
Abstract
Research suggests that the quality of care provided by family members may be influenced by the quality of relationship they have with the person living with dementia. The study investigated this in the context of assisting with daily activities. The quality of the relationship was assessed using the conceptual framework of relationship continuity/discontinuity which focuses on whether the carer experiences their relationship as continuous or discontinuous with the pre-dementia relationship. Thirty spousal carers completed the Birmingham Relationship Continuity Measure. Participants were also interviewed about how they provide care for their partner’s daily activities. Passages consistent with a more person-centered approach were identified, and the total number of these in each transcript was used as the measure of care quality. There was a significant correlation between questionnaire scores and the number of person-centered passages: Those reporting greater continuity more frequently described using a person-centered approach. Findings were consistent with earlier research suggesting associations between the quality of the relationship and the quality of care. The concept of relationship continuity suggests ways in which relationship and care quality are connected, and these suggestions could be used to develop interventions to help family carers provide better care.
Plain language summary
Previous research has suggested that the quality of care that family members give to a person with dementia is influenced by the quality of their relationship. For example, family carers who describe having a poor relationship with the person they are looking after, are more likely to exclude them from making decisions and more likely to engage in psychological and physical abuse.
This study looked at whether relationship quality may be connected with how well family carers help with routine activities of daily life, such as getting dressed and preparing food.
To measure the quality of the relationship, we used a questionnaire called the Birmingham Relationship Continuity Measure. This asks questions about whether the carer feels like they have the same relationship and feelings towards the person with dementia or they feel like the relationship and their feelings are now very different.
To measure care quality, participants were interviewed about how they helped their family member with routine activities of daily life. We rated these interviews in terms of how often the approach was in line with the principles of person-centred care. Person-centred care is an approach to dementia care in which the carer treats the person with dementia with respect, tries to understand how the person is feeling, considers the person as an individual with their own needs and wishes, and creates a positive and supportive atmosphere.
Thirty spouses who cared for someone with dementia took part. Those who reported a sense of continuity in their relationship more often reported care practices that were in line with person-centre care.
It is important to help couples maintain a good relationship when living with dementia. A good relationship is a source of many benefits. Along with other research, this study suggests one of those benefits may be the quality of care.
Introduction
There has been relatively little investigation of the quality of care provided by family members to people living with dementia.1-3 The issue merits more attention. Most dementia care is provided by family members. 4 Relatively high rates of psychological and physical abuse have been self-reported by family carers, and this suggests that the quality of the care often falls below a satisfactory level. 5 Evidence from paid carers indicates that the provision of better-quality care benefits the well-being of both the care-receiver and the carer.6,7
One aspect of this issue is why some family carers provide better care than others. Much of the research about this has focused on variables associated with abuse. Characteristics of the carer associated with a greater likelihood of abuse from the carer toward the person living with dementia include a greater sense of burden, low mood, poor coping, and low levels of support, with mixed evidence relating to the gender and age of the carer. 5 Another topic that has received some attention is the extent to which the carer involves the person living with dementia in decisions. Less involvement is associated with the carer experiencing low mood, being less educated, and being younger, with, again, mixed findings in relation to gender. 8 A few studies have focused on variability across a broader range of positive aspects of care quality, drawing explicitly on the construct of person-centered care. In a quantitative study, McClendon and Smyth 3 reported that certain personality traits (agreeableness, openness, neuroticism, and conscientiousness) were associated with more person-centered care, whereas extraversion, avoidant coping, and low mood were associated with less person-centered care.
As well as investigating characteristics of the carer, some of these studies have also reported an association between quality of care and the relationship. Compared to spouses, son, or daughter carers are more likely to abuse the person living with dementia or exclude them from decision-making.5,8 The quality of the relationship between the carer and the person living with dementia has also been found to be relevant. A poor pre-dementia and/or poor current relationship are quantitatively associated with a higher risk of the carer abusing the person with dementia 5 and excluding them from decision-making. 9 In a qualitative study, Smebye and Kirkevold 10 suggested that the promotion of personhood (a central tenet of person-centered care) was associated with close emotional bonds within the relationship, whereas the diminishment of personhood was associated with a poor pre-dementia relationship, current resentment toward the care receiver, and a task-focused relationship.
Some other qualitative studies, incorporating an evaluation of the relationship using the concept of relationship continuity, have similarly suggested a link between the quality of care and the quality of the relationship. This concept focuses specifically on the experience of the spouse/partner (as opposed to other family carers), and is a description of a range of closely connected ways in which they experience relationship changes.11-13 In relationship discontinuity, the person living with dementia is perceived as very different and disconnected from their pre-dementia self; the relationship feels like one between a caregiver and a care-receiver, rather than a marriage/partnership; and the emotional warmth and bonds are diminished. In relationship continuity, despite the changes that are occurring, the relationship and the person living with dementia are experienced as a continuation of what was in place before the onset of dementia. Some qualitative studies have suggested that perceptions of discontinuity are associated with a more controlling and restrictive style of caring, and a less individualized understanding of the partner11,14,15; whereas perceptions of continuity are associated with a more tolerant and empathic response that seeks to understand the situation from the individual perspective of the partner.15,16
The extent to which findings from qualitative studies can be generalized is limited, and quantitative methods can provide useful complementary support. In a mixed methods study, Riley et al 17 reported a significant correlation between scores on a questionnaire measure of relationship continuity and spousal carer accounts of how they made sense of, and tried to manage, challenging care needs (eg, aggression, repetitive questions). Participants whose scores suggested an experience of discontinuity provided relatively narrow and impersonal explanations that characterized the needs and behavior as symptoms of dementia. By contrast, participants who reported greater continuity provided more elaborate and person-centered explanations that incorporated the perspective of the person living with dementia and made use of the participant’s knowledge of that person as an individual. Those reporting discontinuity also reported more restrictive and controlling management practices that were likely to upset the other person and took less account of their individual needs and wishes.
The aim of the present study was to extend this earlier study by investigating the connection between relationship continuity and quality of care in a different care context (providing support for activities of daily living), and by asking spousal carers about their actual care practices rather than their understanding of their partner’s needs. Activities of daily living were chosen as the focus for the study because, although it is the care activity most frequently engaged in, there has been relatively little investigation of how person-centered that care is, with previous research focusing mainly on decision-making 8 and responses to challenging care needs. 17 It was hypothesized that those reporting a greater degree of relationship continuity would show a more person-centered approach in the care they provided for activities of daily living.
Method
The STROBE 18 reporting checklist for cross-sectional studies was completing in preparing this paper. This paper reports the quantitative findings from a larger observational mixed-methods study. For the study, participants were interviewed about their care practice in relation to activities of daily living. The interviews were coded in relation to their person-centered qualities in both a qualitative and a quantitative way, and the quantitative codes were correlated with scores on a questionnaire of relationship quality. Only the method and analysis relevant to the quantitative testing of the hypothesis are described in this paper. The qualitative aims and findings will be reported elsewhere. Data collection took place in 2022.
Participants
The sample was self-selected. Participants were recruited through Join Dementia Research, which is an online service provided by the National Institute for Health and Care Research in the UK that allows those living with dementia and their families to register an interest in taking part in dementia research. People on the register were notified of the study and asked if they wanted to participate.
To be considered eligible to participate, the carer needed to be the spouse or partner of someone with a diagnosis of dementia and to be currently providing help to this person for activities of daily living. To ensure that there was a substantial pre-dementia relationship in relation to which they could experience continuity or discontinuity, they were required to have lived together for at least 5 years before the onset of dementia. Carers were not eligible to participate if they had any learning disability, major mental health disorder, or other condition that may have impacted on their ability to have a meaningful conversation about their caring role; if their command of English was insufficient to take part in such a conversation; or if they had provided substantial care to the person with dementia prior to the onset of dementia for some other condition.
Power analysis was used to establish a satisfactory sample size. The hypothesis was to be tested using correlation analysis. Power analysis was conducted using G*Power. 19 For a two-tailed test and an alpha level of .05, with power set at 0.80, the analysis indicated that a sample of 26 would be required for the detection of a large correlation (.5). Accordingly, a sample of at least 26 participants was targeted.
Procedure
Due to the risks associated with carrying out face-to-face interviews during the COVID-19 pandemic, participants were interviewed via an online platform or a phone call, depending on their preference. Interviews took between 30 and 90 min, and were audio-recorded and transcribed. After completion of the interview, the participants completed a questionnaire evaluating relationship continuity.
Prior to the interview, participants were asked to identify some activities of daily living in which their partner was still engaged but for which they needed some supervision or support from the participant. In the main part of the interview, the participant was asked to describe in detail how these tasks were carried out, what support or supervision they provided to their partner during these tasks, why they provided support in that way, and what challenges there were to providing the support in that way. Participants were also asked about what assistance they provided for a range of other activities of daily living, and what guidance and support they had received about providing care.
Measures
To provide a measure of relationship continuity, participants completed the Birmingham Relationship Continuity Measure. 12 This contains 23 items, possible scores range from 23 to 115, and higher scores indicating a greater sense of continuity. Items address whether the relationship is no longer experienced as a marriage/partnership, whether the person living with dementia is perceived as radically changed as a person, whether feelings toward the person living with dementia have changed, whether the sense of couplehood and togetherness has been lost, and whether there is a sense of loss for the pre-dementia relationship. In the initial evaluation study, 12 the questionnaire showed good internal reliability (.95) and test-retest reliability (.93), and good construct validity in relation to other questionnaires addressing aspects of the relationship in dementia.
The measure of how person-centered participants were in their care was provided by coding passages in each interview according to whether they were more person-centered or less person-centered, and then, for each participant, summing the number of more person-centered and the number of less person-centered passages. Thus, for each participant, there was a more person-centered total and a less person-centered total.
The VIPS conceptualization of person-centered care 20 was used to decide whether a passage in the interview was relevant to person-centered care, and whether the passage showed a more person-centered or a less person-centered approach. This conceptualization has 4 components relating to the provision of care:
Valuing: Carers should value, respect, and promote the personhood of the care recipient, including their autonomy and agency. Valuing is also about treating the care recipient with respect and in ways that everyone expects to be treated. In the present context, valuing was evident in the efforts of participants to maintain some degree of independence and control for their partner in relation to the activities of daily living, minimizing the assistance provided, giving choices, and keeping the person informed and involved. A less person-centered approach was evident in the opposite of these, such as taking over task completion unnecessarily or restricting choice.
Individual: Carers should treat the care recipient as an individual with a unique personal history and personality, and with their own wishes, values, and goals. In the present context, this was evident when participants prioritized their partner’s involvement in activities that were perceived to be important and meaningful to the partner.
Perspective: Carers should try to understand situations from the perspective of the care recipient, and act in accordance with that understanding. In the present context, this was evident when participants showed an understanding of why the partner was finding the task cognitively challenging and made appropriate adjustments. It was also evident in their efforts to understand the emotional response of their partner to the situation and to respond with empathy.
Social: Carers should create a positive and supportive social environment in which the care recipient feels valued and appreciated. In the present context, this was evident in efforts to avoid the partner feeling embarrassed or upset by their difficulties in completing tasks, in the provision of encouragement, and in otherwise creating a positive social context for task completion. Less person-centered responses were shown in abrupt commands, criticism, arguments, and losing one’s temper with the partner.
The less person-centered total provided a less satisfactory measure than the more person-centered total. Although there were some clear descriptions of a less person-centered approach in the valuing and social domains, more often the interview suggested that the participant took a less person-centered approach because of the absence of positive examples of a person-centered approach. In the individual and perspective domains, it was almost exclusively the absence of examples of a person-centered approach that suggested a poorer quality of care. It was difficult to incorporate absence of a person-centered approach into the less person-centered total in a meaningful way. Although the correlations with this total are reported in the analysis, it was expected that a fairer test of the hypothesis would be provided by the more person-centered total.
Framework analysis was used to code the interview data. The main advantages of this approach for the present study were that it allows codes to be based on prior research and conceptualizations, as well as generating codes from the data itself; it is more appropriate for qualitative research seeking answers to specific research questions (as opposed to a more open-ended exploration of a topic); and it is suitable for the analysis of larger data sets. 21 Following the guidance for applying framework analysis, 21 an initial framework of codes was established using the VIPS framework. Using this initial framework, the first 3 transcripts were then coded by the first and third author. Points of disagreement were discussed and resolved. Subcodes for each VIPS domain were inductively established, indicating how a more (or less) person-centered approach was manifest within the domain. Full details of the coding system are provided in the accompanying paper that reports on the qualitative aims and findings for the study. As an example, one of the subcodes for the valuing domain concerned the degree of assistance provided. A passage from the interview that was coded as more person-centered described how the participant stood back during the activity and encouraged the person living with dementia to ask for help if they needed it; a passage that was coded as less person-centered described how the participant had taken over all the food preparation for meals because the person living with dementia was taking too long.
To evaluate the reliability of the coding, the first and third authors independently coded 10 transcripts. The first author highlighted passages in the transcript judged to contain material that was more (or less) person-centered. Highlighting indicated where each passage began and ended. Both authors then coded the passage in terms of which of the 4 VIPS categories it related to, with the possibility that the same passage could relate to more than 1 category. Both authors also rated each coding in terms of whether the approach was more person-centered or less person-centered. Overall, 178 passages were highlighted. In 28 passages, one of the authors had used more codes than the other author. Because of the lack of a clear solution for dealing with this issue, these passages were excluded from the calculation of inter-rater reliability. For the coding of the passages in terms of a VIPS category, Cohen’s kappa was .80, and for the rating of whether it was more person-centered or less person-centered, it was 0.91. A value of 0.8 or above indicates strong agreement. 22
Data Analysis
The data were screened prior to analysis, using published recommendations. 23 Variables were first inspected for univariate and multivariate outliers. One participant was a univariate outlier on the more person-centered total and also a multivariate outlier for the correlation between this total and the Birmingham Relationship Continuity Measure (BRCM) total, scoring very highly on the more person-centered total but in the lower half of scores on the BRCM. This individual had a qualification in a caring profession, had received training in the concept of person-centered care, and had applied it in their professional practice. They were judged to be unusual in this respect, relative to the rest of the sample, and were therefore excluded from the rest of the analysis. Kurtosis and skew statistics, along with plots, were assessed to evaluate whether the variables were normally distributed. Bivariate scatterplots were inspected to evaluate homoscedasticity and whether there was any non-linear relationship between variables. The distributions of the BRCM and the more person-centered total did not depart significantly from normality. The scatterplot indicated homoscedasticity and no non-linear relationship, and so it was deemed appropriate to evaluate this relationship using parametric correlation. For the less person-centered total, there was a floor effect with a bunching of values at the lower end: Half the participants scored 5 or less on this variable, and all but 2 scored 10 or below. Parametric correlation was carried out for this variable, but it should be interpreted with caution.
Results
The sample consisted of 30 people, 10 men and 20 women, in a heterosexual relationship with the person living with dementia. Ages ranged from 56 to 88 (mean = 73, median = 72). With one exception, all identified as White British. The length of time they had lived together ranged from 11 to 64 years (mean = 38, median = 42). Information was also obtained about the dementia. The length of time since diagnosis ranged from 1 to 9 years (mean = 3, median = 3), although many had been providing care for some time before an official diagnosis was given. Alzheimer’s disease was the most common form of dementia (19 cases), followed by vascular dementia (5) and mixed dementia (5), with one case being “dementia not otherwise specified.” Most of the participants lived at home with their partner but, in 3 cases, the partner now lived in a nursing home. These participants did still assist with activities of daily living during their visits.
Table 1 shows the descriptive statistics for the variables and Table 2 shows the correlations. Those who more frequently made comments evidencing a more person-centered approach scored significantly higher on the BRCM. The frequency of less person-centered comments was not correlated with either the BRCM or the more person-centered total.
Descriptive Statistics.

Note. BRCM = Birmingham Relationship Continuity Measure; More PC total = more person-centered total; Less PC total = less person-centered total.
Correlations.
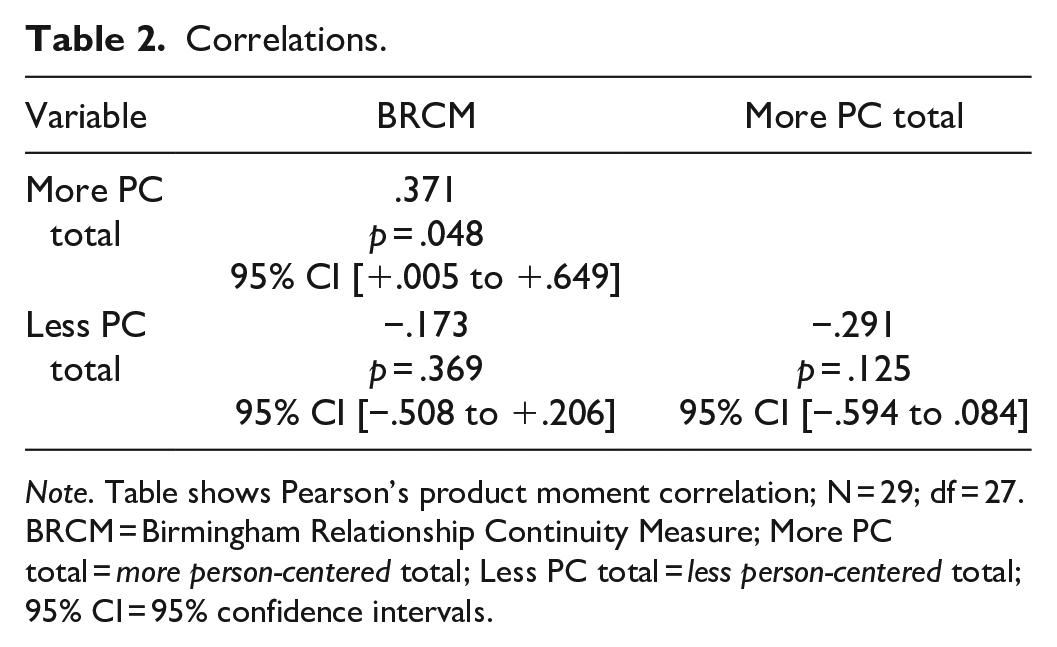
Note. Table shows Pearson’s product moment correlation; N = 29; df = 27.
BRCM = Birmingham Relationship Continuity Measure; More PC total = more person-centered total; Less PC total = less person-centered total; 95% CI = 95% confidence intervals.
Discussion
The results provided some support for the hypothesis in that better quality relationships were associated with more frequent descriptions of a person-centered approach to the provision of support for activities of daily living. The quality of the relationship was not significantly correlated with the frequency of less person-centered descriptions. The floor effect evident on the less person-centered variable reduced the possibility of obtaining any significant correlation. Moreover, as suggested earlier, it was expected that this variable would provide a less fair test of the hypothesis because it included only positive examples of less person-centered practices and failed to capture the absence of more person-centered practices in the participant’s account. In the individual and perspective domains, it was these absences that suggested that the participant was less person-centered in their approach.
The finding of an association between relationship continuity and the quality of care is consistent with previous studies suggesting that poorer quality relationships are associated with a higher risk of abuse 5 ; excluding the partner from decision-making 9 ; a more controlling and restrictive style of caring10,11,14,15; and a less individualized and less person-centered understanding of the partner.11,14,15,17 This link between the quality of care and the quality of the relationship is predictable from the perspective of person-centered care. In his original development of the concept, Kitwood drew inspiration from the work of Carl Rogers on the therapeutic relationship and conceptualized person-centered care in terms of the quality of the personal relationship between the carer and the person with dementia. 24 Indeed, many have argued that the relational aspect of person-centered care should be made the primary focus, and that care should be “relationship-centered” rather than “person-centered.” 25
The concept of relationship continuity can be used to generate some ideas about why there is this association between quality of care and quality of the relationship, ideas that can be investigated in future research. One example relates to using previously acquired knowledge about the partner. When the carer experiences continuity (ie, the partner and the relationship are continuations of what has gone before), presumably they will carry on making use of their extensive knowledge of their partner and their relationship to make sense of their situation. This may help their sensitivity to what might upset their partner about the completion of activities of daily living and to signs that the partner is getting upset; it may help them be more effective in creating a positive social context for task completion; and it may guide them in selecting what activities to prioritize because of their importance to their partner. By contrast, in discontinuity the person with dementia and the relationship no longer feel the same and these longstanding ways of understanding the person may seem less relevant. The carer is faced with the task of constructing a new identity for the person with dementia and finding new ways of understanding them. This may lead to uncertainty and/or reliance on a more generic understanding of how people are affected by dementia obtained from services, media or published materials. 17 A related idea is that continuity in the way in which the couple interact with one another may help create a positive social context for the completion of tasks. For example, findings by Hickman et al 26 highlighted humor as a way in which the continuity of relationships is sustained. The continued use of humor during completion of tasks may help create a positive social context. Another potential explanation of the link between the relationship and the quality of care concerns the loss of emotional closeness and sense of partnership that characterizes discontinuity. It is possible that this loss decreases the empathy generated by difficulties, reduces the motivation to protect from distress and maintain a positive social context during activities of daily living. Instead, the carer may experience their partner’s involvement in activities of daily living as burdensome and may be critical of their actions. 27 More generally, there is evidence of an association between discontinuity in the relationship and a sense of burden, resentment, and a less tolerant response to the partner’s difficulties.15,16,28 By contrast, the experience of continuity is associated with finding the act of caring more satisfying and rewarding. 28
This study has several limitations. First, the sample was not representative of the wider population of spouse/partner carers. The sample was almost exclusively White British, and exclusively heterosexual. Although a formal measure was not taken of the severity of dementia or the degree of support provided by the participants to their partners, information gathered in the interviews suggested that relatively few of the partners were in the more severe stages of dementia. Previous research has noted that the characteristics and relational dynamics of providing care and assistance change as cognitive impairment increases. 29 Second, the sample was self-selected from an online voluntary research register. This may have been associated with a bias in the sample—for example, those with a greater interest in providing better quality care may have been more likely to take part. Third, the data relied on self-report. Previous research has suggested discrepancies between self-report and observational measures in this context. 30 A study using observational measures of both the quality of the relationship and the quality of care would be a useful way forward. This may also offer a way of addressing the difficulties created by the unsatisfactory nature of the measure of less person-centered care used in this study. Finally, the study was not experimental. The correlation between relationship continuity and person-centered care may have arisen because of their relationship to other confounding variables rather than because relationship continuity has the hypothesized impact on the delivery of care. For example, it may be that both are related to the severity of the dementia. When the dementia is more severe, it may be more difficult for the carer both to experience continuity in the relationship and to provide more person-centered care.
Some family carers need guidance to help them deliver good quality care. Previous research suggests that the quality of care can fall short of a satisfactory standard5,31 and family carers themselves have also expressed a wish for more guidance. 32 As noted in the Introduction, the quality of family care in the context of the activities of daily living is a relatively under-researched area. Findings from the present study suggest that some carers also need support in delivering good quality care for these activities: There was wide variation across participants in terms of the frequency of examples of more person-centered practices and some accounts contained several instances of a less person-centered approach (Table 1).
Relatively few existing family interventions focus on improving the quality of care. 2 The present study suggests that future development of interventions with this focus should address the role of the relationship, and ideas about this role suggested by the concept of relationship continuity could be used to shape those interventions. For example, following on from the earlier consideration of the links between relationship continuity and the quality of care, carers could be encouraged to make more use of the pre-dementia ways of understanding the care receiver, rather than generic ways of understanding people living with dementia obtained from other sources. This might enable them to provide more person-centered care that is based on treating them as a unique person with their own personality and motivations (the individual domain) and on a better understanding of their responses to situations (perspective).
Conclusion
The quality of care provided by family members is a relatively under-researched area. Evidence suggests that this care can sometimes fall below optimum standards. The present study suggests this is also the case with support provided for activities of daily living. Consistent with earlier research, the study also found an association between the quality of the relationship and the quality of care. Although further research is needed to establish this, it may be that improving the quality of the relationship will lead to improvements in the quality of care.
Supplemental Material
sj-docx-1-inq-10.1177_00469580241307798 – Supplemental material for The Association Between the Quality of Care Provided by Family Members and the Quality of Their Relationship With the Care Receiver in Dementia: A Mixed-methods Observational Study
Supplemental material, sj-docx-1-inq-10.1177_00469580241307798 for The Association Between the Quality of Care Provided by Family Members and the Quality of Their Relationship With the Care Receiver in Dementia: A Mixed-methods Observational Study by Chiara Carparelli, Jan R. Oyebode and Gerard A. Riley in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Author Contributions
Carparelli was involved in preparations and planning for the study, recruitment and data collection, analysis and interpretation. Oyebode was involved in preparations and planning for the study, analysis and interpretation. Riley was involved in preparations and planning for the study, analysis and interpretation. Riley took the lead in writing up the study, but all authors read, provided feedback, and approved the manuscript.
Data Availability
Carparelli, Oyebode, Riley 459 AS-PhD-18-012, Mendeley Data, V1, doi: 10.17632/5tn53kfckf.1.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by The Alzheimer’s Society, United Kingdom, under Grant 459 AS-PhD-18-012.
Ethical Considerations
Ethical approval was provided on 4.3.2022 by the STEM research ethics committee at the University of Birmingham, UK, reference ERN_18-1795C.
Consent to Participate
Participants provided verbal consent that was fully informed and audio-recorded.
Consent for Publication
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.