
Abstract
COVID-19 mortality disparities for socially vulnerable patients, including individuals facing higher levels of poverty, housing insecurity, and limited transportation, have been linked to the quality of hospitals where they received care. Few studies have examined the specific aspects of hospitals, such as nursing care quality, that may underlie disparate outcomes. Recent studies suggest that nursing resources in the pre-pandemic period were associated with mortality during the COVID-19 public health emergency. In this study, we examined the association between social vulnerability, the nurse work environment, and inpatient mortality among Medicare beneficiaries hospitalized with COVID-19. A cross-sectional analysis was conducted of linked survey data collected from nurses working in New York and Illinois, Medicare claims, American Hospital Association Annual Survey data, and the Social Vulnerability Index (SVI). Higher mortality rates were observed among patients in the highest quartile of social vulnerability compared to the lowest (6870 [25.8%] vs 5019 [19.1%]; P < .001). Using multivariable regression modeling, a statistically significant interaction was found between the highest SVI quartile and the nurse work environment (OR, 0.86; 95% CI, 0.76-0.98; P < .05), implying that the effect of a higher quality nurse work environment on mortality was decidedly greater for patients in the highest quartile (odds ratio = 0.86 × 0.94 = 0.80) compared to patients in the lowest quartile (OR, 0.94). Post-hoc analyses demonstrated that hundreds of COVID-19 related deaths among the most socially vulnerable patients may have been avoided if all hospitals had a high-quality nurse work environment. Strengthening the quality of nurse work environments may help to reduce health disparities and should be considered in public health emergency planning, specifically in hospitals serving socially vulnerable communities.
Mortality disparities among socially vulnerable patients, including individuals facing higher levels of poverty, housing insecurity, and limited transportation, were well documented during the COVID-19 pandemic and were linked in part to hospital quality. Less is known about the specific aspects of hospitals, including the extent to which the pre-pandemic quality of the nurse work environment was associated with the outcomes of socially vulnerable adults hospitalized with COVID-19 during the pandemic.
In this cross-sectional study of 105,560 Medicare beneficiaries with a diagnosis of COVID-19 in 238 acute care hospitals, higher nurse work environment quality was associated with a 20% reduction in the odds of mortality among patients residing in the most socially vulnerable neighborhoods. Our finding that mortality disparities narrowed when patients from the most socially vulnerable neighborhoods were cared for in hospitals with the best nurse work environments suggests the need for investments in nursing resources in hospitals serving these communities. Of note, we find that hundreds of deaths could have been avoided had the most socially vulnerable patients been admitted to hospitals characterized by high quality nurse work environments.
Strengthening the quality of nurse work environments may represent a public health intervention to promote the health of socially vulnerable adults and should be incorporated into emergency response planning, specifically in hospitals serving socially vulnerable communities.
Introduction
Since the start of the coronavirus disease 2019 (COVID-19) pandemic, hospitalization and mortality rates have been demonstrably higher for residents of socially vulnerable communities. 1 The burden of the pandemic among the most socially vulnerable is the product of pre-existing structural factors such as inequities in community resources including housing, transportation, income, and access to health care.1-3 Some studies suggest that higher mortality rates among socially vulnerable populations, including racial and ethnic minorities, may be attributable to differences in hospital quality.4,5 Few studies, however, have examined the specific facets of hospital quality, including the care delivered by registered nurses (RNs), that underlie disparate outcomes.
A recent National Academy of Medicine (NAM) report emphasized how nurses can reduce disaster-related disparities among vulnerable populations through the implementation of evidence-based interventions and the provision of high-quality clinical care. 6 Clinical care guidelines for hospitalized adults with COVID-19 include the delivery of oxygen therapy and intravenous fluids and medications, as well as monitoring for respiratory distress and mental status changes 7 —care typically provided by registered nurses (RNs). The RN role also includes assessing health-related social needs, evaluating cultural- and language-based needs and preferences, providing patient- and family-centered education, and coordinating care. 6 Even prior to the pandemic, multiple studies found that nurses reported being unable to provide such care due to poor work environments, insufficient organizational resources, and excessive patient workloads.8,9
The ability of nurses to deliver high-quality care hinges upon a supportive work environment. 10 The nurse work environment is defined as the organizational characteristics of a work setting that facilitate or constrain professional nursing practice. 11 In the best work environments, nurses have strong collegial relationships with physicians, contribute to organizational decision making, and have adequate staffing and resources. In a recent meta-analysis of 17 international studies, the quality of nurse work environments was linked to several patient outcomes, including mortality. 12 Associations between the nurse work environment and outcomes of hospitalized patients during the COVID-19 pandemic have also been described.13,14 For example, a recent study by Aiken et al 13 found that poor work environments in place prior to the COVID-19 pandemic were associated with poorer ratings of quality and patient safety during the pandemic. Likewise, Lasater et al 14 found that more robust pre-pandemic nursing resources, including sufficient staffing, supportive work environments, and higher levels of education, were associated with lower COVID-19 associated mortality among Medicare beneficiaries. Despite the evidence linking work environments to patient outcomes, attention to whether nursing resources in place prior to the pandemic were sufficient to meet the needs of patients from socially vulnerable communities is largely absent from emergency preparedness planning. Patients admitted from socially vulnerable communities face higher levels of poverty, housing insecurity and limited transportation. These factors place patients at higher risk for poor health outcomes and necessitate more intensive nursing care during hospitalization, including extensive patient education and facilitating connections to community-based resources. Our study focuses on the quality of nurse work environments as an organizational measure to assess nurses’ ability to provide necessary care. We posit that a high-quality nurse work environment would have a greater impact on the outcomes of COVID-19 patients admitted from socially vulnerable communities.
We suspect that nurses lacking a supportive work environment would have less time, resources, and support to address the complex needs of patients admitted from socially vulnerable communities resulting in disparate outcomes.
New Contribution
Our study offers several new and novel contributions. First, using data about hospital nursing resources collected in the weeks prior to the first wave of patients with COVID-19 entering U.S. hospitals, we evaluated whether variation in hospitals’ nurse work environments was associated with COVID-19 mortality disparities among patients with varying levels of social vulnerability. The RN4CAST-NY/IL nurse survey data, collected before the pandemic, provide a unique assessment of health system readiness for public health crises by evaluating the baseline infrastructure of nursing in place before the emergency. Efforts to mitigate the effects of natural disasters such as the pandemic require careful assessments of resources in place prior to the event to determine the potential impact on socially vulnerable communities. A useful example would be the case of Hurricane Katrina. Had a proper evaluation of the flood protection levees in New Orleans been completed prior to the devastating storm, they would have concluded that the parishes where Black residents lived were at the greatest risk. 15 We posit that a similar assessment of nurse work environments prior to the onset of the pandemic may have provided important signals to clinicians, healthcare administrators, and policymakers of the ability of hospitals to effectively care for the most socially vulnerable patients.
A second novel aspect of this study is our use of a sequential hierarchical modeling approach instead of hospital-level random effects employed by others 4 which allowed us to examine the independent contribution of individual hospital characteristics to mortality disparities. A final new contribution is our estimation of how many in-hospital COVID-19 deaths might have been prevented had the most socially vulnerable patients been cared for in hospitals that were characterized by high-quality work environments.
The aims of the current study were to: (1) determine if COVID-19 patients from socially vulnerable communities experienced higher odds of in-hospital mortality, and (2) evaluate to what extent variations in hospital nurse work environments where COVID-19 patients from socially vulnerable communities received care explain differences in mortality outcomes. We hypothesized that patients residing in more socially vulnerable communities would be more likely to die from COVID-19, and that the quality of the nurse work environment would moderate the relationship between social vulnerability and mortality.
Methods
Study Design and Sample
This cross-sectional observational study linked data from 4 sources using a common hospital identifier. The 2020 Centers for Medicare and Medicaid (CMS) Medicare Provider Analysis and Review (MedPAR) file provided demographic and clinical information for hospitalized Medicare beneficiaries with COVID-19. The American Hospital Association (AHA) Annual Survey of hospitals provided data on the structural characteristics of hospitals, such as size and teaching status. The US Centers for Disease Control and Prevention (CDC)/Agency for Toxic Substances and Disease Registry (ATSDR) Social Vulnerability Index (SVI) database 15 was used to classify patients’ social vulnerability based on their residential zip code. The SVI is the gold standard metric used by public health officials and emergency response planners to identify and map the communities that will most likely need support before, during, and after a hazardous event. 16 The study protocol was deemed exempt by our Institutional Review Board.
The RN4CAST-NY/IL survey of RNs was collected between December 16, 2019, and February 24, 2020, and provided information about the nurse work environment of hospitals. Emailed surveys were sent by the National Council of State Boards of Nursing to all actively licensed RNs in NY and IL. Our method of direct outreach to nurses through licensing registries is preferred over approaching hospitals to recruit nurses, which could lead to significant non-response bias because hospitals with poorer results might be less inclined to take part. Non-respondents received repeated follow-up invitations to participate over 2 months using the Dillman method. 17 In a previous nurse survey using a similar instrument, we evaluated non-response bias using a double-sampling approach of nonrespondents and found no discernible differences in ratings of nurse work environments between survey respondents and nonrespondents. 17 The nurse-level response rate from surveying over half a million actively licensed RNs in NY and IL was 18%, which is within the usual range of response rates for electronic surveys. 13 On average, study hospitals had 65 nurse respondents to the RN4CAST-NY/IL survey. Notably, our sample includes 93% of general acute care hospitals in NY and IL; with 100% representation among the larger hospitals (>250 beds) which care for the greatest share of patients.
On the survey, nurses reported their employment setting (eg, hospital, nursing home) and position (eg, staff nurse, nurse manager). If a respondent worked as a direct care staff nurse at an acute care non-federal hospital, they were included in the sample. Nurses not directly involved in adult inpatient care were excluded. We received 24 114 responses from hospital-based RNs working in direct care. Nurse respondents also provided the name of their employing hospital, allowing for the aggregation of responses within hospitals. Like others, 17 the reports of nurses working in hospitals with at least 10 survey respondents were used to construct reliable hospital-level estimates of the nurse work environment. The RN4CAST-NY/IL study methodology has also been described elsewhere.13,17
Our sample includes acute care, non-federal, and general hospitals that had at least 10 responses to the RN4CAST-NY/IL survey, had COVID-19 admissions in 2020, were located in NY or IL, and responded to the AHA Annual Survey of hospitals. After all inclusion criteria were applied, our final sample included the survey responses of 13 963 direct care staff RNs (see Supplemental Material Table 1 for nurse respondent characteristics) employed in 238 hospitals.
Our patient sample included Medicare beneficiaries aged 18 to 99 years hospitalized between January 1, 2020, and December 31, 2020, with a primary or secondary diagnosis of COVID-19 as identified by International Classification of Diseases, 10th Revision (ICD-10) codes U071, U072, or B9729. Patients with a length of stay of <24 h were excluded.
Outcomes and Measures
Our outcome of interest was 30-day inpatient mortality defined as death occurring in the hospital within 30 days of admission.
Key independent variables of interest were the Social Vulnerability Index (SVI) and the nurse work environment. The SVI was obtained from the 2020 CDC/ATSDR SVI database. 15 The SVI is constructed using 16 variables derived from U.S. Census/American Community Survey (ACS) data that are organized into 4 themes: socioeconomic status (eg, income, employment), household composition (eg, age, single parent), minority status and language (eg, racial minority, limited English proficiency), and housing and transportation (eg, housing type, vehicle). The SVI is reported as a relative percentile rank ranging from 0 to 1 (with higher values indicating greater vulnerability) for every U.S. Census tract. Using a crosswalk, 18 we linked census tract-level SVI to patients’ residential zip codes included in the MedPAR file. Following procedures outlined by others, we categorized patients into 4 quartiles based on their SVI with higher quartiles representing higher levels of social vulnerability.5,19,20
The nurse work environment was measured using a short form of the Practice Environment Scale of the Nursing Work Index (PES-5) that was included on the RN4CAST-NY/IL survey. The PES-5 was adapted from the National Quality Forum-endorsed Practice Environment Scale of the Nursing Work Index and includes 5 items: (1) administration that listens and responds to employee concerns; (2) a nurse manager who is a good manager and leader; (3) a lot of team work between nurses and physicians; (4) enough staff to get the work done; and (5) a clear philosophy of nursing that pervades the patient care environment. 21 Respondents rated the degree to which each item was present in their primary job on a scale of strongly agree (1) to strongly disagree (4). A hospital-level work environment score was calculated as the mean of the 5 items across all units within each hospital. 21 In a recent psychometric evaluation of the instrument using RN4CAST-NY/IL data, the PES-5 demonstrated strong reliability (Cronbach alpha = 0.81) and predictive validity. 22 The PES-5 score was treated as a continuous variable in the analysis and was standardized for use in the logistic regression models.
Covariates
Patient characteristics were obtained from the MedPAR file and included: age (<55, 56-65, 66-75, 76-85, and 86-99), race/ethnicity (White, Black, Hispanic, Asian, Other/Unknown), sex (male/female), the Elixhauser Comorbidity Index, 23 and days between January 1, 2020, and date of admission (to account for changes over time in COVID-19 diagnostics and treatment). 4
Hospital characteristics were obtained from the AHA Annual Survey. Hospital size was defined as small (<100 beds), medium (101-250 beds), and large (>250 beds). Hospitals with high technology capability could perform major organ transplants and/or open-heart surgery. Teaching status was based on the ratio of medical trainees to beds: none, minor (0-4 trainees per bed), and major (≥4 trainees per bed). Core-based statistical area (CBSA), a U.S. Census-based measure of population density, was defined as metropolitan (≥50 000), micropolitan (≥10 000-49 999), and rural (<10 000). We also accounted for the state in which the hospital was located (NY/IL).
Statistical Analysis
We compared patient and hospital characteristics, and nurse work environment scores between patients across the 4 SVI quartiles using chi-square tests for categorical variables and analysis of variance (ANOVA) for continuous variables. Next, we fit a series of multi-level hierarchical logistic regression models to estimate the association between SVI quartile, nurse work environment and 30-day inpatient mortality among patients with COVID-19. Models were hierarchical in that each adjusted model added a variable or set of variables to those included in the previous model. Model 1 (unadjusted) included SVI quartile. Model 2 added patient characteristics (age, race/ethnicity, sex, Elixhauser Comorbidity Index, and number of days between January 1, 2020, and date of admission). Model 3 added hospital characteristics (size, technology capability, teaching status, CBSA, and state). Model 4 added the nurse work environment measured by the PES-5. Model 5 was a fully adjusted model including an interaction term between SVI quartile and nurse work environment to examine how the effect of SVI quartile on mortality varied by the nurse work environment. Models were estimated using Huber-White (robust) procedures to account for clustering of patients within hospitals and to adjust the standard errors of estimates. 24 Using post-hoc estimates, we predicted how many deaths among COVID-19 patients could have been potentially avoided across all levels of social vulnerability had all patients been admitted to study hospitals in the top quartile of the nurse work environment score. Analyses were conducted using STATA 17.0. The EQUATOR STROBE guidelines were used for reporting.
Results
Characteristics of the 105 560 patients included in the study by SVI quartile are presented in Table 1. The mean (SD) age of patients was 75.2 (11.5) years. Patients in the most socially vulnerable communities (quartile 4) were younger compared to patients in the least (quartile 1) vulnerable communities (mean age 73.7 years vs 76.7 years, P < .001). 54 812 (51.9%) of patients included in the sample were male. Patients had a mean (SD) Elixhauser Comorbidity Index score of 10.8 (16.0). Most patients in the lowest SVI quartile were White (21 799[82.8%]), while Black patients comprised the largest racial/ethnic group (10 437[39.1%]) in the highest SVI quartile. Roughly 1 in 5 (23 437[22.2%]) patients with COVID-19 died in the hospital within 30 days of admission. Higher mortality rates were observed among patients in the highest SVI quartile compared to the lowest (6870 [25.8%] vs 5019 [19.1%]; P < .001). Patients in the highest SVI quartile presented significantly earlier in the pandemic compared to patients in the lowest as measured by the mean number of days from January 1, 2020, to the date of admission (160.6 [96.4] vs 222.0 [107.0]; P < .001).
Characteristics of Patients With COVID-19 in Study Hospitals by Social Vulnerability Index Quartiles (n = 105 560).

Note. Percentages may not add to 100 due to rounding.
SD = Standard deviation; SVI = Social Vulnerability Index.
Characteristics of the 238 study hospitals and the distribution of patients in them by SVI quartile are presented in Table 2. On average, patients in the highest SVI quartile were admitted to hospitals with lower mean (SD) nurse work environment scores compared to patients in the lowest (2.58 [0.21] vs 2.72[0.23]; P < .001). Compared to patients in the lowest SVI quartile, patients in the highest were more likely to be admitted to large (23 038 [86.4%] vs 19 314 [73.4%]), major teaching (17 836 [66.9%] vs 7210 [27.4%]) hospitals, with high technology capability (16 081 [60.3%] vs 14 382 [54.6%]). While the hospital sample was evenly distributed between NY (112 [47.1%]) and IL (126 [52.9%]), most patients in the highest SVI quartile (21 292 [79.8%]) were admitted to hospitals in NY.
Characteristics of Study Hospitals by Social Vulnerability Index Quartiles of Patients Treated in Them.

Note. SD = standard deviation; PES-5 = Practice Environment Scale-5 item.
Table 3 provides unadjusted and adjusted odds ratios (ORs) indicating the effects of SVI quartile and work environment on 30-day inpatient mortality among Medicare beneficiaries diagnosed with COVID-19. Across all models, there was a significant association between SVI quartile and patient mortality, with higher quartiles being associated with higher odds of mortality. In the unadjusted model (Model 1), patients in the highest quartile experienced 47% higher odds of mortality within 30 days of admission compared to patients in the lowest quartile (OR, 1.47; 95% CI, 1.30-1.67; P < .001). This effect was attenuated, but not eliminated, after controlling for patient characteristics in Model 2 (OR, 1.29, 95% CI 1.16-1.43; P < .001), hospital characteristics in Model 3 (OR, 1.17; 95% CI, 1.07-1.27; P < .001), and nurse work environment in Model 4 (OR, 1.14; 95% CI, 1.05-1.23; P < .01). For all patients, a 1 SD increase in the nurse work environment score was associated with a 11% decrease in the odds of 30-day inpatient mortality (OR, 0.89; 95% CI, 0.84-0.95; P < .001). In Model 5, a statistically significant interaction was found between the highest SVI quartile and the nurse work environment (OR, 0.86; 95% CI, 0.76-0.98; P < .05). The interaction implies that the effect of nurse work environment improvement on mortality was decidedly greater for patients in the highest quartile (odds ratio = 0.86 × 0.94 = 0.80) compared to patients in the lowest quartile (OR, 0.94). This fully adjusted model had a c-statistic of 0.691.
Odds Ratios Indicating the Effects of Social Vulnerability Index (SVI) Quartile and Nurse Work Environment on 30-Day In-Hospital Mortality Among Medicare Beneficiaries with a Diagnosis of COVID-19 (n = 105 560).

Note. All models utilize multivariable logistic regression that account for clustering within hospitals. Higher quartiles of SVI indicate greater social vulnerability. Patient characteristics include age (categorical), sex, race/ethnicity, Elixhauser Comorbidity Index, and number of days between January 1, 2020 and date of admission. Hospital characteristics include teaching status, technology capability (ability to perform open-heart surgery and/or organ transplants), size, core-based statistical area (metropolitan, micropolitan, rural), and state. The PES-5 (nurse work environment) variable was standardized; thus, the associated coefficient reflects the change in the odds of mortality associated with a one standard deviation increase in the PES-5 score.
CI = confidence interval; OR = odds ratio; SVI = Social Vulnerability Index; PES-5 = Practice Environment Scale-5 item.
P < .05. **P < .01. ***P < .001.
To facilitate the interpretation of the interaction, we calculated adjusted predicted probabilities of 30-day inpatient mortality for patients in each SVI quartile under 3 different conditions of the nurse work environment: (1) 1 SD below the mean, (2) at the mean, and (3) 1 SD above the mean. Figure 1 shows that, while more favorable nurse work environments may reduce the likelihood of death for patients in all SVI quartiles, there was a pronounced outcomes advantage for patients in the highest SVI quartile. The figure suggests that the probability of death for patients in the highest SVI quartile decreased from approximately 30% in the hospitals with lower nurse work environment scores to 22% in hospitals with higher work environment scores. If all study hospitals had been in the top quartile of the nurse work environment score prior to the pandemic, we estimated that 585 in-hospital deaths associated with COVID-19 could have been potentially avoided, with the largest number (n = 291) among patients in the highest SVI quartile (Table 4).
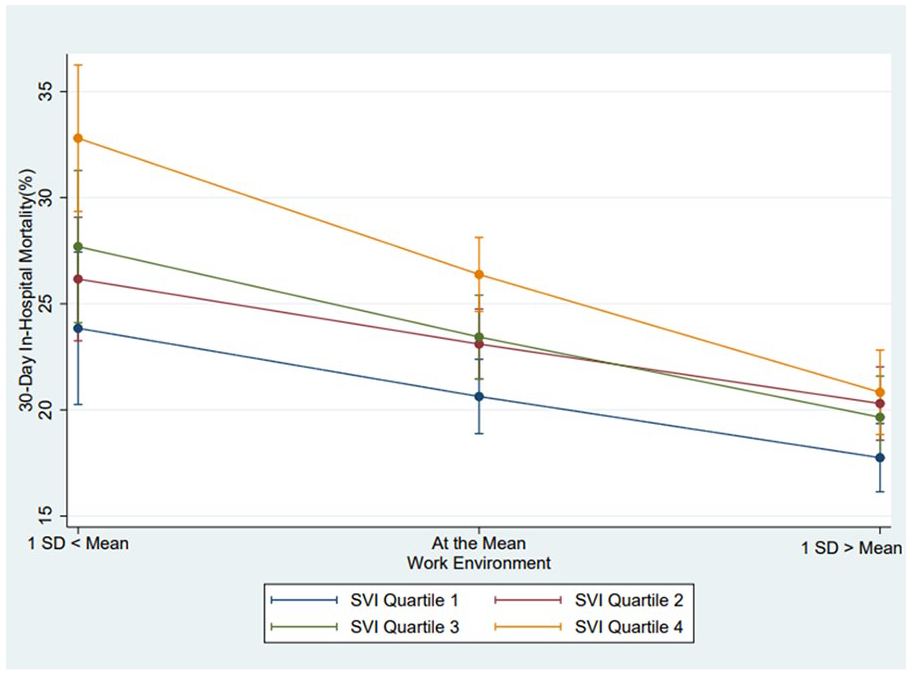
Work environment was measured using a short form of the Practice Environment Scale of the Nursing Work Index (PES-5), mean (SD) = 2.67 (0.28).
Number of Potentially Avoidable Deaths Among Medicare Beneficiaries Hospitalized with COVID-19 if Study Hospitals Were in the Top Quartile of Nurse Work Environments by Social Vulnerability.

Note. Estimates derived from fully adjusted model where all patients were simulated to have been admitted to hospitals with a work environment score at or above the 75th percentile.
Discussion
In this large cross-sectional study of 105 560 Medicare beneficiaries in 238 hospitals, we found that adults admitted to hospitals from the most socially vulnerable communities experienced nearly 50% higher risk of death compared to those in the least. This disparity narrowed when they were cared for in hospitals with high quality nurse work environments. These results suggest that had the most socially vulnerable patients been cared for in hospitals with high quality work environments, nearly 300 deaths could have been avoided. Despite the evidence linking nurse work environments to patient outcomes,10,12 we observed that, on average, the most socially vulnerable COVID-19 patients in New York and Illinois were cared for in hospitals with lower quality nurse work environments. In the early days of the pandemic, images of nurses without adequate personal protective equipment (PPE) and a lack of ventilators made headlines. Nurses’ assessments of work environments taken in the days prior to the first COVID-19 wave in March 2020 corroborate this lack of hospital preparedness, which also likely hindered their ability to meet the needs of the most socially vulnerable patients.
Research on COVID-19 disparities among patients residing in socially disadvantaged communities is extensive though it has focused largely on the role of patient and neighborhood factors.1,20,25-27 Like others,5,30 we note a lowered risk of mortality once accounting for sociodemographic characteristics suggesting that hospitalized patients with COVID-19 from more socially vulnerable neighborhoods may have more intensive care needs during hospitalization. Our study extends this prior work in 2 important ways. First, we used sequential hierarchical modeling instead of hospital-level random effects to examine the independent contribution of hospital characteristics to mortality disparities among socially vulnerable patients with COVID-19. Using this approach, we found that mortality among patients from the most socially vulnerable neighborhoods was significantly reduced after accounting for hospital characteristics, suggesting that these patients were admitted to different types of hospitals.
Second, our study is among the first to consider the quality of the nurse work environment as a contributing factor to COVID-19 outcome disparities. While others have documented significant variation in nurse work environment quality across hospitals immediately before the pandemic,13,14 we find that these differences may have been particularly consequential for patients with COVID-19 who lived in socially vulnerable communities. We found that the predicted probability of death for patients with COVID-19 admitted from the most socially vulnerable neighborhoods was reduced by over 20% when treated in a hospital with a better work environment, as opposed to a poorer one. Our nurse work environment measure captures the key dimensions of collegial interprofessional relationships, adequate staffing and resources, and supportive management—all of which have been named by physicians and nurses as important elements of care delivery during the pandemic.29,30 Here we note the importance of these aspects of the work environment specifically when caring for patients hospitalized from socially vulnerable communities who may require more intensive discharge preparation, care coordination, and connections to community-based resources. Like others,9,31 our findings suggest that socially vulnerable patients are more likely to be cared for in settings with unfavorable nurse work environments, leading to care delays and omissions that contribute to disparate outcomes.
Our study also holds important implications for racial and ethnic minorities who experienced disproportionately higher rates of mortality during the pandemic.4,32 The U.S. healthcare system reflects a historical framework of law and policy marked by racism and segregation.33-35 Despite progress, many facilities remain segregated and some care for much larger shares of minority and low-income patients. 36 In our sample, Black patients comprised the largest racial group (39.1%) in the highest SVI quartile and hence were treated less often in hospitals with better nurse work environments. Others have noted that mortality disparities for Black patients during the pandemic were largely explained by the hospitals where they received care. 4 Our findings suggest that the most socially vulnerable, including minoritized and economically disadvantaged patients, were cared for in settings that were under-resourced at the onset of the pandemic and thus, were more susceptible to the disruptions in care delivery posed by COVID-19. Our findings highlight the importance of ensuring an adequate nursing infrastructure as a part of public health emergency preparedness, specifically in hospitals serving communities with greater social needs.
Conclusion
The results of this study suggest that the quality of the nurse work environment was associated with 30-day inpatient mortality among Medicare beneficiaries admitted from socially vulnerable communities with COVID-19. Our findings suggest that members of socially vulnerable communities were hardest hit by COVID-19 and that hundreds of these lives could have been saved if adequate nursing resources were in place prior to the pandemic. Strengthening the quality of nurse work environments may help to reduce health disparities and should be considered in public health emergency planning, specifically in hospitals serving socially vulnerable communities.
Supplemental Material
sj-docx-1-inq-10.1177_00469580241284959 – Supplemental material for COVID-19 Mortality Disparities Among Socially Vulnerable Medicare Beneficiaries Associated With the Quality of Nurse Work Environments in U.S. Hospitals
Supplemental material, sj-docx-1-inq-10.1177_00469580241284959 for COVID-19 Mortality Disparities Among Socially Vulnerable Medicare Beneficiaries Associated With the Quality of Nurse Work Environments in U.S. Hospitals by Margo Brooks Carthon, Jane Muir, Christin Iroegbu, Christine Langston, Kelvin Amenyedor, Jacqueline Nikpour, Karen B. Lasater, Matthew McHugh and Ann Kutney-Lee in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors wish to thank Timothy Cheney (blinded for review) for his statistical and methodological expertise.
Correction (October 2024):
The article is updated with affiliation of the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by grants from the National Institutes of Nursing Research (R01NR020471; R01NR014855; T32NR007104), the Agency for Healthcare Research and Quality (R01HS028978), and the National Council of State Boards of Nursing. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health, the Department of Veterans Affairs, or the U.S. Government.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.