
Abstract
According to the Centers for Disease Control and Prevention, the opioid epidemic remains a major issue in the United States, with over 80,000 deaths attributed to opioids in 2021. This public health crisis continues to impact communities across the country, highlighting the need for intervention and reflecting the nation’s failed attempts at prohibition through criminalization to reduce opioid use. Harm reduction methodshave proven to be effective in preventing adverse health outcomes and promoting the overall well-being of individuals with opioid use disorders. However, significant gaps remain in the universal implementation by healthcare providers. This review evaluated the PICOT question: What barriers exist among providers in implementing evidence-based harm reduction methods for adults aged 18 years and older, with and without opioid use disorders? A literature search was conducted across databases using key words which included: “Health care provider,” “Physician,” “Pharmacist,” “Harm reduction,” “Harm reduction programs,” “Naloxone,” “Buprenorphine-naloxone induction,” “Methadone,” “Naloxone take home kits,” “Stigma,” “Barriers,” “Negative perception,” “Refusal.” The inclusion criteria focused on identifying provider barriers, specifically regarding opioid use. . The review revealed 3 major barriers that exist among providers to prevent harm reduction: stigma, lack of education and knowledge, and lack of access to resources for long-term management. Recognizing these barriers among providers can help organizations develop targeted interventions to overcome them, leading to widespread adoption of opioid harm reduction methods. The results provide an initial narrative review of the current evidence at the time of the authors search to inform practice, policy, and future research.
The opioid epidemic continues to be a major public health issue. Harm reduction strategiesare evidence-based methods proven to reduce negative consequences of substance use and aide in relieving social determinants of health associated with drug use. However, despite proven effectiveness and promotion of opioid harm reduction methods, significant inconsistences remain regarding consistent implementation and practice at the community and organizational level.
This narrative review was conducted August to December 2022. The review synthesizes research on identifying specific barriers among healthcare providers in implementing harm reduction methods for opioid use. The review identifies 3 major barriers: stigma, lack of knowledge/training, and lack of access to treatment resources. The review provides a framework to encourage further systematic review of the topic and evidence-based interventions to address these barriers.
This review highlights the need for community and organizational assessment of potential provider barrier in the implementation of opioid harm reduction methods. The review identifies provider barriers and encourages the consideration of implementing programs to address stigma reduction, provider education and easily accessible resources for providers to link patients with treatment programs and community support. Addressing these needs can help increase the adoption of harm reduction practices. It also promotes a need for policy changes to reduce structural stigma and increase funding for more comprehensiveprograms which can address these barriers.
Introduction
The opioid epidemic continues to be a significant problem in the United States (U.S.), with 80,816 deaths related to opioids in 2021. 1 The use of prescription opioids increased in the 1990s due to promotion by pharmaceutical companies for their safety and effectiveness, and minimization of concerns for potential abuse and dependence. 2 However, the dissemination of false information has led to widespread opioid prescriptions, ultimately causing a significant increase in opioid use, opioid-related overdose deaths, and negative health outcomes including transmission of blood-borne pathogens, infection, and dependence (pp. 187–189). 3 In 2016, the Centers for Disease Control and Prevention (CDC) 2 reported an alarming number of 47,600 opioid-related deaths, prompting the White House to declare the opioid crisis a public health emergency. The U.S. has changed its approach to managing the opioid crisis by moving away from ineffective abstinence-based programs such as prohibition and punitive strategies such as legal sanctions toward harm reduction methods. These include supervised injection sites (SIS), distribution of take-home naloxone kits, safe syringe programs (SSP), and medication-assisted treatment (MAT), such as buprenorphine-naloxone or methadone induction.
According to Denis-Lalonde et al, 4 harm reduction encompasses a broad range of concepts and practices and can be considered a philosophy, movement, framework, strategy, approach, perspective, intervention, program, goal, and measure. Harm reduction aims to reduce the social, health, and legal impacts associated with a variety of high-risk behaviors, including drug use, gambling, sex work, and other risky behaviors by addressing both individual needs and social determinants of health which coincide with high-risk behaviors. 4 Harm reduction does not condemn these individuals but instead accepts people for “where they’re at” and empowers them to meet their own goals by meeting them with compassion instead of judgment.
However, despite numerous evidence-based studies showing the effectiveness of harm reduction methods, such as MAT and take-home naloxone kits, significant inconsistencies remain between national opioid use patterns and strategies to encourage their universal implementation. 5 CDC data from 2018, 2 revealed that only 1 naloxone prescription was dispensed for every 70 high-dose opioid prescriptions, and health care providers prescribed only 1.5 take-home naloxone kits for every 100 high-dose opioid prescriptions. This discrepancy highlights the need to identify barriers that exist among providers in implementing evidence-based harm reduction methods.
Although various harm reduction methods, such as MAT and take-home naloxone kits, are universally available to providers, it is unclear what barriers prevent their implementation. Additionally, it is unknown which provider specific barriers contribute to the hinderance of this harm reduction initiative. . Without identifying the specific barriers that providers experience,, it is difficult for organizations to create targeted strategies to address these barriers and improve widespread adoption. Our narrative review aimed to evaluate the following question: What barriers exist among healthcare providers in implementing evidence-based harm reduction methods?
Methods
The intention of this review was to provide an overview of the available literature at the time of the search to answer the authors’ PICOT question. Articles considered for review concentrated specifically on identified provider barriers of opioid harm reduction programs. The study was not registered with PROSPERO/INPLASY as it was not a systematic review of all relevant research. Exclusion criteria was applied to articles involving individuals below the age of 18 defined as pediatric patients, those studies which took place outside of North America and articles that focused on polysubstance use. Articles considered for review were based on relevance to the topic of provider barriers and the implementation of opioid harm reduction programs at the time of the search.
A literature search was conducted from August 2022 to December 2022 using databases PubMed, and Google Scholar. Key words were chosen based on the authors’ experiences in this topic area as psychiatric mental health professionals. Boolean phrases such as “OR” and “AND” were used with the following key words which included the following: “Health care provider,” “Physician,” “Pharmacist,” “Harm reduction,” “Harm reduction programs,” “Naloxone,” “Buprenorphine-naloxone induction,” “Suboxone induction,” “Methadone,” “Naloxone take-home kits,” “Stigma," “Barriers,” “Negative perception,” “Refusal.”
Articles were screened by 2 reviewers independently to ensure relevance and reduce bias. A third reviewer served to resolve conflicts. All articles deemed relevant by at least 2 reviewers were reviewed again with all 4 reviewers, with the aim to further reduce selection bias. No formal tracking methods were used in the selection process.
The narrative approach allowed for flexibility in identifying key themes of provider barriers to answer the reviewers PICOT question. Three reviewers reached consensus using a phenomenological and epistemological approach. The reviewers utilized symbolic interactionism to determine themes and consensus and reliability was ensured by the fourth reviewer who revised conflict. All reviewers were licensed healthcare providers specializingin psychiatry . Saturation was based on reviewer expertise that further articles were unlikely to contribute to the development of new themes.
Results
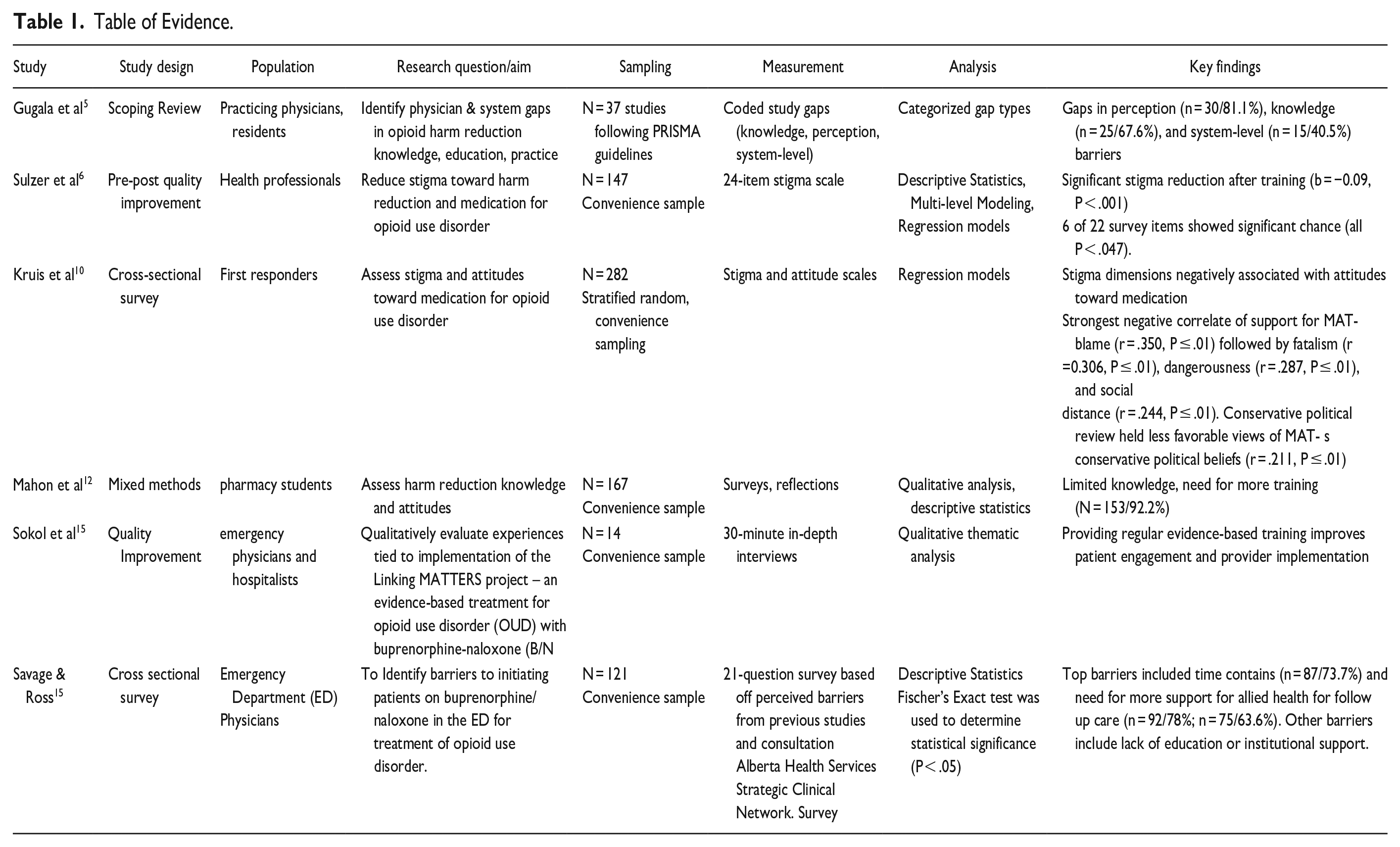
Our search identified 6 articles which met our inclusion criteria. Information collected from each article included study design, study, study populations, research question/aim, sampling, measurable variable method, statistical analysis, and key findings were documented in Table 1.
Table of Evidence.
Discussion
Our review identified 3 main themes through the identification of recurring patterns and commonalities amongst the articles. representing the main barriers to harm reduction: stigma, lack of provider knowledge and training, and lack of access to resources for long-term management as shown in Table 2.
Article Theme.
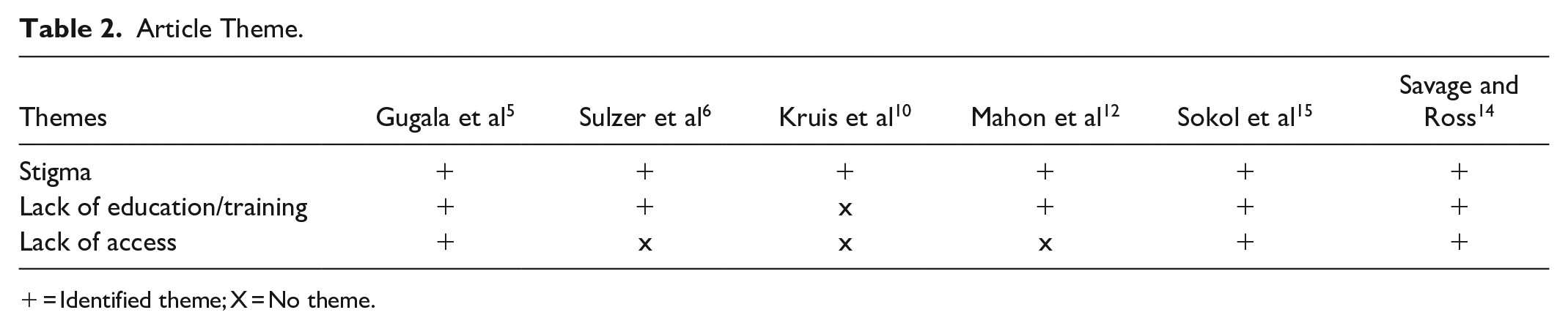
= Identified theme; X = No theme.
Stigma
Stigma presents a significant barrier to the implementation of harm reduction methods. Stigma is defined as a relationship that involves assigning undesirable labels, qualities, and behaviors to a person based on their attributes and stereotypes (pp. 187–189). 3 Stigma often serves as a tool to marginalize and discourage unhealthy behaviors such as problematic substance use, which then unintentionally devalues social groups, consequently leading to inequality and discrimination. 6 Once stigma is established, individuals are less likely to willingly challenge those stigmas, as these perceptions are widely shared and challenging them is often met with resistance. Sulzer et al 6 suggested that, although evidence-based research supports harm reduction methods, stigma may widely impact their implementation.
Stigma can be further subdivided into structural, public, and personal categories. 7 All categories of stigma can pose unique obstacles to providers. Public stigma refers to stigma endorsed by the general population or community. 8 In the U.S., the public stigma of substance use disorders has a long history and is rooted in the notion that substance use disorders are viewed as moral failures. 9 This public stigma has been reinforced by abstinence-based recovery and criminal punishments. Additionally, substance use has been demonized, resulting in discrimination, inequality and stereotypes among certain sociodemographic groups. President Nixon’s War on Drugs in the 1970s promoted abstinence by using criminal punishment as a deterrent to drug use. 2 However, this political narrative, coupled with ongoing substance use in society, has caused further stigmatization. Sociodemographic groups highlighted by the media as substance users are often portrayed as dangerous, which can worsen fear in public perception and further strengthen these stigmas. 9 An analysis of public stigma in a cross-sectional exploratory study among first responders by Kruis et al 10 found that practitioners who perceived individuals with opioid use disorders (IWOD) as dangerous were less likely to implement harm reduction methods. This negative social narrative leads to widespread stereotype acceptance and endorsement of stigmatizing attitudes, which in turn influences structural stigma and results in a lack of public advocacy. Structural stigma refers to the institutional and systemic barriers which perpetuate ongoing inequality and discrimination of those with substance use disorders and it impacts provider barriers to the implementation of harm reduction methods (p. 6). 8 An example of structural stigma can be seen in U.S. federal policy. While the U.S. opioid response grant is meant to facilitate programs and harm reduction methods, it prevents the use of federal funding for methods, such as the purchase of syringes for SSPs or SISs. 9 Another example of structural stigma occurred in 2019 when the U.S. attorney for the Eastern District of Pennsylvania sued a nonprofit organization SIS called Safe House, arguing that they violated federal law and the crack house statute from the 1986 Controlled Substance Act. 11 This outdated U.S. federal policy reinforces a contradictory narrative which contributes to continued structural stigma and impacts harm reduction methods.
Changing the narratives of individuals with substance use disorders can decrease societal and public stigma. By identifying this subcategory of stigma and exploring internal policies in an organization, the same state and federal policies that impede harm reduction can aid in the universal adoption of harm reduction methods among providers. 4
Althoughorganizational and local support for implementing harm reduction methods exists, resentment, bias, and personal (individual) stigma toward these approaches may still persistamong providers. A cross-sectional survey conducted by Mahon et al, 12 gathered reflections from pharmacy students regarding substance use and naloxone administration. The coding of the student reflections revealed personal stigma and bias, indicatingthat not all students felt compelled to help IWOD. Additionally, personal tragedy and repeated negative professional interactions with IWOD cannegatively impact perceptions of IWOD and the perceived effectiveness of harm reduction methods. 10 Personal stigma among providers toward IWOD can influence their attitudes toward harm reduction and prevent their engagement in harm reduction methods.
Interventions aimed at personal stigma can alter a provider’s view and result in the implementation of harm-reduction methods. A cross-sectional study by Mahon et al, 11 found that pharmacy students who expressed personal stigma toward harm reduction methods and IWOD experienced a shift in their views after receiving an educational lecture on the purpose and goals of harm reduction. This educational experience alterede pharmacy students’ attitudes toward harmreduction practices and provided a non-judgmental experience for those experiencing biasesrelated to opioiduse. Promoting the disease model of addiction has also been shown to promote positive attitudes among first-time responders. 10 These shifts in attitude highlight the need for organizations to identify provider barriers to effectively implement appropriate anti-stigma interventions and educational initiatives. Without identifying these barriers, the implementation of harm reduction methodsrisk failing due to lack of provider buy-in, rooted in preconceived beliefs and personal stigma reinforced by public and structural stigma. By addressing these obstacles, organizations can improve provider buy-in and facilitate universal adoption of harm reduction methods. 6 Additionally, identifying provider perceptions and potential stigma toward individuals can help guide the curriculum and development of harm reduction programs.
Lack of Provider Knowledge and Training
A review of the literature revealed another barrier: a significant lack of education among providers regarding harm reduction and methods. Multiple studies identified subthemes, including provider misperception of harm reduction strategies, and lack of training.5,12,13,14 A systematic review by Gugala et al 5 found that physicians’ fear of liability and the perception that harm reduction methods would enable continued opioid use were significant barriers in their willingness to implement these methods. An exploratory factor analysis by Kruis et al 10 found that providers believed that implementing harm reduction methods would not decrease the death rate and instead encourage continued opioid use. Additionally, a cross-sectional survey by Kestler et al 13 revealed that 64.2% (419/652) of emergency department (ED) physicians felt that initiating buprenorphine for IWOD was a major responsibility. In a quantitative analysis by Holland et al (2020), 42.4% (50/118) of providers were unsure which patients would benefit from naloxone/buprenorphine, and 65.3% (77/118) of providers were unfamiliar with the risks and benefits. This limited understanding is a reflection of a lack of education for providers on the benefits of opioid harm reduction methods and how to discuss them with their patients.
Additionally, the lack of training and subsequent skills for implementing opioid harm reduction methods has proven to be a significant barrier for healthcare providers. A cross-sectional survey by Kestler et al 12 found that 58.2% (380/652) of ED physicians reporteda lack of adequate training as a barrier to ED buprenorphine induction, despite supportive evidence for this harm reduction method. In a study by Savage & Ross, 14 ED physicians identified lack of time as a barrier to buprenorphine/naloxone induction. However, further analysis revealed that a lack of skill resulted in incorrect knowledge of buprenorphine/naloxone induction; induction was then viewed as cumbersome and ultimately led to provider resistance and limited adoption of treatment. 14 In a mixed-method survey administered by Mahon et al 12 using the Brief Opioid Overdose Knowledge (BOOK) questionnaire, 99.2% (154/167) of pharmacy students felt that they would need further training in naloxone before feeling comfortable handling an overdose situation and educating patients about using naloxone.
Lack of comprehensive provider knowledge and training on opioid harm reduction methods reprents a major barrier to provider implementation. The consequences of inadequate skills and training among health care providers can be far-reaching and damaging. Not only can it lead to anxiety and fear among providers, which result in negative interactions, but it can also lead poor quality of care and poorer outcomes. Improving provider knowledge and skills through education, as well as promoting organizational training infrastructure can address and dismantle misconceptions regarding these harm reduction methods.
Lack of Access
Lack of access to care was identified as a major barrier to the implementation of opioid harm reduction methods. IWOD are known to have poor continued long-term care owing to a lack of appropriate access to services and support that will facilitate successful treatment. 14 Unfortunately, the ED is often the primary entry point for IWOD for opioid-related treatments, including buprenorphine/naloxone administration, drug-related health issues, and emergency naloxone administration. Post-discharge access to services and support is crucial for treating IWOD; however, the lack of services is challenging. 15 Savage & Ross 14 emphasized the challenge of limited access to referral services for long-term treatment of IWOD after ED treatment and bridge clinics. In a cross-sectional survey of ED physicians, 14 42.1% (274/652) indicated that a lack of adequate follow-up options was a barrier to the implementation of buprenorphine induction.
Lack of access to care impacts provider willingness ininitiating harm reduction methodsdue to concernabout the patient’s ability to continue their treatment successfully without adequate support. 7 A convenience survey by Savage &Ross, 14 found that providers (n=121 physicians) identified the lack of support by allied health members in arranging follow-up care as a major barrier to the initiation of buprenorphine/naloxone in the ED. A systematic review by Gugala et al 5 also foundthat lack of access to care was a major barrier to the implementation of harm reduction methods, stating that many physicians were unaware of the substance use services available to their patients. Identifying this barrier and empowering providers with the necessary resources to give patients access to care, can ease feelings of anxiety among providers when implementing harm reduction methods.
Further research is needed to provide a systematic review of the available literature to understand provider barriers to harm reduction. Implementing a harm reduction strategy can be a significant change for an organization. It is important to mitigate these barriers through education and to address the concerns of healthcare providers. Involving a diverse group of stakeholders in the planning and implementation process can help ensure buy-in from providers as well as address the needs of the community.
Limitations
Several limitations are identified in this narrative review. First, it is worth noting that the literature search was conducted from August to December 2022. At the time of review a federalaiver was still needed by prescribers for MAT. 16 This requirement presented a significant barrier in the ability of providers to prescribe MAT. Additionally, this narrative review primarily focused on identification of provider barriers and did not discuss facilitators or strategies to address these barriers thereby limiting its use. As emphasized multiple times throughout the review, it is important to clarify this is not a systematic review. The reviewers did not perform an exhaustive search of multiple databases and did not use formal tracking methods, contributing to possible bias and limiting generalizability of findings. Furthermore, the literature search included the term “stigma.” This term and lack of article tracking may have contributed to selective identification of articles and bias of search results.
Conclusion
The continued increase in opioid-related overdoses in the U.S. indicates the need for harm reduction programs, yet, significant inconsistencies between national patterns of opioid use and implementation of opioid harm reduction methods. 4 This inconsistency highlights the need to identify barriers that exist among providers when implementing evidence-based opioid harm reduction methods for adults aged ≥18 years, both with and without opioid use disorders. Without identifying and addressing provider barriers, there is a risk of losing provider support, and the widespread adoption of universal opioid harm reduction strategies is unlikely to occur.
Our review indicated three major barriers affecting providers’ implementation of opioid harm reduction methods: stigma, lack of education, and access to substance use treatment resources. Further systematic review is recommended to identify both the provider barriers that impact harm reduction implementation for opioid use and evidence-based methods to identify these barriers within an organization. By gaining insight into these barriers within organizations, program planners can provide interventions to address these obstacles and improve the implementation of harm-reduction methods. This will lead to greater universal adoption of and guidance for harm reduction projects.
Footnotes
Author’s Note
Stacie A. Dee is also affiliated to Northwell Health, Glen Oaks, NY, USA.
Sources of Support/Acknowledgments
Dr. Sandeep Kapoor, Dr. Renee Mcleod-Sordjan & Stephen Butkus The authors wish to acknowledge Dr. Renee McLeod-Sordjan, for her patience, guidance and mentorship.
Author Contributions
All authors equally contributed to the conception, literature collection and drafting of the original manuscript. Author S.D. served as the primary author for critical revision of the article in consultation with KA.D, D.B. and F.J.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics
The reviews did not need any ethical approvals or informed consent.