
Abstract
Telehealth use among individuals with and without transportation challenges remains understudied. This study aims to compare telehealth utilization and types of healthcare services between subjects with and without transportation challenges. Using data from the 2021 Medical Expenditure Panel Survey (MEPS), we identified telehealth use for office visits by adults (≥18 years old) in 2021, categorizing the type of healthcare services received, such as checkups and mental health counseling. Weighted logistic regression was employed to identify factors associated with telehealth usage. The total population analyzed was 204 621 985 (unweighted n = 17 674). The average (SD) age of the subjects was 49 (18) years old, and 53% were female. On average, individuals with transportation challenges had 1.40 telehealth visits, while those without such challenges had 0.87 visits (P = .03). Additionally, individuals with transportation challenges had more visits related to behavioral health compared to those without transportation challenges (22% vs 11%, P < .01). Those facing transportation challenges were 40% more likely to use telehealth compared to those without transportation challenges (OR = 1.40, P = .01). The findings suggest that telehealth could serve as a viable solution to overcome transportation barriers and improve access to care. However, it is crucial to assess access to care through telehealth to enhance the health outcomes for individuals facing transportation challenges.
While transportation barriers can impede access to healthcare services, there is limited information available on the relationship between transportation barriers and the utilization of telehealth.
Our research contributes by comparing telehealth utilization and the types of healthcare services accessed among subjects with and without transportation challenges.
Telehealth could play a crucial role as a bridge for individuals with limited access to transportation, facilitating their connection to essential healthcare services.
Introduction
The lack of transportation negatively impacts healthcare utilization, as it has been consistently linked to poor medical treatment.1 -4 Addressing this issue, telehealth visits have emerged as a viable solution to overcome transportation barriers. However, while telehealth could offer a promising alternative, it may not fulfill all healthcare needs,5,6 emphasizing the multifaceted nature of healthcare.
The COVID-19 pandemic significantly exacerbated existing transportation barriers,2,7 underscoring the urgent need for alternative healthcare delivery methods. During the pandemic, there was a remarkable surge of telehealth use,8,9 serving as a critical avenue to access medical care. Despite this notable increase in telehealth use, limited research has investigated how the lack of transportation could be associated with an increase in telehealth use during the pandemic.10,11 Two studies have suggested that telehealth could ease transportation challenges, 10 However, these studies used small sample sizes to evaluate the relationship between transportation challenges and telehealth use. Because of these limited sample sizes, their results could not be generalizable to other populations. The use of a national survey helps to address these issues and is critical to provide more broadly applicable results. In addition, this study highlighted potential differences in healthcare use between those with and without transportation challenges. Understanding these distinctions between the 2 groups could be critical for delivering targeted care to reduce existing healthcare disparities.
The aims of the study, using a national survey, were to examine (1) if there were potential differences in the types of healthcare services received by individuals with and without transportation challenges, and (2) if those experiencing a lack of transportation were more likely to use telehealth as a means of seeking medical care compared to those without transportation barriers.
Methods
Data
This study employed a cross-sectional study design, utilizing data from the 2021 Medical Expenditure Panel Survey (MEPS), which gathers information from families, individuals, and medical providers across the U.S. The MEPS surveys nationally representative samples of the U.S. civilian noninstitutionalized population to measure healthcare use, spending, health insurance coverage, and the health status of the population. For the study, the 2021 Full-Year Consolidated Data file and the 2021 Office-Based Medical Provider Visits file were used. The 2021 Full-Year Consolidated Data file, representing the most recent available data in the MEPS, included social determinants of health (SDOH) for adults (≥18 years old in the survey) such as affordable housing, access to transportation, home problems, and food insecurity. The 2021 Office-Based Medical Provider Visits file provided data on telehealth use and types of office visits (eg, dental visit, behavioral health visits). More details about the MEPS and the SDOH components can be found elsewhere.12,13 As this study exclusively used publicly available MEPS data, ethnical approval was not required.
Subjects
Adult respondents (≥18 years old) in 2021 were included in the study. Among them, those with missing information in the outcomes and the control variables were excluded in the study. The total number of adults surveyed in 2021 was 258 042 685 (unweighted n = 22 779). Among them, subjects with missing information in the lack of transportation question and subjects with missing data in age, sex, race/ethnicity, poverty level, type of insurance, and comorbid conditions were excluded (weighted n = 53 420 700; unweighted n = 5105).
Outcome
The type of care received during office visits (whether in-person or via telehealth) was 1 outcome. The type of care recorded in the Office-Based Medical Provider Visits file included checkups, diagnosis or treatment, mental health counseling, follow-up visits, emergency visits, and vision exams. The other outcome was based on the telehealth visit flag (Yes or No) in the dataset, indicating whether the office visit was conducted through telehealth versus in-person.
Independent Variable
The independent variable, lack of transportation, was created by using the following survey questionnaire in the MEPS: “During the last 12 months, has a lack of transportation kept the person from medical appointments, meetings, work, or getting things needed for daily living.” Based on this question, a binary variable was created to indicate presence or absence of a lack of transportation (Yes/No).
Covariates
Variables potentially associated with the outcomes were created using the existing variables in the survey. These variables included age categories (18-30, 31-40, 41-50, 51-64, 65-74, and ≥75), sex (male vs female), race/ethnicity (non-Hispanic White, Hispanic, non-Hispanic Black, non-Hispanic Asian, and non-Hispanic other races), family income as a percentage of the poverty line (poor, near poor, low income, middle income, and high income), type of health insurance (private, Medicaid, Medicare and no insurance), physical limitation (Yes or No), education (no high school graduate vs high school graduate), marital status (married, widowed/divorced/separated, or never married), comorbid conditions (hypertension, diabetes, asthma, cancer), access to public transportation (poor vs good), neighborhood availability of places to get medical care (poor vs good), total number of office visits, and census region (northeast, Midwest, south, west). The neighborhood availability of places to get medical care indicated the accessibility of healthcare services within a neighborhood or community. The total number of office visits per subject in 2021 was calculated from the data in the Office-Based Medical Provider Visits file.
Statistical Approach
Survey weights, reflecting the U.S. population with the surveyed sample, were applied to all analyses. 13 Survey-weighted summary statistics such as mean, standard deviation (SD), and percentage were used to present the characteristics of the population. Survey-weighted T-tests and Chi-Square tests were used to compare the characteristics of subjects between the 2 groups (lack of transportation vs no transportation challenges). 13 Weighted logistic regression, with the binary outcome indicating any telehealth use (Yes or No for office visits in 2021), was used to estimate odds ratio (OR) and P-values for the controlled variables. To calculate correct standard errors of the controlled variables, the Taylor-series linearization method, recommended by the MEPS survey, was applied to account for the complex sample design of the survey. 13 P-value <.05 was considered statistically significant. Stata Version 18.0 was used for the analysis.
Results
A total of 204 621 985 (unweighted n = 17 674) subjects were included in the analysis. Average (SD) age of the subjects with and without a lack of transportation was 47 (18) years old and 50 (18) years old, respectively (P < .01). About 56% of subjects with a lack of transportation were female, while 53% of subjects with transportation were female (P = .01). The racial and ethnic distribution between the 2 groups differed significantly (P < .01). Among those with a lack of transportation, 20% and 17% were Hispanics and non-Hispanic Black, respectively. In those without transportation challenges, 16% and 11% were Hispanics and non-Hispanic Black, respectively. However, the average number of office visits between the 2 groups were similar: 8.4 for those without transportation challenges versus 8.6 for those with transportation challenges (P = .73) (Table 1).
Characteristics of Adults With and Without Transportation Barriers.

The total number of office visits for subjects included in the study was about 1.72 billion visits (unweighted visits n = 157 286). Among them, 5.6% of the total office visits were from those with a lack of transportation, while 94.4% were from those without transportation problems (Table 2).
In the group with a lack of transportation, about 17% of the total office visits were for general check-ups, 31% were for diagnosis or treatment, and 22% were for behavioral health visits. The group without transportation issues had a similar number of office visits for general check-ups (18% vs 17%, P = .24), but had a higher proportion for diagnosis or treatment (40% vs 31%, P < .01) than those with a lack of transportation. However, those with a lack of transportation had more visits with behavioral health than subjects without transportation challenges (22% vs 11%, P < .01) (Table 2).
Type of Healthcare Received During Office Visits Between 2 Groups: Those With and Without Transportation Challenges.

Note: Others included emergency, vision exam, and pregnancy-related visits.
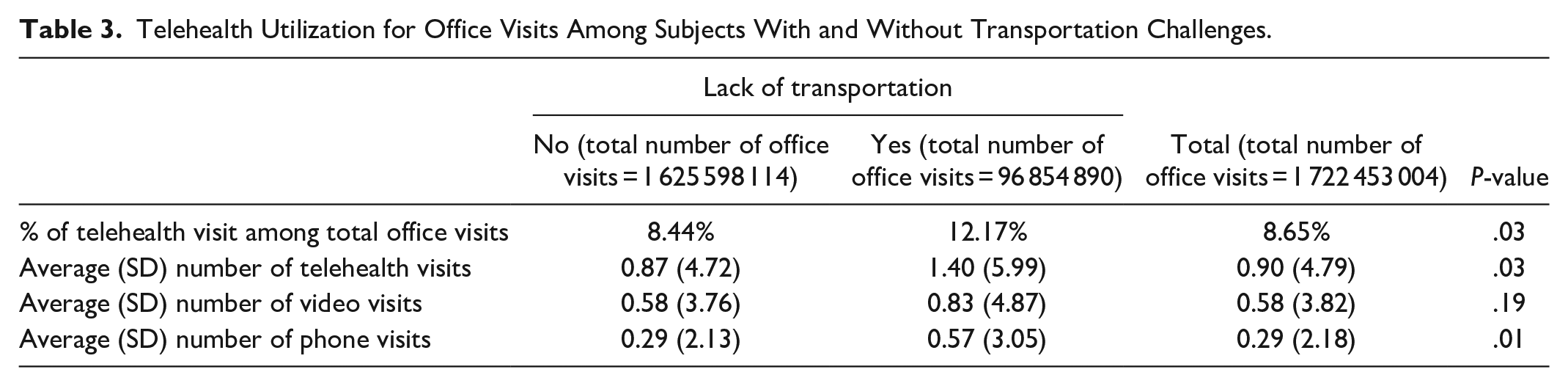
Of the total office visits, about 12% for those with a lack of transportation were conducted through telehealth, compared to 8% for those without transportation challenges (P = .03). The average numbers of telehealth visits for those with and without a lack of transportation were 1.40 and 0.87, respectively (P = .03). Among these telehealth visits, an average of 0.82 visits for those with a lack of transportation were based on video interactions, while those without transportation challenges had an average of 0.56 visits based on video interactions (P = .19) (Table 3).
Telehealth Utilization for Office Visits Among Subjects With and Without Transportation Challenges.
Those who had a lack of transportation were 40% more likely to use telehealth compared to those who had no lack of transportation (OR = 1.40, P = .01). Females were 36% more likely to use telehealth for office visits than males (OR = 1.36, P < .01). Non-Hispanic Black individuals (OR = 0.70, P < .01) and non-Hispanic Asian individuals (OR = 0.65, P = .02) were less likely to use telehealth than non-Hispanic White individuals (Table 4).
Factors Associated With Telehealth Use for Office Visits Using Weighted Logistic Regression.

Discussion
The findings in the present study demonstrate that individuals facing transportation barriers were significantly more likely to use telehealth visits (ie, by 40% more) compared to those with access to transportation. These findings align with previous studies by Vinella-Brusher et al and Svistova et al10,11 In a survey of 324 individuals about telehealth usage from April 2020 through April 2021, Vinella-Brusher et al 11 reported higher rates of telehealth use in individuals with a transportation barrier. Further, in a study involving focus groups with providers and Medicaid organizations, Svistova et al 10 reported that telehealth visits alleviated transportation barriers for patients. While these studies highlight the relationship between the adoption of telehealth usage and individuals with transportation barriers, the research in this area is sparse. The robust analysis and sample size of the present study using a national survey data strengthen the evidence that individuals with transportation barriers during the COVID-19 pandemic rely on telehealth to access care.
Telehealth usage varies by specialty. For example, the rate people use telehealth visits for mental health services are consistently high .8,14,15 The results from the current study support this finding. In an analysis of 16.7 million individuals, Patel et al, 8 showed a wide variation of telehealth usage based on specialties during the COVID-19 pandemic. Their results showed that 56.8% of psychiatry visits used telehealth from March 2020 through June 2020. Drake et al , using a sample size of 1 110 337 illustrated changes in telehealth usage pre- and during the COVID-19 pandemic. They showed that psychiatry visits minimally decreased because nearly all visits transitioned to telehealth, a trend that persisted through September 2020. The current study, which includes data from 2021, showed lower rates of telehealth usage, but did demonstrate higher rates of behavioral health visits. Furthermore, the current study revealed that those with a lack of transportation had more visits for behavioral health than subjects without transportation challenges (22% vs 11%).
Demographic differences of telehealth utilization in the present study were consistent with other studies, indicating that females were more likely to use telehealth compared to males, and non-Hispanic White individuals had higher telehealth utilization compared to non-Hispanic Black and non-Hispanic Asian indiviauls.11,14,15 Drake et al, reported rates of telehealth visits during the COVID-19 pandemic in a sample of 1 110 337 individuals. In comparison to White individuals, Black individuals had a risk ratio of 0.90, Hispanic 0.80, and Asians 0.95. They also reported that males had a risk ratio of 0.78 compared to females. 15
The observation that individuals with transportation barriers experience worse health outcomes and have a greater challenge accessing healthcare, has been well established.1 -4 Thus, the findings of the present study support the hypothesis that the use of telehealth by those with transportation challenges could narrow the gap in healthcare disparities. However, concerns about telehealth availability persist, especially considering that individuals with transportation barriers often have low socioeconomic status, and previous literature suggests that individuals with low socioeconomic status are associated with lower adoption of telehealth.8,16 Furthermore, socioeconomic factors surrounding race and ethnicity influence telehealth utilization, and individuals from these groups are also disproportionately impacted with transportation challenges. 17 While telehealth could present an opportunity to bridge a gap in healthcare disparities caused by a lack of transportation, additional modalities, such as targeted healthcare or mobile clinics, should be explored to improve health outcomes and eventually narrow disparities in health and healthcare.
Although telehealth holds promise for individuals with transportation challenges, it may have inherent constraints. Care that requires a physical examination, immunizations, and laboratory tests are not feasible during remote consultations. This technological limitation underscores the importance of exercising caution when interpreting the scope of telehealth interventions. However, because tele-psychiatry visits do not have this constraint, there is a greater opportunity to create more access for mental health services.
While this study revealed increased telehealth utilization among subjects with a lack of transportation, several limitations could impact the findings in the study. First, the study was not able to examine how telehealth use among those with a lack of transportation impacted their health and health outcomes, as there was no follow-up data post-telehealth use. Second, due to survey constraints, the study focused on adults, limiting the generalizability of findings to children or adolescents. Third, the survey relied on self-reported responses. Therefore, there could be the potential for recall bias, which could impact our findings. Further, the access to transportation variable is binary, making it impossible to discern between varying degrees of transportation barriers.
Conclusions
The findings of this study support the increased use of telehealth among individuals confronting transportation challenges, particularly in the domain of behavioral health. Considering these findings, it is conceivable that telehealth could serve as a crucial bridge for those with limited access to transportation, facilitating their connection to essential healthcare services. While we recognize the potential of telehealth in addressing healthcare disparities, it is essential to maintain a vigilant stance on evaluating its ongoing impact on health outcomes. Continuous assessment ensures that telehealth not only remains a viable solution but also evolves to be an effective and sustainable means of healthcare delivery for individuals navigating transportation challenges.
Footnotes
Acknowledgements
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent/ Patient consent
Not applicable.
Trial registration number/date
Not applicable.
Grant number
Not applicable.
Ethical Statement
As we utilized a publicly available dataset, ethical approval for the study was not required.