
Abstract
In the context of an aging population, the concept of peaceful end-of-life care has gained increasing significance as an essential component of individuals’ fundamental well-being. This underscores the importance of researching and developing hospice care facilities and service systems dedicated to providing a tranquil resting environment. This study focuses on selected hospice care buildings, examining their service model evolution and architectural design. Through case analyses, it explores contemporary hospice care architecture, identifying various types and spatial design features that cater to the end-of-life needs of individuals. The findings guide the design of hospice care buildings in China, emphasizing patient-living areas, medical care zones, and auxiliary functional spaces. This comprehensive approach aims to enhance terminally ill patients’ comfort, serenity, and dignity. Moreover, it aims to provide emotional and post-funeral support to terminally ill patients’ families.
The theories and practices of hospice care buildings had developed rapidly in other countries. However, studies on hospice architecture and spatial design were scarce in China, and there was no systematic or standardized theoretical guidance for hospice building design in practice.
This article systematically summarized the development characteristics of hospice architecture and service models from the aspects of developing origin, prototype of the hospice care buildings, the transition from “home care” to “hospital services,” the first modern hospice care institution, hybrid services for hospice inpatient and home care, and the philosophical concept of “spatial practice.” Second, we summarized 4 types of architectural and spatial design features of contemporary hospice care buildings by analyzing architectural cases. Based on the above research, the design strategies for Chinese hospice care buildings were summarized in 3 aspects—patient living spaces, medical, and nursing spaces, and auxiliary functional spaces–aimed at meeting the needs of Chinese patients for pain control, emotional care, and spiritual comfort.
This article supplemented the existing research on well-being architecture and highlighted the need for more research on hospice buildings in China. It improved its theoretical system by advocating for the gradual inclusion of institutional and home hospice care service fees within the scope of basic medical insurance, developing a hospice education and training base to elevate the professional standards of medical staff, and building an integrated round-trip composite model of “home care - day care -inpatient care” for comprehensive hospice care building design. It proposed the principles and essentials of hospice building design and provided useful references for the construction of hospice buildings in China.
Introduction
Increasing Tendency of Population Aging and Isolated Death
Alongside the increasing elderly population, the prevalence of empty nesters and widows living alone leads to the phenomenon of “isolated death,” a growing concern in our society. This prominent manifestation of population aging underscores the need for end-of-life hospice care for elderly individuals. These evolving social challenges highlight the essential role of hospice care services in an aging society. 1
Increasing Needs for Hospice Care
Currently, healthcare resources predominantly focus on curative treatments, neglecting the needs of terminally ill patients and their families. Projections indicate that by 2050, China’s elderly dependency ratio will reach 27.9%, according to National Development Bulletin on Aging in 2022 by the Ministry of Civil Affairs of the People’s Republic of China, emphasizing the imminent demand for hospice care owing to a population aging and the rise in non-communicable diseases. However, there exists a noticeable imbalance between the supply and demand for hospice care in China, hindering access to high-quality end-of-life care. 2 Figure 1 illustrates relevant service policies and basic construction standards released in 2014.

Development history of China’s hospice care service policy.
Significance of Research
Hospice care addresses the emotional and spiritual needs of terminally ill patients, providing comprehensive care and attention to patients through medical, nursing, psychological, ethical, and social means. This approach aims to alleviate pain and symptoms, improve patients’ quality of life, and maintain their dignity. Additionally, hospice care extends support to the families of patients, offering mental comfort and bereavement care.3 -5 Although hospice care may not fundamentally alter the trajectory of terminally ill patients, its humanistic and humanitarian principles align with the evolving norms of modern civilized society. This study explores the significance of hospice care in the context of China’s increasing trend of population aging.
Scientific Definition and Architecture Development History of Hospice Care
Scientific Definition of Hospice Care
Hospice or Palliative care, distinct from curative therapies, aims to facilitate a dignified end-of-life experience by alleviating suffering, managing symptoms and providing psychological and spiritual support.6,7 This extends to supporting the families of terminally ill individuals, addressing their emotional needs even after the patient’s passing. In 2017, China’s National Health and Family Planning Commission proposed the collective term “hospice care” for both hospice and palliative care services.
Development of Hospice Care Buildings and Service Patterns
Developing origin
Throughout its historical development, hospice care architecture finds linguistic roots in “hospes,” linking it with hospitality, hospital, hostel, and hotel. They all derive from the Latin word “hospes.” This connection underscores similarities between early and modern hospice care institutions. Originating in the UK after the Second Industrial Revolution, hospice care shifted from a medical-centric approach to prioritizing the wishes of the terminally ill. 8 Figure 2 illustrates the 2 phases of foreign hospice care development, anchored by the establishment of St. Christopher’s Hospice in 1967.

The development history of hospice care service pattern.
Prototype of hospice care buildings
In the Middle Ages, hospice buildings served as refuges for travelers. Similar facilities emerged in 17th-century France, 18th-century Germany, 18th-century Ireland, and early 20th-century St. Joseph’s Hospice in Ireland. 9 These historical places for the terminally ill serve as prototypes for modern hospice care institutions.
The transition from “home care” to “hospital services” and “hospice.”
In the late 19th century, deaths primarily occurred at home, shifting to hospitals in the early 20th century. By the 1950s, societal changes led to a more common transition from home to hospital. 10 Dissatisfaction with hospital systems prompted the hospice care movement in the late 1960s, redirecting care for the terminally ill from hospitals to dedicated hospice facilities.
Birth of the first modern hospice care institution, St
Christopher’s Hospice (Dr. Dame Cicely Saunders).
The modern hospice movement emerged in the late 1960s as a realistic response to dissatisfaction with hospital treatment of death. 10 Dr. Dame Saunders, considered the founder, established St. Christopher’s Hospice in 1967, symbolizing the beginning of the global hospice care movement. When it was established in England it was recognized as “the beacon that lit the world hospice care movement,” 11 as shown in Figure 4. Subsequently, hospice care services emerged in more than 60 countries, including the United States, Canada, Germany, Sweden, and Australia, and countries began to study hospice care institutions at the architectural.
One-way and hybrid services for hospice inpatient and home care services
In the mid-1970s, the philosophy of hospice care gained prominence, fostering the development of home care service patterns. This era saw the rise of one-way or hybrid services, incorporating hospice inpatients and home care services, contributing to diverse programs in the 1990s. 10
Development of the philosophical concept of “spatial practice.”
In the early 21st century, hospice care transcended specific buildings, evolving into a philosophy based on space and spatial practice. This innovative concept broadened hospice care beyond architectural boundaries, emphasizing space as a crucial element in hospice care practice.
Types and Design Features of Contemporary Hospice Care Buildings
Hospice care service institutions are recognized as emerging building types globally. For example, Sarah McGann asserts that “hospice and hospice architecture is an emerging and continuously evolving building type,” and Verderber and Refuerzo describe hospice buildings as “innovative.” Countries like the United States, the United Kingdom, The Netherlands, Japan, and others, evolving into aging societies, have conducted in-depth theoretical research and extensive practical work in the architectural design of elderly service facilities. Their research on hospice care architecture precedes that of many other countries, with their related support facilities and design experiences are becoming more mature and complete. According to their different patterns, hospice care services can be categorized into home hospice care services and institutional services. 9 Figure 3 and Table 1 outline the 4 basic international classifications of hospice care facilities:
(1) Independent hospice care institutions.
(2) Hospice care centers attached to hospitals.
(3) Day care/home care hospice buildings.
(4) Nursing facilities with hospice-specific beds.
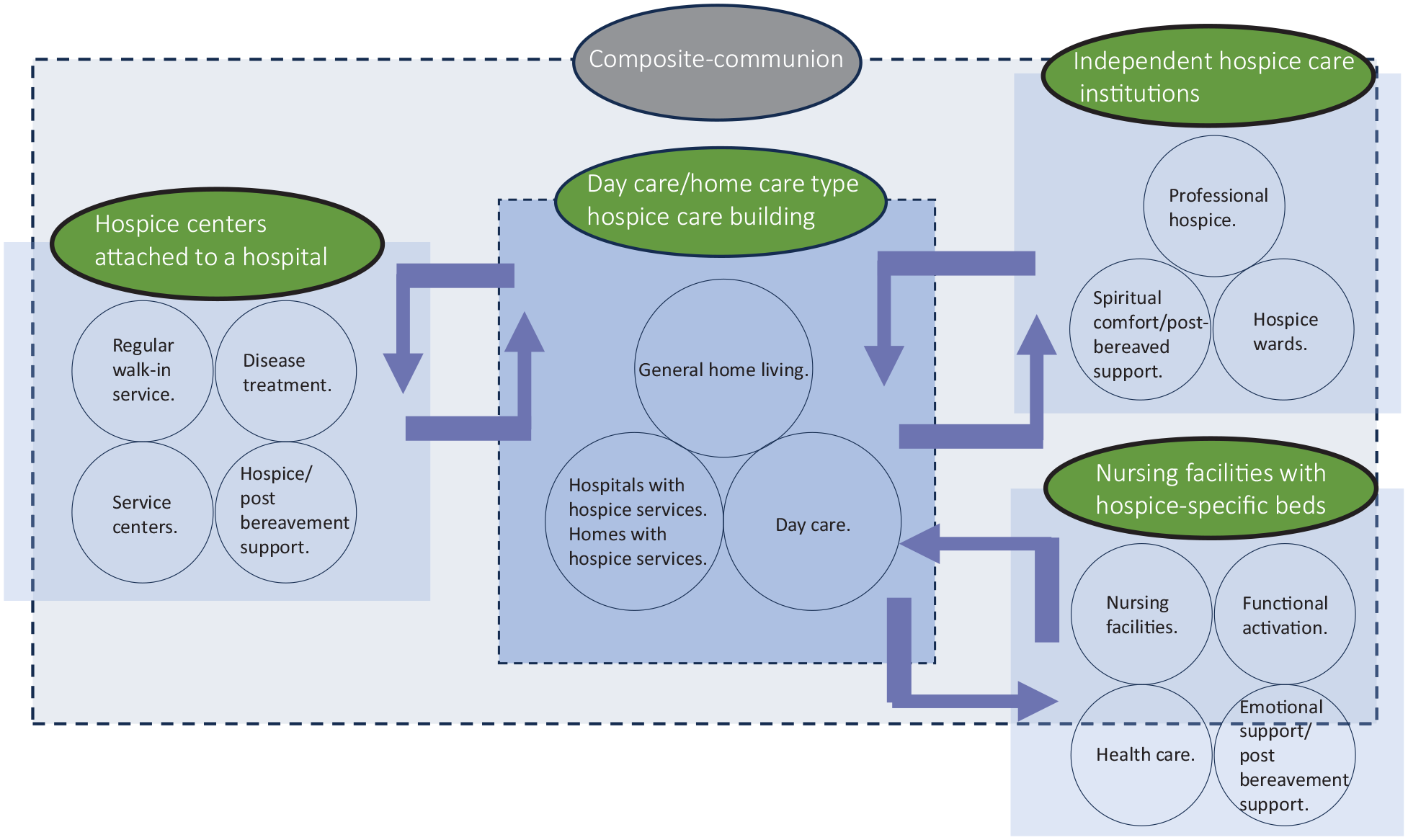
Hospice care building types and service patterns.
Plan Layout and Perspective View of Building Space for 4 Types of Hospice Care Building Design Cases.

The functional configuration and spatial design characteristics of these 4 types of hospice buildings are analyzed through case studies.
Type 1—Independent Hospice Care Institutions
Sharon S. Richardson Hospice, a community-based freestanding hospice care building in Wisconsin, focuses on a north-facing main elevation, providing scenic views of the river, pond, and healing gardens. The layout includes 3 inpatient units, each with additional activity and service spaces such as lounges, chapels, libraries, playrooms, spas, dining rooms, and kitchens. Wards are arranged at a 60° angle to the corridor, extending outdoor views while maintaining patient privacy and dignity. Each ward has a private terrace with direct access to the outdoor garden, ensuring maximum use of the tranquil surrounding views and rolling hills to provide a rustic retreat atmosphere for patients and family members. Each ward has a private and sheltered terrace with direct access to the outdoor garden, 9 as shown in Table 1a.
Type 2—Hospice Centers Attached to a Hospital
LaGrange Hospice, located on the campus of the West Georgia Medical Center in Georgia, USA, features an administration building and 3 inpatient units around a central courtyard. The design avoids long, institutionalized, double-loaded corridors of traditional hospital and nursing home styles, providing semi-private patios between inpatient units for temporary breaks and occasional conversations. Each inpatient unit consists of 4 wards, a living room, and related living support facilities, including kitchens, dining rooms, spa rooms, lounges, and laundry rooms. Double doors in each ward provide outdoor access for nursing beds and wheelchairs, 12 as shown in Table 1b.
Type 3—Day Care/Home Care Hospice Buildings
Dundee Maggie’s Center, a notable cancer-related architectural project in the UK designed by Frank Gehry, rejects large-scale institutional systems. As shown in Table 1c, the building rejects the frustrating large-scale and monolithic institutional system of the medical care institution center as well as the rational, complete presentation of the medical care institution, presenting a fun and human-scale composition. The building, resembling a family home, prioritizes the human scale, incorporating dining kitchens, libraries, and lounges to create a family-life atmosphere. Gehry’s design emphasizes the human scale, promoting acceptance rather than rejection, fostering a sense of security for visitors. There are no cold, gray, or seemingly endless corridors that are often set in medical care institutions. 12
The roof is the focal point of Gehry’s expression, with a creative, quirky, dynamic, and complex form mirroring the continuous landscape around it. Through scales and materials, the dining kitchen, library, and lounge portray the atmosphere of family life rather than the feelings of a medical institution. The office area, which is open and resembles a family living room, makes the elderly feel accepted instead of rejected, and dissolves the boundaries between the elderly and the staff. This also increases the visitors’ sense of security. 12
Type 4—Nursing Facilities With Hospice-Specific Beds
The Ark Center for Palliative Care, located in the Netherlands, is located in a forested area independent of the hospice care center. It employs a small architectural vocabulary with a curved planar geometry and a cylindrical spiritual space at its center. Public spaces are housed within 2 curved elliptical walls, enhancing the vertical dimension with an angular skylight. The triangular skylight, passing through the roof of the chapel, provides a visual impact. The use of natural light creates a calm, contemplative atmosphere, allowing emotional interactions and social activities. Curved sliding doors can be opened within a cylindrical spiritual space to form an open area for activity with the neighboring public space. 12 This provided a place for emotional interactions with other general social activities in the institution, as shown in Table 1d.
Hospice Building Space Design Measures
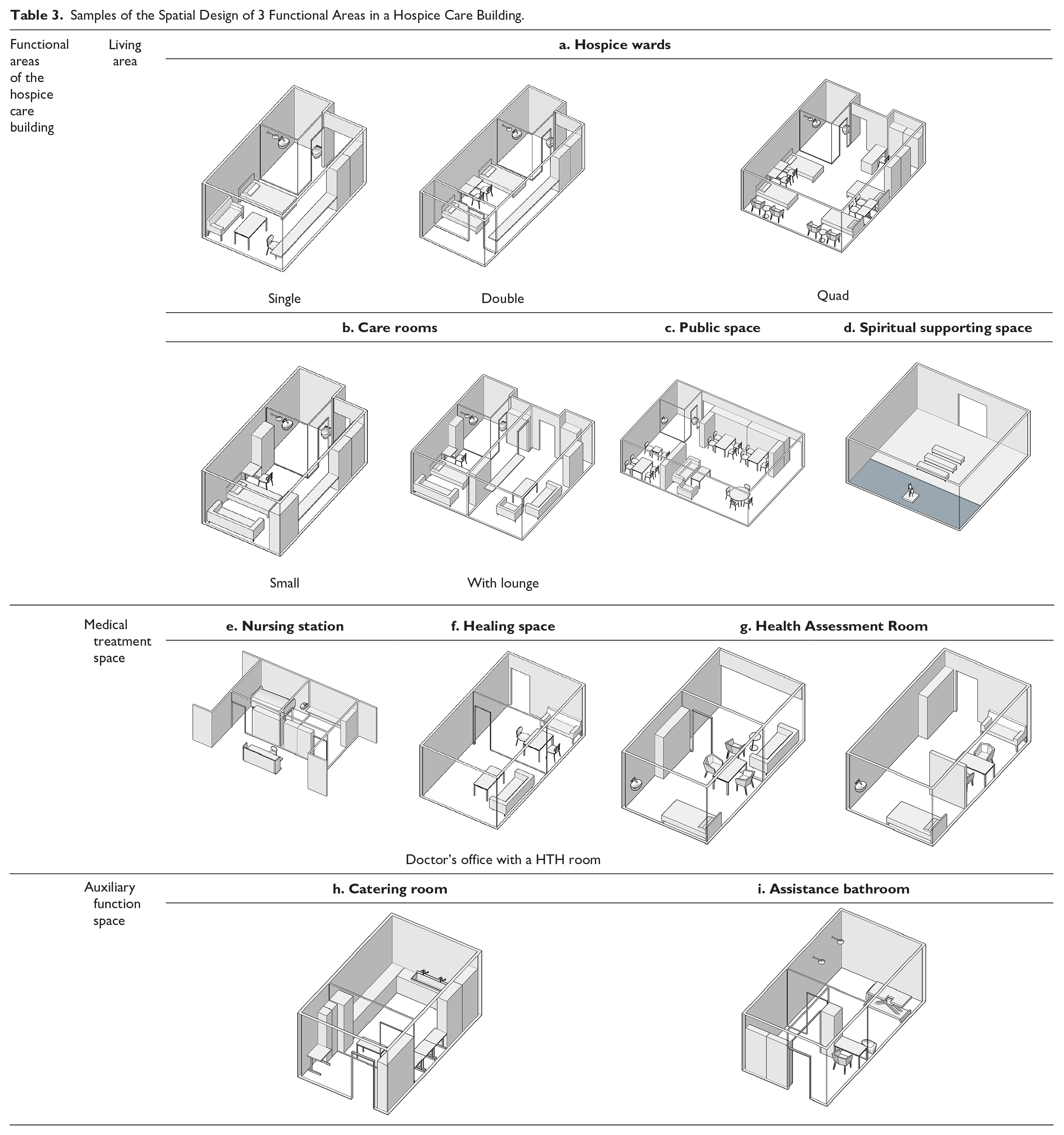
The functional configuration, space design, space use, and operational services of hospice care buildings are significantly different from those of common hospitals and elderly service facilities. However, their design principles have certain commonalities with those of hospitals and elderly institutions, and there are certain special features. As shown in Table 2, the hospice care building design included 3 major functional areas: living areas, medical care areas, and auxiliary function area.13 -15
Functional Space Layout of Hospice Care Buildings.

Living Area
Hospice ward design
The hospice ward is the smallest living unit in a hospice care building. It is the primary place for patients to conduct their daily lives and receive routine checkups, nursing care by medical staff, and cleaning care. Moreover, it is a social space for terminally ill patients, friends, and relatives. The impact of space design on patients’ lives and quality of life is especially significant. Simultaneously, the “adaptability” of the building spaces should be enhanced. At the beginning of the architectural design, it is necessary to consider possible changes in space. When designing the space, we should try to increase the adaptability of the space, so as to provide the possibility of transforming the hospice care ward in the future and meet the changes in patients’ needs. For example, a 4-room hospice ward can be converted into 2 single rooms, 2 double rooms, or a couple suite, as shown in Table 3a. 14
Samples of the Spatial Design of 3 Functional Areas in a Hospice Care Building.

Care room design
The care room is a place for family members and friends to remember terminally ill patients, send their condolences, and bid farewells to the deceased when they die. It has commonalities and differences with the designs of general hospice care wards. In addition to meeting the aforementioned design points of the hospice care ward, corresponding spiritual care spaces should be set up according to the service characteristics. 15
As patients in the care room usually have less than 48 h to live, there are more friends and relatives visiting the room. Consequently, care rooms should be designed with sufficient “family support space” to meet the needs of family members for overnight companionship, and the needs of family and friends for rest and conversation. The design should try to create a “home scenario” atmosphere. 16 Table 3b demonstrates equipment that supports patients’ religious beliefs, as installed in the care room to offer spiritual comfort to the terminally ill.
Public space design
Public spaces are places of continuous connection and positive interaction among patients and their families, friends, healthcare workers, and volunteers. Through interpersonal interactions, terminally ill patients gain a greater sense of control in their lives and a better connection with society. Creating a relatively homely environment is conducive to patients communicating more easily with others, relieving mental tension in the elderly, and establishing more intimate interpersonal relationships. 17 To increase the comfort of the spatial environment, a home-like interior design should be adopted, as illustrated in Table 3c.
Spiritual supporting space
Quiet environment
A quiet atmosphere should be created in the design of the space, and sound, light, and ventilation should be reasonably controlled. As shown in Table 3d, the location of the space should be as far away as possible from noisy rooms, such as public activity rooms and dining rooms, to create a quiet environment for patients to meditate. 18
Minimalist furnishings
When patients are in meditation or prayer, they require a less distracted spatial environment. Therefore, minimalist furnishings were used in the spatial design of buildings, as shown in Table 3d.
Installation of music playing equipment
As demonstrated in Table 3d, music-playing equipment can be installed in the spiritual support space. Music can be played quietly and softly in space to assist users to remove distractions quickly and concentrate easily. 18
Introduction of water
Water can soothe and alter an individual’s mood positively. Calm water can create an atmosphere conducive to prayer and meditation activities, calming the patient’s mind, whereas dynamic water, with sound acting as a lively element, can trigger positive emotions in patients. Additionally, artworks such as sculptures, have a strong expressive power and may serve as inspiration. It is most likely to touch the souls of the people. 10 The layout is shown in Table 3d.
Medical Treatment Space
Nursing station
A nursing station is a space in which medical staff provide services to other people, for instance patients, family members, and consultants. Terminally ill patients may interact with medical staff in brief sessions during their daily lives. The nursing station and ancillary spaces, such as disposition rooms, medication change rooms, and medication supply rooms, are backup spaces to meet the daily medical care needs of the patients. 19
Patients in the terminal state usually require certain medical care treatment to alleviate their physical pain, therefore the interaction between medical staff and patients in the ward is very frequent. To improve work efficiency, the distance of the movement line must be shortened, as shown in Table 3e.
Healing space
As shown in Table 3f, the healing spaces mainly consist of functional rooms such as art therapy rooms, psychological counseling rooms, and heart-to-heart rooms. They provide spiritual comfort and relief from psychological distress for terminally ill patients. Furthermore, they provide psychological and spiritual counseling for patients’ family members, as well as bereavement counseling for family members after the death of a patient. To avoid wasting space, they can be combined when the area is limited or merged with other functional spaces (such as offices and assessment rooms). 20
Health Assessment Room
Health assessment rooms are spaces where patients’ vital signs are assessed prior to being admitted to a hospice care facility, or where patients or family members go to receive related consultations regarding palliative care. To avoid space wastage, it can be combined with an office when the space is limited. A waiting area, with reserved observation beds, is also required. Furthermore, a curtain should be installed to protect the privacy of patients, as shown in Table 3g.
Auxiliary Function Space
Catering room
The catering room is appropriate for providing patients, family members, and medical staff with a spacious and fully functional dining space with cupboards, stoves, microwaves, and sinks. Some catering rooms can also include boiling water stations in rooms, which are convenient for patients, family members, and medical staff to consume hot water at any time, as shown in Table 3h. 21
Assistance bathrooms should contain basic functions, such as dressing, showers, and commodes. When conditions permit, hairdressing, laundry, and other functions can be combined in a bathroom. The floor was made of non-slip, easy-to-clean materials, and the walls were made of moisture-proof, mold-resistant materials. The height of the shower can be adjusted to a suitable position, and heating equipment can be provided. Moreover, toilet seats were available as shown in Table 3i.
Conclusion
Recommendations for Policymakers
In response to the challenges posed by an aging population, policymakers should consider the following recommendations to enhance hospice care:
Build a comprehensive service system
Establish hospice care departments or beds within medical institutions, and if possible, create independent hospice care centers. Extend hospice beds to community health service centers and township health centers, ensuring a balanced service system covering both urban and rural areas. Integrate hospice care services into various medical departments such as geriatric medicine, oncology, and pain management. Encourage the establishment of hospice care wards in suitable conditions, while also promoting hospice care services in medical and elderly care institutions and community health service centers. 22
Enhance Support Policies
Advocate for the gradual inclusion of institutional and home hospice care service fees within the scope of basic medical insurance, long-term care insurance, and other supplementary medical insurance.
Establish Education and Training Bases
Develop a hospice education and training base to elevate the professional standards of medical staff. Foster a multidisciplinary professional talent team encompassing medicine, nursing, psychology, nutrition, and social work. Encourage the active participation of social organizations and volunteers in hospice care services.
Integration of Round-Trip Composite Model for Comprehensive Hospice Care Building Design
To realize diverse hospice care services, the design of hospice care buildings should align with the round-trip composite model of “home care - day care - inpatient care.” Currently, hospice care service phases are unidirectional, but the future ideal involves a composite model integrating home, day, and inpatient care (see Figure 4). 22

Future hospice care building design and service development model.
Creating a Family-Centric Atmosphere in Hospice Care Building Design
Designing hospice care spaces to emulate family life promotes a positive response to the spiritual needs of terminally ill patients. Transforming the institutionalized atmosphere to a family-orientated one helps maintain continuity in patients’ activities, preferences, and consciousness, easing the transition from home to institution. 23
Balancing Spiritual Comfort and Healing Medical Spaces in Hospice Care Facilities
Hospice care facilities prioritize spiritual comfort and quality of life assessment, necessitating the coexistence of spiritual support spaces and healing medical spaces. The design should consider effective communication and interaction between patients and their families, addressing physical, psychological, social, and spiritual aspects of end-of-life care.
Enhancing Patient Well-Being Through Nature-Inspired Hospice Care Wards
Spatial design of hospice care wards should maximize enhance patients’ visual and physical contact with nature, incorporating services for pain control, emotional care, and spiritual comfort. Studies indicate that exposure to natural landscapes positively impacts patients’ psychological and spiritual well-being, potentially reducing pain medication dependency and complications. Visual and physical contact with nature is an important standard for evaluating the quality of life of patients in hospice care. It can increase patients’ psychological and spiritual comfort and satisfaction, thus enhancing their positive emotions, reducing fear and anxiety, soothing pain, and keeping them calm. 12 Several studies have shown that patients who experience natural landscapes for longer periods tend to be more relaxed and take less pain medications, with fewer complications. 24
Footnotes
Acknowledgements
All tables and figures presented in the manuscript are original and have been obtained from the respective copyright holder(s) with the necessary permission to reproduce and adapt the images in this manuscript. The authors would like to thank Donghui Li and Ling Zhang for the data collection assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Humanities and Social Science Youth Fund of Ministry of Education of China: A study on the end-of-life care model and response strategies for the design of hospice care spaces for elderly people who have lost their only child in the context of Healthy China (No. 22YJCZH167).