explaining the urban-rural differences in healthcare utilization among older adults. Based on the crucial findings, continual development of the health insurance scheme and investment is recommended to support the rural older population in accessing healthcare. Future research opportunities include exploring a more comprehensive understanding of this field, such as examining the factors influencing the choice of healthcare facilities, reimbursement rates, and out-of-pocket expenses for older individuals in urban and rural areas. Additionally, longitudinal studies are recommended to investigate causal relationships in healthcare service utilization among older Vietnamese.
Keywords
What do we already know about this topic?
Urban-rural gaps have been a critical issue in all socio-economic and health aspects, particularly in low- and middle-income countries (LMICs) facing aging populations. The gap in utilization of healthcare services has been emerged in both academic and policy studies since demand for healthcare and accessibility to healthcare services between urban and rural older people are diverse.
Our study contributed to the existing literature by using a nationally representative data with various approaches to decompose differences to show the case of older persons in Vietnam as a middle-income country with a rapidly aging population.
Our study provided different policy implications for LMICs which are facing rapidly aging populations along with high demand for healthcare of older persons, that is, developing health insurance schemes for the rural older persons is essential to provide equitable benefits, particularly for chronic disease management and preventive care, while minimizing out-of-pocket expenses through subsidies or free services for low-income individuals.
Background
Population aging is one of the common socio-economic concerns where numerous countries have been experiencing profound population transitions. For the international comparability, several population aging terms were provided. An aging society is determined if the percentage of people aged 65 years and above ranges between 7% and 14%, meanwhile an aged society is defined if this percentage varies between 15% and 20%, and a super-aged society is classified if this percentage is 21% and above. 1 By regions, East and Southeast Asia region is leading this demographic transition where Hongkong, South Korea, and Japan were expected to experience the highest proportion of older population (those aged 65 and above) by 2050: 40.6%, 39.4%, and 37.5% of the total population, respectively.2,3 Following this trend, Vietnam became an aging society and was forecasted to experience a rapid older population growth rate within this region.2,4 While high-income countries took several decades to transit from aging to aged societies, for instance 26 years for Japan and 33 years for Hongkong, Vietnam is estimated to take only 20 years for this transition (from 2015 to 2035). 5
As a middle-income country, experiencing a bulging aging population posed an enormous social and economic challenges for Vietnam. In response to the rapid aging population, the Government of Vietnam (GOV) has simultaneously raised awareness to society and made tremendous efforts on enhancing the well-being, ensuring the social protection for this sub-population, and boost the macroeconomics of Vietnam. The Law on the Elderly and the Law on Social Health Insurance have been impactful policies that GOV has promulgated with the aim of improving access to and utilization of healthcare among older adults.6,7 In detail, these laws emphasized the rights and benefits of older citizens, as well as the responsibilities of families, establishments, and society in supporting older persons. Moreover, these laws designed to support disadvantaged and vulnerable older persons in accessing healthcare and social supports. Combining with the social assistance programs, which were amended by Decree 136/2013 (dated 21 October 2013), Decree 20/2021 (dated 15 March 2021), and the most recently Decree 76/2024 (dated 1 July 2024), older persons are provided with more packages of health and social care services along with better financial protection. For example, Decree 76/2024 regulated that older persons aged 80 and over without pension and other social welfare benefits are eligible to get free health insurance, and those with severe disabilities can receive home-based care where their voluntary care-givers can receive financial support. Also, commune health centers (CHCs) are in charge of managing treatments for older persons with high blood pressure and/or diabetes and all are paid by social health insurance. Previous evidence was revealed the efficacy of these policies on improving the accessibility and reducing economic burden on healthcare among the Vietnamese older adults.8 -10
As people in their advanced age, the prevalence of comorbidity (mainly non-communicable and chronic diseases) was relatively high among older population, resulting in a growing demand for healthcare utilization in Vietnam.11 -13 The healthcare system in Vietnam has three levels of health service delivery: (i) primary level, known as “grassroots healthcare system” (i.e. district health facilities and commune health centers); (ii) secondary level (i.e. provincial health facilities); and (iii) tertiary level (tertiary hospitals under the central government of Vietnam). These levels provide multiple healthcare services for older adults, depending on the nature of services and the severity of health conditions. Previous literature reported that the Vietnamese older adults were more likely to use outpatient services than inpatient services. Moreover, older adults were revealed differences in their healthcare seeking behaviors with respect to the choice of healthcare facilities. 14 Accordingly, among those who used healthcare services, only 8.84% chose commune health centers, while approximately 66.63% chose higher level of healthcare providers (i.e. district, provincial and central hospitals). Due to a shortage of trained personnel and limited availability of specialized care services for older patients in commune health centers, older adults with more complex health conditions are referred to higher-level hospitals.7,15,16 Healthcare-seeking behaviors and utilization among older adults are associated by various factors, such as age, gender, place of residence (urban/rural), employment status, household wealth, ability to pay for healthcare expenses, educational attainment level, health insurance, health-risk behaviors (such as alcohol and tobacco consumption), health programs supports, and health conditions.17,9,18,14,19
Urban-rural differences in accessibility and utilization of healthcare services are a crucial issue that need to be solved to promote a healthy aging society. Urban-rural differences in healthcare utilization among older persons have been widely investigated in countries at different income levels.20 -24 Interestingly, urban older persons were reported to have better probabilities or higher frequencies of healthcare utilization than their rural counterparts, highlighting that, regardless of wealth status, nations encounter relatively similar urban-rural differences in healthcare access, but might be different level of the differences. Previous studies consistently elaborated that urban people benefit from more developed infrastructure, a higher density of medical professionals, a wider range of specialized services, and easier access to healthcare than those in rural regions. 20 In other words, as a result of healthcare system factors, rural older persons might face multiple barriers in utilizing healthcare services when their needs arise. Thus, alleviating these differences within a community is essential for improving population health and avoiding further severe consequences, such as health inequalities or unmet need for healthcare and social care.25 -27
Although the bulging older population has been observed in a decade, urban-rural differences in healthcare utilization among older persons have received little attention in Vietnam. To the best of our knowledge, few related studies have been conducted in Vietnam, and none of them investigated urban-rural difference aspect.14,28,29 One of them studied gender differences, 28 while the remaining studied differences in choosing healthcare facilities.14,29 Moreover, these studies explored the issue by using outdated data and applying the logistic regression analysis, which made it inadequate for capturing the nuanced drivers behind the observed differences.
Given the international findings on urban-rural differences on healthcare utilization among older persons, it should be explored urgently in the Vietnam context as older population is substantially growing in this middle-income country. Thus, this study was conducted to address two research objectives: i) determine differences on healthcare service utilization among urban and rural Vietnamese older persons; and ii) examine factors contributing to the differences. This study was conducted using the nationally representative data on older persons of Vietnam, and thus all estimations can be inferential for the Vietnamese older population as a whole, rather than outdated or non-representative groups of older persons as in various previous studies.14,28,29
Data and Methods
Data
This study utilized secondary data from the Survey on Older Persons and Social Health Insurance in Vietnam in 2019 (in short, OP&SHI 2019). This cross-sectional survey comprised rich information of older participants in terms of demographic characteristics (such as age, gender, marital status, and ethnicity), family life and living conditions (such as living arrangements, housing conditions, and assets), health conditions (such as self-rated health and access to healthcare services), economic activities and sources of income (such as current employment, income and social protection benefits), and social relations (such as participation in community activities).
The OP&SHI 2019 sample was derived from the 2019 Population and Housing Census using the probability proportional to size (PPS) method. This sample was proportionately distributed according to the older population size across six ecological regions of Vietnam, namely Northern Midlands and Mountains, Red River Delta, Central Coast, Central Highlands, Southeast, and Mekong River Delta. The OP&SHI 2019 sample was drawn from both urban and rural residents. A multiple-stage sampling approach was employed to recruit eligible participants. In short, adopting the PPS method, 12 provinces/cities were selected across six ecological regions of Vietnam. From each of these provinces/cities, three districts were chosen, followed by the selection of four communes per district. Subsequently, three villages (clusters) were selected from each communes using a systematic random sampling. Finally, 10 eligible participants per village were chosen using the same systematic random sampling technique. One eligible participant each household were recruited in this study. The OP&SHI 2019 utilized complex household survey data with a large sample size applied using the PPS sampling technique. Since study interviewed one older adult per household, the unit of analysis in this study was individual older adults. As such, in all calculations and estimations, we used the sample weight to make all results representative for the entire Vietnamese older population.
This study applied the definition of older persons as those who aged 60 and above. 30 Regarding the inclusion criteria, eligible participants were those who: (i) were Vietnamese residents; (ii) aged 60 and above at the time of conducting interviews; (iii) currently resided and were available in the assigned villages for conducting research. Concerning the exclusion criteria, ineligible participants were those who: (i) dead; (ii) were absent at the time of conducting research (due to several reasons such as permanent changes in residence or short-term stay at different locations for medical treatments). In such cases of older persons who were unable to answer questionnaires, instead, their household representatives participated in the study. However, some questions required to be answered by the older participants (such as self-rated health) were excluded. Given the final response rate of the OP&SHI 2019 was 97.2%, the sample size of the OP&SHI 2019 was 3,049 older persons (those aged 60 and above).
Data was collected through face-to-face interviews. Prior to participating in the interviews, the eligible respondents were informed clearly about the purposes and content of the questionnaire. The interviews were conducted after the eligible respondents signed the informed consents. The ethical approval for the OP&SHI 2019 was issued by the Institutional Review Board of Biomedical Research of the Institute of Social and Medical Studies (ISMS) via Decision No. 01/HDDD-ISMS dated July 12th, 2019. Authors were allowed to use the OP&SHI 2019 data with the permission from the Asian Development Bank (as technical adviser and funder) and ISMS (survey conductor).
Methods
Conceptual framework
Regarding the conceptual framework, this study applied Andersen & Newman’s behavioral model 31 to investigate determinants of healthcare services utilization. The model has been widely adopted in previous literature.32,33
The demand for healthcare utilization of an older individual depends on not only ill health conditions but also multiple socioeconomic factors surrounding that individual, for instance ability to pay for healthcare, health belief, age, gender, healthcare infrastructure.34,35,31 Accordingly, three groups of determinants of healthcare utilization: (i) predisposing factors reflect respondents’ demographic characteristics and health behaviors which have been appeared over a long period of time before that individual experienced ill health conditions, (ii) enabling factors refer to the conditions that facilitate the use of healthcare services, (iii) health need factors reflect health conditions of individuals and refer to the direct factors associated with the use of healthcare services (Figure 1).

Conceptual framework of study.
Measures of variables
Measurement of dependent variables:
The healthcare services utilization was measured by the number of inpatient admissions and outpatient visits of Vietnamese older persons in the past 12 months. Participants were asked two following questions: “During the last 12 months, how many times you were in inpatient care?” and “During the last 12 months, how many times you were in outpatient care?”. The answer to these questions were “0, 1, 2, 3, 4, etc.”. The respondents were considered to access inpatient admissions or outpatient visits if their responses were at least one time of these two types of services. Persons who answered “0” for inpatient admissions or outpatient visits were considered those who did not use healthcare services.
As such, there were four dependent variables: (i) Frequency of inpatient admissions; (ii) Frequency of outpatient visits; (iii) Probability of inpatient admissions; and (iv) Probability of outpatient visits. The first two variables were count variables, while the last two variables were binary variables.
Measurement of explanatory variables:
Following the Andersen & Newman behavioral model, the explanatory variables were classified into three clusters: (i) predisposing variables; (ii) enabling variables; and (iii) health need variables.
All the explanatory variables were treated as categorical variables, with a value 0 as reference groups.
Statistical analysis
The descriptive analyses were presented in frequency, mean, and standard deviation to describe the characteristics of the older people for the full sample and the place of residence-disaggregated sample.
We used Pearson’s chi-square test to examine whether differences in the healthcare services utilization between rural and urban areas and other characteristics were statistically significant. This non-parametric statistic test was widely applied to examine differences between two categorical variables.37 -40 More specifically, Pearson’s chi-square test was employed to analyze differences in dependent variables as well as independent variables among urban and rural older persons.
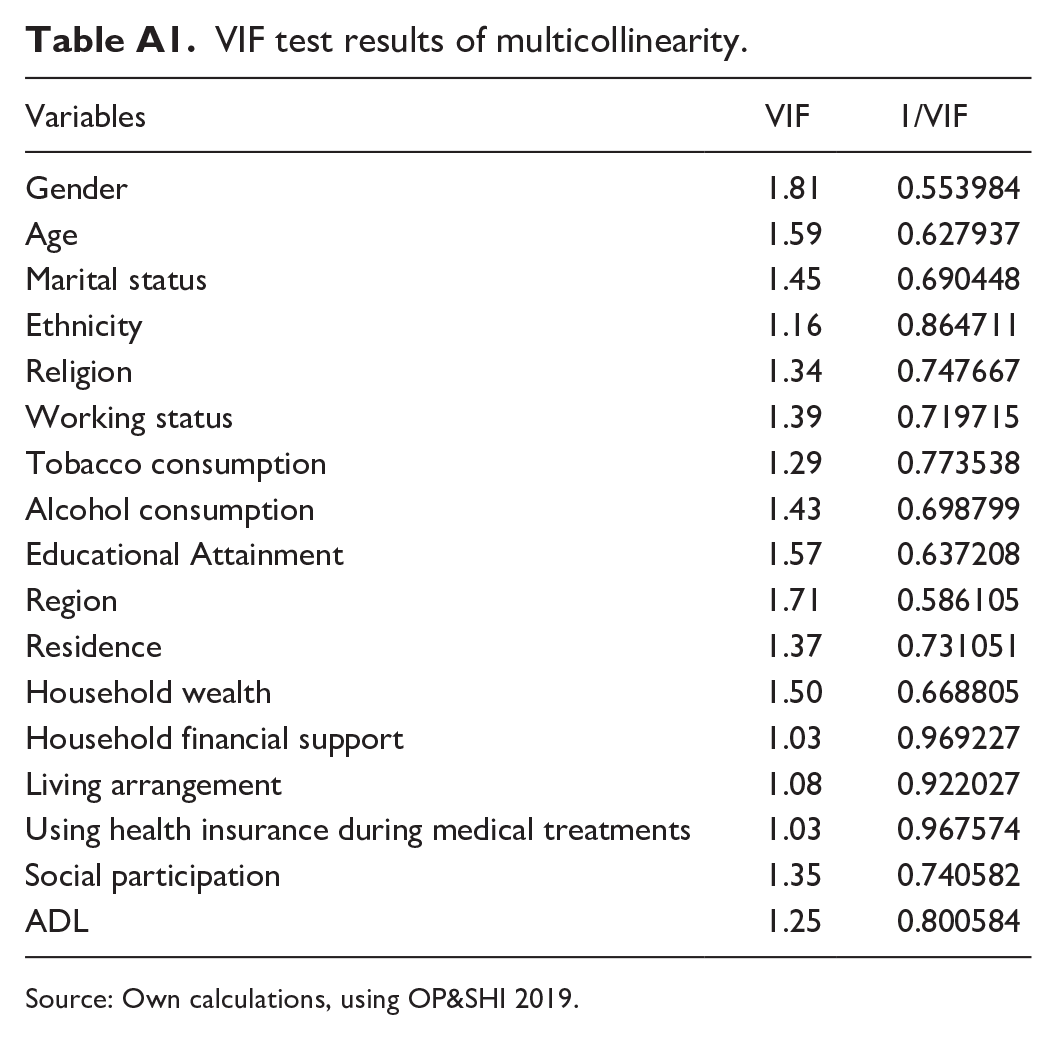
Moreover, to select the final independent variables for the regression models, the variance inflation factor (VIF) statistic was applied to detect the multicollinearity issues among the explanatory variables, and those with VIF values lower than 4 were included in the following analyses. 41
Regression models
Given two of dependent variables were binary outcomes, 42 multivariate logistic regressions were applied to estimate the likelihood of using or not using inpatient or outpatient services. Previous studies on this field also employed this regression model.38,43,44 The multivariate logistic regressions were performed as follows:

In which: p is the probability of an older person using inpatient or outpatient services;
The Poisson regressions were used to examine factors influencing the frequency of inpatient or outpatient services utilization. The Poisson regressions are applied in the case that the dependent variables are count data (only integer, non-negative values).45 -47 The Poisson regressions were performed in the following formula:

In which: f(Y|yi) represents the probability that variable Y takes on a non-negative, integer value yi, and yi! (y! = y.(y - 1).(y - 2). . . . .2.1, with 0!=1) and λ is the parameter of the Poisson distribution. Note that the Poisson distribution has a single parameter (λ) which is unlike the normal distribution with two parameters (i.e. mean and variance).
The Poisson regression model can be written as follows:

In which: y is independently distributed as Poisson random variables with mean λi for each individual, expressed as follows:

In which: exp(BX) (or eXB); B are parameters; and X are independent variables in the model.
Results were presented as regression coefficients and standard errors. A p-value of .05 or less was regarded as statistically significant.
Measures of differences
This research adopted the standard concentration index (CI) and the Erreygers concentration index (EI) for measuring differences. CI has been widely adopted as a measurement of health gap in the previous literature,48 -50 and it was employed in this study for difference analysis. The formula of the CI can be written as follows:

Where:
CI is twice the area between the concentration curve and the line of equality, 51 and its value ranges between −1 and +1 to reflect the degree of difference in healthcare services utilization. When CI equals 0, namely “perfect equality” (or no difference), healthcare services utilization is equally distributed between two groups in comparison. When CI ranges between −1 and 0 (i.e. −1<CI<0), it is indicated that healthcare utilization is more concentrated among the poor. When CI ranges between 0 and 1 (i.e. 0<CI<1), it is indicated that healthcare utilization is more concentrated among the wealthy.
Although the standard CI has numerous properties for measuring health differences, it reveals some limitations that caused biases in the health difference calculations elsewhere. 52 To solve CI’s drawbacks, the Erreygers concentration index (EI), also known as the corrected CI, was used in this paper and could be computed as follows:

Where:
Various studies on health differences have been conducted using the application of EI measurement theory.54 -56 Wagstaff et al. 57 re-emphasized that the original CI reflected the relationship between the health variable and the rank of the living standard variable, not on the living standard variable itself. This study ranked the household wealth index to construct the difference indices. We calculated both CI and EI for health variables and compared the estimates for urban and rural older persons.
Decomposition analysis of socio-economic differences
We adopted the extension of the Oaxaca-Blinder decomposition analysis to quantify the contribution of individual and social determinants to differences in healthcare services utilization between urban and rural older persons. The Oaxaca-Blinder decomposition analysis has been applied to address similar issues in previous literature.33,27,58 In particular, we decomposed the logistic regression models for quantifying factors contributing to the urban-rural differences in the probability of healthcare services utilization. Respectively, we decomposed the Poisson regression models for quantifying factors contributing to the urban-rural differences in the frequency of healthcare services utilization. The extension of the Oaxaca-Blinder decomposition formula could be simplified by:

Where: Y denotes the N x 1 dependent variable vector; X is an N x K matrix of independent variables; and
The difference in Y between group A (rural – comparison group) and B (urban – reference group) could be decomposed as:

Where
Results
Healthcare Services Utilization Among the Vietnamese Older Persons
The weighted results of respondents’ characteristics for full sample, for urban sample, and rural sample are presented in Table 1. On average, 76.91% and 18.39% of older people had at least one outpatient visit or inpatient admission in the past 12 months prior to the survey, respectively. However, the difference in the healthcare service utilization rates between urban and rural older persons was statistically insignificant. About 88% of older persons had no difficulties in ADLs, and no significant differences were observed between urban and rural groups. More than 50% of older persons self-rated their health status as very poor/poor.
Weighted percentages and means of respondents’ characteristics of the Vietnamese older people, by full sample and residence-disaggregated sample.

Note. *Pearson’s chi-square test; sd: standard deviation. Figures in bold indicate coefficients with statistically significant.
Source. Own calculations, using OP&SHI 2019.
p < .05. **p < .01. ***p < .0001.
Some of highlights in descriptive results as follows. As for the predisposing factors, women dominated men (55.18% vs. 44.82%) and the youngest old (aged 60-69) accounting for the largest share of the study sample (58.91%), followed by the middle-old (aged 70-79) (23.48%). Being married was the most common marital status among older Vietnamese people (about 70% in both areas). Regarding employment status, the number of non-employed people was higher than that of employed counterparts in both areas (56.86% vs. 43.14%, respectively). The majority of older persons did not consume alcohol and tobacco at the time of the survey (64.35% and 79.41%, respectively).
Regarding the enabling factors, the difference in household wealth between urban and rural groups was statistically significant. The poorest and the near-poor quintiles of household wealth were disproportionately concentrated among rural residents, while the richest and the near-rich quintiles were highly concentrated among urban residents. Most of respondents (about 90%) received financial supports from their families and the weighted mean in household financial supports in the rural group was statistically significantly higher than that in the urban group. Approximately two-thirds of older persons (66.77%) used health insurance during medical treatments. No statistically significant differences in social participation and using health insurance during medical treatments were observed between urban and rural groups.
Regarding health conditions, Figure 2 reported the weighted percentage of older persons receiving medications in the last 12 months prior to the survey. It shows that those taking medicines for their comorbidities (at least two diseases) accounted for the largest share among all age groups. About 20% of those in the youngest and middle-old groups and nearly 10% of the oldest-old had no medical treatments since they did not suffer from any disease in the last 12 months.

Weighted percentage of the Vietnamese older persons reporting morbidities received medications in the last 12 months by age group.
Factors associated with utilization of healthcare services
Table 2 reports several factors that were associated with the probability and frequency of healthcare services utilization. Interestingly, using health insurance during medical treatments and poor health status had statistically significant association with both probability and frequency of healthcare services utilization.
Factors associated with healthcare services utilization among the Vietnamese older persons.

Note: Multivariate logistic regressions for the probability of using inpatient/outpatient services. Poisson regressions for the frequency of using inpatient/outpatient services.
Source: Own calculations, using OP&SHI 2019.
p < .05. **p < .01. ***p < .0001.
All independent variables included in the following multivariate logistic regression analyses based on the VIF results which were presented in Table A1.
Differences in Healthcare Services Utilization Among Urban and Rural Older Persons
Tables 3 and 4 respectively present the measure of healthcare services utilization differences among Vietnamese older persons by place of residence samples and the full sample. The magnitude of results was relatively small and nearly 0.
Standard concentration index (CI) and Erreygers concentration index (EI) of inpatient utilization among the Vietnamese older persons.

Source. Own calculations, using OP&SHI 2019.
Standard concentration index (CI) and Erreygers concentration index (EI) of outpatient utilization among the Vietnamese older persons.

Source. Own calculations, using OP&SHI 2019.
When considering the economic differences in the healthcare utilization among older persons, findings indicated that both inpatient service utilization and outpatient service utilization were equally distributed across all household wealth quintiles. This pattern of equitable healthcare utilization strongly consistent, regardless older persons resided in urban or rural areas.
The Extension of Oaxaca-Blinder Decomposition Analysis
Decomposition of rural-urban differences in inpatient services utilization
Table 5 shows that the difference in the mean of inpatient admissions between urban and rural older persons was −0.075 (95% CI = −0.193; 0.043) visits, but it is statistically insignificant. Similarly, the difference in the probability of inpatient admissions among rural and urban older people was 0.8% (95% CI = −0.049; 0.066) points, but it is statistically insignificant.
Oaxaca-Blinder decomposition of rural-urban differences in inpatient services utilization among the Vietnamese older people.

Note. Numbers in bold indicate that coefficients are statistically significant.
p < .05. **p < .01. ***p < .0001; Coef indicated Coefficient; S.E: denoted standard error.
Source: Own calculations, using OP&SHI 2019.
Although there was statistical insignificance in overall urban-rural differences, some determinants were reported to contribute to the explained part of the differences. More particularly, gender, region, using health insurance during medical treatments, household wealth, and ADLs were reported to be the statistically significant factors contributing to differences in both frequency and probability of inpatient services utilization. More specifically, using health insurance during medical treatments was the only factor reducing the difference, while being female, living in Central and Southern regions, living in households at 2nd, 3rd and 4th wealth quintile, and suffering from at least one ADL were factors that worsen the difference.
When the rural regression coefficients were substituted for those of the urban regression, no significant contributors to the difference in the “unexplained” component were found.
Decomposition of rural-urban differences in outpatient services utilization
Regarding the frequency of outpatient services, Table 6 shows that older persons living in rural areas had a lower frequency of outpatient visits than those living in urban areas. More particularly, the statistically significant difference in the mean of visits between older persons living in urban and rural areas were −3.033 visits (95% CI = −4.282; −1.783), of which −3.201 visits (95% CI = −4.567; −1.833) (or 105.53% of total differences) were explained by differences between rural and urban in the distribution of social determinants. The remaining 0.168 visits (95% CI = −1.809; 2.144) (or −5.53% of total differences) were explained by unobserved factors.
Oaxaca-Blinder decomposition of rural-urban differences in outpatient services utilization among Vietnamese older people.

Note. Numbers in bold indicate coefficients with statistically significant.
p < .05. **p < .01. ***p < .0001; Coef indicated Coefficient; S.E: denoted standard error.
Source: Own calculations, using OP&SHI 2019.
Similarly, as for the probability of utilization, older persons living in rural areas had a lower probability of outpatient visits than those living in urban areas. More specifically, the statistically significant difference in the probability of visits between older persons living in urban and rural areas were 4.9% (95% CI = −0.084; −0.013) was statistically significant. This difference was explained by characteristic effects by −8.5% (95% CI = −0.117; −0.054) points (or 175.84% of total differences), which was statistically significant. The remaining 3.7% (95% CI = −0.009; 0.083) points (or −75.84% of total differences) were explained by unobserved factors but were not statistically significant.
Gender, region, employment status, social participation, financial support, living arrangements, using health insurance during medical treatments, ADL and SRH contributed to the difference in the frequency and probability of outpatient services utilization among older persons. More specifically, living in Central and Southern areas and using health insurance during medical treatments were two main factors contributing to reduce urban-rural differences, while the other factors worsened the differences.
When the coefficients in regression for rural older persons were substituted into those of regression for urban counterparts, there were no significant contributors to urban-rural differences in the “unexplained” component.
Discussion
To our best knowledge, this study was the first attempt to bridge the knowledge gap concerning urban-rural differences in healthcare services utilization among Vietnamese older population. This study is significantly essential, given Vietnam is a middle-income country experiencing a rapidly aging population. By considering inpatient and outpatient healthcare service utilization of older persons, this study revealed some key findings that need to be informed.
Generally, most of Vietnamese older persons reported using outpatient services (76.91% of older persons, average of 10.49 visits). However, the significantly lower percentage of Vietnamese older persons using inpatient services (18.39% of older persons, average of 2.25 admissions). In this study, the healthcare utilization information was self-reported by older persons when they have to visit medical professionals for diagnoses and treatments. Hence, the scope of this study merely focused on the healthcare utilization raised due to the presence of diseases. Apparently, the higher prevalence of comorbidity, particularly chronic diseases and non-communicable diseases, was observed among Vietnamese older persons in previous studies.33,59 Frequent medical diagnoses and medications for following up and managing the disease severity were explained the findings on healthcare utilization of older persons in this study. 60
When considering the economic differences in the healthcare utilization among older persons, findings indicated that both inpatient and outpatient services utilizations were mostly equally distributed across all household wealth quintiles. This pattern of equitable healthcare utilization strongly consistent, regardless older persons resided in urban or rural areas. The findings implied that the distribution healthcare service utilization was not significantly associated with their household wealth status. One thing to note that the EI and CI analyses were conducted in entire population and by place of residence separately. Differences in healthcare utilization between urban and rural older residents failed to capture within these analyses. Thus, while the inpatient and outpatient service utilization appeared to be mostly evenly distributed, further analyses should explore whether other factors exist which may cause rural-urban differences in healthcare utilization.
In further analyses, the Oaxaca-Blinder decomposition analyses revealed that there were significant rural-urban differences in outpatient services utilization among Vietnamese older persons. Particularly, older adults residing in rural regions had 4.9% lower in the probability of outpatient services utilization than those in urban regions. Similarly, rural residents had 3.033 times lower in the frequency of outpatient services utilization than urban residents. These urban-rural differences were consistent with some previous findings, particularly in China and India.20,61,62,24
The urban-rural differences could be attributable to health system and individual factors. Given the scope of this study focusing on older individuals, it revealed several interesting factors influencing the urban-rural differences, including poor health status and the use of health insurance during medical treatments. Firstly, findings indicated that while poor health status (suffering at least one ADL limitation and very poor/poor SRH) was a health need factor worsening the rural-urban differences, using health insurance during medical treatments was an enabling factor improving urban-rural differences. In other words, very poor/poor SRH or suffering at least one ADL limitation were contributed to widen urban-rural differences in healthcare utilization. In contrast, those using health insurance during medical treatments were found to reduce the urban-rural differences in healthcare utilization.
As people get older, their health needs become more complex, and they may require more medical attention to manage their health conditions. Older persons having at least one difficulty in ADL and very poor/poor SRH were found to worse urban-rural differences. These findings were consistent with some previous literature.32,63 -65 Possible reasons could be: (i) rural older persons tend to face more economic difficulties than their urban counterparts, and as such, rural people find financial barriers in receiving healthcare services; (ii) rural older persons might face with difficulties in travelling to the healthcare facilities due to poor infrastructure and limited transportation modes.
Secondly, the use of health insurance during medical treatments was a crucial factor in reducing urban-rural differences in healthcare services utilization among the older Vietnamese. Given the coverage rate of social health insurance for older persons was about 90.85% in 2020 66 that 66.77% of respondents used health insurance when receiving medical treatments as found in this study apparently implied that, for various reasons, there was a particular proportion of insured older persons not using health insurance for treatments. Previous studies illustrated the importance of health insurance as a third-payer party in improving access to healthcare utilization among older adults.32,61 Older adults were more likely to face financial constraints due to limited income sources from pensions or social security and insufficient retirement savings. Together, the urban-rural gap in employment and income in Vietnam has been investigated elsewhere, 67 and as a result, the healthcare utilization behaviors between urban and rural older adults might be different and the use of health insurance may help to improve the access to healthcare, especially for rural residents. Apparently, the important role of health insurance on mitigating the urban-rural differences in healthcare services utilization was emphasized in previous investigations, especially in rural areas.68,18,69
In Vietnam, health insurance was considered to be the best solution for reducing the financial burden of healthcare utilization among older persons, especially when their income mainly depends on pension fund and family supports. 70 GOV has shifted its concerns to aging field since aging population was alarming in the early 2010s. More particularly, the Health Insurance Law and the Social Insurance Law have been amended in various aspects relating to the older population. For instance, older persons aged 80 and over who do not have monthly pension or monthly social assistance are eligible for receiving social protection benefits and a free-of-charge social health insurance card. The amendment has helped change older persons’ behaviors toward using health insurance in medical examination and treatment services.
The universal health insurance coverage has been implementing with the aim of increasing the health equity, but several issues have been raised. Although the health insurance coverage rate reached about 90.85% of the entire population, 66 numerous medications and medical supplies failed to be covered by health insurance. In addition, the out-of-pocket payment was relatively high (approximately 40% of total health spending) 71 , incurring potentially catastrophic burdens, especially for the older poor. Thus, in the scope of the aging field, health insurance policies related to older persons should be designed more specifically to reduce their out-of-pocket payments when using healthcare services. Some policy recommendations are: (i) achieving 100% of health insurance coverage rate for older persons; (ii) expanding the scope of healthcare services covered by insurance (such as expanding the list of medications and medical supplies frequently used by older persons); (iii) increasing the reimbursement rate for inpatient and/or outpatient services. Expanding the range of health services provided was reported to have a significant impact on reducing inequality in the healthcare services utilization among Korean older people. 72 Addressing the above challenges that older individuals usually face in accessing healthcare services can improve the quality of life of this vulnerable population and promote healthy aging. Maintaining a good health status for older people and thus improving their capacity to work will also be beneficial to other policies such as Social Insurance Law aiming at higher retirement ages for both men and women to actuarially balance the pension fund. 70
This study had some limitations that need to be stated for further improvements. First, the study analyzed evidence based on the total sample population and sub-populations (urban and rural residents), but it is insufficient to observe the comprehensive picture of socioeconomic differences by analyzing only subgroup of residence, meaning that more dimensions in subgroups need to be analyzed. Second, although the database is reliable and representative, it was a cross-sectional data in 2019 so that it was impossible to establish causal relationships between the dependent and independent variables. Third, this study examined the status of possessing social health insurance but failed to report the use of social health insurance while using healthcare utilization. Hence, the results might not reflect the comprehensive picture of social health insurance on mitigating urban-rural differences.
Our findings revealed several policy implications and future research opportunities for addressing the urban-rural differences in healthcare utilization among older adults. Regarding policy implications, developing health insurance schemes supporting the rural older population in accessing healthcare is essential to ensure that they receive benefits equivalent to those of their urban counterparts, particularly for chronic disease management and preventive care. Moreover, GOV should implement subsidies or free-of-charge for low-income rural older persons to minimize out-of-pocket expenses.
This study focused on some individual factors but failed to examine health system-related factors. Hence, for future research directions, studies investigating the choice of healthcare facilities of older persons when they use healthcare utilization are crucial to exploring deeper nuances. It is expected to reveal interesting findings that provide explicit information about the current health system in Vietnam. Regarding the health insurance factor, future information on the reimbursement rates and out-of-pocket payment should be investigated since the capacity to pay for healthcare is an important determinant for understanding the health-seeking behaviors and healthcare utilization among older adults. In terms of study design, this cross-sectional study failed to investigate any causal relationships. Hence, in subsequent studies, available longitudinal data will help address socioeconomic issues in further detail and explore causal relationships in the use of healthcare services among older Vietnamese.
Concluding Remarks
Using the nationally representative data for older Vietnamese persons, this study confirmed the differences in healthcare services utilization among urban and rural older persons. Several important factors were reported to contribute to urban-rural differences. While the poor health status widen the rural-urban differences, the health insurance contributes to reduce the rural-urban differences. Findings are crucial as evidence for continually developing the health insurance scheme and investment to support the rural older population in accessing healthcare. Future research opportunities are proposed to explore deeper comprehensive understanding on this field, including investigations on the choice of healthcare facilities, the reimbursement rates and out-of-pocket payment of older persons when using healthcare services among urban and rural older residents. Also, longitudinal studies are proposed to explore further causal relationships in the use of healthcare services among older Vietnamese.
Footnotes
Appendix
VIF test results of multicollinearity.
| Variables | VIF | 1/VIF |
|---|---|---|
| Gender | 1.81 | 0.553984 |
| Age | 1.59 | 0.627937 |
| Marital status | 1.45 | 0.690448 |
| Ethnicity | 1.16 | 0.864711 |
| Religion | 1.34 | 0.747667 |
| Working status | 1.39 | 0.719715 |
| Tobacco consumption | 1.29 | 0.773538 |
| Alcohol consumption | 1.43 | 0.698799 |
| Educational Attainment | 1.57 | 0.637208 |
| Region | 1.71 | 0.586105 |
| Residence | 1.37 | 0.731051 |
| Household wealth | 1.50 | 0.668805 |
| Household financial support | 1.03 | 0.969227 |
| Living arrangement | 1.08 | 0.922027 |
| Using health insurance during medical treatments | 1.03 | 0.967574 |
| Social participation | 1.35 | 0.740582 |
| ADL | 1.25 | 0.800584 |
Source: Own calculations, using OP&SHI 2019.
Acknowledgements
We would like to thank the Asian Development Bank (ADB) and the Institute of Social and Medical Studies (ISMS) for permitting us to use the data.
Ethical Considerations
Our study did not require an ethical board approval because we used the secondary data, which was ethically approved.
Author Contributions
The study’s concept and design were performed by Long Thanh Giang and Tien Thuy Ngoc Doan. Material preparation was performed by Tien Thuy Ngoc Doan and verified by Long Thanh Giang. Both authors worked on data analyses and the drafts of the research. The final manuscript and its revised versions were read and approved by all authors.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.