
Abstract
In the dynamic panorama of China’s shifting social mobility, characterized by a transition from individual to family mobility, the migration of the first cohort of migrant workers and their families has taken center stage. However, the scholarly discourse on how family migration influences the health of migrant workers remains contentious. This study uses data from the China Migrants Dynamic Survey (CMDS) of 2017 to focus on the first cohort of migrant workers. Drawing on the theories of family stress and life course, the empirical analysis incorporated heterogeneity tests, total effects, robustness tests, mediation effects, and propensity score matching to explore the mechanisms underlying the impact of family migration on migrant workers’ health. Data analysis reveals a substantial negative impact of family migration on the health status of the first cohort of migrant workers. Variations in health outcomes were identified across different family migration patterns. Further analysis indicates that the first cohort of migrant workers, when confronted with family livelihood pressures, tends to prioritize economic resources to support urban family life over their own health. This is because they are influenced by a family-centered culture. Our findings reveal a nuanced landscape. While family migration provides potentially enhances social support systems, it also imposes significant health trade-offs due to increased life stressors. These stressors include economic instability, increased responsibility for family care, and the psychological impacts of adapting to new urban environments. There are the health crowding-out effect of family migration on first cohort migrant workers.
Keywords
Our prior research has demonstrated a cultural change in behaviors of intergenerational exchange. The older generation continues to fulfill the cultural tradition of downward transfer of support. Addressing the research perspective on the impact of parental health in family-oriented migration studies.
This research not only addresses an ongoing academic debate but also holds substantial implications for policy-making. By understanding the health impacts of familial migration, policymakers can better tailor social services to meet the evolving needs of migrant families. This comprehensive analysis aims to elucidate the mechanisms through which family migration affects migrant workers’ health, providing a foundation for informed policy interventions.
This study demonstrates the proposal of the family-oriented essential direction of the social welfare policy support system in the process of urbanization in China. Social insurance policies are needed to ensure well-being of citizens.
Background
Fueled by urbanization and globalization, migration has emerged as a critical aspect of family life worldwide. In developing countries, millions migrate to urban centers or more developed nations, seeking improved employment and living conditions.1(pp. 231-235),2(p. 125)
This study examines population migration through the lens of individual and household livelihoods.3,4 Notably, most first-cohort migrant workers in China have integrated into urban employment sectors, reflecting the country’s emphasis on family-oriented migration. Such migration trends are evidenced by a prevalent household size of at least 2.5 individuals, with over 81.8% of migrating households comprising 2 or more members. 5 These trends are increasingly driven by needs related to childbirth, medical care, and elder care, intensifying the demand for public services and social security.6(pp. 212-234) The concept of the first cohort of migrant workers, defined as those rural individuals born before 1980 who began working outside their hometowns around 1985, aligns with China’s period of accelerated industrialization and urbanization. 7 This era marked a significant increase in the floating population and initiated the largest influx of rural migrant workers in Chinese history, commonly referred to as the “migrant worker wave.” 8 This historical context is crucial for understanding the unique economic behaviors and challenges faced by this population segment.
Amid these dynamics, a debate persists in academic circles regarding the adequacy of health care services for these migrants. This study poses a critical question: Does family migration safeguard the health of migrant workers? Employing quantitative methods, our research explores various factors impacting the health of China’s first-cohort migrant workers. Against the backdrop of familial migration trends among migrant worker households, there is an ongoing academic controversy regarding whether their health issues are adequately addressed.
Family Stress Theory from a Life Course Perspective
The life course theory, as developed by Glen H. Elder 9 and others, suggests that individual life trajectories comprise a series of roles, life events, and the long-term impacts of these events on individual outcomes. 10 A fundamental principle of this theory, the “temporality of life,” highlights the societal importance of age, interpreting its significance within the framework of social time.11,12 This principle posits that societal expectations vary significantly across different life stages, influencing individual privileges and social status benefits accrued over time.11,12
The Family Stress Model (FSM) specifically addresses how economic stress affects family functioning.13,14 Initially articulated by researchers like Conger and Elder, FSM posits that economic hardship, characterized by low income or adverse financial events, creates economic pressures that manifest as day-to-day strains. 9 These include difficulties in managing bills or affording basic necessities, impacting the psychological well-being and emotional health of family members. 15 The impact of economic stress is further nuanced by the life stage of family members, as each stage carries unique vulnerabilities to socio-economic changes. For instance, younger individuals might experience these pressures differently compared to adults who are responsible for providing for a family. This difference underscores the importance of considering the life course stage when examining the effects of economic stress on family dynamics.16,17
Understanding the interplay between life stages and family stress is crucial for developing targeted interventions that address the specific needs of families at different life course stages. By integrating life course theory with the Family Stress Model, researchers and policymakers can better understand how age-related social expectations and economic pressures interact to influence family health and well-being.
Cohort Effect on Migrant Workers’ Health
The cohort effect, defined as the homogenizing influence on individuals within the same or similar age groups due to shared sociocultural environments and historical events, plays a significant role in the health outcomes of migrant workers. 10 Elder et al. 18 note that cohorts born during the World Wars exhibit pronounced depressive symptoms, highlighting how age reflects not only physiological but also social factors. In the context of migrant workers, age differences signify varying life courses shaped by macro-social policies.19,20 This perspective is crucial when considering the diversity among migrant workers, particularly as those over 45 face significant pressures including employment, healthcare, and income. Jin et al. point out that migrant workers experience a peak in income at 35, earlier than urban counterparts who peak at 45, suggesting a premature loss in earning capacity in the job market. This indicates a need for policies that address these unique challenges faced by different cohorts of migrant workers. 21
Research by Ni et al. using CHIPS data reveals a U-shaped relationship between age and savings rate among residents, with savings dipping during the middle-age period. 22 This trend is particularly evident among the cohort of migrant workers in their 40s, who are in a high-expenditure phase of their family life cycle, primarily financing significant life events such as the education and marriage of their children.These financial burdens substantially deplete their savings, leading to a scarcity of resources for personal development. 23
Migrant Workers Income and Health
Research consistently shows a reciprocal relationship between health and income, particularly in industrialized settings, where health significantly influences employment and income opportunities.24,25 This dynamic is also crucial among migrant workers, where good health not only boosts income but deteriorating health severely reduces it. 26 Conversely, income influences health through improved living standards and access to medical care, forming a cyclical relationship crucial for understanding the socio-economic dynamics of migrant workers.27,28
However, the inherent endogeneity between health and income—each influencing the other—complicates this research, necessitating sophisticated statistical methods like using lagged health variables to disentangle these effects.21,23,29 Furthermore, the impact varies among different income groups: lower-income migrant workers benefit more significantly in income from improvements in health than their higher-income counterparts, suggesting differential impacts based on economic status. 30
Income disparity among migrant workers not only affects their physical health but also their mental well-being, influenced by their perceived social status. 31 Particularly vulnerable are those classified in the 4D employment category (Dirty, Dangerous, Difficult, and Damaged), who face heightened health risks after age 50.18,32
Moreover, access to healthcare is disproportionately lower among low-income migrant workers, highlighting systemic barriers that prevent equitable healthcare utilization.33,34 Duleep 35 points out that higher income facilitates better health through improved access to nutritious food, housing, and medical services, underscoring the necessity for comprehensive policies that enhance both economic and health outcomes for migrant workers.
Migration and Health of Migrant Workers
Research on international migration, particularly from underdeveloped to developed regions, has highlighted a complex relationship between migration and health.36,37 This relationship is encapsulated in the “immigrant health paradox,” where, despite lower socioeconomic statuses, immigrants often exhibit better initial health conditions than local residents in the destination areas—a phenomenon also referred to as the “Latino Mortality Paradox.”38,39 Empirical studies indicate that the health of immigrants tends to deteriorate over time due to factors like acculturation and changing lifestyles.40,41 This deterioration is often exacerbated by the challenges migrant workers face in accessing healthcare, due to both high mobility and the localization of medical insurance systems.42,43 The distance of migration significantly affects the social integration of migrants, leading to psychological and physiological health issues.44,45 Migrants often face reduced medical reimbursement rates and accessibility issues due to the “administrative distance” from their registered homes. 46 Economic disparities and challenging living conditions further contribute to the health decline of migrant workers. Low income and inadequate housing conditions reduce the utilization of medical services, promoting unhealthy lifestyles.47 -49 Moreover, the mental health of migrants is adversely affected by stress related to work and family dynamics, as highlighted by studies on rural-to-urban migrants.50,51
Family Migration and Health
Previous research primarily focused on the health of migrants, but more recent studies have begun exploring how migration impacts the health of family members left behind. These studies generally fall into 2 categories: the negative and positive effects of migration on household members. 52 Migration can negatively affect the psychosocial health of family members due to the disruption of family structures and reduced social support. The absence of family members often leads to increased emotional burdens and additional stress from needing to compensate for the decreased labor available at home. However, these negative effects might be mitigated by the economic and social resources that migrants send back to their families.53,54 Conversely, migration can have beneficial effects on the households left behind, primarily through significant economic contributions. These contributions can enhance household consumption and improve living standards, impacting sanitation, nutrition, and housing positively.55,56 Additionally, studies suggest that the mental health of refugees improves with the presence of a strong family network in the new country, although this benefit is restricted to core family members and does not extend to the wider “extended family” network. 57 Traditional migration theories argue that migration for work is driven by the maximization of economic benefits, often resulting in individuals migrating without their families. 58 Further research indicates that nonmigration family can significantly harm the mental and physical health of adults in families that left-behind compared to those in migrating families.59 -61
Since the initiation of China’s reform and opening-up policies, population migration has been a significant shift from “local China” into “migratory China” characterized by sustained economic and social development. This transformation has brought about profound changes in the family dynamics of migrant workers.62 -64 The core of the study examines how family migration influences the psychological and physical well-being of children. These children often face numerous challenges, including weakened social networks, social discrimination, adaptation difficulties, and limited healthcare access.65,66 Despite these obstacles, studies suggest that migrant children benefit significantly from migration, gaining better educational opportunities and enhanced social supports. The close presence of parents during migration strengthens emotional bonds, which is pivotal for boosting the children’s human capital.67,68
Migrants and their familiesfaced the socio-economic nulnerabilities. Migrants and their families often struggle to utilize available public services fully, highlighting their socio-economic vulnerabilities.69,70 Despite facing societal discrimination and adaptation challenges, migrant children are considered primary beneficiaries of the migration process. 71
The literature indicates mixed findings on the migrant workers’ health impacts of family migration. While some studies highlight the positive effects of emotional support from family presence—especially from spouses or close family on mental health and self-rated health levels, 72 others present contrasting results. For instance, Shang and Shi argue that spousal migration does not significantly affect health outcomes, and using data from the China Labor Force Dynamic Survey, it is suggested that family migration might have varied impacts on migrant workers’ health.73,74 Jiang notes a significant negative effect on migrant workers’ health due to family migration, whereas Chu reports significant health improvements among migrants.75,76
There is a growing body of evidence regarding the adult population, albeit still limited. Existing research on health issues within immigrant families has predominantly focused on family members such as children and spouses. However, there has been a lack of discussion regarding the health status of migrant workers, who form the primary workforce in immigrant families. Specifically, a knowledge gap exists concerning the health conditions of Chinese migrant workers within the framework of family migration, including their own health as they navigate the responsibilities of supporting family members in urban environments. This discourse explores the impact of family migration on their health. The dynamics of family migration among Chinese migrant workers may differ from those observed in other global contexts. In China, migrant workers typically relocate to urban areas in pursuit of economic opportunities. Historically, they often migrated individually, leaving other family members behind to maximize economic benefits for the family unit. However, as migrant workers recognize the potential advantages of family migration for the entire household, there is a growing trend towards migrating as a family unit, especially with children, with the aim of improving living conditions for all family members. Do the factors influencing their health differ from those influencing family migration? Does family migration enhance or detract from their health status? These are crucial questions requiring further exploration.
The current scholarly discourse lacks consensus on the impact of family migration on the health of migrant workers, indicating a substantial need for further exploration. Literature reviews reveal that studies on migrant health predominantly concentrate on occupational impacts, economic status, and the migrant health paradox, rather than family dynamics. Discussions that do address the role of family migration in influencing health outcomes often cite emotional support as a primary mechanism; however, findings in this area remain inconsistent.
This study leverages data from the China Migrants Dynamic Survey (CMDS) of 2017 to investigate the impact of family migration on the self-rated health of migrant workers. The research methodologically focuses on the total effects, mediating effects, heterogeneity tests, and Propensity Score Matching (PSM) tests, among others. This investigation is situated within the broader context of urbanization, aiming to elucidate the relationship between family migration and health outcomes among migrant workers.
The objectives of this study are multi-fold: it seeks to provide empirical support for policies concerning migrant workers’ family migration, to alleviate pressures of intergenerational support, and to augment the effective utilization of human capital resources. By doing so, this research contributes to the existing body of literature in 3 significant ways:
Ι. Focuses on the impact and mechanisms of family migration on the health of migrant workers from the perspective of family stress theory.
II. Introduces the perspective of intergenerational support in families, discusses cultural traditions related to intergenerational support in China, and engages in relevant discussions.
III. By aligning the health implications of migration with broader socio-economic processes. This approach not only deepens the understanding of migrant health dynamics but also aids in formulating targeted interventions to improve health outcomes in migrant populations.
Study Design and Data Description
In light of the above analysis, this study proposes the following hypotheses:
Hypothesis 1: Family-oriented migration negatively affects the health-maintenance capacity of first-cohort migrant workers, leading to adverse health effects.
Hypothesis 2: Family capability factors mediate the relationship between family-oriented migration and self-rated health among first-cohort migrant workers.
Hypothesis 3: There is heterogeneity in the health impacts on first-cohort migrant workers based on their family migration patterns.
Data Sources and Variables
The data for this study were obtained from the China Migrants Dynamic Survey (CMDS, 2017), which focused on rural migrant workers aged 45 years and above. In this study, the definition of the first cohort of migrant workers was individuals aged 45 years and above with rural household registration and employment. The specific definition used for inclusion in our study was those over 45 years old with rural household registration. Jin 21 defines the first cohort of migrant workers in terms of their physical health, job type, and social security. They found that migrant workers over the age of 45 years faced significant pressure in terms of employment, medical care, and income. In the working life of migrant workers, their income peaks at the age of 35 years, after which it stabilizes and then declines. 18 This decline occurs earlier than for urban residents who maintain their peak income until the age of 45, indicating that migrant workers lose job opportunities and earning capacity too early in the job market. The first cohort of migrant workers over 45 years of age faced amplified health and market livelihood risks, and their ability to resist these risks weakened. Their opportunities to continue working in urban areas have decreased, and their livelihood risks have increased. 16 Rural migrant workers aged over 45 years were selected for this study. After processing the variables, the sample contained 19 517 observations.
Variable Selection and Measurement
Dependent Variable
In this study, the health status of the migrant workers was regarded as the dependent variable. Health status was assessed by surveying the migrant workers’ self-rated health conditions. Health status is considered a multi-dimensional concept and difficult to measure. For this reason, rious proxies are used to conceptualize and measure health. existing research argues that, despite subjective measurement errors, self-rated health remains a robust indicator for predicting health conditions. Results show that sel-rated health is a highly reliable measure of individual health, and self-rated health is a valid summary measure of individual’s self-perceived and known health conditions.77,78 Self-rated health (SRH) is one of the most commonly used indicators in the health literature. 79 It can reflect an individual’s overall health status comprehensively. It is also recognized as a valid proxy for fitness, loss of functional ability, and morbidity. 80
In the CMDS (2017) questionnaire, the health status of migrant workers was divided into 4 categories: “Healthy,” “Basically healthy,” “Unhealthy but able to manage daily life,” and “Unable to live independently.” Based on existing research conclusions, this study categorizes migrant workers selected as “Basically healthy” as having potential health risks or being in a suboptimal health state. 81 The categories “Basically healthy,” “Unhealthy but able to manage daily life,” and “Unable to manage daily life due to illness” are merged into an “Unhealthy” status and assigned a value of 0, while “Healthy” is categorized under the “Healthy” status and assigned a value of 1.
This study not only used self-rated general health and self-rated health status in different dimensions, but also analyzed a series of objective health test indicators collected during the survey. These analysis not only enriched the dimensions and content of health, but also enhanced the reliability of the research results and the comparability in different populations. The use of these multidimensional, subjective and objective health indicators can not only help to comprehensively reflect the broad health conditions of different groups, but also provides an important means to accurately reveal the specific health differences of these groups.82,83
This study introduced variables such as “Have you personally suffered from illness in the past year?” and “Have you experienced the following symptoms in the past year?” in the robustness test. These variables were used for comprehensive calculations, providing a composite indicator of migrant workers’ health status that combines both subjective and objective measures. “Have you personally suffered from illness (injury) or discomfort in the past year?” is coded as 0 for yes and 1 for no, and “Have you experienced the following symptoms in the past year?” is coded as 0 for yes and 1 for no.
Independent Variable
Family migration was the explanatory variable. There is variation in the definition and operationalization of family migration in related studies, encompassing binary divisions based on the family size of migrant households (2 or 3 people), as well as diverse measurements from the perspectives of different migrant family structures or patterns. Drawing on existing academic research, this study adopts a definition of family migration in which living with 2 or more family members in the destination is considered family migration.13,84 Family migration was coded as 1, whereas other situations were coded as 0 for non-family migration.
Control Variables
Four sets of control variables were introduced based on the research requirements.
Ι. Personal characteristics of migrant workers: this included income, gender, and occupational status scores. (In the context of social stratification research, occupation is an indispensable indicator. Following the International Socio-Economic Index (ISEI) developed by Ganzeboom et al. 85 , which ensures non-overlapping and comprehensive coverage, 19 occupational categories from the CMDS (2017) data are mapped to the ISEI occupational codes. This results in occupational prestige scores ranging from 22 to 67. The weighted average of occupational prestige scores is obtained based on the proportion of each occupation in the migrant population, yielding an average score for occupational prestige.
II. Migration characteristics of migrant workers: this included migration range, duration, and willingness.
III. Individual medical conditions of migrant workers: this included medical education, medical records, and health insurance.
IV. Working conditions of first-cohort migrant workers at the job location: these encompassed the difficulties faced locally, local social network relationships, settlement intentions, and local housing conditions.
Mediator Variable
According to the theory of family stress, family difficulties can cause physiological and psychological stress in family members. In conjunction with existing research, this study considers family capability as a mediating variable, primarily focusing on 2 dimensions: family economic capability and intergenerational support within the family. Aligned with the research theme and based on the CMDS (2017) questionnaire, family economic capability was measured using indicators such as family expenses, income, housing expenses, difficulty buying a house, and job instability. Intergenerational support within the family was assessed through difficulties in children’s education, older adult care, and care for children, thus generating a new indicator of intergenerational support. These factors reflect family capability elements for the first cohort of migrant workers after family migration, justifying the selection of these indicators as mediating variables. 86
Regulated Variable
The incorporation of family social integration capacity as a moderating variable was intended to explore the connection between the family social networks of first-cohort migrant workers and their health. The key metric for assessing family social integration capacity was the response to the question, “Do local residents look down upon you?” with “yes” represented as 1 and “no” as 0.Variables and their descriptive statistics as Table 1.
Variables and Their Descriptive Statistics.

Analysis of Data Results
Descriptive of Family and Non-Family Migration of the First Cohort Migrant Workers
As this study utilizes cross-sectional survey data and the dependent variable “health” can be treated as a binary variable, the logit model is employed for regression analysis. The focus was on examining the impact of factors, such as sources of stress and economic conditions during the family migration process, on the health of the first cohort of migrant workers. Additionally, to compare the differences in the health impact between family and non-family migration, this study also conducted a heterogeneity analysis of these 2 subgroups.
When comparing family migration with non-family migration, the self-rated health of migrant workers was lower than that of non-family migrants. Specifically, for family migration, the health rate for the first cohort of migrant workers was 67.7%, whereas for non-family migration, it was 73.0%. In terms of self-reported unhealthy conditions, family migrant workers accounted for 32.3%, compared to 27.0% for non-family migrants. Statistical analysis of the heterogeneity in health between the first-cohort of migrant workers as Table 2.
Statistical Analysis of the Heterogeneity in Health Between the First-Cohort of Migrant Workers (n = 19 517).

Source. The data of CMDS 2017.
Analysis of the Correlation Regression Results
To test our hypotheses, a logit probability model was employed with the health variable as a dummy variable and 2 levels: healthy and unhealthy. The Healthi values are 1 and 0, where 1 represents a healthy status, and 0 represents an unhealthy status.
The probability of being in a healthy state:



Models 1 to 4 in Table 3 illustrate the factors influencing migrant workers’ health. Gradually introducing factors related to personal characteristics, mobility features, healthcare services, and local work and life conditions for migrant workers while excluding family-related factors, the regression results show that family migration remains significantly associated with health at a 0.1% significance level. However, the coefficient gradually decreased, and factors such as mobility and healthcare services explained the impact of family migration on the health of the first cohort of migrant workers. The results indicate that holding other conditions constant, the health score of the family migration group is only −0.22 times that of the non-migration group (e^(−0.2448) − 1 ≈ −0.22).
Multivariate Regression Analysis of the Relationship Between Family Migration and Health of the First-Cohort of Migrant Workers.

Note. The numbers in parentheses represent standard errors. ***, **, * indicate significance levels at .1%, 1%, and 5%, respectively, based on significance tests.
In terms of gender and health, using female migrant workers as the reference, the influence of family migration on men’s health gradually increases. After introducing the fourth group of control variables for migrant workers concerning local life.Regarding the housing situation of migrant workers’ families, for each increase of 1 level in housing difficulties, the self-rated health of migrant workers decreases by 0.6 times (e^(−0.9211) − 1 ≈ −0.60). This suggests that housing conditions significantly affected the health of the first cohort of migrant workers.
Concerning the settlement intentions in the destination area, for each increase of 1 level in the intention to settle, the self-rated health improve by 0.1 times (e^(−0.0939) − 1 ≈ 0.1). This indicates that the pressure on the first cohort of migrant workers to settle in a city significantly affects their health. The correlation with social relationship networks for the first cohort of migrant workers was not high, possibly because the migrant workers’ family migration disrupted their social relationship networks to a certain extent, diminishing their role in daily life.
The results obtained regarding family migration also raised some questions for the existing research in the academic community. In the existing research, rural-to-urban migration is seen as an important way to improve the health and mental health of migrant workers.87,88 However, the results of this study showed that, for the first cohort of migrant workers, migrating with their family had a negative impact on their health. The family stress theory may better explain the impact of family migration on the health of the first cohort of migrant workers. The first cohort of migrant workers were in the low-end job market with low incomes, and they tried to maximize the comparative benefits between rural and urban areas by squeezing their own consumption. However, regarding home-based migration, a family’s living expenses in the city are obviously higher than those in the countryside. Single migrant workers can be more frugal in terms of accommodation, food, and daily life. However, when they migrate with their family, their offspring need to study close to where the parents work, incurring more expenses. Therefore, the first cohort of migrant workers had to further compress their health expenditures, seek more dangerous or worse jobs to strive for higher incomes, and provide more economic support for their offspring’s development in the city. Family stress, therefore, further strengthened the health vulnerability of the first cohort of migrant workers.
In the robustness test of the relationship between family migration and health for the first cohort of migrant workers presented in Table 4, Models 5 to 7 redefine the concept of health after replacing the dependent variable. Model 5 integrates self-rated health and “Have you personally been ill in the last year?” as variables to comprehensively calculate the combined subjective and objective health statuses of migrant workers. The health variable in Model 5 is named Health1. Model 6 redefines the health variable for migrants: 1 = unable to live independently, 2 = unhealthy but able to live independently, 3 = basic health, and 4 = healthy. To distinguish it from the health variables in Table 2, the health variable in Model 6 is named Health2. Model 7 uses being sick as a variable to measure the health status of migrant workers, “Have you experienced the following symptoms in the latest year,” with 0 = sick and 1 = not sick, and it is named Health3. To distinguish them from the health variables in Table 2, the health variables in Models 5 to 6 were named Health1 and Health2.
Robustness Test of the Relationship Between Family Migration and Health of the First Cohort of Migrant Workers.

Note. The numbers in parentheses represent standard errors. ***, **, * indicate significance levels at .1%, 1%, and 5%, respectively, based on significance tests.
As the dependent variable (dependence on different health) was an ordinal categorical variable, and the independent variable comprises not only continuous variables (such as the household size) but also categorical variables (such as gender), we used the ordered logit regression model (OLOGIT) to find the factors that influence the health of the first cohort of migrant workers. The ordered logistic model is specified below:

where
The descriptive statistics of the grouped data showed a high correlation between the covariates and treatment variables, indicating a high level of similarity between the treatment and control groups in various aspects. This suggests the possible existence of a “self-selection” issue, meaning that the migration of the first cohort of migrant workers is largely influenced by external factors rather than spontaneous behavior. To enhance the robustness of the analysis, this study employed various methods such as 1:1 matching, 1:4 matching, radius matching, kernel matching, and local linear regression for propensity score matching, as shown in Table 5. The results indicate that even after eliminating systematic differences in the samples, family migration still significantly reduced the health status of the first cohort of migrant workers, and this finding was not sensitive to the matching method used.
Robustness Test of the Relationship Between Family Migration and Health of the First Cohort of Migrant Workers PSM.

To further understand the impact of family stress factors on the health status of the first cohort of migrant workers during the process of family migration, mediation analyses were conducted using family economic capabilities and intergenerational support as intermediary variables. Family economic capability was measured comprehensively using indicators such as family expenditure, family income, housing expenditure, difficulty buying a house, and difficulty finding stable employment. Intergenerational support was analyzed as a composite variable using indicators related to children’s education, older adult care, children’s educational expenses, and childcare.
To test whether family factors mediate the relationship between family migration and migrant workers’ health, this study employs the KHB method. The results in Table 6 show that the 2 variables reflecting family stress serve as mediators between family migration and the health of migrant workers. Specifically, 4.869% of the overall impact of family migration on migrant workers’ health (−0. 0026/(−0. 0026+(−0. 0508))) was attributed to household economic capability, and 12.337% of the overall impact (−0.0066/(−0.0066+(−0. 0469))) was attributed to intergenerational support. These results confirm that family stress factors are indeed one of the factors that influence the impact of family migration on the health of migrant workers, validating Hypotheses 1 and 2. The analysis suggests that under the pressure of family economic stress and intergenerational support, especially in terms of children’s education and older adult care, the first cohort of migrant workers must cut their health expenditures to meet the needs of intergenerational support, leading to a decline in their health status.
The Mediating Effect of Family Migration on the Relationship Between Health and the First Cohort of Migrant Workers.

Note. The standard was obtained by mistakenly passing the Bootstrap method after repeated sampling 500 times.
Table 7 further examines the moderating effects of .social integration on the health factors of the first cohort of migrant workers. In Model 8, the main effects are analyzed, and Model 9 introduces the interaction term. Model 8 shows that .social integration improves the health status of the first cohort of migrant workers, whereas migration has a negative impact on health. However, the .social integration analysis in Model 9 clearly indicates that the impact of .social integration on health is distinctly different. With other conditions unchanged, the regression coefficient of the interaction term characterized the nonlinear effects of social integration and migration on health. This finding indicated a mutually weakening relationship between the effects of social integration and migration on the health of the first cohort of migrant workers. For migrant workers, an increase of 1 level in social integration improves health by 3.65% (e^(0.1919 − 0.1756) − 1 ≈ 0.0365), suggesting that social integration can effectively enhance the health status of migrant workers.
The Moderating Effect of Family Migration on the Relationship Between Health and the First Cohort of Migrant Workers.
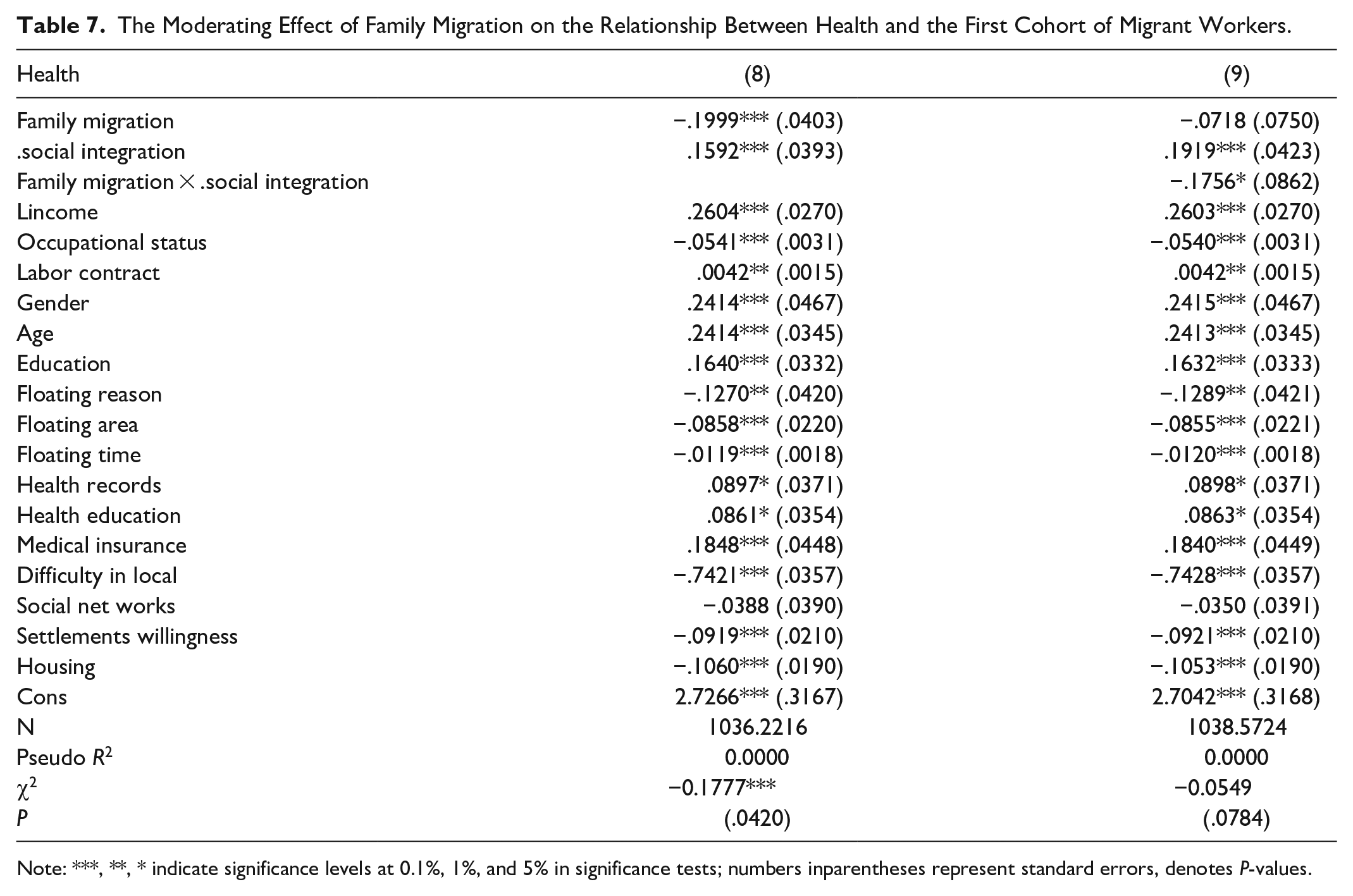
Note: ***, **, * indicate significance levels at 0.1%, 1%, and 5% in significance tests; numbers inparentheses represent standard errors, denotes P-values.
The Instrumental Variable (IV) method is a practical approach to addressing endogeneity based on the fundamental principle of identifying a variable (instrumental variable) that is correlated with the endogenous variable but unrelated to the random error term. In this study, whether an individual has contracted land was considered an instrumental variable that influences family migration. Effective instrumental variables must satisfy both the relevance and exogeneity requirements. Existing research indicates a significant negative correlation between the per capita contracted land quantity in rural areas and the outward migration trend, implying that more per capita land capital weakens the migration trend.89,90 Therefore, land tenure is an important institutional factor restricting the outward migration of the floating population. This study posits that migrant workers’ family migration is related to the land they have contracted and that they are more inclined toward family migration after transferring land tenure. In terms of exogeneity, land tenure is typically exogenous to the health status of the migrant population. According to Chinese land tenure regulations, contracted land is the right of members of rural collective economic organizations to contract rural land allocated by their collective economic organizations legally. Therefore, whether an individual owns contracted land is mainly a result of institutional arrangements and is unrelated to health status. In the investigation of the correlation between long-distance migration among migrant workers and their health, research employs the variable “individual land contracting status” as an instrumental variable for long-distance migration. 91
Additionally, both the Kleibergen-Paap rk LM test and the Hansen J test reject the null hypothesis, suggesting satisfaction with the underidentification and overidentification tests. The regression results in the second stage show that, after introducing the instrumental variable, the estimated coefficient remains significant at the 1% level, and the direction of the estimated coefficient has not changed. Family migration continues to have an adverse effect on the physical health of the first cohort of migrants. This implies that endogeneity bias has not significantly affected the robustness of causal inference, and the causal relationship is robust.
Table 8 reports the estimation results of 2SLS. If the first-stage estimate of 2SLS is weak, the effectiveness of the IV estimation may be affected by finite-sample bias and low asymptotic efficiency. Following the empirical rule proposed by Staiger and Stock, 92 most tests correlate the magnitude of distortion with the first-stage F-statistic. The results in Table 8 show that the first-stage F-value is 79.65, significantly higher than the 10% bias threshold of 16.38 for a single endogenous regressor, as indicated in the weak instrument literature.93,94 Moreover, the t-value of the instrumental variable passes the test at the 0.1% significance level. In terms of asymptotic efficiency, the precision of IV estimation increases with the correlation between the instrumental variable and the endogenous variable. The general measure of this correlation is the partial R2 of the excluded instrumental variable in the first stage. Nelson and Startz 95 suggest that if the R2 of the bias-corrected part does not reach the reciprocal number of observations, weak instrumental variables are likely. The results of this study show that the R2 of the bias-corrected part is 0.1128, greater than the reciprocal number of observations (19 146). Therefore, the null hypothesis of weak instrumental variables can be rejected, indicating a strong correlation between the instrumental variable selected in this study and the core explanatory variable, namely migration.
The Endogeneity of Family Migration and Health of First Cohort of Migrant Workers: An Instrumental Variable Regression Approach.

Note. ***, **, * indicate significance levels at .1%, 1%, and 5% in significance tests; numbers in parentheses represent standard errors, denotes P-values, { } indicates the 10% critical value for the Stock-Yogo weak identification test.
Migrant workers’ roles and family responsibilities evolve across different life stages. The roles and pressures experienced by the first cohort of migrant workers vary based on distinct family migration patterns. Table 9 highlights the 4 selected family migration patterns, spouse migration, only children migration, spouse and child migration, and other migration types. Models 10 to 13 elucidate the nuanced impact of these diverse family migration patterns on first-cohort migrant workers’ health. The regression results underscore that while the correlation between different family migration patterns and migrant workers’ health remains significant at the .1% level, the coefficients exhibit changes.
Heterogeneity Analysis of the Impact of Family Migration Patterns on the Health of the First Cohort of Migrant.

Note. ***, **, * indicate significance levels at .1%, 1%, and 5% in significance tests; numbers in parentheses represent standard errors.
Migrant workers experience shifts in their roles and family responsibilities as they progress through different stages of life. The pressures faced by the initial group of these workers are influenced by various family migration patterns. Specifically, Table 9 delineates 4 primary types of family migration: migration of the spouse alone, migration of only the children, migration of both spouse and children, and other types of migration. In analytical Models 10 to 12, the subtle effects of these distinct migration patterns on the health of the first cohort of migrant workers are thoroughly examined. The regression analysis emphasizes that the relationships between various family migration patterns and the health outcomes of migrant workers are statistically significant, with a confidence level of 0.1%. However, it also highlights that the magnitudes of these effects, as represented by the coefficients, vary.The findings from Models 10 to 12 illustrate that the self-rated health of the first cohort of migrant workers who migrated only with spouses is 0.066 percentage points higher than those who migrated solely with children. Additionally, it is 0.0617 percentage points higher than the self-rated scores of those who migrated with both spouses and children.
In Model 13, there was no observed correlation between non-core family migration patterns and the health self-rated of first-cohort migrant workers. This research suggests that varying family migration patterns are associated with differences in stress levels among migrant workers, which in turn affect their health. Specifically, migration involving the core family appears to have a more significant influence on migrant workers’ health, likely due to the role of intergenerational support within Chinese family culture. The study confirms Hypothesis 3 by demonstrating that different family migration patterns have varied impacts on the health of migrant workers.
Conclusion
Firstly, regardless of other variables, the regression analysis shows a statistically significant negative correlation between family migration and health, with a significance level of 0.1%. This detrimental impact remains consistent even after rigorous tests using self-rated and objective health measures as dependent variables, and when addressing potential biases through instrumental variable methods.
Secondly, family dynamics mediate the effect of family migration on the health of migrant workers. Using the KHB method, the results reveal that family economic pressure and intergenerational support are significant mediators in this relationship. This highlights the crucial role of family stress factors in determining how family migration affects the health of migrant workers.
Thirdly, for first-cohort migrant workers, family migration supports their social integration. This mitigates the social isolation these workers often face and subsequently improves their self-rated health.
Lastly, the patterns of family migration differ in their impact on migrant workers’ health. Core family migration, a process reflecting the tradition of downward intergenerational support in Chinese families, significantly affects their health outcomes.
Family-Centered Perspective on Migrant Workers’ Family Migration
Carrington et al. 96 posit that the family migration process is characterized by phased and dynamic patterns, suggesting that migration decisions are rationally made based on the collective interests of the family rather than individual benefits. This view is supported by the theory that migration aims to optimize family well-being, which encompasses both economic and social rationality, particularly within the context of Chinese cultural traditions where family unity is paramount over individual self-interest. 97 The decision for migrant worker families to relocate is thus deeply rooted in familial considerations and the pursuit of comprehensive family values, rather than merely economic incentives. Such migrations often aim to secure better educational opportunities for children and to ensure a complete family life, providing emotional and economic support to all family members. 98 In this dynamic, migrant workers leverage family resources to the maximum, offering economic support especially to those family members who are not in the workforce. Nonetheless, this mobilization of resources can lead to familial strains, as the economic and emotional burdens may crowd out the needs of other family members, consequently imposing additional economic, health, and psychological stresses within the household.
Family Stress “Crowding-Out Effect” in Family Migration
Influenced by a family-centric culture, Chinese society places significant emphasis on the internal value system, complete family structures, and the operational dynamics of the family unit. 99 This cultural framework fosters a distinctive pattern of intergenerational support, often characterized by an asymmetric distribution of family resources and the prevalence of downward mobility within the familial hierarchy.100,101 Such dynamics lead to unique stress distributions among family members across different age groups, particularly impacting the first cohort of migrant workers who shoulder considerable responsibilities in sustaining family functionality. 102
These migrant workers, who often assume parental roles, experience significant stress levels, a phenomenon similarly observed in the United States among immigrant families. Researchers have noted that the obligation towards family welfare compels these immigrants to undertake more demanding work, exacerbating their stress levels. In the U.S, immigrants predominantly occupy low-wage, low-status jobs due to limited technical skills, with nearly 18% living below the poverty line. 103 Unlike their local counterparts, these families are frequently ineligible for welfare benefits, which significantly intensifies the familial pressure. 104
This scenario mirrors the experiences of migrant worker families in China, particularly after their transition to urban settings. The first-generation migrants typically invest a substantial portion of their family savings in their children’s education and upbringing, resulting in living expenses that far exceed those in rural areas. Consequently, these families often reduce their consumption, especially in health-related expenditures, driven by a long-term strategy focused on their children’s future development.
The Lag of Public Social Welfare Policy Supply for Family Migration
Mincer’s theory of rational family migration suggests that while the overall welfare of a migrating family increases, the individual welfare of its members may not progress uniformly. This phenomenon can result in a “spillover effect,” where the welfare of some family members is enhanced, and a “crowding-out effec,” where the welfare of others is diminished due to the increased welfare of some. 105 This study largely corroborates the “crowding-out effect” experienced by migrant families, particularly among migrant workers in urban China. Despite improvements by the Chinese government in providing public services to migrant workers, these families continue to face increasing pressures in housing, healthcare, education, and so on. These pressures, often exacerbated by insufficient public social welfare provisions, force migrant workers to rely heavily on their limited private resources. In turn, this reliance on private resources for economic gains often leads to health sacrifices.106,107
Moreover, this research underscores the persistent anxieties faced by migrant families concerning unemployment, children’s education, and other life stresses driven by economic pressures. These factors significantly impact the mental health of migrant workers.108,109 The initial decision of migrant workers to seek better economic opportunities to support their families, followed by a transition to a more stable job in the city, represents a strategic yet fragmented approach to family migration. However, the engagement in low-wage, precarious jobs (categorized as dirty, difficult, dangerous, and demeaning or 4D jobs) often leads to higher living costs post-migration, transferring significant financial pressures onto the migrant workers and diminishing their ability to maintain health and quality of life.17,42
Study Contributions and Limitations
This study highlights the complexities and dilemmas faced by the first cohort of migrant workers during the urbanization process in China. It challenges the assumption that family migration inherently provides better psychological support and health maintenance. Instead, it reveals how delayed basic public services, coupled with high urban living costs and institutional constraints, notably the household registration policy, adversely affect the living standards of migrant worker families. This study advocates for a focus on the resilience and resourcefulness of migrant families, suggesting that positive social change is possible when host societies bolster this resilience with adequate social support.
Study Limitations
First, it relied on cross-sectional data, and owing to existing limitations in data collection, it was challenging to achieve a clear before-and-after comparison of the health status of the first cohort of migrant workers. Specifically, comparing health status before and after engaging in labor work is constrained by the data available.
Second, this study did not provide a comparative analysis of the health status of urban populations in the same age group. It remains unclear whether the health status of urban residents in the same age group was superior to that of the migrant workers in this study. Currently, there is a lack of clear data for such comparisons, making it difficult to determine how migrant workers’ mobility and 4D employment patterns affect their capacity for medical health maintenance.
Footnotes
Author Contributions
FQ made the conceptualization, designed methodology, wrote the main manuscript text and reviewed and edited. HZ prepared from Tables 1 to ![]() . FQ was responsible for funding acquisition. All authors have reviewed the manuscript.
. FQ was responsible for funding acquisition. All authors have reviewed the manuscript.
Availability of Data and Materials
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Philosophy and Social Science of Anhui Province Office, Grant number: AHSKY2022D172. Anhui Province Federation of Social Science, Grant number: 2022CX105.
Ethics Approval and Consent to Participate
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Georgia State University (H21264; 18 November 2020).
Consent for Publication
All authors contributed to the article and approved the submitted version. All authors have read and agreed to the published version of the manuscript. Informed consent was obtained from all subjects involved in the study.