
Abstract
Emergency department nurses may fail to see medical items in emergency cart drawers, such as syringes and tubes, while handling emergency situations, which can often contribute to a delay in managing the case. This is a phenomenon known as Looked-but-failed-to-see (LBFTS) and occurs when the observer fails to detect a visible visual stimulus among various other stimuli. LBFTS is a group of human errors, including inattentional blindness (IB), satisfaction of search, and biased search processes, and is associated with constraints on human visual processing. LBFTS has been studied extensively in the fields of aviation, military, radiology, and road safety; however, the role of LBFTS in hospital ED has generally been overlooked. Hence, a key aim of this study was to investigate the possibility of the occurrence of LBFTS among ED nurses while searching for a particular medical item during a real-life emergency. An observational cross-sectional blinded study was conducted to determine the occurrence of LBFTS in a real-life visual search task during resuscitation cases in ED. The A-B-C (antecedent-behavior-consequence) observation and recording naturalistic observation technique was used. A total of 45 ED nurses who were assigned to either the crash cart or the intubation trolley at the time of data collection agreed to participate and were included in the analysis. The results revealed that LBFTS accounted for 66% of the cases where emergency items were brought from another location. Participants missed seeing an item, although the item was directly in front of their eyes. Factors such as the perception of cognitive workload at the time of data collection positively impacted the increase in LBFTS (P = .021). Taken together, the results of the present study and recent visual studies support the occurrence of LBFTS among nurses working in ED. Devising successful strategies to reduce this phenomenon could translate directly into saved lives.
LBFTS errors suggest a common underlying cause for multiple failures, whether it is overlooking an unexpected object or a clearly defined search target.
A scientific approach to exploring the concept of LBFTS within the emergency department is crucial to guide the development of practical strategies that could directly translate into saved lives. This study contributes to this approach by empirically investigating LBFTS among nurses in the ED context, demonstrating the phenomenon’s significance, and emphasizing the need for further investigation.
According to the current study findings and previous research within the context of an ED, this study has taken steps toward integrating the concept of LBFTS into nursing clinical practice. Understanding the likelihood that an emergency nurse may fail to notice emergency items holds substantial safety and quality value and has important applications to everyday nursing practice. In the fast-paced, multitasking, and dynamic emergency department (ED) work environment, nurses need to maintain a high level of attention focus.
Introduction
A visual search is an everyday task of nurses’ work and ranges from searching for a specific medical item in the supply room to monitoring clinical changes in patient condition. The visual search paradigm typically encompasses an active scan of a visual scene to identify a particular item or feature among a set of competitive items. 1 Consider the activity of checking emergency mobile units. Nurses’ familiarity with emergency cart drawers allows them to anticipate where a particular item is likely to be found. Indeed, medication tends to be found in the first drawer and not in the second drawer. Adult intubation supplies tend to be in the third drawer. According to cognition scientists, searching for an item where the location is known is more effective than searching for an item where the location is not. 2 This type of knowledge can rapidly guide attention focus during a search activity toward parts of the scene that have a high likelihood of having the item. However, this is not always true. Nurses may fail to see and pick up what should have been visible on familiar visual displays. In many cases, nurses cannot explain this observation error and have been labeled negligent or careless, although these types of errors can be made by cared-for, experienced, and vigilant nurses.3,4
Readers interested in cognitive science are likely familiar with the classic gorilla experiments conducted by Simons and Chabris
5
;
Observers are instructed to count how many times the white-shirted team passes the ball as they watch two groups of actors. Then, in the middle of the game, an actor in a gorilla suit enters, pounds on her chest, and leaves.
In the gorilla example, approximately 50% of observers fail to report the presence of the gorilla when asked after the video clip finishes. Now, let’s consider this example: a radiologist has reported one lesion and failed to report further tumor lesions. 6 Another example is carrying out a standard visual search task, like spotting a C among numerous Gs. Around 5% to 10% of observers failed to see the visible “C.”1,7 In the 3 examples, the errors may seem different, but they have the same outcome, so “what do they have in common”?
The gorilla error is recognized as a typical inattentional blindness (IB) a condition that occurs occasionally when an observer fails to see a visible unexpected item. 8 The tumor lesions error might be considered a “satisfaction of search” error, 1 a condition that occurs once a lesion is recognized and the search process is terminated early before searching for another lesion takes place. 6 Searching for the “C” example is suggested as a biased search process a condition that occurs when more target-similar unsegmented regions of the background are relatively neglected. 9 Although these phenomena related to failure to notice a visible visual stimulus are studied as different visual search errors, each of these is an example of a Looked-but-failed-to-see (LBFTS), a human error associated with constraints on human visual processing rather than a problem in vision. 10
LBFTS can be described as a failure to detect a visible visual stimulus among various other stimuli. 1 Wolfe 1 argued that LBFTS-related phenomena can happen in an “un-deliberated setting” when the attention of the observer is misdirected to something else (eg, a missed gorilla); it might happen in a “deliberate setting” as when the observer is purposely searching for an object (eg, a missed C) and some might occur in between when the nurse misses significant clinical signs. For example, a nurse, monitoring a patient, commits a potentially risky LBFTS error if he misses visible evidence of clinical deterioration. 4 Another example is a radiologist, searching for a lung lesion, commits a potentially dangerous LBFTS error if they miss visible evidence of rib fracture. 1
Collectively, phenomena related to LBFTS can be a key source of medical error. 11
The LBFTS related phenomena have been studied extensively in the aviation industry, 12 in the military, 13 and road safety. 14 IB has grown in interest because these industries believe that visual failure rather than mechanical failure can dictate the outcome of an event. The factors contributing to the occurrence of LBFTS related phenomena, safety implications and strategies for reducing its occurrence have been well described in the fields of aviation, 15 military, 16 and road safety. 17 Despite this growing understanding of LBFTS in these fields, the role of LBFTS in the healthcare setting in general and in emergency departments has been overlooked. 4
The visual search pattern has become essential to the study of safe nursing practices and has been explored in studies ranging from simple visual scans 18 to studies of individual differences in visual attention focus. 19 A few recent studies have intended to narrow the gap in our understanding of nurses’ visual search behavior between the assumption of what we think of as failure in nurses’ practice and occasional existing LBFTS. Al-Moteri et al 20 found that nurses in general departments failed to notice the salient features of patients and therefore failed to act as needed. In emergency departments (EDs), the problem is perhaps worse. The ED is the most stressful and challenging work environment, increasing the possibility of LBFTS. Strategies such as “advanced life support” (ALS) have been used to ensure that all emergency team members working in the ED follow the same guidelines. 21 However, the focus is on technical skills, and visual search skills are not considered in these strategies.4,21 Failure of patients to appropriately acknowledge the presence of an IB or other visual search failures can occur. Hence, a key aim of this study was to investigate the possibility of the occurrence of LBFTS among ED nurses while searching for a particular medical item during a real-life emergency intervention.
Methods
An observational cross-sectional blinded study was conducted to determine the occurrence of LBFTS in a real-life visual search task that typically involved an active search of the drawers of emergency mobile trolleys for a particular emergency item. Cross-sectional studies are needed when investigators observe a participant at one particular point in time and no data are collected multiple times. The study was conducted for 4 months, from February to June 2023. The choice of the period was intentional and related to the Umrah season. During the Umrah season, healthcare professionals deal with and are responsible for a large number of people who are gathering for religious and spiritual purposes. 22
Participants and Setting
A total of 103 nurses working in an emergency department (ED) of a large public hospital in the Madinah region were invited and recruited during regular emergency department meetings. In general, the hospital has 500 beds and accepts approximately 9021 inpatients annually and approximately 250 emergency patients per day. During the Umrah season, 350 to 520 emergency patients per day may visit the ED. Participants were considered eligible if they were assigned to the resuscitation room. Those who were assigned to the triage room, procedure room, and consultation room were considered illegible and were excluded.
Emergency Mobile Trolleys
The ED includes 2 types of emergency mobile trolleys: crash carts and intubation trolleys. These emergency mobile trolleys are checked and maintained regularly to ensure that their contents are available when needed. The checkup process includes but is not limited to ensuring that the trolleys are fully equipped, that the medications have not expired, that the defibrillator is functioning well and that the battery is charged.
Visual Search Error
During some emergency situations, nurses who are assigned to the emergency trolley may find that items are missing from the cart (eg, syringes, EET sizes, oropharyngeal airway sizes, fluid, IV tubing, plaster, lidocaine gel, Yankauer suction tip), which forces the nurse to travel to the ED storage room to collect that specific item (Figure 1). Due to the criticality of the situation, any delay resulting from the time the nurse spends bringing the item from the storage unit could have a significant impact on patient safety.
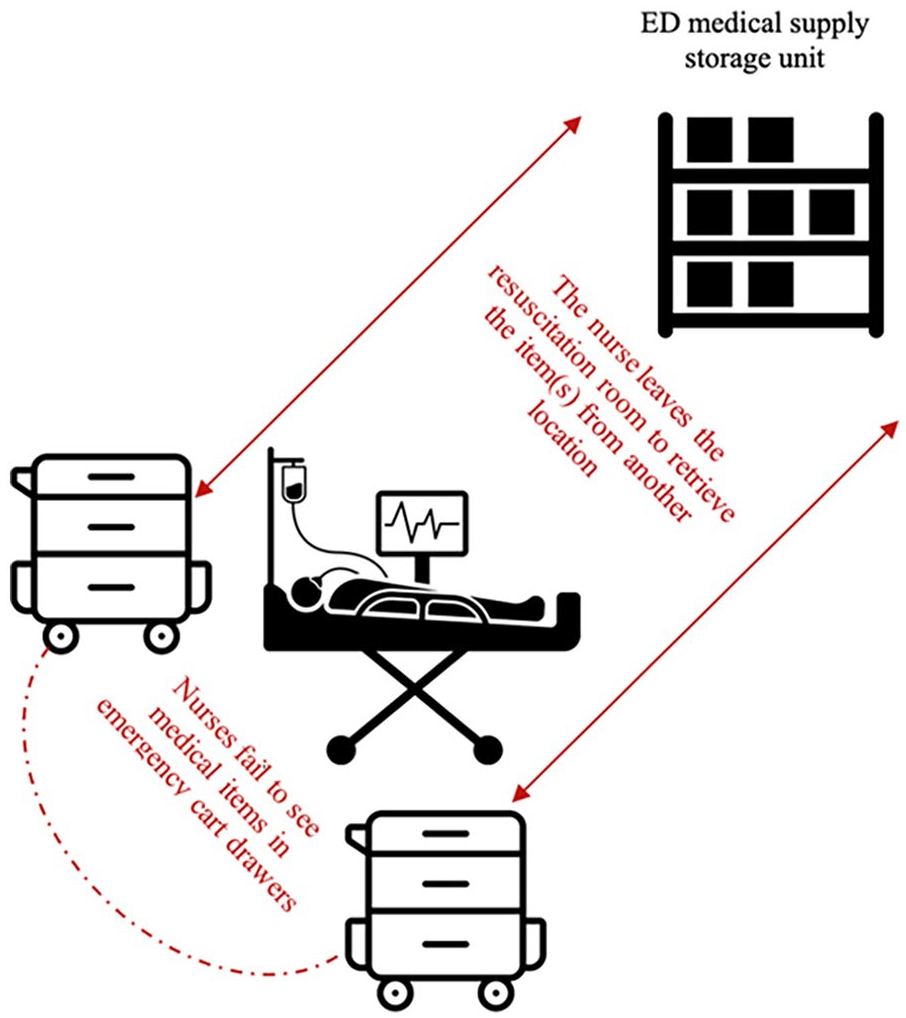
Nurses’ travel path when medical items are unavailable.
Data Collection Tool
The data collection tools included 3 sections: general demographic data, descriptions of work conditions, and an observation checklist. In section 1, the demographic survey collected information on age group, sex, work experience in the ED, and qualifications. In section 2, data were gathered on 3 items related to work conditions, namely, the shift, the workload at the time of data collection, and the frequency of missing items per month—which refer to the number of times specific medical items are reported as missing from emergency trolleys during the handling of an emergency situation within a 1-month period. This measure helps to track and quantify how often necessary supplies are missed by nurses when needed, which can impact the efficiency and safety of patient care in emergency settings. In section 3, data were collected on 3 items related to observation, which involved (i) the observation checklist, consisting of a list of all items available in emergency care trolleys, (ii) direct observation of participants’ active search behavior, and (iii) a confirmation item where the observer checks the availability of the item in the trolley being used.
Observation Technique
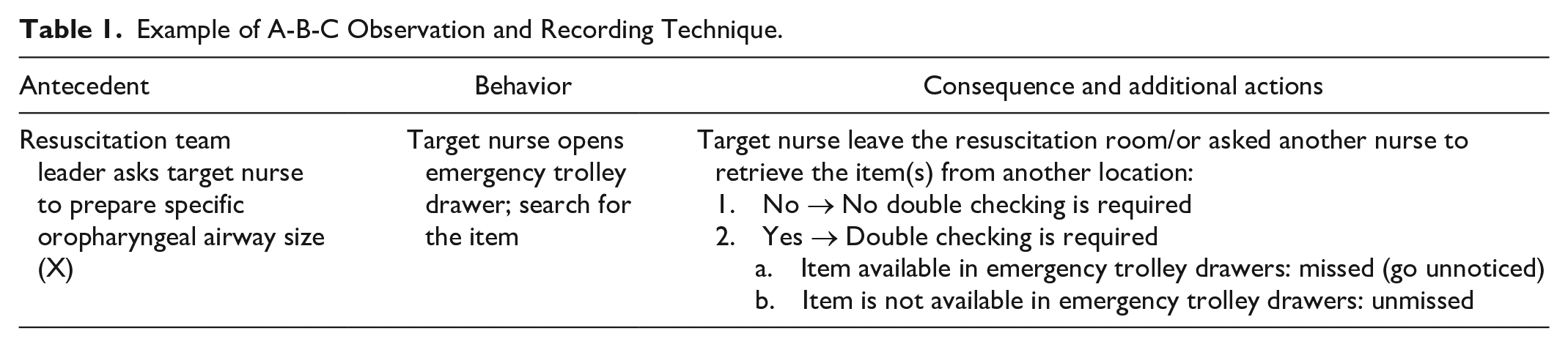
The A-B-C (antecedent-behavior-consequence) observation and recording naturalistic observation technique was used. 23 The A-B-C technique is simple, straightforward, and easily applied and understood (Table 1). The observer simply observed the occurrences of leaving the resuscitation room and/or sending a colleague to collect the medical item and record the result using Yes/No.
Example of A-B-C Observation and Recording Technique.
Procedure
The purpose and process of the data collection were explained to the ED administration with granted permission. In ED meetings, the primary researcher frequently explained the study to all nurses, and a somewhat misleading rationale was given for the study. Participants were informed that the study aimed to investigate the impact of an emergency medical supply shortage on patient care outcomes. This approach was essential for preventing the “hawthorne effect” and eliminating any change in participants’ behavior that could impact patient safety during the emergency event. The Hawthorne effect is defined as a “type of human behavior reactivity in which individuals modify an aspect of their behavior in response to their awareness of being observed.” 24 The actual rationale was presented to participants after the study was completed, after which nurses could decline to participate in the data collection. A verbal informed consent was sufficient to be enrolled as a participant.
Conducting blinded observation
The primary researcher is a full-time nurse in the ED where the study took place; thus, he is well-integrated with the everyday work of the emergency department. When a call for an emergency situation is initiated to treat acutely unwell ED patients, the primary researcher shadowed the target nurse on the medical emergency team (MET). The primary researcher made his observations as unobtrusively as possible so that participants were unaware that they were being observed and consequently changed their behaviors. Immediately after the emergency situation, participants were shown the emergency checklist and asked a direct “Yes/No” question if the item they had traveled to bring from another place was listed in the checklist; participants looked at the written checklist and gave their answer. The participants were then asked how confident they were in their answer (very, somewhat, not at all) and were asked to complete the demographic survey. This was followed by double-checking of the trolley content; both the researcher and the participant who had been observed together confirmed or denied the presence/absence of the item in the emergency mobile trolleys, and the participant’s comment was recorded on the observational checklist. For ethical reasons, once the data collection period ended and no further data collection was needed, all the observed nurses who initially gave their verbal consent were gathered, and the study purpose was disclosed and fully exposed; nurses were then allowed to withdraw their participation. Out of the 48 nurses being observed, 45 provided written consent, and their data were included in the analysis. No patient information was collected.
Statistical Analysis
The Statistical Package for Software Sciences (SPSS) version 26 (Armonk, New York, IBM Corporation) was used to analyze the data. Categorical variables are presented as numbers and percentages. The relationships between the sociodemographic characteristics and the experiences of the nurses in the Emergency Department during the search tasks for emergency items were determined using Fisher’s exact test. 25 A P value < .05 was considered to indicate statistical significance.
Results
Descriptive Data
A total of 45 ED nurses who were assigned to either the crash cart or the intubation trolley at the time of data collection agreed to participate and were included in the analysis. Of these nurses, 91% (n = 41) were female. A total of 96% (n = 43) of the participants were relatively young, ranging from 20 years old to 40 years old. Most of the participants (96%, n = 43) held a bachelor’s degree, and 63.5% (n = 29) had 5 or fewer years of work experience in the ED.
Table 2 shows a descriptive analysis of the nurses’ perceptions of the working conditions at the time of data collection. Nurses’ visual search behaviors were tracked during the morning shift (42%, n = 19), afternoon shift (33%, n = 15) and evening shift (24%, n = 11). Approximately 60% (n = 27) of participants reported encountering 2 to 5 instances of missing items from emergency trolleys while responding to emergency situations in the previous month. Regarding workload, 49% (n = 22) and 29% (n = 13) of the participants perceived the workload as moderately to very stressful, respectively.
Variables Related to Work Conditions at the Time of Data Collection.

LBFTS Occurrence Among ED Nurses
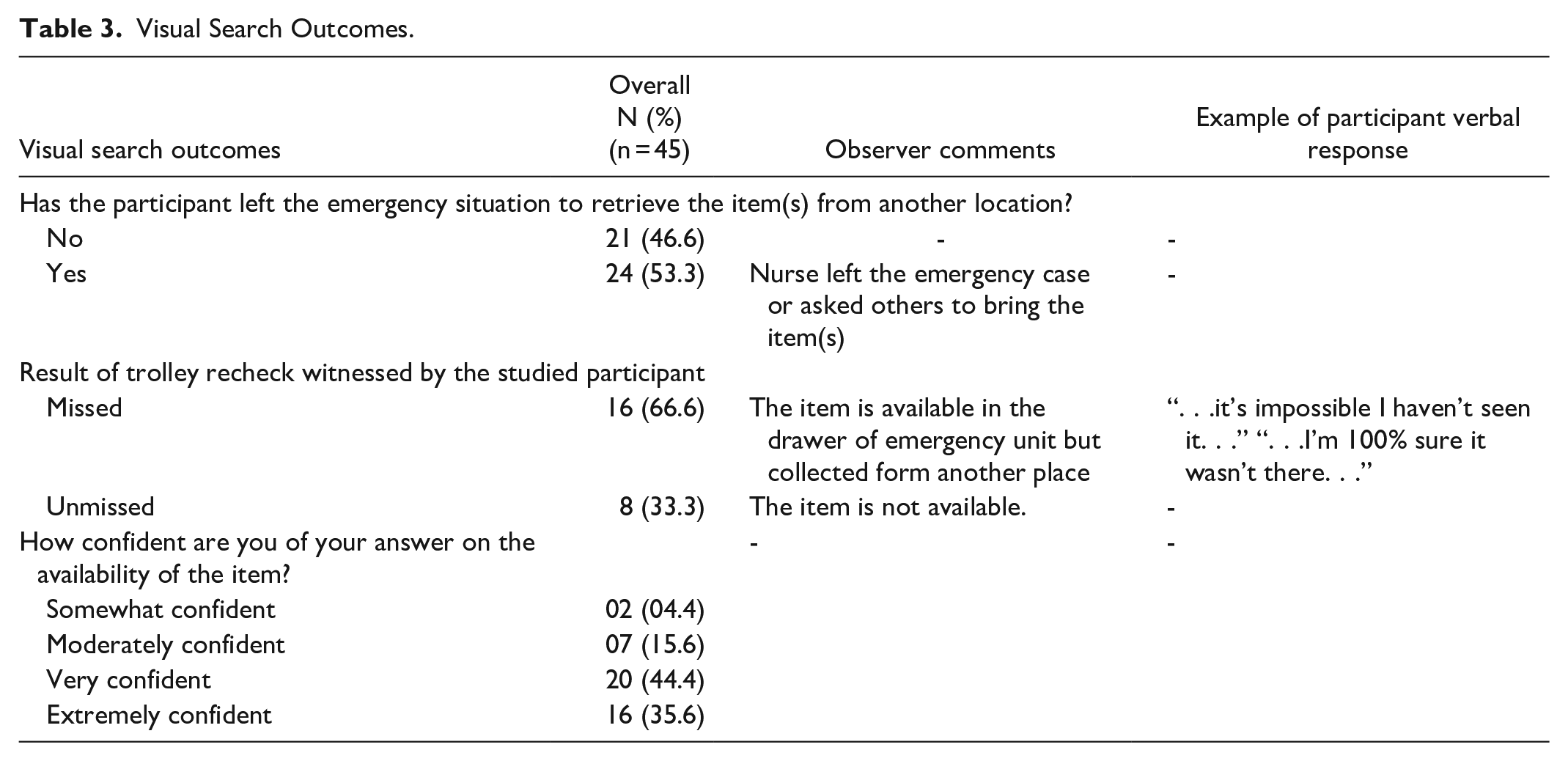
Table 3 shows the results of the visual search outcomes. More than half of the participants (53%, n = 24) left the emergency case or asked another nurse to retrieve the item(s) from another location, either from the medical supply storage room or the nearby mobile emergency trolley. Eighty percent (n = 36) of participants were confident about their answers regarding the availability of the item in the emergency mobile trolley drawers. Among participants who brought the emergency item(s) from another location, 66% (n = 16) missed seeing the item they were searching for, although the item was available in the drawer and directly in front of the participant’s sight indicating the presence of LBFTS. When participants saw the item on the mobile emergency trolley during the double-checking step, they were surprised and found it hard to believe they had missed it.
Visual Search Outcomes.
Relationship Between LBFTS and Demographic Data
Table 4 represents the results of the association analysis between the search behavior outcome (missed vs unmissed) and the other variables. There was a significant association between participants who had missed the item and their perceived workload at the time of data collection as stressful (P = .021). There was also a significant association between participants who had an unmissed item and their perceived confidence (P = .006).
Association Between the Visual Search Outcome and the Different Variables.
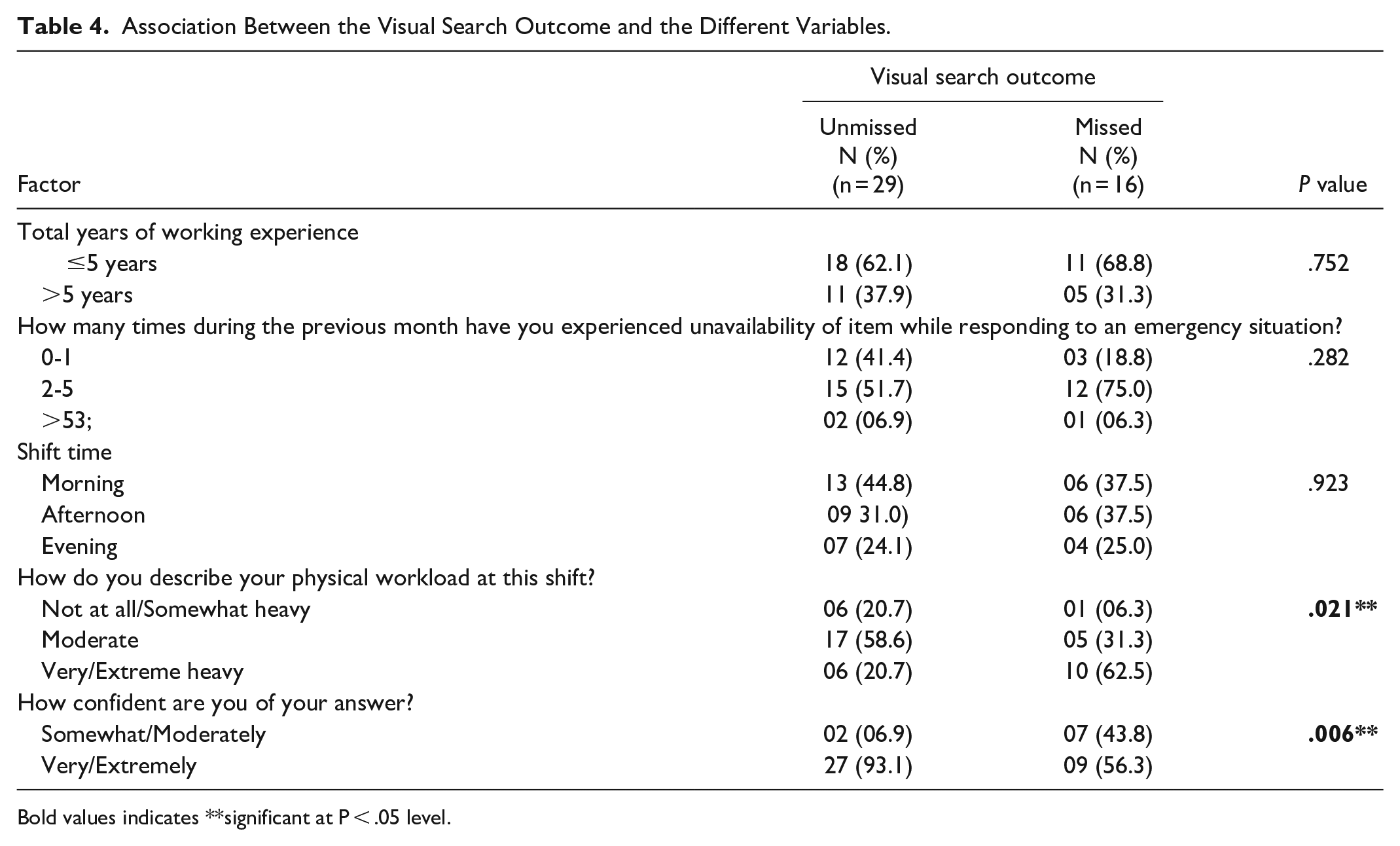
Bold values indicates **significant at P < .05 level.
Discussion
In this study, we aimed to investigate the occurrence of LBFTS among ED nurses while searching for a specific medical item during a real-life emergency intervention. The results of this study showed that LBFTS accounted for 66% of the cases where emergency items were brought from another location. LBFTS-related phenomena are common in both lab experiments and real-life tasks.26,27 Although it is unlikely that these errors can entirely be eliminated, it is still worthwhile to make efforts to reduce them as they hold significant impact potential for interfering with patient safety in the medical field. 28 Several medical cases have ended up in court, with suits for malpractice due to failure to report clinically significant findings that are visible (Brady). 29 Hence, over the last decade, health studies have switched their focus from malpractice as a root for suboptimal care to observation lapses.20,30 Research in nursing practice is now more than ever dedicated to understanding how nurses search for and notice clinical signs within the types of complex nursing working environments that encompass daily work.20,31
In this study, LBFTS errors are not the result of malpractice, but rather the outcome of situations where the normal functioning of the visual search system leads to undesirable results. 32 In the current study, when those participants were confronted by the fact that the item was present, they were surprised. Taken together, the results of the present study and recent studies of visual search in the healthcare discipline support the occurrence of LBFTS among nurses working in the ED.20,33,34 The missed items in the current study do not mean that there was malpractice. The fast-paced, multitasking, and highly dynamic emergency department (ED) work environment often can lead to LBFTS, which can cause the failure of rescue and lead to potential adverse events. 31 In the current study, there was a significant relationship between LBFTS and participants’ perception of cognitive workload at the time of data collection (P = .021). This is in line with the literature as nurses who perform complex activities filled with distractions, their attentional field may be distracted, and some information may go unnoticed. 34
These LBFTS-related phenomena could have serious consequences in critical emergency situations where an item is essential for saving a patient’s life. This includes emergency triage screening to identify patient needs and immediate life-saving interventions. 20 It is also critical to inspect crash carts to ensure a prompt response and effective management of patients’ life-threatening issues. 33
Given that such errors can lead to adverse consequences, several strategies have been attempted: (1) enhancing memory for category targets 7 ; (2) implementing a comprehensive checklist procedure that required participants to explicitly respond to the presence or absence of each type of target 7 ; (3) asking a colleague to assist in searching for the item as a second pair of eyes. Out of these measures, only the full second pair of eyes technique may decrease errors related to categorical targets.
Al-Moteri et al 35 reported that playing attention games significantly improved nurses’ clinical observation skills by enhancing their attention focus. Devising successful strategies to reduce the LBFTS could translate directly into lives saved. Furthermore, practicing under stressful complex working environments is being combined into training programs to maximize individuals’ ability to focus their attention and ensure safe performance.36,37 Future studies must focus on developing a model of LBFTS that provides healthcare policymakers with some of the tools they need to understand it and work to reduce it.
Limitation
This study has some limitations. Firstly, the sample used in the study may not accurately represent the entire population, and the data collected from a specific geographical area may not be enough for statistical generalization. Although the sample size was consistent with similar studies, a formal sample size calculation was not performed. Consequently, further research is required with larger sample sizes and different geographical locations. Secondly, observational studies per se are limited by a lack of randomization, making it difficult to rule out bias. Thirdly, data analysis in the current study may not be deep enough. The relationship between different variables was not investigated thoroughly due to the primary focus of the study was to identify the occurrence of LBFTS. Additional comprehensive studies are required. Despite these limitations, we believe that the insights gained from this study can be appreciated for practice, research, and education. Fourthly, this study is the first to assess the occurrence of LBFTS phenomena in real-life tasks, and the lack of laboratory manipulation made researchers unsure which LBFTS phenomenon they measured: is it “IB,” “satisfaction of search error,” “biased search,” or “search failure”? More studies may provide more valid evidence.
Conclusion
In the present study, the failure to notice required medical items in emergency trolleys was the result of human visual search limitations, where the complex and stressful environment of the ED makes nurses vulnerable to missing a medical item that is “right in front of their eyes.” This phenomenon is referred to as LBFTS, highlighting that errors resulting from missing medical items are not always a form of malpractice. Given that such errors can lead to adverse consequences, future research must focus on developing a model of LBFTS that provides healthcare policymakers with the tools needed to understand and prevent this phenomenon. Additionally, future studies should explore educational strategies and practical interventions to mitigate LBFTS in clinical settings.
Footnotes
Acknowledgements
The authors extend their appreciation to Taif University, Saudi Arabia, for supporting this work through project number (TU-DSPP-2024-282). The authors wish also to express their grateful to the nurses who participated in this study.
Author Contributions
All authors contributed in conceptualization, formal analysis, writing—original draft.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Taif University, Saudi Arabia, Project No. (TU-DSPP-2024-282).
Ethical Approval
Permission to conduct the study was obtained on 19/01/2023 from the Madinah Health Cluster Scientific Research Ethics Committee (IRB23-005).
Consent
Initially, verbal informed consent was collected, followed by written informed consent from each participant before their data was included in the current study’s analysis.