
Abstract
Behavioral health crisis care (BHCC) is a care delivery model for individuals experiencing acute distress related to a mental health or substance use disorder. We examined market factors associated with comprehensive BHCC availability using 2022 data on mental health treatment facilities (n = 9385) obtained from the Substance Abuse and Mental Health Services Administration. We aggregated facility-level data by county (n = 3142) and merged with county-level market factors. Logistic regression models were used to examine the adjusted associations between market factors and BHCC availability. We found that 468 (14.9%) counties had at least one mental health treatment facility offering comprehensive BHCC services. Specifically, counties with more mental health providers (Adjusted Odds Ratio = 2.26, Confidence Interval = 1.32-3.86) and metropolitan counties (AOR = 3.26, CI = 1.95-5.43) had higher odds of having a comprehensive BHCC facility. Our findings highlight the importance of developing the mental health workforce to increase BHCC availability and a need to address disparities in rural counties.
While behavioral health crisis care services are recommended as best practices, less than 10% of mental health treatment facilities offer comprehensive services, limiting access to care.
This study identifies market factors associated with comprehensive behavioral health crisis care availability.
By applying resource dependence theory to study comprehensive behavioral health crisis care availability, this study expands the application of the theory to a new context and generates insights into factors that policy makers may address to increase access to care.
Introduction
Behavioral health crisis care (BHCC) is a care delivery model designed to meet the needs of individuals experiencing acute distress related to a mental health (MH) and/or substance use disorder.1 -3 As defined by the Substance Abuse and Mental Health Services Administration (SAMHSA), BHCC includes emergency behavioral health services available on a 24/7 walk-in basis to all patients, regardless of ability to pay. 3 Additionally, BHCC best practice guidelines from SAMHSA state that facilities should provide comprehensive services, including the following: emergency psychiatric walk-ins, crisis intervention teams, onsite stabilization, mobile crisis responses, suicide prevention, and peer support specialists. 3 When implemented effectively, BHCC offers a promising alternative to the emergency department for individuals experiencing a behavioral health crisis.1 -3
In addition to promising potential for diverting emergency department visits, comprehensive BHCC services also offer an opportunity to provide more appropriate, patient-centered care.4 -7 Yet, despite SAMHSA recommendations, most MH treatment facilities have not fully adopted best practice BHCC services.8 -12 As of 2022, only 1 in 20 MH treatment facilities offered comprehensive BHCC best practices. 12 Recent studies examining the availability of crisis intervention teams and mobile crisis services have identified disparities in rural counties,10,11 whereas other BHCC services have only been described at the state-level.8,9,12 Thus, additional research is needed as no study has examined county-level market factors associated with comprehensive BHCC services. Without a better understanding of the factors associated with comprehensive BHCC availability, policy makers are unable to formulate policies that encourage service adoption in counties with the greatest need.
The current study aims to examine market factors associated with availability of BHCC services offered by MH treatment facilities in the US. We apply resource dependence theory (RDT) to guide the conceptualization of the market for BHCC services, expanding the application of this theory to a new health care setting. Policymakers and funding bodies may use our findings to address disparities in access to BHCC through policy changes or distribution of resources to underserved communities.
New Contribution
While there is a growing body of evidence demonstrating the value of BHCC services as evidence-based best practices for delivering care to patients in crisis, there is limited research on the factors influencing availability of these services. A deeper understanding of environmental market factors that may influence availability of comprehensive BHCC services is needed to address low uptake of these services among MH treatment facilities. Our study fills this knowledge gap by applying RDT to conceptualize the market of MH treatment facilities. We take advantage of SAMHSA’s Behavioral Health Treatment Locator Tool, an underutilized resource that allowed us to identify the exact locations of MH treatment facilities and services offered at the time data were downloaded. This facilitated our ability to conduct analyses at the county-level rather than the state-level, providing more granular detail than previous studies on BHCC service availability at the state-level.
To our knowledge, this is the first study to apply RDT to holistically examine county-level market factors associated with several BHCC services that have been recommended by SAMHSA as best practices. Additionally, we created a composite indicator to measure comprehensive BHCC availability. Examining market factors associated with comprehensive BHCC availability is an important question, as when services are not implemented comprehensively, care may be fragmented and inadequate. By filling this knowledge gap, our study is responsive to recent calls for research that helps ensure access to evidence-based innovations in behavioral health care are widely available. 13 Findings from our study can help guide future research on adoption and implementation of BHCC services.
Conceptual Framework
Resource dependence theory (RDT) argues that organizations acquire resources from their external environments through various strategies to reduce uncertainty and increase their chances for survival.14,15 From this perspective, organizational survival depends on how well an organization functions within its external environment, 16 and organizations face the threat of closure if they cannot secure enough resources. 17 RDT has been applied to study the provision of various services, such as IT adoption, emergency services, and community assessments by hospitals, health departments, nursing homes, and medical practices. 15 Thus, RDT is well-suited for examining BHCC services offered by MH treatment facilities. Three constructs encompass the resources and uncertainty in an organization’s environment: munificence, dynamism, and complexity. 18
Munificence
Munificence represents resource abundance in the environment. Organizations operating in munificent environments are able to offer a wider range of tactics in pursuit of goals, 17 and are more likely to adopt innovative strategies. 19 In the context of MH treatment facilities, resources may be conceptualized as patients, providers, and payments which drive demand for services and influence the organization’s survival. Thus, thinking of patients as a resource, MH treatment facilities may be more likely to offer BHCC best practices in communities with high rates of patients with unmet behavioral health needs as this translates to greater demand for services. One way of capturing unmet patient needs is through assessment of mental distress, a quality-of-life measure that indicates individuals with unmet behavioral health needs who are at risk of experiencing a crisis, in the community. 20
Not only do MH treatment facilities need patients, they rely on their patients’ ability to pay for services. As a proxy for ability to pay for health care services, previous studies have used income levels and insurance rates when operationalizing resources essential to a munificent environment.15,17,21 Given that MH treatment facilities need mental health providers (MHPs) on site to provide services, MHPs are another valuable resource. Finally, urban versus rural geographic area serves as a measure of munificence, as organizations in urban areas may have access to more environmental resources than those available to facilities in rural areas. 15
Hypothesis 1: Mental health treatment facilities operating in more munificent environments are more likely to offer behavioral health crisis care best practices compared to those operating in less munificent environments.
Dynamism
Dynamism represents how much change is taking place in that environment, or how stable the environment is. Dynamism is typically operationalized as the degree of instability and uncertainty in the external environment. 15 An environment that constantly changes results in greater uncertainty for decision-makers. 15 Thus, decision-makers in environments with high levels of uncertainty may be less likely to take risks or adopt new strategies. 22 A key characteristic of BHCC is providing services to anyone, anywhere, at any time. 3 The uncertainty around offering BHCC services can pose a challenge for MH treatment facilities as it can be difficult to maintain the necessary infrastructure and capacity to offer services. Thus, MH treatment facilities may be more likely to offer BHCC services in communities where the environment is stable, and subsequently more predictable. Changes in population size and unemployment rates have previously been used to operationalize dynamism in the environment.17,23 These measures are also appropriate for the current study, as changes in population size and unemployment rates may influence demand for BHCC.
Hypothesis 2: Mental health treatment facilities operating in more dynamic environments are less likely to offer behavioral health crisis care best practices than those operating in less dynamic environments.
Complexity
Complexity represents environmental factors that complicate decision making or access to resources in the environment. 15 In the context of MH treatment facilities, barriers that reduce access to services or policies that influence payment amounts may be operationalized as complexity, as such barriers make it more challenging for MH treatment facilities to acquire patients. For example, stigma towards behavioral health disorders is a well-established phenomenon 24 which can deter individuals from seeking care (reducing demand for services) and impede efforts to direct government funding towards behavioral health services.25 -28 Previous studies have demonstrated that political liberals are less likely to hold stigmatizing attitudes and are more likely to support policies that increase funding for behavioral health treatment than conservatives. 28 Thus, the political affiliation of the community that MH treatment facilities are located in can be operationalized as a measure of complexity since communities with a higher percentage of political conservatives may hold more stigmatizing attitudes.
Additionally, previous research has demonstrated that minority racial groups face greater stigma associated with utilizing behavioral health services.29,30 Cultural and contextual factors, such as racial discrimination, may act as barriers and may reduce willingness to receive treatment.30,31 Furthermore, serving a diverse population in an effective and sustainable way requires that MHPs adapt and learn about cultural beliefs, values, and practices in order to provide culturally competent care.32 -34 Thus, racial and ethnic diversity within the county is operationalized as a measure of complexity for this study.
Hypothesis 3: Mental health treatment facilities operating in more complex environments are less likely to offer behavioral health crisis care best practices than those operating in less complex environments.
Methods
Sample and Design
This study uses a cross-sectional design to analyze the relationship between market factors and BHCC availability. Secondary data were obtained from the following sources: SAMHSA’s National Mental Health Services Survey (N-MHSS), 35 County Health Rankings (CHR), 20 Area Health Resources File (AHRF), 36 U.S. Department of Agriculture (USDA), 37 and Presidential Election Returns (PER). 38 The MH treatment facilities included in this study were identified using a list from SAMHSA’s Behavioral Health Treatment Services Locator tool, 39 which was downloaded on January 8, 2022. Residential treatment facilities, facilities owned by the U.S. Department of Veterans Affairs, and facilities outside of the U.S. were excluded.
Dependent Variables
The 2021 N-MHSS data for MH treatment facilities across the U.S. were obtained from SAMHSA’s Behavioral Health Treatment Services Locator tool, which can be accessed at https://findtreatment.samhsa.gov/. This online, searchable database includes information on MH treatment facilities surveyed as part of the N-MHSS, which includes nearly all public and private U.S. facilities offering MH services. Importantly, while this database is informed by the N-MHSS, it is also updated on a weekly basis when facilities notify SAMHSA of changes in services, making it the most up-to-date source of information on service availability. 39
The main dependent variable, availability of a comprehensive BHCC facility, was determined by at least 1 MH treatment facility in the county indicating that they serve all age groups and provide all of the following services: emergency psychiatric walk-ins, crisis intervention teams, onsite stabilization, mobile crisis responses, suicide prevention, and peer support specialists. Consistent with a previously published methodology, 12 we created a binary composite outcome indicating whether a facility comprehensively offers all BHCC services. These services were selected as SAMHSA recommends them as critical components of a comprehensive crisis response system in order to prevent gaps in access to care. Additionally, information on whether MH treatment facilities offer each of these services is captured in the N-MHSS and represented in the Locator data.35,39
Because we were interested in the availability of BHCC services at the county-level, we aggregated data on MH treatment facility (n = 9385) services to the county-level (n = 3142) to determine whether each county had at least 1 MH treatment facility offering comprehensive BHCC services. Given our use of nationally representative data sources, we were able to include all US counties in our sample (n = 3142). In addition to examining availability of comprehensive BHCC facilities, we also examined availability of at least 1 MH treatment facility offering each of the aforementioned individual services at the county-level.
Independent Variables
The independent variables used to operationalize RDT constructs in this study are presented in Table 1. Data on variables representing county-level munificence were extracted from the 2021 CHR, 20 including reported rate of mental distress, median household income, percent insured, and the number of MHPs per capita. Geographic location was measured using the most recently available 2010 Rural-Urban Commuting Area (RUCA) Codes from the USDA. 37 To represent dynamism, data on county-level unemployment and population size were obtained from the 2021 AHRF. 36 Change in unemployment and change in population size were both calculated by taking the absolute value of the percent change over a 5-year period from 2016 to 2021. Variables representing complexity include political affiliation and county diversity. Political affiliation is measured as the percent of individuals who voted republican in the county, obtained from the 2020 Presidential Election Returns. 38 County diversity is measured using an index score that measures diversity across the following racial groups: African Americans, American Indians or Alaskan Natives, Asians, Native Hawaiians or other Pacific Islanders, Hispanics, and non-Hispanic Whites.30,40,41
Variables and Data Sources Used in the Current Study.
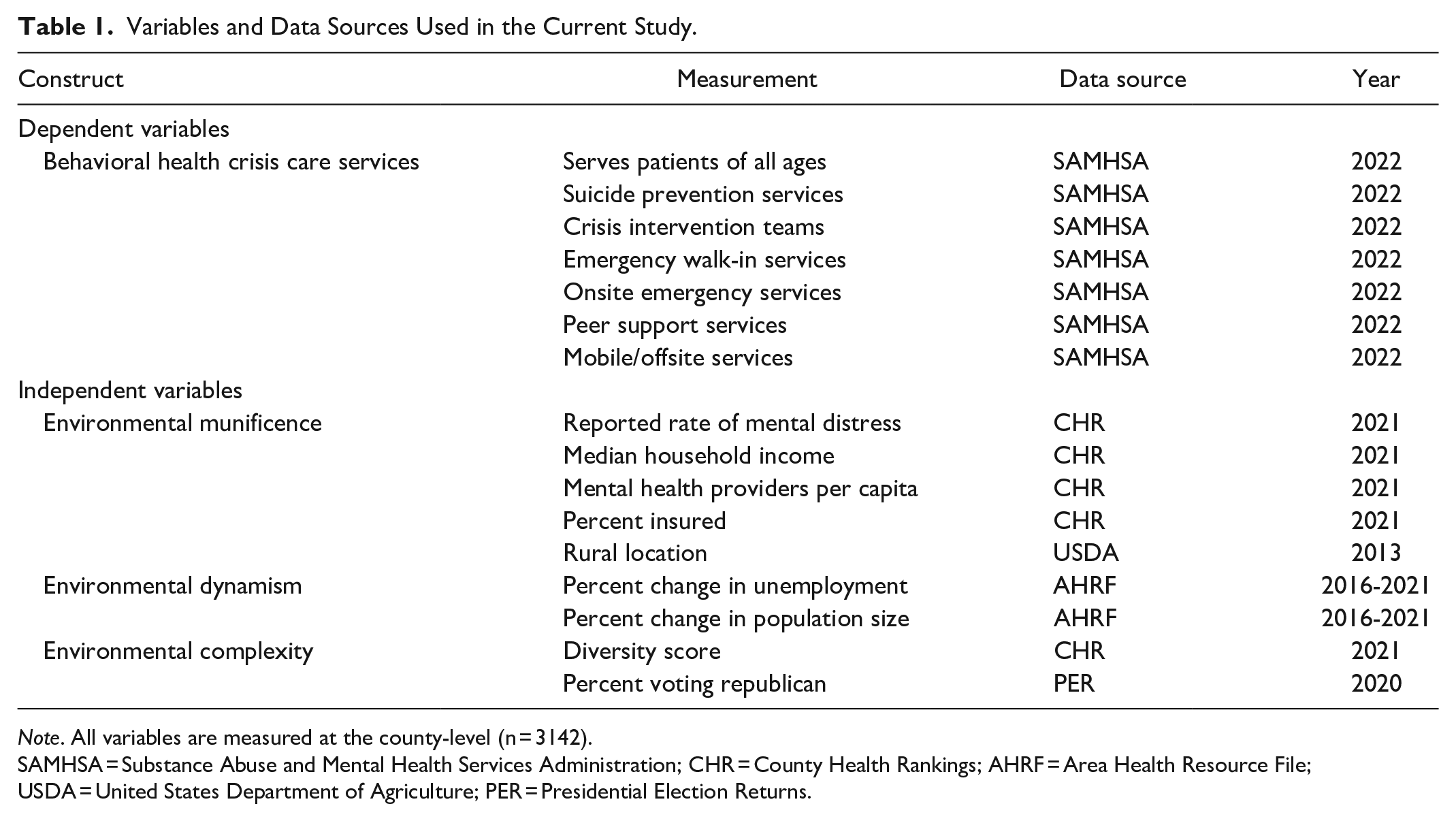
Note. All variables are measured at the county-level (n = 3142).
SAMHSA = Substance Abuse and Mental Health Services Administration; CHR = County Health Rankings; AHRF = Area Health Resource File; USDA = United States Department of Agriculture; PER = Presidential Election Returns.
Due to concerns around multicollinearity and a lack of linearity in the logit for several independent variables, we transformed most of the independent variables into categorical variables coded 1-4 based on corresponding quartiles (Quartile 1 = 1, Quartile 2 = 2, Quartile 3 = 3, Quartile 4 = 4). Additionally, we transformed geographic area into a categorical variable using pre-defined RUCA classifications, with 4 indicating metropolitan, 3 indicating micropolitan, 2 indicating urban, and 1 indicating frontier (rural).
Statistical Analyses
Data was initially obtained for the study on January 8, 2022 and all analyses were conducted between January 2022 and February 2024. We used bivariate analyses (chi-squares) to examine associations between each independent variable and availability of a comprehensive BHCC facility. A series of logistic regression models described the adjusted association between each independent variable and BHCC availability. Given the nesting of MH treatment facilities within states in our dataset, we adjusted our regression models to account for clustering by state. Statistical analyses were conducted using Stata SE17.0.
Results
All 3,142 counties across the U.S. were included in analyses (Table 2). About two-thirds of all U.S. counties (66.1%, n = 2078) have a MH treatment facility that serves all age groups. Suicide prevention was the most common BHCC service, offered by MH treatment facilities in 64.9% of counties (n = 2040), followed by crisis intervention teams (60.1%, n = 1887). Just under half of all U.S. counties have a MH treatment facility that offers emergency walk-in services (49.7%, n = 1561), onsite crisis stabilization services (48.9%, n = 1538), and peer support specialists (48.0%, n = 1507). Finally, 39.6% (n = 1245) of counties have a MH treatment facility that offers mobile/offsite services, making this the least common BHCC service.
County-level Availability of Behavioral Health Crisis Care (BHCC) Services and Environmental Market Factors (n = 3142).

Note: All variables are measured at the county-level. A comprehensive BHCC facility is defined as having at least 1 mental health treatment facility in the county that offers all specified BHCC services and serves all ages.
Bivariate associations between all independent variables and comprehensive BHCC availability are presented in Table 3. Counties with a comprehensive BHCC facility were more likely to have higher rates of reported mental distress (P = .006), have lower median household income (P < .001), have more MHPs per capita (P < .001), and be located in metropolitan areas (P < .001). Counties with a comprehensive BHCC facility were also more likely to have lower rates of change in unemployment (P < .001), higher diversity scores (P < .001), and a lower percentage of individuals voting Republican (P < .001).
Bivariate Associations Between County-level Environmental Market Factors and Comprehensive BHCC Facilities (n = 3142).
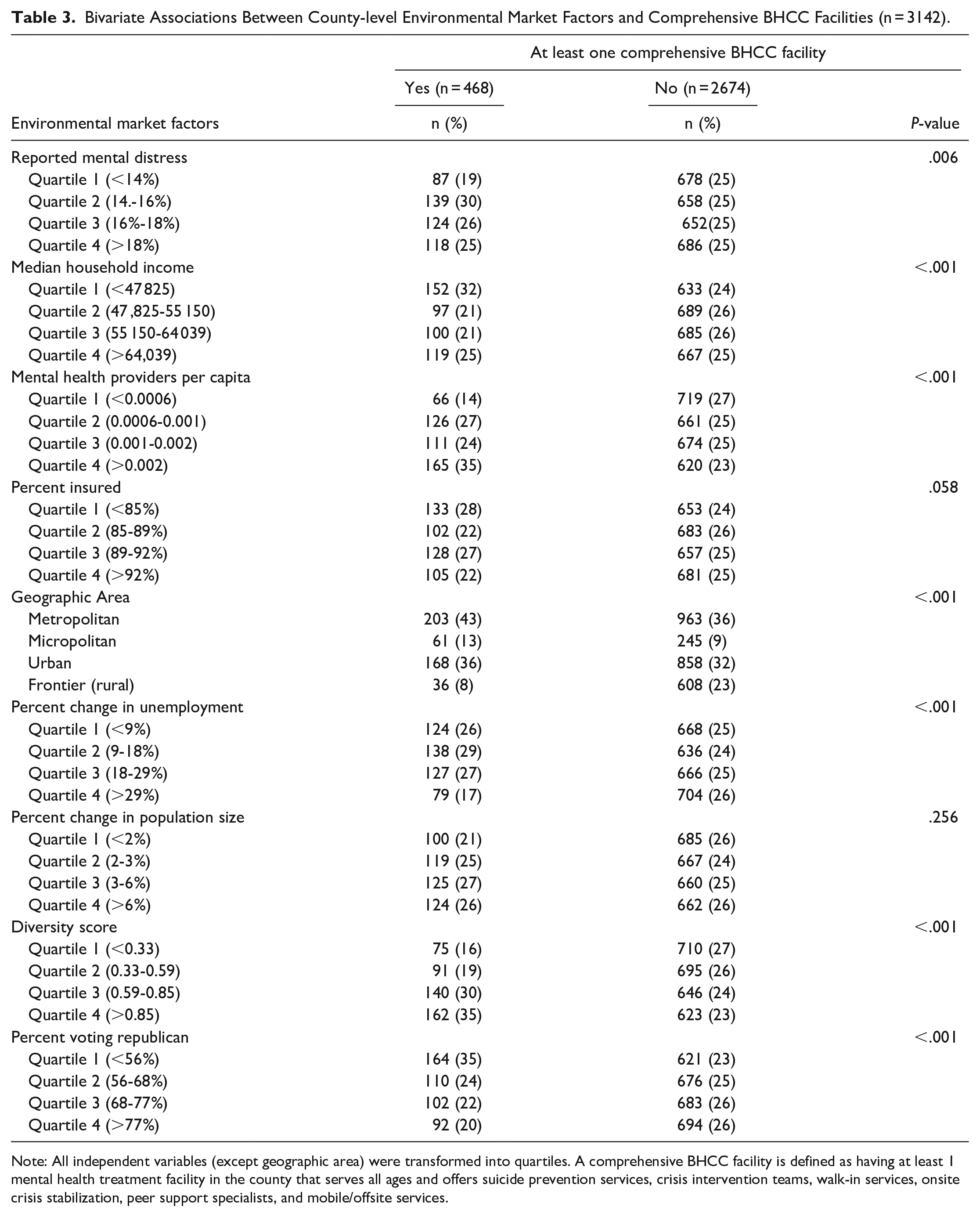
Note: All independent variables (except geographic area) were transformed into quartiles. A comprehensive BHCC facility is defined as having at least 1 mental health treatment facility in the county that serves all ages and offers suicide prevention services, crisis intervention teams, walk-in services, onsite crisis stabilization, peer support specialists, and mobile/offsite services.
Multivariate associations between market factors and BHCC availability are presented in Table 4. Among variables representing munificence, counties with the highest levels of reported mental distress had higher odds of having a MH treatment facility that offers suicide prevention services (Adjusted Odds Ratio = 2.76, CI = 1.53-4.98), crisis intervention teams (AOR = 2.17, CI = 1.08-4.39), walk-in services (AOR = 2.42, CI = 1.40-4.17), onsite crisis stabilization (AOR = 2.62, CI = 1.46-4.70), and peer support specialists (AOR = 2.26, CI = 1.25-4.09) compared to counties with the lowest levels of mental distress. Counties with the most MHPs per capita had higher odds of having a comprehensive BHCC facility (AOR = 2.26, CI = 1.32-3.86) and higher odds of having a MH treatment facility that offers each individual service examined (AOR range: 2.43-5.23). Urban, micropolitan, and metropolitan areas had higher odds of having a comprehensive BHCC facility (AORs = 3.06, 3.63, 3.26, respectively) and a MH treatment facility that offers each individual services compared to frontier (rural) counties (AOR range: 2.28-6.43).
Multivariate Associations Between County-level Environmental Market Factors and Availability of BHCC Services (N = 3142).

Note: Reference group for geographic area is frontier (rural). For all other variables, Quartile 1 is used as the reference group. “Comprehensive” is defined as having at least 1 mental health treatment facility in the county that serves all ages and offers suicide prevention services, crisis intervention teams, walk-in services, onsite crisis stabilization, peer support specialists, and mobile/offsite services. Bolded values indicate statistical significance at the P < .05 level. AOR = adjusted odds ratio.
Among variables representing dynamism, counties with the highest change in population size had lower odds of having a MH treatment facility that offers suicide prevention services (AOR = 0.69, CI = 0.54-0.88), crisis teams (AOR = 0.68, CI = 0.52-0.88), walk-in services (AOR = 0.68, CI = 0.49-0.93), and onsite crisis stabilization services (AOR = 0.62, CI = 0.45-0.86). Among variables representing complexity, counties with the highest diversity score had higher odds of having a MH treatment facility that offers walk-in services (AOR = 1.79, CI = 1.15-2.81), onsite services (AOR = 0.62, CI = 0.45-0.86), and mobile/offsite services (AOR = 2.17, CI = 1.26-3.76). Counties with the highest percent of individuals voting Republican had lower odds of having a MH treatment facility that offers suicide prevention services (AOR = 0.52, CI = 0.32-0.85) and crisis teams (AOR = 0.60, CI = 0.38-0.95).
Discussion
Despite SAMHSA recommendations that MH treatment facilities offer comprehensive BHCC services, 3 few facilities currently do so. As efforts to implement the national mental health crisis lifeline (988) are underway, 10 understanding factors that influence adoption of BHCC best practices is particularly salient to ensure access to high-quality, patient-centered care. The current study contributes to how environmental munificence, dynamism, and complexity are associated with comprehensive BHCC availability, filling an important gap in the BHCC literature. We found partial support for the use of RDT constructs to explain the influence of environmental market factors on BHCC availability. The hypothesis pertaining to munificence was most strongly supported by our findings, whereas we found limited support for the hypotheses pertaining to dynamism and complexity. Previous studies applying RDT to other health care settings have reported similar findings.17,42
Our results suggest that more munificent counties are more likely to have MH treatment facilities that offer BHCC services. Most notably, counties with more MHPs had higher odds of having a comprehensive BHCC facility, as well as higher odds of having a facility that offers every single type of individual BHCC service examined in our analyses. This finding highlights the importance of MHPs as a resource to MH treatment facilities. Workforce shortages that limit access to affordable behavioral health care have been a recognized challenge for decades, 43 and BHCC services are no exception. BHCC models often rely on a mix of providers, including licensed MHPs and peer support specialists. 1 In areas that have a shortage of MHPs, MH treatment facilities may struggle to recruit and retain staff needed to adopt BHCC services. In order to increase adoption of services, policymakers may want to consider strategies for training more MHPs and building a stronger workforce.1,43 Future research should further explore workforce challenges faced by MH treatment facilities that may influence adoption and implementation of BHCC best practices.
Additionally, our findings highlight disparities in access to BHCC in rural counties, further supporting previous literature and suggesting that existing MH treatment facilities located in rural areas may be lacking the environmental resources needed to offer comprehensive services.1,10,11 We found that facilities in metropolitan, micropolitan, and urban geographic areas have higher odds of offering all BHCC services. While rural areas may differ from urban areas in a variety of ways, a lack of organizations to partner with in rural areas may be one factor contributing to this disparity. 1 Strong community partnerships, including law enforcement, first responders, jails, and schools, are needed to divert individuals from less appropriate settings and successfully implement BHCC. 1 It is also possible that MH treatment facilities in rural areas may face additional challenges when recruiting MHPs. Policy makers and grant funding bodies may be able to mitigate disparities in access to BHCC by directing resources to help foster community partnerships and support adoption of services in rural communities.10,11 Future research should further explore differences in adoption and implementation challenges faced in rural communities.
The rate of individuals experiencing mental distress (i.e., potential patients) appears to be another important resource for MH treatment facilities, as higher rates of reported mental distress were associated with higher odds of having a MH treatment facility that offers several types of BHCC services. This suggests that MH treatment facilities may be more likely to adopt services in communities with unmet behavioral health needs. However, that does not mean there is a sufficient amount of services to cover demand. In fact, this finding brings up an important question regarding other community level factors that may be influencing MH and contributing to the need for BHCC services. For example, limited access to outpatient behavioral health services may contribute to unmet behavioral health needs in the community. 43 Previous literature has found that office-based practices of MH professionals are more likely to be located in higher-income communities, limiting access to office-based MH services in lower-income communities. 15 While increasing access to BHCC best practices is important to ensure that individuals who are in crisis can receive the most appropriate care, 3 decision makers should also consider ways that may increase access to resources for earlier intervention to promote MH in the community. 43 Addressing upstream factors may reduce the number of individuals who require BHCC services by preventing a crisis from occurring in the first place, improving quality of life for individuals with MH and substance use disorders while reducing the burden on a system that frequently cannot keep up with demand. Overall, from a RDT perspective, our findings related to munificence are aligned with the theory as organizations need to be in an environment with sufficient resources to ensure sustainability of services.14,15
We did not find statistically significant relationships between dynamism variables and availability of a comprehensive BHCC facility, although we did find that counties with the highest rates of change in population size were less likely to have a MH treatment facility offering several individual types of BHCC services. There may be a number of factors that influenced this finding. We operationalized dynamism using variables that are commonly used by studies that employ RDT 15 ; however, it is possible that these variables are not sufficient to fully capture environmental dynamism. 42 Furthermore, the timeframe of this study overlaps with the COVID-19 pandemic, a time during which all communities experienced instability and unexpected changes. In particular, dramatic changes in unemployment have occurred since the onset of the COVID-19 pandemic, which may have influenced our findings related to dynamism and is a noted limitation of our study.
Similarly to dynamism, we did not find statistically significant relationships between complexity variables and availability of a comprehensive BHCC facility. In operationalizing complexity, our findings related to racial diversity were in opposition of our hypothesis, suggesting that counties with the highest levels of diversity actually had higher odds of having a MH treatment facility that offers 3 different types of BHCC services. Given documented disparities in access to behavioral health services among racial minorities, 10 this was an unexpected finding. However, just because services are available in racially diverse counties does not mean that these services are accessible to all populations. 10 Further research is needed to examine realized access to and utilization of BHCC services among racially diverse populations.
More in line with our hypothesis on complexity, we also found that counties with a higher percentage of individuals voting Republican had lower odds of having a MH treatment facility that offers several BHCC services. Moving forward, additional variables for complexity such as state policies and regulations may be needed, as these factors may also influence service provision. 13 More complex regulatory environments may impose barriers to implementing new services, particularly if regulations are inconsistent with BHCC best practice guidelines. However, comprehensive data on all policies specifically regulating BHCC services were not available at the time of this study. Future research should examine state policies regulating BHCC services and assess alignment with BHCC best practice guidelines.
This study has strengths and limitations. We use a nationally representative data set that allows us to examine BHCC services across the US. However, a small percentage of mental health treatment facilities opt out of inclusion in SAMHSA’s Locator, and therefore are not represented in our study. We operationalized the “market” in this study as the county, providing more granular insight into the geographic distribution of services than previous, state-level studies. We also recognize this as a limitation of our study, as it is difficult to cleanly control for possible confounding of variables. Mental health treatment facilities may also serve surrounding counties in addition to the county they are located in; given that we do not have detailed information on the specific service areas of mental health treatment facilities, we were unable to account for this. Future studies should collect more detailed information on service areas and control for this information. Additionally, while there may be other measures that capture the constructs of RDT, we were limited by the types and quality of publicly available data sources. For example, there are additional variables that could be used to operationalize unmet behavioral health needs, such as overdose rates and suicide rates. 10 However, due to large amounts of missing data in publicly available data sources, we did not include these variables in our study. Furthermore, while we used independent variables that predated our dependent variables, this study is still cross-sectional and does not allow us to infer causality. Given that SAMHSA did not make facility- or county-level data on mental health treatment facilities publicly available in a usable format prior to 2022, we were unable to examine BHCC services in previous years. Future research should follow changes in BHCC availability over time to generate stronger evidence regarding the relationship between market factors and service availability.
Conclusion
In examining market factors associated with comprehensive BHCC availability, our study found that communities with fewer MHPs and rural communities were far less likely to have a comprehensive BHCC facility. These findings suggest that workforce shortages may limit the ability of mental health treatment facilities to adopt BHCC services, and highlight disparities in rural communities. As efforts to transform the nation’s crisis care system are underway, policies and practices that enhance the capacity of the mental health workforce are needed to ensure availability of someone to respond to individuals in crisis in every community.
Footnotes
Acknowledgements
Funding for this study was obtained through an R36 Dissertation Grant awarded by the Agency for Healthcare Research and Quality.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Agency for Healthcare Research and Quality R36 Health Services Research Dissertation Program (1R36HS029654-01).