
Abstract
Maintaining health cannot be achieved individually; it is influenced by social, legal, and institutional factors surrounding the individuals. This study aimed to identify regional-level factors that may influence the occurrence of chronic diseases among people with disabilities. To achieve this, we conducted a Delphi survey with experts to identify a set of regional indicators required for studying the health status of people with disabilities, particularly for predicting the occurrence of chronic diseases. Through the process of the Delphi survey, 24 indicators were finally selected. The major categories of the indicators were demographic factors (4 indicators), health behaviors (6 indicators), healthcare resources and utilization (11 indicators), and local community policies (3 indicators). Each category and subcategory of indicators plays a crucial role in understanding and improving the health and well-being of people with disabilities at the regional level. By addressing these factors comprehensively, policymakers and healthcare providers can develop more effective and targeted interventions, ultimately fostering a more inclusive and supportive environment for people with disabilities. The findings underscore the importance of a holistic approach to health assessment and the need for continued monitoring and evaluation to inform policy and practice.
Keywords
People with disabilities face a higher burden of chronic diseases due to limited access to healthcare and socioeconomic barriers.
Regional disparities significantly impact health outcomes, but studies on targeted interventions to reduce inequitable access to healthcare services for people with disabilities are still sparse.
Community-level factors, including healthcare resources and local policies, are critical yet under-researched in addressing health inequities.
Introduces 24 validated regional-level indicators to assess health outcomes for people with disabilities.
Employs a modified Delphi method to ensure a multidisciplinary and consensus-driven approach.
Bridges gaps in disability-focused public health research by providing actionable data for regional analysis.
Supports the development of region-specific health interventions to address disparities and improve health equity.
Provides policymakers with a framework to allocate resources and design inclusive health policies.
Introduction
To address health management issues, improve accessibility to healthcare services, and prevent secondary conditions for people with disabilities, systematic data collection and analysis related to the occurrence and prevention of comorbidities and secondary conditions among people with disabilities are required. 1 People with disabilities are at high risk for chronic diseases due to their disability itself, susceptibility to poverty, and limited access to healthcare services. 2 Among individuals with disabilities aged 19 and older, 84.8% have at least 1 chronic disease, with an average of 2.5 conditions per person, indicating the need for a broad approach that addresses multiple chronic diseases rather than focusing on a single condition. Also, for those aged 30 and above, the prevalence of chronic diseases is notably higher than in the general population. Hypertension affects 52.9% of individuals with disabilities, compared to 34.8% in the general population, while diabetes affects 26.8%, compared to 14.8%, indicating a disproportionate burden of chronic conditions. 3
People with disabilities also face limited access to healthcare services, leading to negative effects on achieving their optimal health outcomes. Studies on targeted interventions to reduce the inequitable access to healthcare services for people with disabilities are still sparse. 4 Meeting their needs and maintaining health require locally-driven approach, including social, legal, and institutional factors surrounding the individuals. For example, legislation, regulations, and policies are crucial in obtaining relevant health knowledge, improving participation in decision-making, and promoting healthy behaviors among people with disabilities.2,5 Societal, economic, and environmental infrastructures such as transportation, cost coverage, and healthcare resources are another factors for people with disability to facilitate chronic diseases management. 5 Therefore, the European Commission declared the European Disability Strategy 2021-2030 to empower persons with disabilities for equal opportunity and equal access. 6 In Korea, since implementing the Act on Guarantee of Rights to Health and Medical Services for Persons with Disabilities in 2017, regional health and medical centers for persons with disabilities were launched to improve their access to healthcare at the local level. 7 Nevertheless, in South Korea, there have been differences in the prevalence of chronic diseases among people with disabilities depending on their place of residence. As of 2021, the prevalence was 87.6% in large cities and 90.6% in rural areas, indicating a disparity based on the region.
Internationally, various studies have recognized the importance of regional-level data for understanding health disparities at community levels. For instance, the European Core Health Indicators (ECHI) and Eurostat provide health-related data at the level of large geographic regions (e.g., Northern, Southern, and Eastern regions) or counties and municipalities, enabling regional analysis of healthcare access and health disparities for people with disabilities across the EU.8,9 Similarly, in the United States, the County Health Rankings Model and the SHARE-NW initiative (Solutions in Health Analytics for Rural Equity across the Northwest) focus on making county-level health data accessible, helping local health agencies identify underlying social determinants of health.10,11
Despite these efforts, there remains a gap in research focusing specifically on regional-level factors affecting the health of people with disabilities, especially concerning chronic disease risk. And there are only a few studies on the determinants of health for people with disabilities at the community level compared to the ones for people without disabilities.4,12 Therefore, this study aimed to identify regional-level factors that may influence the occurrence of chronic diseases among people with disabilities. Given the limited prior research on regional-level indicators specific to chronic diseases among individuals with disabilities, this study employed the Delphi method to systematically gather expert insights. The Delphi approach is suitable for studies aiming to establish consensus in areas where empirical frameworks are sparse, thus supporting the development of foundational indicators for this underserved population. We reviewed relevant conceptual frameworks and indicators to select regional-level variables. Then, Delphi surveys were conducted among panel experts to select a set of regional-level indicators essential for research on the health of people with disabilities.
Methods
Study Design
We used a RAND/UCLA-modified Delphi Panel method, which integrates evidence review with expert consensus processes to select regional-level variables related to the health of people with disabilities. 13 Initially developed for military decision-making, the Delphi method is a structured and iterative group communication process employed to generate evidence or make decisions amidst uncertainty and incomplete information. It entails administering a series of anonymous questionnaires to a select group of experts, known as Delphi panelists, who provide responses based on their expertise and personal experience.14,15 It uses a series of rounds where experts independently evaluate and refine their responses to reach a consensus. The procedure in this study comprises five steps: (1) literature review; (2) formation of a multidisciplinary panel; (3) round 1 Delphi; and (4) round 2 Delphi (Figure 1). The two rounds of the Delphi surveys were conducted from September 3rd, 2022, to October 27th, 2022.

Delphi study flowchart.
Step 1: Literature Review (Identify Candidate Indicators)
A comprehensive review of frameworks, including the World Health Organization’s (WHO) social determinants of health, the County Health Rankings Model, and databases from the Korea Disease Control and Prevention Agency (KCDA), was conducted to develop initial indicators.11,16 -18 The County Health Rankings Model provides actionable data and evidence for local communities to improve health outcomes and reduce disparities. It emphasizes the influence of social factors—such as education, income, housing, and community power—on health outcomes, aiming to empower communities to set priorities, make decisions, and implement equitable policies. The researchers compared lists of publicly available data from the KDCA’s database and Statistics Korea with the County Health Rankings Model to construct an initial framework and pool of regional-level indicators. Indicators were evaluated considering (1) data availability (able to obtain data at the city, county, and district levels), (2) potential impact on health outcome, (3) possibility of improvement through advancing the capability of communities), and (4) ease of interpretation. As a result, five major categories (demographic and economic factors, physical environments, health behaviors, healthcare resources, and utilization, local community policies), 13 subcategories, and 42 indicators were derived (Table 1). The indicators’ units of measurement were at the city, county, and district levels.
Initial Major and Subcategories and Indicators for Delphi Surveys.
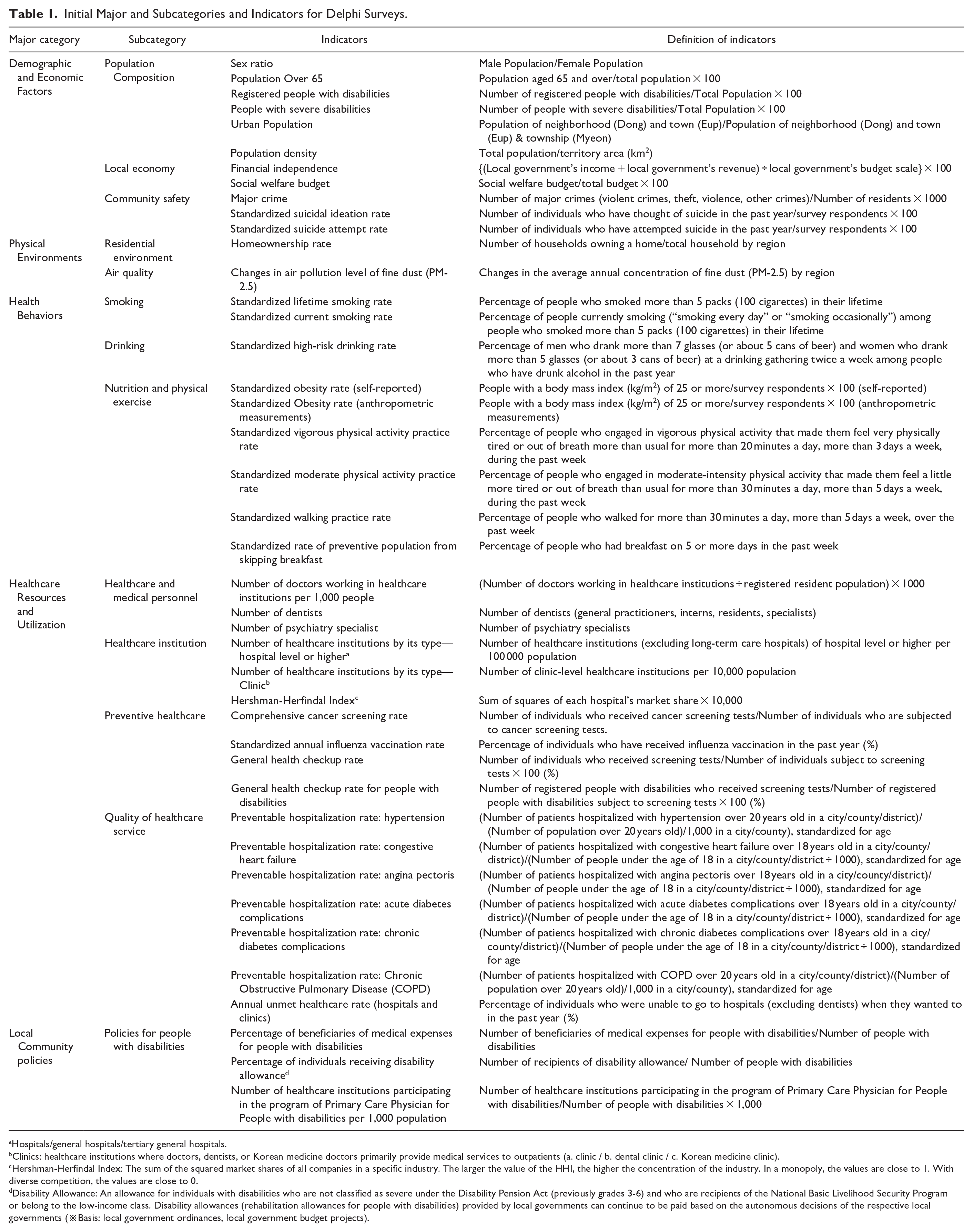
Hospitals/general hospitals/tertiary general hospitals.
Clinics: healthcare institutions where doctors, dentists, or Korean medicine doctors primarily provide medical services to outpatients (a. clinic / b. dental clinic / c. Korean medicine clinic).
Hershman-Herfindal Index: The sum of the squared market shares of all companies in a specific industry. The larger the value of the HHI, the higher the concentration of the industry. In a monopoly, the values are close to 1. With diverse competition, the values are close to 0.
Disability Allowance: An allowance for individuals with disabilities who are not classified as severe under the Disability Pension Act (previously grades 3-6) and who are recipients of the National Basic Livelihood Security Program or belong to the low-income class. Disability allowances (rehabilitation allowances for people with disabilities) provided by local governments can continue to be paid based on the autonomous decisions of the respective local governments (※Basis: local government ordinances, local government budget projects).
Step2: Forming a Multidisciplinary Panel (Recruit Multidisciplinary Experts)
A purposive sampling method was used to recruit a multidisciplinary panel of experts. The panel of experts in this research consisted of researchers from academia whose expertise in public health statistics, epidemiology, and research methodology, government offices related to policies related to people with disabilities, members of academic societies, such as the Public Health Administration Society, healthcare professionals, and people with disabilities. Invitations were sent via email, explaining the study and inviting participation. The adequate number of panelists in a modified Delphi study varies depending on the study’s specific objectives, the topic complexity, and the desired level of consensus. 19 Previous studies suggest that the quality and commitment of panelists are more important than the number of participants.19,20 Given the lack of a clear standard for the panel size in Delphi studies, we aimed for a target of around 30 experts, considering previous studies on public health in Korea.21,22 Considering the commonly high attrition rate in Delphi studies, surveys were sent to 43 experts, and out of these, 26 completed both rounds of the survey with signed informed consent.
Step 3. Round 1 Delphi (Initial Rating of Indicators, Deriving Consensus on 42 Indicators)
In the first Delphi round, panelists were presented with 42 indicators to evaluate their overall importance, validity, timeliness, possibility of improvement through community capability, and data availability. Each criterion was rated on a 5-point scale (1 = Very low, 5 = Very high). This round allowed panelists to provide additional qualitative feedback on each indicator and suggest other indicators they deemed relevant. The results from this round helped refine and clarify the initial indicator set.
Step 4. Round 2 Delphi (Refinement and Consensus)
In the second round, panelists were given a summary of results from Round 1, including the mean, standard deviation, mode of each indicator, and any qualitative feedback from their peers. They were asked to evaluate the indicator considering this feedback. The objective of this round was to refine the indicator set further and achieve a higher level of consensus on each item. Indicators meeting a predetermined consensus threshold were retained, while others were either modified or excluded based on the group’s input. This round provided the final set of regional indicators, reaching a consensus suitable for regional-level health assessments.
Statistical Methods
In the first round of the Delphi survey, indicators with an average score below 3.3 and a Content Validity Ratio (CVR) value below 0 were excluded. The CVR measures the degree of consensus among panelists on the importance of each indicator relative to what would be expected by chance. 23 A CVR threshold of 0 was chosen due to the sample size of approximately 30 panelists, as this threshold helps distinguish indicators with weak consensus without overly restricting the indicator set. 24 The CVR was calculated based on the frequency of panelists rating the indicators as “very high” (5 points) or “high” (4 points) on a 5-point scale. 25
In the second round, we calculated the sum, mean, standard deviation, and CVR for each item. According to Ayre and Scally, 26 a CVR threshold of 0.8 was recommended for expert panels of at least 10 members. Therefore, 2 researchers assessed and excluded, indicators with a CVR below 0.8. 27
Ethical Approval
This study was approved by the Institutional Review Board of Korea National Open University (KNOU) (IRB No. ABN01-202207-13-V1). All participants provided informed consent before participating in the Delphi survey.
Results
Profile and Characteristics of the Expert Panel
The expert panel comprised 26 professionals with specialized knowledge in various fields: 5 in rehabilitation medicine (19.2%), 6 in public health (23.1%), 5 in social welfare (19.2%), 6 in nursing/medicine/pharmacy (23.1%), 2 in special education (7.7%), 1 in medical statistics (3.8%), and 1 in occupational therapy (3.8%) (Table 2). This Delphi survey was conducted over 2 rounds from September 3 to October 27, 2022.
Characteristics of Study Participants.

Delphi Survey Results
Through the first round of the survey, 3 indicators (population density, number of major crimes per 1000 people, Huffman-Huffman index) with a mean score below 3.3 and a Content Validity Ratio (CVR) below 0 were excluded.
In the second round, the survey was conducted with the remaining 38 indicators. Items with CVR values less than 0.8 were reviewed and removed by 2 researchers’ decisions after the discussion.
Selection of Final Indicators
This study conducted 2 Delphi surveys based on the initial indicators and then selected the major and sub-categories and final indicators based on the collected results (Table 3). The final indicators consist of 4 major categories (demographic and economic factors: 4 indicators, health behaviors: 6 indicators, healthcare resources and utilization: 11 indicators, and community policies: 3 indicators), 10 sub-categories, and 24 individual indicators. The subcategory of community safety and the major physical environment category (residential environment, atmosphere) were not included in the final indicator set.
Number of Selected Indicators During the Process of Delphi and Final Indicators.

Additional Feedback From the Panel Experts
Additional feedback was provided on the indicators. Experts recommended splitting the budget for social welfare into medical and healthcare-related funding. Related to the physical environment, experts emphasized the accessibility of roads and buildings by wheelchairs for people with disabilities or having enough green areas such as public parks as significant indicators. Regarding healthcare and medical personnel, the experts recommended that the indicators be more specific by narrowing them down to specialists or primary care physicians with expertise in disabilities. Regarding the indicator of the number of healthcare institutions, the experts mentioned it should be more specific, such as those designed and equipped to be more disability friendly. For example, people with hearing or speaking disabilities need access to healthcare institutions with communication support. However, data related to these indicators were not available for collection.
Discussion
In this study, we aimed to select regional-level variables necessary for researching chronic diseases among people with disabilities. As one of the first studies to develop regional-level indicators for chronic diseases among individuals with disabilities, this research serves as foundational work, providing a structured basis for future studies to build upon. The Delphi method was instrumental in achieving this foundational framework, as it allowed us to integrate expert insights systematically in the absence of existing regional health indicators for this population. Through the process of the Delphi survey, 24 indicators were finally selected. The major categories of the indicators were demographic and economic factors (4 indicators), health behaviors (6 indicators), healthcare resources and utilization (11 indicators), and local community policies (3 indicators).
Demographic Factors
Demographic factors such as age and the population of people with disabilities are basic indicators related to chronic disease among people with disabilities. According to the results of the 2023 survey on people with disabilities, the proportion of older adults 65 years old is 54.3%, an increase compared to 49.9% in the 2020 survey, showing a continuous aging trend. 28 Also, understanding the distribution of registered people with disabilities by region is essential to examine chronic disease among people with disabilities. Therefore, it is important to note that the number of unregistered people is omitted from the indicator values, which may lead to an underestimation of the most vulnerable and remoted people with disabilities.
Health Behaviors
In our study, 6 variables within the health behavior category were identified: current smoking rate, high-risk drinking rate among annual drinkers, self-reported obesity rate, measured obesity rate, moderate physical activity rate, and walking practice rate. These variables indicate that a community’s health behaviors can significantly impact the chronic disease outcomes of individuals with disabilities. Research has shown a direct relationship between smoking, alcohol consumption, and chronic diseases in individuals with disabilities. A study by Sarmiento et al 29 examined smoking and heavy drinking among adults with disabilities using the 2020 NHIS data, finding that adults with disabilities had higher smoking rates (23.5% vs 11.2%) and similar heavy drinking rates (5.3% vs 7.4%) compared to those without disabilities. A study by Kerr et al identified a need for more tailored support for behavior changes in tobacco and alcohol use among individuals with mild to moderate intellectual disabilities, although the rates of drinking and smoking in this group are similar to those in the general population. 30
Obesity and physical inactivity are also critical issues for individuals with disabilities. People with disabilities were found to have more obesity problems and were less likely to engage in physical activities 31 Ryan et al identified a strong link between overweight/obesity and chronic health conditions in older individuals with intellectual disabilities, emphasizing the need for prioritizing weight management in this population. 32 In Korea, Lee et al reported that from 2008 to 2017, individuals with disabilities had higher odds of both obesity and underweight, with severe and mental disabilities showing the highest obesity rates. 33
Medical Resources and Utilization
Healthcare resources and their utilization are vital for managing the health of individuals with disabilities. Eleven indicators in this category reflect the availability and accessibility of healthcare services, including the number of medical professionals, dental professionals, and various healthcare institutions. Effective healthcare utilization ensures that individuals receive timely and appropriate care, which is crucial for managing chronic conditions and improving overall health outcomes. 34
Interestingly, access to dental care emerged as an important indicator of the health and well-being of people with disabilities. In the US, significant challenges were reported in providing oral health care to individuals with intellectual or physical disabilities. It was reported that 32.6% of individuals in households experiencing disabilities had not visited a dentist in 2 or more years compared to 19.7% in households not experiencing disability, while they were more likely to visit an emergency room for dental care or pain (9.0% for those with disability vs 3.1% for those without disability). 35 A survey study on dentists found that barriers across different healthcare system levels affect individuals with disabilities. 36 These barriers include healthcare costs, untrained healthcare workforces, issues of inclusive and coordinated service delivery, societal stigma, and health literacy, emphasizing the critical role of tailored healthcare services in improving oral health outcomes among disabled populations. 36 The Korean government has tried to improve dental care for people with disabilities by establishing specialized dental care centers since 2011. 37 By 2021, one central center and 13 regional centers had been established, offering specialized care and fee reductions for low-income patients, thereby increasing access to dental services for people with disabilities. 38 However, these facilities remain insufficient, with wait times for procedures under general anesthesia extending up to 5 months. Despite fee reductions, the high cost of many non-covered dental procedures remains a significant barrier.
The number of medical institutions by type, particularly clinics, reflects the accessibility of primary healthcare services. Clinics are often the first point of contact for individuals seeking medical attention. Effective healthcare utilization ensures that individuals receive timely and appropriate care, crucial for managing chronic conditions and improving overall health outcomes. 39 The rates of integrated cancer screening, annual influenza vaccination, general health checkups, and health checkups for people with disabilities can be meaningful indicators because screening tests are vital for early detection and prevention of diseases. However, a previous study showed that women with disability are 30% less likely to receive breast cancer screening services, and mortality from breast cancer is as “highly statistically significant” compared with women without disabilities. 40
Preventable hospitalization rates for hypertension, acute complications of diabetes, and Chronic Obstructive Pulmonary Disease (COPD) are all relevant to examining chronic disease among people with disabilities. 41 Many studies suggested a strong relationship between effective primary care and hospitalization due to ambulatory care-sensitive conditions (ACSCs).42 -44 Additionally, the annual rate of unmet healthcare needs reflects the accessibility and quality of healthcare services. According to the 2020 Survey on People with Disabilities, about one-third of people with disabilities expressed unmet healthcare needs, which means that they could not receive appropriate healthcare services when needed. The main reason for not receiving healthcare was primarily due to difficulty in mobility to the clinic and economic burden. 45
Local Community Policies
Four indicators in this category focus on policies designed to assist people with disabilities, such as the proportion of local governments’ social welfare budgets, individuals receiving disability medical benefits and allowances, and the number of healthcare institutions participating in the program of Primary Care Physicians for People with Disabilities. The proportion of local governments’ social welfare budgets reflects their capacity to provide essential services and benefits to people with disabilities. A higher proportion indicates a stronger safety net, which can mitigate some of the socioeconomic disadvantages faced by people with disabilities. 46
According to a study evaluating the effectiveness of pilot projects for healthcare institutions participating in the Primary Care Physician for People with Disabilities program, people with disabilities who face mobility challenges were highly satisfied with visiting medical treatment. 47 However, low system awareness, financial burdens, and insufficient professional services such as rehabilitation were reported as barriers to access. Moreover, healthcare providers faced challenges in participating in these systems due to concerns about financial viability, including expected profitability and labor costs associated with home visiting treatments. 47
This study excluded all indicators corresponding to the major physical environment category. The indicators related to community safety, such as the number of major crimes per 1000 population, were not considered as a direct factor influencing chronic disease among people with disabilities. Indicators related to mental health, such as standardized suicide ideation rate and standardized suicide attempt rate, were considered as one of the chronic diseases, not as an independent variable. Indicators, such as trends in fine dust (PM-2.5) air pollution levels, were evaluated as less important when comparing its impact by region.
One of the strengths of this study is the construction of the indicator pool considering the availability, responsiveness, and improbability at the city, county, and district levels. Particularly, for the availability of indicators, the feasibility of data acquisition was considered, and indicators at the city, county, and district levels were included in the final set of data obtainable from the Database of Community Health-Related Factors published by the KDCA. Providing foundational data on variables to consider when formulating policies for the health of people with disabilities at the local level will be meaningful.
Practical Implication
This study provides healthcare researchers with a comprehensive set of regional-level indicators for assessing chronic disease risks among individuals with disabilities. These indicators offer policy makers valuable tools to evaluate health outcomes and design tailored interventions that address specific needs of people with disabilities, ultimately fostering more effective health policies for chronic conditions. Additionally, the selected indicators in each dimension help prioritize healthcare programs by accounting for regional factors supporting improved access and health outcomes for people with disabilities.
However, this study has several limitations. While the Delphi method is useful for eliciting expert opinions and achieving consensus, it poses potential sample selection bias, panel member attrition, and the subjective nature of expert opinions. However, efforts were made to mitigate these limitations through rigorous panel selection criteria, clear communication protocols, and transparent data analysis procedures. In some variables, there is a possibility that there may be little variation in values at the cities, counties, and district levels, and some variables may even be calculated as “0” (e.g., the number of medical institutions participating in the Primary Care for People with Disability program). Nonetheless, given the high value attributed to local community policies by the panel, we retained the policy-related variables even if they exhibited low-variation. Such variables might be analyzed by applying measures of relative values between regions, such as quintiles. Although the Delphi method provides valuable expert consensus, it does not incorporate external validation beyond the panelists involved. Future studies could consider incorporating external validation methods to further enhance research credibility. This study could not consider the specific types of disabilities. Future studies need to consider different types of disabilities (e.g., hearing/speaking, mobility, mental, etc.), as the nature of the disability and challenges related to managing health and accessing healthcare services vary among people with disabilities. While the number of healthcare professionals and medical institutions were included in this study, we could not fully consider more detailed accessibility to healthcare services experienced by people with disabilities. For example, there may not be many clinics where wheelchairs are accessible or with doctors and nurses with deep understanding and knowledge of disabilities. Therefore, it is necessary to consider these practical accessibility challenges faced by individuals with disabilities when developing indicators.
Conclusions
This study identified 24 key regional-level indicators for understanding and addressing chronic diseases among people with disabilities. Using a RAND/UCLA-modified Delphi Panel method, we categorized these indicators into demographic factors, health behaviors, healthcare resources and utilization, and local community policies. Each category and subcategory of indicators plays a crucial role in understanding and improving the health and well-being of people with disabilities at the regional level. By addressing these factors comprehensively, policymakers and healthcare providers can develop more effective and targeted interventions, ultimately fostering a more inclusive and supportive environment for people with disabilities.
Footnotes
Acknowledgements
The earlier version of this study was presented at the Korean association of health economics and policy conference in May 19, 2023.
Author’s Note
So-Youn Park is now affiliated to Inha University Hospital, Jung-gu, Incheon, Republic of Korea.
Authors’ Contributions
YJ, BJ, JM, and SP made substantial contributions to the study design and data collection; SP and BJ drafted the manuscript, and SP, BJ, YJ, JM, and SP substantively revised it. All the authors revised the manuscript critically for intellectual content, have read and approved the final manuscript, and have agreed both to be personally accountable for their contributions and to ensure that questions related to the accuracy or integrity of any part of the work.
Data Availability Statement
Data used during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI21C2122). The KHIDI had no role in the design of the study, data collection, analysis, or interpretation, nor in writing the manuscript.
Ethical Approval and Informed Consent Statements
This study was approved by the Institutional Review Board of Korea National Open University (KNOU) (IRB No. ABN01-202207-13-V1). All participants provided informed consent before participating in the Delphi survey.
Short Article Summary
Health is influenced by social, legal, and institutional factors, not just individual actions. This study identified 24 regional indicators, including demographics, health behaviors, healthcare resources, and community policies, to help predict chronic diseases in people with disabilities and guide effective interventions.