
Abstract
The bulk of care for older adults who need assistance but do not require hospitalization or skilled nursing care typically falls to families and friends due to the lack of comprehensive long-term care services for older adults in the United States. To assist with the needs of these key members of the care team who are not typically included in the electronic medical record of the older adult, and to provide them with the care they need to live healthy lives of their own while providing care for an older adult, Caring for Caregivers (C4C) was created by RUSH University System for Health. The goal of the model is to provide information and support for family caregivers due to the extraordinary level of stress they experience, and to do this within a structure that gathers data and addresses the lack of research on caregivers for older adults within health systems. This case study demonstrates the benefits of a customizable model that focuses on What Matters to the caregiver and the care recipient, while adapting to the needs of the staff, the health system, and the community.
For a health system to provide optimal care for older adults, treatment needs to be customized to address their individualized areas of vulnerability. The Institute for Healthcare Improvement and The John A. Hartford Foundation partnered with the American Hospital Association and the Catholic Health Association of the United States to address the typical needs of older adult patients within the health systems through the creation of the Age-Friendly Health System model, composed of four evidence-based elements of high-quality care, known as the “4Ms,” for all older adults: What Matters, Medication, Mentation, and Mobility. A key component of the model is What Matters to the older adult and, of necessity, their family caregivers. As Rani Snyder, MPA, Vice President of Programs at The John A. Hartford Foundation asks, “How can a health system be Age-Friendly if it doesn’t address caregivers?”
Because of the lack of comprehensive long-term care for older adults in the United States, the care for older adults who need assistance outside of facilities typically falls to families and friends. Yet healthcare providers’ assumption that families are ready, willing and able to provide this care without physical, emotional and financial support is a dangerous one for older adult patients and their caregivers. AARP and National Alliance for Caregiving reports that over 41 million Americans are caring for an older adult, performing complex medical tasks without medical training, feeling unprepared and unsupported in their caregiving roles. 1 They further report that caregivers are more likely than non-caregivers to have other disorders, including anxiety disorders and chronic diseases, and that 21% of caregivers view their health as fair or poor. The seminal work by Schreiner et al 2 states that 40% to 70% of caregivers experience clinically significant symptoms of depression, with 25% to 50% of these individuals meeting the criteria for Major Depression. According to the National Academies “Families Caring for an Aging America” report, caregivers are often juggling work obligations while dealing with increasing expenses due to care provision, yet frequently need to cut back on work to provide care, leaving them more financially strapped than ever. They are attempting to address their own physical and mental health needs, maintain social relationships, retain employment and engage in self-care, often while maintaining households that include two or three generations of people needing their time and attention, yet doing so with few supports. 3
To provide these key members of the older adult’s team with the support needed to live healthy lives while providing care for an older adult, Caring for Caregivers (C4C) was created by RUSH University System for Health in 2019. The goal of C4C is to provide information and support for family caregivers, and to gather data and research on caring for caregivers of older adults within health systems. The model was not designed as a randomized control trial, nor as a model requiring fidelity to a particular intervention to test it thoroughly, but rather as a clinical model offering a robust set of interventions with a customized Intervention Plan for support provision. This person-centered approach fits with American Geriatrics Society Expert Panel on Person-Centered Care’s definition of person-centered care, as well as with the values-based approach to supporting the dyad described by Tuzzio et al.4,5
The goals of the C4C model are to identify caregivers in the health system in compliance with the CARE Act (enacted into law in 45 states and territories); to thoroughly understand their unique needs; and to assist them with expanding their care team, addressing individual and family dynamics, and connecting with resources. RUSH staff developed the model based on literature reviews and clinical expertise from staff and consultants, with periodic modifications made in response to research updates and feedback from the C4C National Advisory Council and the C4C Caregiver Advisory Council, both established for this purpose.
Once referred to C4C from any source, including self-referral, the intervention begins with a thorough evidence-based assessment conducted as a “Getting to Know You Meeting” by a clinical member of the C4C team in person, via phone, or through telemedicine. Tools include the Generalized Anxiety Disorder-2/7 (GAD-2/7) testing for symptoms of anxiety, the Patient Health Questionnaire-2/9 (PHQ-2/9) testing for depressive symptoms, the Burden Scale for Family Caregivers—short version (BSFC-s), the BRIEF health literacy scale and RUSH’s Social Determinants of Health (SDOH) scale. All assessment tools may be changed at the discretion of the implementing organization.
Following assessment, an individualized Intervention Plan is created by the caregiver and C4C clinician. The interventions are based on What Matters to and the values of the dyad, and may include any or all of the following:
Skill-Building Meetings are conducted by nurses, physical or occupational therapists, dietitians, social workers, pharmacists, and/or other professionals using checklists to identify needs, with intervention length and type determined by the service provider. The focus of these meetings is to increase confidence in care provision and to learn to provide any physical care needed without incurring injury to the caregiver or care recipient.
Planning for What Matters Sessions are brief psychotherapy sessions conducted by a designated clinician in one to five sessions, depending on caregiver need. These sessions are held with the caregiver and, when appropriate, the care recipient, and begin with a biopsychosocial/spiritual assessment of the caregiver. Content of the sessions may include reducing stressors, improving communication with each other and with the care team, addressing unresolved family conflicts, expanding the family care team, and planning for the future, including advance care planning. Clinicians utilize family systems theory in addressing caregiver needs, and each session is based on What Matters to both the caregiver and care recipient. A detailed Planning for What Matters Sessions manual was developed as a resource when providing individual sessions, or as an outline for session content when providing the sessions in groups.
Care Team Planning Meetings are conducted with the caregiver and care recipient dyad and the care recipient’s health care team, both internal and external. These meetings focus on What Matters to the care recipient, the caregiver, and the dyad to develop person-centered care goals, and to coordinate the roles of each person involved to support those goals. Medication coordination among all providers and deprescribing as needed is an important part of these meetings.
Figure 1 depicts the components of the Caring for Caregivers model and the flow from referral to assessment, intervention, reassessments within follow-up conversations 1- and 3-months (or other pre-determined times) post-completion of C4C, and referrals for services and/or back into C4C at any point, regardless of care recipient location.

Caring for caregiver model flow diagram.
The ability to customize the intervention to address the unique needs of each participant is a clinical benefit for the dyad. C4C has gathered data that demonstrates its impact on both caregivers and care recipients. The clinical outcomes for caregivers of C4C involvement at RUSH are depicted in Figure 2. Statistically significant reductions in caregiver symptoms associated with depression, anxiety and caregiver burden were seen 1- and 3-months post-intervention.
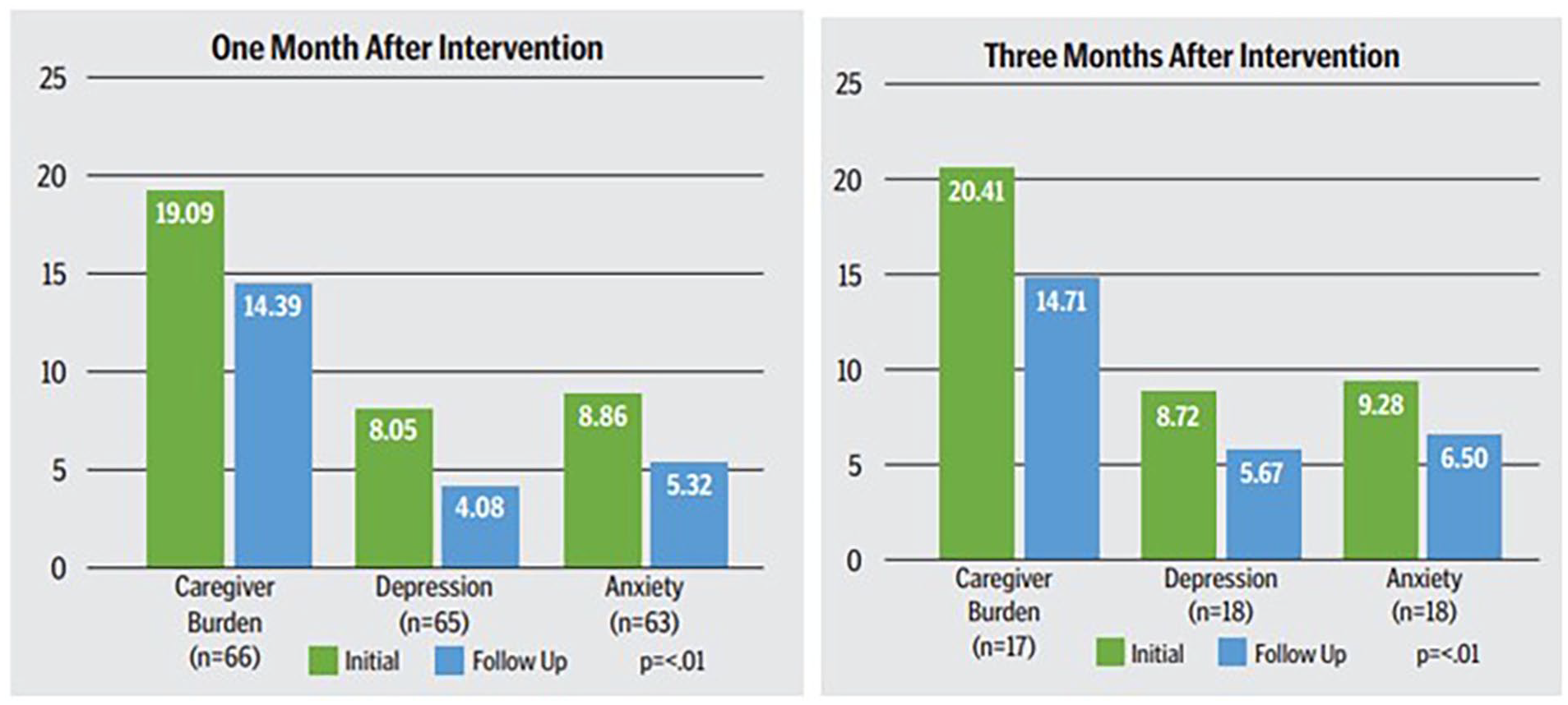
Clinical outcomes for caregivers.
The preliminary associational data for care recipients whose caregivers received C4C interventions were also explored by looking at number of inpatient stays, length of stay and Emergency Department visits during the 6 months prior to the 6 months after caregiver completion of C4C (n = 169). The reductions are not meant to imply causality, yet the fact that they represent over 50% drops in number of inpatient admissions, length of stay and number of ED visits is notable. These outcomes are of particular interest to health system administrators due to financial penalties for overage. The preliminary data are depicted in Figure 3.

Clinical outcomes for care recipients.
National Spread
In 2021, C4C staff within the Department of Social Work and Community Health at RUSH received an 18-month planning grant from The John A. Hartford Foundation to refine, scale and test the model for nationwide spread in collaboration with the Institute for Healthcare Improvement.
The model was beta tested in six health systems and feedback was gathered and analyzed to determine what adaptations were required to best fit the needs of Age-Friendly Health Systems, Area Agencies on Aging, and other health-oriented organizations in urban, suburban and rural settings with diverse patient populations. Again, the flexibility of the program was attractive given each setting’s unique staffing, site, organizational, community and patient needs. An additional 3 year grant in 2022 from The John A. Hartford Foundation allowed staff to work with interested organizations to understand the model and explore how to best operationalize it in their health systems. Implementation within health systems has begun, with technical assistance from C4C staff.
Customization, Adaptations, and Sustainability
Billing for services, underway at RUSH since the first year of operation, was a key consideration in C4C development. Sustainability is discussed with interested health systems, and various options are considered based on their unique patient populations and internal structures. Options have included incorporating C4C into a clinic’s customary service line, billing insurance using psychotherapy billing codes, securing external funding, and/or allowing health systems to contract with community providers to provide and bill for any C4C services that the health system does not provide. Funding opportunities have recently arisen out of the new Centers for Medicare and Medicaid Services caregiver services billing codes, and their Guiding an Improved Dementia Experience (GUIDE) Model. Providing C4C using these caregiver services is discussed with interested health systems as well.
Additionally, stemming from the needs of rural settings with few or no psychotherapists available, the provision of the model in groups offered by health department professionals with strong program delivery and mental health backgrounds in conjunction with wellness and self-care programming is an option that is being implemented. The flexibility of the model and its ability to meet community needs is an unusual strength allowing for nimble execution of appropriate adaptations.
Lessons Learned
Flexibility in the caregiver services offered through C4C has been seen as a key component of the model since its design. The value of its flexibility with respect to the needs of staff, department, health system, patient population, and community, state and federal government is also highlighted as it is shared nationally. The ability to customize the intervention thus includes environmental factors surrounding the dyad, including historical and cultural aspects of care provision in a variety of settings. The distinctive qualities of each dyad’s community plays a significant role in how C4C may be delivered and caregivers assisted most efficiently and effectively.
However, there are challenges for health systems regarding implementation including their ability to take on new services at a time when budgets are tight and staff caseloads are full. Administrators’ ability to understand the advantages to their patients and their budgets for adopting C4C will determine their willingness to prioritize implementation.
Next Steps
C4C is spreading awareness of the importance of caregiver support throughout the country in Age-Friendly Health Systems, Area Agencies on Aging, and community health-oriented organizations, and is assisting them with their implementation needs. Learning Communities were established to coordinate technical support and new learnings, and to connect providers to learn from each other’s implementation experiences. Updates about billing using new CMS codes and the GUIDE Model are included in each meeting. Adaptations made to C4C based on research, expert input, and health systems’ needs are also included.
An important next step will be to expand health system and community organization education on the value of customizable programming for caregivers. With more complex care provided at home through the Hospital at Home movement, the GUIDE Model, and the new CMS billing codes for caregiver training, support for caregivers of older adults is increasingly in the spotlight and payment options expanding.
As caregiver research demonstrates, caring for caregivers is complex and must move beyond a “one size fits all” approach to be optimally effective. Implementing adaptable treatment is needed to address the complex needs of caregivers. Treatment needs to be truly person-centered, incorporating the voices of our patients, health systems and communities, and reflecting our values as professionals.
Footnotes
Acknowledgements
We would like to thank The John A. Hartford Foundation and RRF Foundation for Aging for their generous support.
Data Availability Statement
Subject to appropriate ethical and legal considerations, the author(s) may share data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project has received funding from RRF Foundation for Aging and from The John A. Hartford Foundation.
Ethical Approval and Informed Consent Statements
Ethical approval was not required.