
Abstract
As housing prices in China continue to escalate and the limitations of the “personal unlimited liability system” for housing loans become more evident, the financial stress on families has significantly increased. This stress not only impacts the physical and mental health of family members but also results in rising health care costs. This paper presents empirical research examining how housing stress influences changes in household health care costs through a panel data analysis. The study is based on the China Family Panel Study (CFPS) database and employs a panel two-way fixed effect model alongside a mediating effect model to examine the impact of housing stress, family income, and health status on health care costs. The findings reveal a significant positive correlation between housing stress and health care costs; specifically, for every 1% point increase in housing stress, health care costs rise by 0.141. Robustness tests and propensity score matching (PSM) further validate these findings, even after addressing endogeneity issues. Mediation effect analysis indicates that for every 1% point increase in housing stress, household disposable income decreases by 1.749, and health status declines by 0.468, thereby increasing household health care costs. Heterogeneity analysis demonstrates that housing stress has a more pronounced impact on health care costs among western, eastern, urban, and rental households. The government should implement various measures, such as promoting a “personal limited liability system” mortgage policy, reducing housing prices, and ensuring equal rights to rent and purchase, to alleviate housing stress, enhance family income, and improve residents’ health status. These actions would contribute to the promotion of both the housing market and medical care, supporting the sustainable development of the health care sector and ultimately improving long-term social welfare.
Introduction
Addressing the increasing stress of rising medical costs is a significant global issue. Studies indicate that the financial burden of healthcare expenses frequently surpasses the economic growth rate of a nation, with health insurance costs constituting up to 20% of total medical expenditures. 1 This research delves into the correlation between costs by utilizing extensive data and empirical analysis to investigate the potential influence of housing stress on health care costs.
It is crucial to differentiate between the concepts of “Housing pressure” and “Housing stress.” 'Housing pressure’ primarily denotes the tangible physical strain imposed by housing costs and demand, which can be quantified and is often represented by the proportion of housing expenditures. Conversely, “Housing stress” highlights the psychological and emotional strain associated with housing-related issues, such as worries about housing conditions or anxieties regarding future stability. This concept encompasses the capacity to endure external pressures, extending beyond mere physical strain. Given its broader implications, this article will concentrate on the concept of 'Housing stress.’
In recent decades, land finance has been a driving force behind China’s urbanization, significantly contributing to local government revenue and urban infrastructure development. However, the overheating of the real estate market due to land finance and urbanization has led to a range of social, livelihood, and ecological challenges,2,3 which remain unresolved. The rapid growth of China’s real estate market has led to an increase in housing expenses, resulting in more households facing a “housing cost burden” where they spend over one-third of their income on rent and utilities. 4 The escalating housing prices have placed significant stress on ordinary individuals, impacting not only their economic well-being by restricting the consumption of daily necessities but also affecting their physical and mental health.5,6 Housing stress has been recognized as a critical social determinant of various health issues.7,8 A growing body of research supports the correlation between housing affordability and health problems.9 -12 As housing prices continue to soar and the limitations of the “personal unlimited liability system”13,14 for housing loans become more evident, the challenges facing Chinese cities have evolved from purely economic concerns to issues that directly impact people’s livelihoods. 15 Concurrently, the health care industry is contending with rising costs that often outstrip a country’s economic growth, consuming a significant portion of the gross domestic product. The parallels between these 2 evolving issues are noteworthy and merit further investigation. However, the direct correlation between housing stress and health care costs, while seemingly logical, remains relatively underexplored in the current research.11,12 In this context, our research holds significant value. Utilizing data from the China Family Tracking Survey (CFPS), this study examines the impact of housing stress on residents’ health care costs. Due to significant housing stress potentially diminishing family income and adversely impacting the health status of family members, which in turn affects health care costs, this article draws upon relevant research literature.12,16,17 Consequently, it utilizes household disposable income and the health status of the household head as mediating variables in the relationship between housing stress and health care costs, constructing a mediating effect model for analysis (as illustrated in Figure 1). Our findings not only expand existing knowledge but also offer insights for policy development to mitigate housing stress and enhance health care costs. This study aims to address 2 primary research questions: First, does housing stress have a significant impact on health care costs? Second, what strategies can be identified to mitigate this relationship and subsequently reduce health care costs?

Graphical representation of conceptual framework.
Literature Review
Research on Housing Stress
The literature on the causes of housing stress in China and its impact on various aspects of individual life is extensive and varied. It is crucial for research to delve into understanding the root causes of housing stress and its influence on the health care costs strategies adopted by individuals.
Housing stress encompasses various challenges related to housing, including instability, unaffordability, eviction, and homelessness.18,19 In China, 3 main factors contribute to housing stress. Firstly, the impact of land policy plays a crucial role, with land supply being a key determinant 20 In China, since land ownership belongs to the government or village collective rather than individuals or families, land-use rights are restricted, leading to significant stress on ordinary people to purchase homes in urban areas with concentrated high-quality resources.21,22 Furthermore, local governments monopolize core revenue and land disposal due to their ultimate land ownership, obtaining funds for urban development through “land public finance,” land mortgage loans, local government financial platforms, urban investment bonds, and other financial instruments (LGFV), which generate substantial income for the government and officials23,24 and result in the implementation of numerous “face projects.” 25 Secondly, the impact of “school district housing” is significant, as access to high-quality educational resources is closely linked to rising housing prices.26 -28 Individuals often accept high mortgages or rents to ensure their children have access to quality education in expensive housing areas. Thirdly, the stress to own a home is driven by the desire to marry, particularly in China where homeownership is often seen as a prerequisite for marriage. 29 Research indicates that men are more inclined to marry if their parents own valuable homes, especially in rural regions. 30 Lastly, China’s “personal unlimited liability system” has significant implications. When a home buyer is unable to continue repaying a bank mortgage, and the proceeds from the auction of the house fall short of covering the loan, the debtor is responsible for the remaining balance. This form of unlimited liability effectively binds numerous mortgage buyers to the bank. Consequently, the "personal unlimited liability system" places many loan buyers in challenging life circumstances, subjecting them to both physical and mental distress, highlighting the severe housing stress they face.
In summary, factors such as “school district housing,” marriage requirements, land policy, and others contribute to elevated housing prices. Additionally, the “personal unlimited liability system” for housing loans has consistently resulted in lenders being susceptible to exploitation. Collectively, these elements exacerbate housing stress and heighten the risk of chronic diseases. Furthermore, housing booms may lead to unexpected health repercussions. 31
At the intersection of housing and health, a study examining the health of homeless Canadians found that homelessness was associated with increased levels of disease, despite a causal link between homelessness and poor health. 32 Research on the link between housing stress and the mental health of migrants indicates that residents of informal housing tend to experience higher levels of perceived stress and poorer mental health. 33 Comparing post-industrial countries with different structures, such as Australia and the UK, researchers have explored the impact of tenure on the link between housing affordability and health. Their findings suggest that rising housing costs and unstable housing conditions can negatively affect mental health, leading to greater harm to individuals and their families. 9 Interestingly, some studies have shown that rising housing prices have a positive impact on residents’ mental health but a negative impact on physical health, with the most significant adverse effects observed in individuals without housing. 34
Housing stress can have various negative consequences, impacting the quality of life and subjective well-being of urban residents. 35 This delay in marriage, influenced by rising housing costs, has also led to a decrease in fertility intentions and actual fertility rates. 36 Disparities between urban and rural populations in China have been exacerbated by urbanization and industrialization, where local governments acquire farmland at low prices and lease it to real estate developers at higher market rates. Consequently, displaced farmers often migrate to urban areas for employment, facing high housing costs as a result. 37
While research on housing stress is abundant, there is a notable absence of studies delving into the correlation between housing stress and health care costs. This gap in the current literature necessitates further exploration, prompting our study to utilize data from the CFPS Phase III panel database to explore the impact of housing stress on health care costs. Through a rigorous empirical methodology, our goal is to offer a thorough insight into these seemingly disparate domains, contributing to discussions on urban development, public health planning, and socioeconomic policy.
Previous Research on Health Care Costs
Research on health care costs has primarily focused on financial forecasting for public health care institutions, particularly in terms of managing health care costs.
The issue of rising health care costs is a significant concern in many developed countries, at times surpassing economic growth rates. To tackle this challenge, developed nations are leveraging Internet of Things (IOT) technology to implement healthcare monitoring applications (HMA), particularly in the healthcare sector, with the aim of lowering healthcare expenses. 38 Digital remote monitoring technology offers promising solutions to these challenges. 39 A study investigated digital supply chains and their impact on hospital costs through the implementation of an enterprise resource planning (ERP) system, utilizing structural equation modeling (SEM) data gathered from 107 Greek public hospitals. The analysis indicates that maximizing digitalization and system functionality can effectively reduce medical costs. 40
Developing countries like China also grapple with the issue of “difficult and expensive medical treatment,” specifically concerning high medical costs. The unequal distribution of medical resources and underutilization of primary healthcare facilities are key obstacles hindering China’s ongoing medical reforms. To promote visits to primary healthcare institutions, China introduced the hierarchical medical system (HMS) in 2015. 41 Feng Jun’s study analyzed China’s medical separation reform policy through a financial lens, providing historical context and showcasing the reform’s viability via data analysis using the TOPSIS method. 42 Li et al Chaoran’s research underscores the advantages of the MBDS system in linking patients to online medical platforms and offline hospitals, integrating online services into traditional medical systems to enhance resource utilization and medical service accessibility. 43 Yu et al Jie and colleagues proposed a multi-patient treatment model to enhance medical efficiency and patient satisfaction, particularly in the strained doctor-patient relationships found in large public hospitals. 44 Sun and Zhu Xiaowei and team developed a DRG-oriented mathematical model to forecast and lower medical service costs, with the aim of alleviating the financial burden of patients’ healthcare expenses. 45 Collectively, the literature indicates that while China has made strides in tackling healthcare challenges, ongoing enhancements are necessary to ensure fair access and affordability of care for all individuals seeking medical assistance.
There is extensive research on the various factors that impact health care costs. Milan and Pinderhughes conducted a detailed study on how the self-presentation of mothers and abused children affects their adjustment to foster care, underscoring the significance of early experiences in shaping future healthcare needs. 46 Mroczek et al delved into the influence of hospital design and staff perceptions on patient outcomes, highlighting the crucial role of the physical environment in healthcare facilities. 47 Environmental factors play a vital role in health care costs, as evidenced by Kamphuis et al’s examination of determinants of fruit and vegetable consumption in adults. 48 Snell et al adopted a social cognitive approach to understanding customer compliance in healthcare, emphasizing the predictive power of past behavior on future intentions. 49 Birch et al explored consumers’ conscious attitudes toward local food, illustrating how ethical, environmental, and health considerations influence food consumption decisions. Collectively, these studies reveal that the determinants of health care costs are multifaceted. 50
A thorough examination of the research literature on “health care costs” reveals a significant gap in the existing studies. While financial forecasting and cost control in public health care institutions are the primary areas of focus in this field, there is a lack of empirical research on the influence of housing stress on medical consumption, particularly within urban socioeconomic contexts.
Gaps in Existing Literature
While extensive research has been conducted on housing stress and health care costs independently, there is a notable scarcity of studies examining the correlation between the two. This gap is particularly pronounced in the current academic literature, especially within the context of China. The direct influence of housing stress on health care costs remains largely unexplored, leading to significant knowledge deficiencies. Existing literature has acknowledged the potential impact of housing stress on health outcomes, but often lacks thorough quantitative evaluations of health care costs related to housing stress. Furthermore, studies frequently analyze the effects of housing stress alongside other stressors, making it difficult to isolate and measure the direct effects of housing stress on health care costs. The predominant focus of current research is on Western countries, resulting in a lack of representation of Asian contexts, particularly China. The distinct dynamics and consequences of housing stress in China have not been extensively studied due to cultural, social, and economic disparities.
Moreover, the current literature tends to concentrate on specific aspects of housing stress, such as affordability or quality, rather than encompassing all dimensions including tenure insecurity, crowding, and housing affordability. This fragmented approach may not offer a comprehensive understanding of the impact of housing stress on health care costs. Additionally, the utilization of various measurement scales in studies can lead to inconsistent findings and conclusions. While the existing literature provides valuable insights into the relationship between housing stress and health care costs, further research is imperative to address the identified gaps in the literature, particularly within the Chinese context. This study aims to delve deeper into the multidimensional aspects of housing stress, considering factors such as household income and health status as mediators influencing health care costs. By employing a unified measurement scale, this research seeks to minimize inconsistencies in findings and provide policymakers with reliable data. Such an approach will contribute to a more comprehensive understanding of the impact of housing stress on health care costs, a crucial aspect given the dynamic nature of the housing and healthcare sectors.
This research aims to investigate the relationship between housing stress and household health care costs by utilizing a panel two-way fixed effects model to analyze data from the China Family Panel Survey (CFPS) spanning from 2016 to 2020. This method offers a more precise understanding of how housing stress influences health care costs over time, allowing for an exploration of potential variations in different economic contexts. The study seeks to address 2 main questions: first, whether housing stress directly impacts household health care costs; and second, whether housing stress indirectly affects health care costs by reducing household income and exacerbating health issues. Through a comprehensive analytical framework (depicted in Figure 1), the research will delve into the Mediation Analysis through which housing stress influences health care costs, drawing on insights from microeconomics, political science, and sociology. The ultimate goal is to provide policymakers with empirical evidence to enhance their understanding of how housing policies can impact health care costs, leading to the development of more effective strategies to alleviate housing stress and enhance healthcare outcomes for families. The use of extensive CFPS data ensures the reliability of the study’s findings and the practicality of the policy recommendations.
Based on the preceding analysis, this article proposes the following hypotheses:
Materials and Methods
Data Source and Sample
This study utilizes data from the China Family Panel Study (CFPS), a nationally representative longitudinal survey conducted by the Institute of Survey of Social Sciences (ISSS) at Peking University since 2010. The primary objective of CFPS is to analyze the social and economic activities of urban and rural populations, as well as their impact on public health and welfare. The extensive information collected by CFPS serves as a valuable resource for empirical analysis on the relationship between housing stress and health care costs. The database includes detailed data on various aspects such as family economic structure, real estate, housing expenses, health status, health care costs, health expenditures, marriage, academic qualifications, education, and employment. 51 By controlling for potential confounders, more accurate estimates can be made regarding the influence of housing stress on health care costs. The relevant questionnaire is detailed in the supplementary material. This study specifically focuses on the 2016, 2018, and 2020 data from the China Family Panel Survey (CFPS). After cleaning the data and selecting households that rented, built, or bought a house within the CFPS from 2016 to 2020, a final sample size of 7343 households was obtained after removing missing and abnormal values, as illustrated in Figure 2.

Flowchart of data processing and analysis.
Measurements
Health care costs
The variable being examined in this article is health care costs, as defined by the ratio of “health care costs/total household income of the year” using data from the China Family Panel Survey (CFPS). 52 This approach effectively accounts for disparities in economic development across regions and price levels, enhancing the scientific validity and generalizability of the regression results.
Housing stress
Based on the theoretical analysis presented earlier, this article identifies family housing stress as the core explanatory variable. The variable is defined as 1 if the family has a mortgage or rents a house, and 0 otherwise. In this study, the head of the household in the China Family Panel Survey (CFPS) questionnaire is considered as the household financial respondent. To account for household heterogeneity, the housing stress for the current year is calculated as the ratio of total mortgage expenditure and total rent expenditure to the annual total household income, expressed as “(total mortgage expenditure + total rent expenditure)/total household income.” A higher ratio indicates greater housing stress for that year, derived from the questionnaire items “mortgage expenditure,” “rent expenditure,” and “total household income.”
Mediating variables
Based on the previous theoretical analysis, housing stress may influence health care costs through its impact on family income and health status.12,16,17 In this study, the mediating variables are family income, measured by household disposable income, and health status. The questionnaire assesses changes in health by asking respondents to compare their current health with that of a year ago, with 3 possible answers: “better,” “no change,” and “worse.” These responses are then converted into a binary variable, where 1 represents “better” or “no change,” and 0 represents “worse.”
Control variable
In this study, sociodemographic and socioeconomic factors were identified as control variables that could potentially affect health care costs. Sociodemographic factors examined included the age of the household head, marital status, and household registration type. Socioeconomic factors encompassed education level, employment status, occupation, medical insurance coverage, and family income. Age was treated as a continuous variable. Marital status was coded as 1 for married and 0 for unmarried. Household registration type was coded as 1 for urban and 0 for rural. Education was categorized into 3 levels: junior or lower, high school, and college or higher. Employment status was coded as 1 for employed and 0 for unemployed. 53 Additionally, family size, health insurance coverage rate, and dependency ratio were considered as continuous variables. Table 1 provides detailed definitions, coding schemes, and descriptive statistics for these key variables.
Descriptive Statics of the Variables.

Model Setting
This article employs a panel two-way fixed effects model54 -57 to investigate the influence of housing stress on health care costs. The bidirectional fixed effect model is employed in this paper due to its effectiveness in controlling unobserved individual and time effects, thereby reducing bias from omitted variables. This model’s advantage lies in its capacity to capture sample heterogeneity while accounting for temporal variation and individual differences. However, a notable limitation of fixed-effect models is that small sample sizes can result in instability in model estimates. Consequently, we place particular emphasis on the sample size during the model specification process to ensure the robustness of our model estimations. The model is structured as follows:

In the formula, “medit” represents health care costs as the dependent variable, “housingstressit” serves as the primary explanatory variable indicating the housing stress situation, and “Xit” includes control variables such as sociodemographic and socioeconomic factors. “δt” and “θi” denote year fixed effects and individual fixed effects respectively, while “εit” represents the random disturbance term.
Additionally, the analysis of the impact mechanism utilizes a mediation effect model to examine the relationship between housing stress and health care costs. The specific model is outlined as follows:



In this model, “medit” remains the dependent variable, “housingstressit”“ is the core explanatory variable, and “Xit” comprises the control variables as in model (2). “Mit” acts as a mechanism variable encompassing household income and health status. When coefficients “c1” and “a” are statistically significant, the presence of both significant “c2” and “b” values indicates a partial mediation effect. Conversely, if “c2” is not significant but “b” is, it signifies a complete mediation effect, with the mediation effect calculated as the product of “a” and “b.”
Results
Baseline Regression
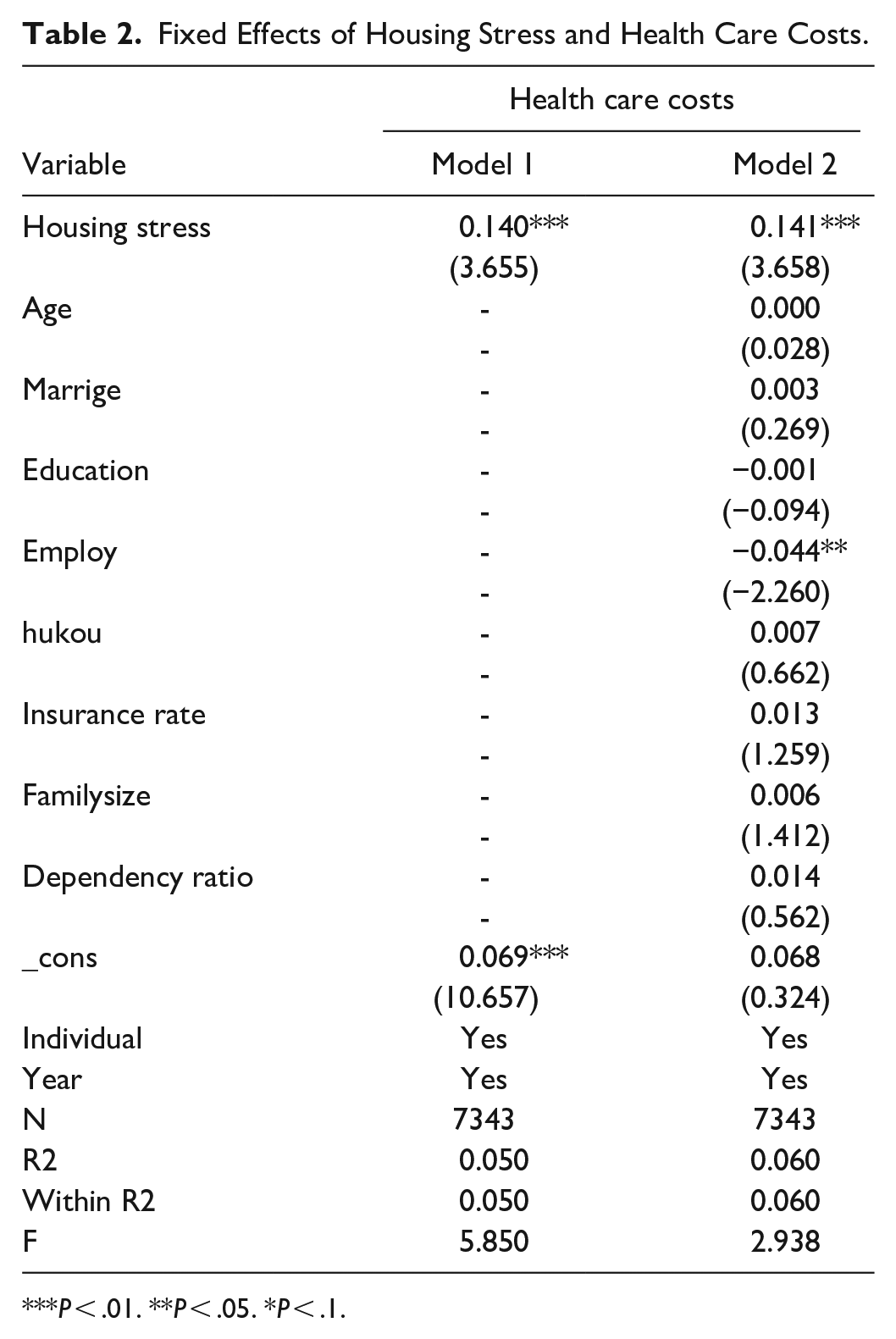
This study employs a two-way fixed effects model to analyze the impact of housing stress on health care costs. Model 1 includes individual fixed effects, year fixed effects, and core explanatory variables, while Model 2 incorporates additional control variables on top of Model 1. The results in Table 2 demonstrate a statistically significant positive correlation between housing stress and health care costs, regardless of whether only core explanatory variables are controlled or additional control variables are included. Specifically, the findings indicate that for every 1% point increase in housing stress, health care costs is projected to increase by 0.141.
Fixed Effects of Housing Stress and Health Care Costs.
P < .01. **P < .05. *P < .1.
Endogenetic Analysis
The previous regression results suggest a significant correlation between housing stress and health care costs. However, there may be endogeneity issues due to sample self-selection. To address this, the study employs K nearest neighbor matching, radius matching, and kernel matching in propensity score matching (PSM) for analysis. Typically, households spending 30% or more of their income on housing costs are classified as experiencing housing stress.6,33 Thus, this study treats housing stress as a quasi-natural experiment, where treated = 1 represents the treatment group and treated = 0 represents the control group.
When utilizing the propensity score matching method to address model selection bias, it is crucial to initially perform a common support test on the treatment and control group samples to validate the PSM estimation. Additionally, a balance test should be conducted on the samples to ensure that, post-matching, there are no systematic differences in variables aside from housing stress between the 2 groups.
Figure 3 illustrates the propensity score kernel density distribution of the treatment and control groups pre and post-matching. The majority of propensity score values for both groups fall within a similar range, and following matching, the disparity in propensity score distribution between the treatment and control groups is notably reduced. This suggests a high matching quality and successful passing of the common support hypothesis test.
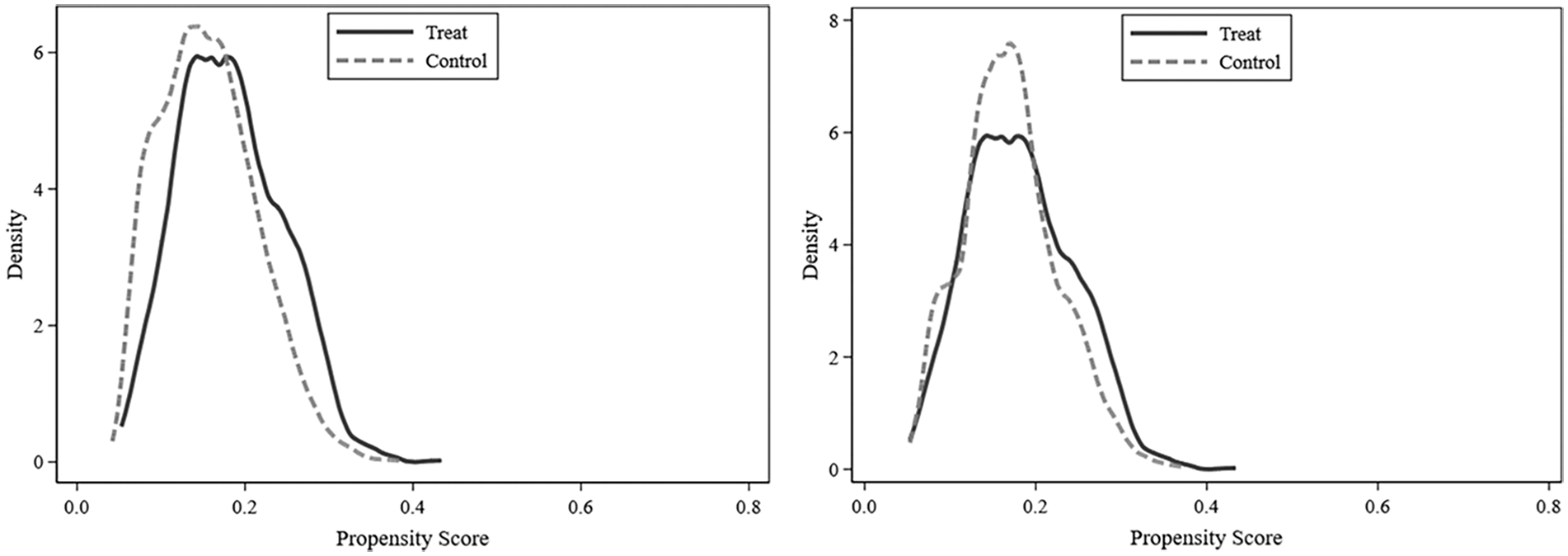
Propensity score kernel density map before and after matching.
Table 3 displays the results of the balance test. In comparison to pre-matching, the Pseudo R2 and LR test values decreased notably across all 3 matching methods. Additionally, MeanBias and MedBias also showed significant decreases, while the B values were below 25% in both cases. Propensity score Matching (PSM) effectively minimizes the disparity between the treatment and control groups, thereby improving control over endogeneity error. The application of PSM satisfies the conditional independence assumption, ensuring the reliability of the research findings.
Results of Balance Test.
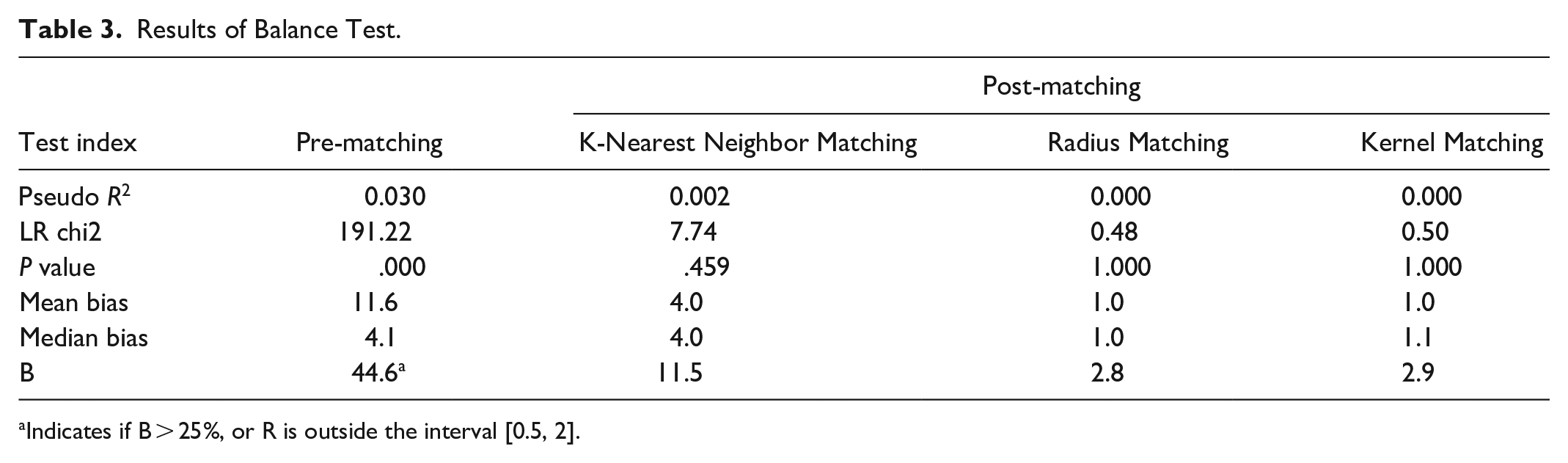
Indicates if B > 25%, or R is outside the interval [0.5, 2].
After conducting the balance test, the Average Treatment Effect on the 2 matched groups of samples is further measured. The influence of housing ownership stress on health care costs is presented in Table 4. The results of the calculations reveal that the matching outcomes obtained in this study are highly consistent across 3 different methods, with statistically significant Average Treatment Effect values at the 1% level. This suggests that the estimation results using various matching methods in this research exhibit consistency. Furthermore, the comparison of regression results remains stable.
Housing Stress Matches Propensity Scores for Health Care Costs.

P < .01. **P < .05. *P < .1.
Robustness Test
In order to ensure the credibility of the benchmark regression results, this study employs 3 main methods for conducting robustness testing. Firstly, future housing stress is assessed by the ratio of (total principal and interest of mortgage loans to be repaid + outstanding balance of private loans) to total household income. This ratio indicates the number of years required to settle the remaining mortgage and private loan balances in the future based on current household income levels. A higher ratio implies a longer future repayment period and increased future housing stress. 58 Both methods involve the substitution of core explanatory variables. Secondly, housing stress is measured using the housing price-to-income ratio, calculated as the total housing price divided by total household income. The third method involves altering the sample by selecting 35 large and medium-sized cities in China as the research subjects and employing 2-way fixed effects for regression analysis. The results of the robustness test consistently show a positive and statistically significant relationship between housing stress and household health care costs at the 1% significance level, with detailed results presented in Table 5. This finding aligns with previous estimations, further confirming the reliability of the empirical regression results presented in this article. In summary, these regression results support hypothesis 1.
Robustness Test of Housing Stress and Health Care Costs.
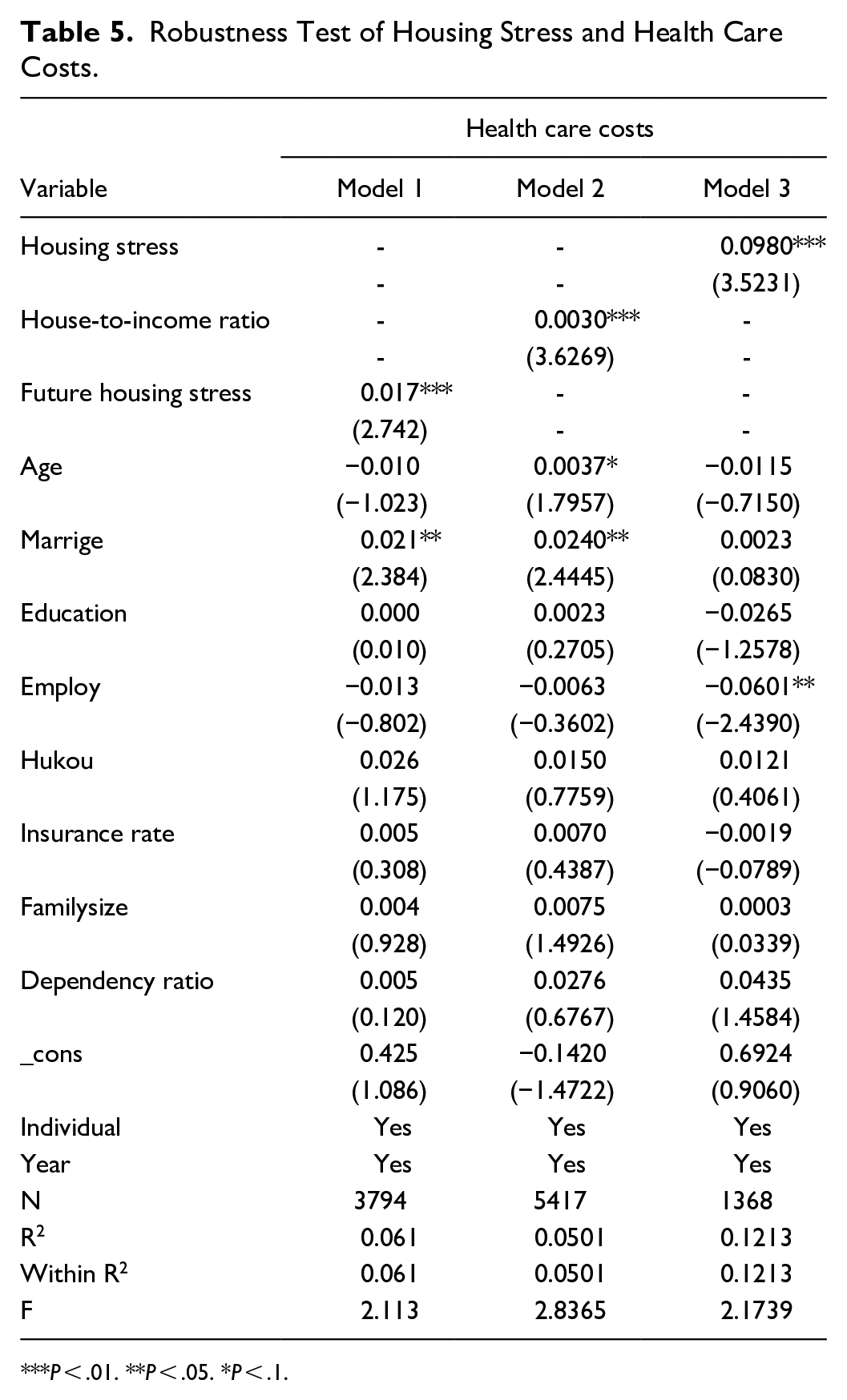
P < .01. **P < .05. *P < .1.
Mediation Analysis
Drawing on existing literature and theoretical frameworks, this study posits that housing stress has a direct impact on household disposable income, residents’ health status, and subsequent health care costs. These relationships are further elucidated through regression analysis, with detailed results presented in Table 6.
The Mediating Effect of Housing Stress and Health Care Costs.

P < .01; **P < .05. *P < .1.
The regression results in Table 6 show that Model 1 and Model 2 analyze the impact of household disposable income and residents’ health status on housing stress. It is evident that higher housing stress reduces household disposable income and negatively affects residents’ health status. Specifically, a 1% point increase in housing stress results in a 1.749 decrease in household disposable income and a 0.468 decline in health status. Moreover, Model 3 and Model 4 in Table 6 address the relationship between health care costs, household disposable income, and residents’ health status. The findings align with existing literature and real-world observations, indicating that higher household disposable income and better residents’ health status lead to a significant decrease in health care costs. The regression results align with this reality and support hypothesis 2.
Heterogeneity Analysis
This paper further analyzes the heterogeneity among regional, urban, and rural groups, as well as rent-purchase groups. By comparing the impact of housing stress on health care costs across the eastern and western regions, as well as urban and rural areas, we find that while the overall regression result is significant, the magnitude of the impact coefficient varies considerably. This variation may be attributed to differences in economic development levels, housing market conditions, and the distribution of medical resources across different regions.
Firstly, the impact of housing stress on health care costs varies significantly across the eastern, central, and western regions. The coefficient for the eastern region is 0.123, for the central region it is 0.055, and for the western region, it is 0.207. Notably, the western region exhibits the greatest impact, which can be attributed to its lagging economic development, inadequate medical resources, and insufficient social security systems. Despite relatively low housing prices in the western region, residents often allocate their limited resources to healthcare to address basic health needs, even in the face of housing stress. The eastern region ranks second in terms of impact. Although it experiences the highest housing price stress, the region benefits from a stronger economic foundation and a more developed healthcare system, enabling it to manage routine health issues more effectively. Conversely, the central region shows the least impact; while its economic development and resident income levels are lower than those in the eastern region, they are higher than in the western region. Income level is a crucial determinant of health care costs, and lower income may result in limited investment in health services.
Secondly, housing stress significantly influences health care costs in both urban and rural areas, with coefficients of 0.164 and 0.106, respectively. However, the effect of housing stress on health care costs is more pronounced in urban areas. This disparity can be attributed to 2 primary factors. On the one hand, excessively high housing prices in urban regions result in a substantial increase in family housing costs, thereby heightening housing stress. Consequently, families are compelled to allocate more resources toward healthcare to meet essential health needs. On the other hand, there is a notable difference in the medical security systems between urban and rural areas in China. Urban regions typically benefit from a more robust medical security framework, whereas rural areas experience a comparatively weaker system. This divergence contributes to varying degrees of increase in health care costs that households face when confronted with housing stress.
Finally, housing stress significantly influences health care costs for both renters and homeowners, with coefficients of 0.243 for renters and 0.121 for homeowners. This disparity may be attributed to 3 primary factors. First, renters lack the assurance of long-term asset accumulation, whereas homeowners benefit from economic security and potential asset appreciation. Particularly during periods of rising housing prices, renters experience heightened psychological stress; their financial vulnerability, stemming from the absence of long-term assets, renders them more sensitive to health care costs in anticipation of potential future health issues. Second, the rental market is characterized by greater mobility and uncertainty, leading renters to confront factors such as rent increases and the need for relocation. This instability may prompt renters to invest more in healthcare to ensure timely and efficient access to services when health issues arise. Third, renters often cannot afford homes in desirable school districts, resulting in their children missing out on high-quality, free educational opportunities and necessitating enrollment in costly private schools. Consequently, renters face the dual stress of rising rents and annual tuition fees. Additionally, the typically subpar living conditions of rental properties can adversely affect the health and well-being of family members, further escalating health care costs. For more detailed information, refer to Table 7 in the manuscript.
Heterogeneity Analysis of Housing Stress and Health Care Costs.

P < .01. **P < .05. *P < .1.
Discussion
Discussion and Implication of the Findings
The empirical findings of this study, based on CFPS data, indicate a significant correlation between housing stress and heightened health care costs. Specifically, a 1% point rise in housing stress corresponds to a 0.141 increase in health care costs, highlighting the direct influence of housing conditions on individuals’ health status. The act of purchasing a house can impose substantial financial and psychological strain on many Chinese individuals, negatively impacting their health status.6,59 These results underscore the necessity for comprehensive social and economic interventions in this domain.
This study delves into the impact of housing stress on health care costs and explores the underlying pathways. The research reveals significant differences in the effect of housing stress on health care costs, even after accounting for sociodemographic and socioeconomic factors. Specifically, the study highlights that household disposable income and health status play a mediating role in this relationship. By investigating the influence of household disposable income and health status on the connection between housing stress and health care costs, the study contributes to existing literature. The findings indicate that housing stress has a negative impact on household disposable income, subsequently affecting health care costs. This could be attributed to the fact that heightened housing stress reduces household disposable income and contributes to deteriorating health status among residents. The results of the study demonstrate that a one-percentage-point increase in housing stress results in a 1.749 decrease in household disposable income and a 0.468 decrease in health status.
Increasing household disposable income has been shown to have a positive impact on household health care costs. Higher levels of household disposable income lead to increased spending on both private and public health inputs, such as medical care, nutritious food, improved sanitation, and water, resulting in improved health outcomes. 60 This ultimately leads to a decrease in the need for extensive health care services. Additionally, the rise in household disposable income enables patients to access better treatment and rehabilitation services, like surgery and physical therapy, which can mitigate the adverse health effects of diseases and potentially eliminate the disease altogether, further reducing health care costs. Research conducted in northwestern Ethiopia demonstrated that maternal health services played a significant role in reducing maternal mortality rates.12,61 In addition, different types of housing stress have varying impacts on health care costs. Renters are significantly affected by housing stress when prices rise, as they are vulnerable to rent increases at any time, influencing their decisions regarding health care costs. Conversely, homebuyers are less affected, likely due to their homeownership and the mindset of “earning money when you buy it,” making them less sensitive to housing stress. However, individuals planning to buy a house often face challenges such as down payments and loan interest, leading them to increase working hours, which can impact their physical and mental health and result in increased health care costs.59,62
Policy Recommendations for Reducing Housing Stress
Housing serves as a fundamental guarantee for human survival and constitutes a vital component of major livelihood projects and basic social welfare security. It holds significant importance for the majority of the Chinese population. The relationship between housing and health care costs is a critical factor in China’s development and progress. The advancement and prosperity of real estate must not compromise public health, underscoring the necessity for sustainable and environmentally friendly development practices that foster both physical and mental well-being.
Firstly, we should implement reforms to the mortgage policy, specifically introducing a “personal limited liability system.” 63 In China, borrowers are obligated to continue repaying their mortgages even when the property is “unfinished”—that is, when the house they purchased has yet to be constructed—or if they opt to cease mortgage payments. This situation arises because the purchase contract and the loan contract are regarded as 2 distinct legal relationships. Currently, China operates under a system of personal unlimited liability, placing all associated risks on the homebuyer.
In the United States, the mortgage system operates under a “personal limited liability system,” 63 where the risk of default is shared between the individual borrower and the bank. In contrast, China employs an “personal unlimited liability system,” wherein all risks are borne solely by the homebuyer. Consequently, Chinese banks are relatively insulated from risk. For instance, consider a scenario where a homebuyer secures a loan of 3 million RMB, makes a down payment of 900 000 RMB, and borrows the remaining 2.1 million RMB from the bank. If the property’s value declines to 1.5 million RMB and the buyer opts to default on the mortgage, the bank in the United States can only reclaim the property and auction it, regardless of the auction outcome. The bank assumes responsibility for any shortfall, and the buyer’s losses are limited to the down payment. Conversely, in China, if the property is repossessed or foreclosed, and the auction yields only 1.5 million RMB, the buyer’s losses extend beyond the initial 900 000 RMB down payment to include the decline in property value. In this case, the borrower would still owe the bank an additional 600 000 RMB, assuming the auction price matches the market value. Should the auction price fall below this amount, the borrower would incur even greater losses.
In terms of repayment methods, the primary obligation for a borrower is to pay the interest on their bank loan. In China, mortgage rates are relatively high, averaging around 5% for commercial mortgages, in contrast to approximately 2% in developed countries. Throughout the typical 20 to 30 year loan period, the interest and principal payments are generally balanced. If a borrower opts to default on their mortgage, the repercussions extend beyond the loss of property; they may also incur substantial debts to the bank. In China, banks are not deterred by the prospect of borrowers defaulting on loans. Even if a borrower purchases a “rotten building”—referring to an off-plan or unfinished property—they remain obligated to repay the bank. Should a borrower choose to halt mortgage payments, the bank will seize every available penny after deducting the borrower’s essential living expenses. In the United States, borrowers can choose to walk away from their loan, risking only their down payment. Conversely, in China, this option is not viable; home loans can result in the loss of “everything,” including property auctioned off, forfeiture of the down payment, incurring interest penalties, negative impacts on personal credit scores, inclusion on credit blacklists, restrictions on daily life (such as prohibitions on air travel or high-speed rail), litigation costs, familial disruption, limitations on consumption behavior, freezing of bank accounts, and an inability to apply for new loans or credit cards. The resultant “housing stress” is significant. From a certain perspective, the “personal unlimited liability system” model employed by modern banks in China is arguably more detrimental than the philosophies of pawnshops or moneylenders prevalent in feudal China. It is ironic that such a model continues to function effectively.
Therefore, the Chinese government should reform the mortgage policy by implementing a “personal limited liability system,” which would ensure that the risks associated with loan amounts are shared between individuals and banks. Additionally, it is essential to draw lessons from the advanced real estate, loan, and financial policies of developed countries. Such measures would effectively alleviate housing stress on the population, subsequently reduce health care costs, and ultimately enhance long-term social welfare.
Secondly, to optimize land policy, it is recommended to implement pilot land privatization reforms. 64 Privatization can facilitate the free flow of land and enhance the efficiency of land resource allocation. The improvement in land use efficiency following privatization contributes positively to overall production efficiency. Furthermore, land privatization can encourage initiative and innovation among land management entities, leading to more rational practices in land use and management. This approach is beneficial in breaking the bureaucratic monopoly over land finance, enhancing the fairness and equality of land use rights, reducing the impact of land finance on housing prices, and thereby alleviating housing stress.
Finally, inclusive and equitable housing policies are essential for ensuring equal rights to rent and purchase homes, reducing inequality, and providing rent subsidies to families with incomes below certain thresholds to alleviate housing burdens. Monitoring mechanisms must be established to effectively distribute these subsidies to targeted households. Furthermore, it is crucial to control housing prices, reduce housing costs, and alleviate housing stress. The “personal unlimited liability system” associated with home loans and elevated housing prices are significant contributors to housing stress, adversely impacting household income and health status, as well as increasing health care costs. It is imperative to address the detrimental practices of local governments that depend on land finance and the real estate market for land sales and speculation. The focus should shift toward a more efficient and transparent government with open elections for local officials, prioritizing service-oriented and environmentally sustainable policies. These strategies will be effective in alleviating public issues such as high housing costs, housing stress, and the challenges associated with accessing affordable health care costs.
Limitations
The study demonstrates notable strengths through the utilization of panel data and a substantial sample size. By incorporating panel data, the research establishes a stronger causal relationship between housing stress and health care costs over time, thereby bolstering the credibility of the findings. Additionally, the identification of household disposable income and health status as pertinent mediating variables holds significant sociological implications, distinguishing this study from others exploring the mediating role of housing stress on healthcare utilization. However, there are some limitations to the study that warrant further reflection. First, the measurement method of housing stress was limited in this study. It mainly focused on the economic burden perspective, neglecting factors such as the neighborhood environment and physical characteristics of the housing community, which could be important control variables. 65 Second, the study concentrated on the impact of housing stress on average health care costs. Future research should investigate how housing stress affects disparities in health care costs, particularly among different socioeconomic and demographic groups, especially disadvantaged populations. Third, due to data limitations, prospective studies were lacking. While this study used panel data and statistical methods for complementary research, it is important to note that the psychology of buyers during periods of rising housing prices may influence the perceived stress on those with mortgage loans compared to renters. However, research on housing stress during housing price declines is lacking, and future studies should consider longitudinal research, case-control studies, randomized controlled trials, and other methods to strengthen the evidence for a causal relationship between housing stress and health care costs. This study utilized an existing CFPS database; therefore, no formal sample size or power analysis was conducted during the study design phase. This limitation may impact the generalizability of the findings. Future research should consider performing sample size calculations to enhance the statistical power and reliability of the conclusions drawn from the study. Despite these limitations, this study represents an initial step in understanding the link between housing stress and health care costs, offering valuable insights. In conclusion, a systematic exploration of the theoretical and practical aspects of housing stress can inform strategic healthcare policies and programs aimed at alleviating financial burdens on families.
Conclusions
This study, based on the analysis and results of the China Family Panel Study (CFPS) data, conclusively confirms the significant impact of housing stress on health care costs. The findings reveal a positive relationship between housing stress and health care costs, indicating that a 1% point increase in housing stress leads to a 0.141 increase in health care costs. This relationship holds true for both the renting and buying groups, highlighting the universal impact of housing stress on health care costs. Furthermore, household disposable income and residents’ health status act as mediators in this relationship. Specifically, a 1% point increase in housing stress results in a reduction of household disposable income by 1.749 and health status by 0.468. According to these findings, policy interventions such as mortgage policy reform and the implementation of a “limited personal liability system”—which allows borrowers the opportunity to declare bankruptcy—are essential for effectively safeguarding their rights to survival and development. Additionally, low-rent housing programs or rent subsidies for low-income families can alleviate housing stress. Furthermore, promoting policies that ensure equal rights for renters and homebuyers can foster a fairer and more harmonious society. It is important to recognize that housing stress is merely a symptom of a larger issue: the monopoly of land ownership. To address this problem, it is crucial to optimize land policy and eliminate land financing by local governments. This approach will enable citizens to genuinely benefit from land policies, rather than being temporary “users” of land ownership and “victims” of real estate development. The ultimate goal is to reduce inequalities and inequities related to land ownership and access. These measures will fundamentally alleviate housing stress, lower survival costs, and achieve a more balanced development between the housing market and the health sector. In turn, this can minimize the social costs associated with health care costs and support the objective of wealth redistribution. Ultimately, these actions can contribute to the long-term social welfare of the population.
Supplemental Material
sj-docx-1-inq-10.1177_00469580241290145 – Supplemental material for How Housing Stress Affect Health Care Costs: A Panel Data Study
Supplemental material, sj-docx-1-inq-10.1177_00469580241290145 for How Housing Stress Affect Health Care Costs: A Panel Data Study by Gai Liu, Jianchao Zhou and Yuxiang Wang in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580241290145 – Supplemental material for How Housing Stress Affect Health Care Costs: A Panel Data Study
Supplemental material, sj-docx-2-inq-10.1177_00469580241290145 for How Housing Stress Affect Health Care Costs: A Panel Data Study by Gai Liu, Jianchao Zhou and Yuxiang Wang in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-3-inq-10.1177_00469580241290145 – Supplemental material for How Housing Stress Affect Health Care Costs: A Panel Data Study
Supplemental material, sj-docx-3-inq-10.1177_00469580241290145 for How Housing Stress Affect Health Care Costs: A Panel Data Study by Gai Liu, Jianchao Zhou and Yuxiang Wang in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors would like to thank the seniors and Zhengzhou University School of Management teacher Tang Ke for their guidance and assistance.
Authors’ Contributions
Data Availability
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The studies involving human participants received approval from the Biomedical Ethics Review Committee of Peking University, designated as CFPS. All participants were required to provide written informed consent prior to their involvement. The ethical approval number for this study is IRB00001052-14010. In cases where participants were unable to provide consent, written informed consent was obtained from their legal guardians or next of kin.
Consent for Publication
All the authors listed in this paper read the manuscript and agreed to submit it for publication.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.