
Abstract
Improving the productivity of healthcare delivery and optimizing the allocation of regional healthcare resources are crucial for the health providers. The objective of this study is to evaluate the productivity dynamics of healthcare delivery at the regional (provincial) level in China, to provide evidence-based policy implications. After a review of literature, actual number of open beds, number of occupational or assistant doctors, number of registered nurses, and number of other staff were selected as input variables. The number of diagnostic visits and number of discharged inpatients were adopted as the output indicators. The panel data of 31 provinces in mainland China from 2010 to 2019 were extracted from Health Statistics Yearbook. Bootstrap-Malmquist Data Envelopment Analysis (DEA) model was used to measure the total factor productivity changes (TFPC) and its components. During the study period, the analysis of total factor productivity (TFP) in China revealed a declining trend with an average annual decline of 0.9% (ranging from 0.860 to 1.204). For each of the 31 provinces, the annual TFP scores varied from 0.971 to 1.029. On average, technical efficiency changes (TEC) had showed a downward trend from 2010-2011 (0.980) to 2013-2014 (0.982), and then an upward trend in 2014-2015 (1.029) and the following three consecutive years since 2016-2017 (1.000, 1.013, 1.009). Similarly, the trend in technological changes (TC) was consistent with the TEC from 2010-2019, which fluctuated between 0.969 and 1.011 on average per year at the provincial level. Notably, the point of inflection appeared at 2013-2014. Regional healthcare inputs and outputs in mainland China saw an upward trend from 2010 to 2019. However, TFPC, TEC, and TC decreased across all 31 provinces. TFP experienced a declining trend from 2010 to 2014, followed by growth until 2019. This may be related to the new healthcare reform being implemented since 2009, as service efficiency and capacity may undergo a reversal at the beginning of the reform.
Measuring the relative efficiency and productivity of the healthcare system is increasingly needed. The Bootstrap-Malmquist-DEA method has already been widely used for productivity measurement in many fields.
This research employs Bootstrap-Malmquist-DEA to measure the productivity of regional healthcare delivery, encompassing all kinds of different healthcare resources.
First, the Bootstrap-Malmquist-DEA method can be used to measure the productivity of healthcare system. Second, the allocation of healthcare resources in some regions still need further optimization. Last, provinces with insufficient healthcare productivity should focus on improving their technical efficiency.
Introduction
China has established a universal healthcare insurance system in the past decade, accompanied with tremendous increase of demand for more healthcare services.1,2 Despite the concerted efforts made by governments at all levels, meeting the increasing demand for healthcare from the population remains a significant challenge. 3 There has been tremendous increase in investments directly toward primary care, secondary and tertiary hospitals over the years. However, despite these substantial investments, the quality of primary care providers remains low. 4 Since primary care facilities typically serve as the initial point for patients seeking medical attention, the limited capacity and quality of these facilities contribute to a continuous influx of patients seeking care at higher-level hospitals.5 -7 In the current mechanism design, healthcare providers in China are allowed to survive by selling drugs and conducting health examinations, which unexpectedly leads to issues such as over-prescription, excessive medical examinations, and unnecessary healthcare services, and finally these practices contribute to a heavy financial burden on patients and an inefficient healthcare delivery system. 8 Unmet health care needs continue to increase, and health expenditure grows up sharply, which leads to problems such as poor doctor-patient relationship and a rapid growth of out-of-pocket payment.9,10 According to Masri and Asbu, 11 improving efficiency of the healthcare system is an important approach to meet rapidly growing health care demand and constrain the growth of health care costs. For China, more and more research requires the use of the latest methods to measure the relative efficiency and productivity of the healthcare system at the local, regional, and national levels.
Data Envelopment Analysis (DEA) is a widely used method in healthcare organizations for estimating relative efficiency and productivity. It utilizes multiple inputs and outputs to evaluate the performance of healthcare systems. Previous literature showed that some traditional DEA models were widely used by Chinese researchers to measure the efficiency of healthcare organizations. These models include DEA-BCC (Banker, Charles, and Cooper) 12 or DEA-CCR (Charles, Cooper, and Rhodes), 13 model for cross-sectional efficiency analysis and Malmquist-DEA model for longitudinal efficiency analysis of panel data. For example, Gai et al 14 applied the DEA-BCC Model and DEA-CCR Model to calculate efficiency. Li et al 8 applied Malmquist-DEA model to measure relative efficiency and productivity. Caballer-Tarazona et al 15 used a DEA model to calculate the performance of 3 healthcare service units of 22 hospitals in East Spain. Sulku 16 proposed a model based on DEA and the Malmquist index on the multiple inputs and multiple outputs of the ministry of health hospitals in Turkey. Also some researchers used related models of DEA to evaluate efficiencies of hospitals in Iran, Greece, US, Norway, Italy, Japan.17 -19 Similar to international research, existing papers on the regional healthcare efficiency in China have obvious limitations. One prominent limitation lies in the flaws of traditional DEA models. The relative efficiency scores calculated by the traditional DEA models tend to be significantly higher than the real scores and are susceptible to environmental and random factors.20 -22 To address this issue, Simar and Wilson, Daraio and Simar, among others, have introduced the Bootstrap method. This method improves the accuracy of DEA efficiency scores by correcting their bias and calculating confidence intervals. Based on the Malmquist index, the Bootstrap-DEA method has already been widely used for productivity measurement in the fields of banking,23,24 transportation,25,26 agriculture,27,28 and more. However, its application in healthcare productivity analysis has been limited. Cheng et al 29 adopted Bootstrap Malmquist-DEA to measure the efficiency and productivity. Wang et al 30 utilized Bootstrap Malmquist-DEA to evaluate the productivity. To date, no study has been found that utilizes Bootstrap Malmquist-DEA for the comprehensive productivity measurement of regional healthcare delivery, encompassing various types of healthcare resources.
DEA, a non-parametric method based on linear programing, has been widely applied to efficiency and productivity measurement. In the context of healthcare organizations with multiple inputs and outputs, DEA is often preferred over stochastic frontier analysis (SFA) as it does not require the construction of a specific function. However, there exist some limitations on the use of MPI based on the traditional DEA method,31,32 as DMUs is more prone to be influenced by environmental and random factors. Although the 3-stage DEA model, proposed by Fried et al, 33 can isolate the influence of external environmental and random factors on efficiency scores, providing a better reflection of the real internal management level of DMUs, the results are still sample-sensitive and are susceptible to extreme values. Hence, Simar and Wilson proposed the Bootstrap-DEA model with bias correction to improve the accuracy of the efficiency and productivity scores.21,22,34 -37 In this study, we used Malmquist productivity index together with Bootstrap-DEA method to evaluate dynamic changes in healthcare productivity across the 31 provinces in China.
Methods
Research Design
A longitudinal analysis was undertaken using a Bootstrap-Malmquist-DEA model. Total factor productivity changes (TFPC), technical efficiency changes (TEC) and technological changes (TC) were generated from the Bootstrap-Malmquist-DEA model for longitudinal comparisons, while the ranking of the average TFPC, TEC and TC of the 31 provinces was sorted for horizontal comparisons.
Input and Output Variables
In this study, input and output variables were selected by conducting an extensive literature review and analyzing available data from China Health Statistics Yearbook. However, selecting appropriate variables to measure healthcare efficiency remains a challenge in the current literature. Previous literature has suggested using statistical methods like cluster analysis and factor analysis for indicator classification and selection.
38
To address this issue, Our previous research conducted a statistical classification and analysis of published literature in Chinese on healthcare organization efficiency over the past 30 years, comparing it with peer international studies.
31
We counted the top 5 input indicators applied in international literature were number of beds, number of physicians/doctors, number of nurses and/or nursing staff, operating expenses/supplies, and number of total FTEs/staff/labor size. While the top 5 output indicators in international studies were number of outpatient visits, number of total surgeries, number of inpatient days, total patient days, number of discharges. This study concluded that combining volume variables with monetary variables could lead to confusion between technical efficiency (TE) and allocative efficiency (AE). Therefore, only quantitative variables were included in the indicator system of this study to enhance the credibility of the results. Ng
39
emphasized that labor and capital are both significant input variables in healthcare delivery. In her research, the numbers of doctors, nurses, pharmacists, and other staff were selected as labor inputs and the number of beds was selected as capital input. Based on available data from China Health Statistics Yearbook, number of occupational or assistant doctors, number of registered nurses, and number of other staff (including other technicians, administrative staff, and handyman) were selected as labor input variables in our study. Regarding capital inputs, the number of beds was typically adopted as a proxy of capital in international research. However, Li et al
8
argued that the dynamic nature of hospitalization in China is characterized by the use of numerous temporary beds. Thus, actual number of open beds was adopted as our capital input variable. For the output variables, we followed the approach of ou
Malmquist Productivity Index
In our study, we employed the MPI (Malmquist Productivity Index) to evaluate total factor productivity changes (TFPC) to reflect the longitudinal changes in the input-output efficiency of each decision-making unit (DMU). Initially introduced by Caves et al 40 for productivity analysis, the MPI was subsequently developed by Färe et al 41 as a tool to explain efficiency change and technological change.
The Malmquist index can be decomposed into technical efficiency changes (TEC) and technological changes (TC), and TEC can also be decomposed into pure technical efficiency changes (PTEC) and scale efficiency changes (SEC) under the hypothesis of constant returns to scale. According to Fare et al, 42 TEC measures the degree of catching-up of production decision-making units to the optimal production possibility boundary from period t to t + 1, also termed as “catching-up to the frontier effect.” If a DMU’s TFPC score is greater than 1, it indicates that DMU has experienced efficiency growth during that period; a TFPC score of 1 signifies unchanged efficiency, while a TFPC score less than 1 suggests efficiency deterioration. A TEC score greater than 1 indicates that the production of decision-making units has been closer to the production frontier and the relative TE has improved. TC shows the movement of the technological boundary from time t to time t + 1, also called “shift in the frontier effect.” A TC score greater than 1 implies that an improvement or innovation in technology, resulting in an upward movement of the production frontier.
Bootstrap-Malmquist-DEA Model
The basic idea of the Bootstrap method is to simulate the data generation process (DGP) through repeated sampling. The resulting sampling distributions and standard deviations therefore closely approximate the original ones. The bias corrected MPI with the confidence intervals on α level is produced based on the expanded simulated sample, which includes TFPC, TEC, and TC. The confidence interval excluding 1 indicates that it is statistically significant and the Malmquist index reflects the efficiency change, and vice versa.
Data Collection, Processing and Analysis
The data for the input and output indicators were extracted from the Health Statistic Year Book from 2011 to 2020. Descriptive analysis of the input and output indicators, including mean and standard deviation (SD), was conducted using SPSS 26.0 version statistical. The productivity and its decomposition indices of the provinces were measured using R 4.0.2 version statistical software, specifically employing FEAR package with 95% CIs. 43 The geometric mean was used to represent the average scores of productivity. A statistical significance was determined if the 95% CIs did not contain the value of 1.0000. The number of repeated sample selection was set at 2000. The statistical significance was set at α = 0.05.
Results
Descriptive Analysis of Input and Output Variables
Table 1 presents a descriptive overview of healthcare input and output variables of the 31 provinces in mainland China from 2010 to 2019. Data on all input and output variables showed a different levels of growth from 2010 to 2019. Notably, the number of discharged inpatients exhibited the highest average annual growth rate of 10.53%. On the other hand, the number of occupational or assistant doctors and the number of other staff showed a slower growth at average annual growth rates of 7.05% and 6.39% respectively. As shown in Table 1, the standard deviation of all input and output variables has been increasing year by year. This may indicate that the balance between regions was getting bad. Just like the result of the Healthcare Access and Quality (HAQ) Index. In 2016, China recorded the biggest range in subnational HAQ performance, which ranged from 91.5 score in Beijing to 48.0 score in Xizang (a 43.5-point difference). 44
Summary of Input and Output Variables.

I1 = actual number of open beds; I2 = number of occupational or assistant doctors; I3 = number of registered nurses; I4 = number of other staff; O1 = number of diagnostic visits; O2 = number of discharged inpatients.
Bootstrap MPI and Its Components
Table 2 shows the Bootstrap MPI (TFPC) and its decomposition indices (TEC and TC) of the 31 provinces in mainland China during 2010 to 2019. The provincial average TFPC fluctuated between 0.860 and 1.204 over this period. Notably, 83.15% of provinces exhibited statistically significant improvements in TFP. From 2010 to 2014, TFP experienced a decline, but it subsequently grew from 2014 to 2019. Furthermore, the provincial average TFPC occurred during the 2014-2015 period. However, 4 provinces (Heilongjiang, Shanghai, Chongqing, Xizang) experienced a decline in TFP during this period. In terms of individual years, only Ningxia exceeded a TFPC of 1 in 2010-2011, and only Yunnan achieved this in 2011-2012. On average, 8 provinces had improvements in TFP between 2010-2019, with Guangdong of the highest average annual growth rate of 0.98%. In addition, the annual TFPC among provinces varied over time. The provincial TE of healthcare in China exhibited a decline from 2010 to 2014, followed by an improvement from 2016 to 2019. The highest improvement in TE occurred in the period 2014-2015, with a growth rate of 2.92%. In that same period, only Chongqing and Heilongjiang do not experience TE growth. Shanghai remained unchanged, except in 2011-2012 and 2013-2014. Surprisingly, TEC was below 1 on average in 2015-2016. Among the 9 provinces analyzed, Guangdong exhibited the best TE improvement between 2010 and 2019, outperforming other provinces. On average, the TC first exhibited a positive trend, indicating a shift from technological regression to technological progress among hospitals in the 31 provinces of mainland China since 2013-2014. Prior to that period, the TC scores were below 1, although the minimum value of TC was greater than the corresponding TFPC and TEC values. The provincial average TC scores fluctuated between 0.942 and 1.169, with the highest score (1.169) observed in 2015-2016. The TC was below 1.025 but Xizang which was above 1.050 from 2015-2019, respectively. In general, all 31 provinces showed varying improvements in TC within the 9-year timeframe, with Xizang having the highest average growth rate.
Bootstrap MPI and its Components by Region in Period 2010-2019.
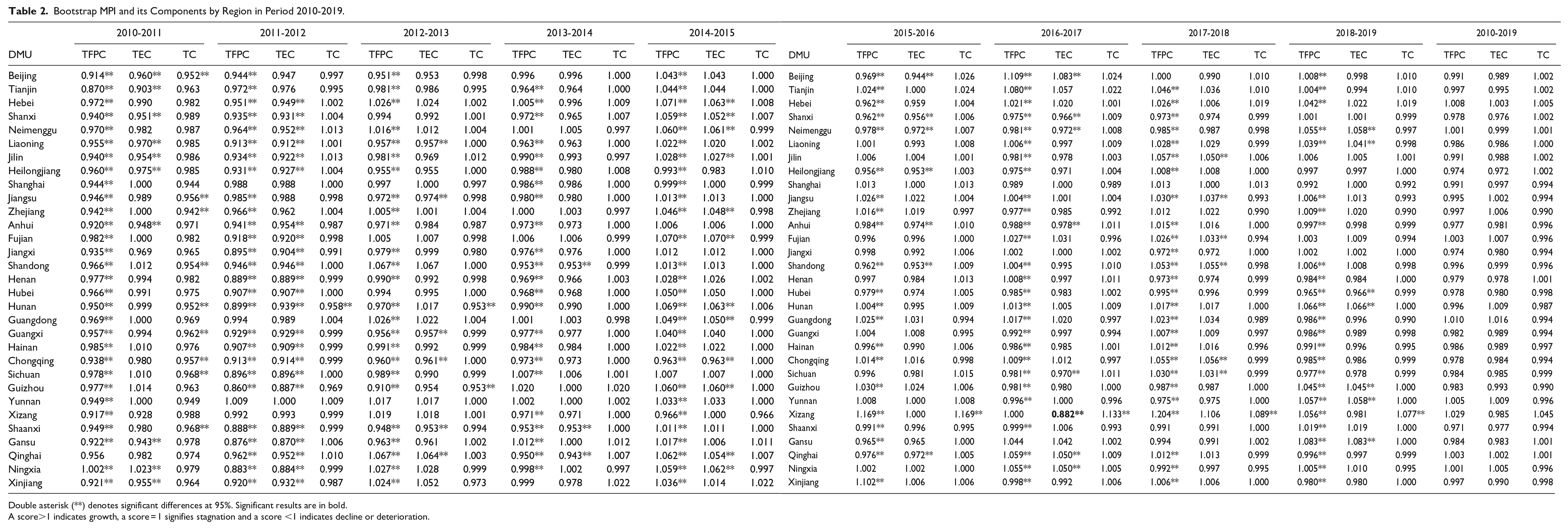
Double asterisk (**) denotes significant differences at 95%. Significant results are in bold.
A score>1 indicates growth, a score = 1 signifies stagnation and a score <1 indicates decline or deterioration.
Ranking of TFPC, TEC, and TC
Hebei, Qinghai and Neimenggu had higher ranks in TFPC, TEC and TC standings. While Guangdong, Yunnan and Fujian had higher ranks in both TFPC and TEC standings but lower ranks (18th, 20th, and 25th) in TC standings. Xizang secured the top rank in both TFPC and TC standings but ranked 21st in TEC. Shaanxi, Heilongjiang and Jiangxi occupied the bottom 3 positions in TFPC standing. For Shaanxi and Heilongjiang, the particular low TEC rankings (29th and 31st) contributed significantly to their low TFP growth. Meanwhile, Guangxi and Guizhou had low rankings primarily due to their disappointing TC standings.
Discussion
Our results indicated that overall regional healthcare inputs and outputs in China kept ascending from 2010 to 2019, driven by growing demands for healthcare services and supported by healthcare organizations’ development strategies and national policies. Du et al 45 demonstrated that there were no obvious productivity fluctuations in public hospitals during the recent observing years, indicating satisfactory performance in meeting the rapidly growing medical demand. However, variations in healthcare inputs (such as open beds and healthcare professionals) and outputs (such as diagnostic visits and discharged inpatients) were observed across provinces each year. This highlighted the imbalanced spatial distribution of healthcare resources in China, as discussed by Yin et al, 46 leading to inadequacy and limited access to affordable healthcare services. To address this issue, it is crucial to redistribute high-quality healthcare resources from urban areas to grassroots and communities, aiming to balance and optimize the allocation of healthcare resources between developed and underdeveloped regions.
Total factor productivity referred to the output growth rate brought about by all production factors except for labor and capital. The core of the Malmquist index was to analyze the reasons for total factor productivity changes, identify whether its growth was based on technological progress, efficiency improvement, or scale efficiency. Technological change referred to a change in the overall production technology, which can be divided into technological progress and technological regression. Technological progress comes from technological innovation, while technological innovation comes from the introduction of new technologies and equipment, as well as the proficient use of new technologies and equipment by professionals. Efficiency changes were caused by the development level of existing technology, the level of operation and management, and the suitability of hospital production scale.
The results indicated that, on average, TFPC, TEC, and TC of all 31 provinces showed a slight decline in 10 years. Al-Hanawi and Makuta 47 also indicated TFP for healthcare services has decreased on average by 5.6% per year primarily due to a technical regression from 2006 to 2018. Base on the overall situation of each province, the decline in total factor productivity may be mainly attributed to changes in technical efficiency. According to Li et al, 8 technical efficiency changes had trivial contributions to TFP growth, which is a common problem among Chinese public hospitals. But between every 2 years, the TFPC, TEC, and TC showed fluctuations from decline to improvement. Cheng et al 29 reported similar results that the township hospitals experienced a positive productivity shift from 2008 to 2012 but experienced deterioration from 2012 to 2014, and that TFPC of the township hospitals declined by 2.14% during the 7-year period. Li et al 48 also noted the efficiency of the county-level public hospitals in Anhui Province has not improved significantly, and the total productivity factor had declined during 2010-2015. To be specific, technology growth started in 2013- 2014, while TFP and TE have increased in 2014-2015. This may be due, in part, to the new healthcare reform being implemented since 2009. 49 The reform aimed to establish a relatively comprehensive healthcare system and has lead to substantial improvement in overall service capacity and medical technology across all levels of the healthcare organizations. However, initially, service efficiency and capacity may have experienced setbacks before progressing. The reform also emphasized the provision of basic public health services, chronic disease management, and mental health services by primary healthcare organizations. As the development of primary healthcare organizations continues, the extensive needs of urban and rural residents for public health services can be meet. In addition, the basic healthcare insurance system improved in the reform covers both urban and rural areas universally. On the one hand, it helps minimize individual healthcare expenses and improve access to healthcare services for both urban and rural residents. 29 On the other hand, third-party purchasers of healthcare insurance institutions are playing an increasingly significant role in intervening and supervising the operating practices of healthcare organizations, contributing to the continuous improvement of regional healthcare service capacity, such as reducing hospitalization lengths and increasing bed turnover rates. 50
Our study shows that, for some provinces such as Xizang, Hebei, and Tianjin, technological improvement is the major contributor to TFP growth. The introduction of new drugs, updated medical technologies and high-tech medical equipment has proven crucial in improving regional healthcare productivity. This suggested that the provinces with insufficient healthcare productivity growth, such as Guizhou and Hunan, should focus on improving their TC. Guizhou Province located in the southwest of China, medical technology may lag behind eastern cities. Guizhou had many highland and mountainous areas, and it is a province where multiple ethnic groups coexist. Hunan is the most populous province in China, medical needs is directly proportional to population. They can introduce new technologies, introduce or update devices, construct clinical specialties, strengthen county hospitals and so on. Their emphasis should be placed on improving the utilization of resources and fully leveraging technological capabilities. Similarly, Nghiem et al 51 revealed technical changes are the driving force of productivity growth in Queensland health in the study period 1996 to 2004. Al-Hanawi and Makuta 47 indicated addressing existing technological challenges can unlock potential gains in healthcare service productivity. However, with the technological advancement and innovation, doctors’ profit-driven behaviors can increase healthcare expenditures, thus undermining the efficiency of healthcare system (it is important to mitigate profit-driven behaviors among doctors that can lead to increased healthcare expenditures and undermine system efficiency). 52 With the new healthcare reform being implemented, this unhealthy mechanism was seen to gradually diminish. The results of Cordero et al 53 showed that the productivity growth of hospitals belonging to the SSF has been much higher than those belonging to the Ministry of Health during the period between 2005 and 2015, primarily due to superior technological advancements, particularly in the later years of the evaluation period. Based on such reasons, the provinces with relatively low TFPC and TEC, such as Heilongjiang, should focus on improving their TEC. This can be achieved through optimizing health personnel training and management to stimulate the scale efficiency, introducing third-party agencies for performance evaluation and adopting benchmarking and cross-organizational learning mechanism to help improve the pure technical efficiency and internal management levels.
Limitations
The Bootstrap-Malmquist-DEA model was used in this study to evaluate the intertemporal healthcare productivity changes in 31 provinces of mainland China. However, this study can be improved in the following aspects. First, the DEA method used in this study has some limitations, such as the inability to assign appropriate weights to the selected input-output indicators. For future efficiency research, it would be beneficial to explore alternative methods like SFA and compare their effectiveness. Second, further studies can consider employing 3-stage DEA combining Bootstrap-DEA for intertemporal data analysis to reduce the impact of some environmental and random factors on efficiency scores, for a more accurate measurements of healthcare productivity changes.
Conclusions and Recommendations
The results indicated that both regional healthcare inputs and outputs in all the provinces have different degrees of growth after the implementation of the new healthcare reform in 2009, but the allocation of healthcare resources in some regions still need further optimization. Moreover, all 31 provinces had experienced healthcare productivity growth during the study period, for which substantial improvement in TC was the main contributor.
Observed differences in the productivity improvements between different provinces suggest that those with insufficient healthcare productivity should focus on improving their TE. On the one hand, the development of hospital scale should be guided by regional health planning and optimized allocation of health resources, adhering to the principle of moderation. Strengthening cooperation and coordination among medical institutions was crucial for optimizing the allocation of medical resources. Implement a graded diagnosis and treatment system was a favorable means to achieve the rational utilization of medical resources. Improve institutional construction was the guarantee. On the other hand, increase government investment to comprehensively improve the efficiency of hospitals from various dimensions. Focus on leveraging technological and specialized advantages.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Key Research and Development Program of China (Grant No. 2020YFC2006000). This study was supported by the National Natural Science Foundation of China (Grant No. 71573061).
Ethics Approval
This paper does not contain data collected from human subjects requires ethics approval.
Consent for Publication
All the authors listed in this paper have already read this manuscript and agreed to submit the paper and for later publication.