
Abstract
The coronavirus disease 2019 (COVID-19) pandemic has presented a globally challenging situation for human physical and mental health. Healthcare workers (HCWs) are affected by increased levels of anxiety, stress, and insomnia. This study aimed to evaluate the effect of COVID-19 on HCWs anxiety, stress, and insomnia levels. This cross-sectional study employed the Hospital Anxiety and Depression Scale, Perceived Stress Scale 10, and Insomnia Severity Index to assess anxiety, stress, and insomnia among HCWs at 10 COVID-19 isolation and treatment hospitals/centers after the first COVID-19 wave in Jordan. A web-based survey was used to collect data from 183 participants. Statistical analysis of factors affecting the mean scores of anxiety, stress, and insomnia was carried using student t-test or ANOVA while factors associated with differences in anxiety, stress, and insomnia frequencies were tested using Chi-square/Fisher exact test. Multivariate analysis was performed to determine the independent risk factors. Among participants, 97.3% reported moderate to severe levels of stress, 68% reported borderline to high abnormal levels of anxiety, and 32% had moderate to severe insomnia. The mean of anxiety total score was 9.8 ± 4.8, stress total score was 22.7 ± 4.5, and insomnia total score was 11.0 ± 7.1. Significant positive correlations were noted between anxiety, stress, and insomnia (P < .005). Female gender, migraine, less working years, increased time spent with patients, lower workforce, clinical insomnia and high stress were significant independent factors associated with anxiety (P < .05). Younger age, being single or divorced, heart disease, smoking, occupation (nurses), lower workforce, vaccination dose, and anxiety were significant independent factors associated with insomnia (P < .05). Increased time spent with patients, lower workforce, lower spouse and colleagues support, sadness due to isolation and anxiety were significant independent factors associated with stress. HCWs at COVID-19 centers had high levels of stress, anxiety, and insomnia. Appropriate interventions to maintain HCWs mental health are recommended.
Keywords
COVID-19 had a significant impact on the mental health of hospital staff.
This study indicated that hospital staff working at COVID-19 isolation and management centers reported moderate to severe levels of stress (97.3%), borderline to highly abnormal levels of anxiety (68%), and insomnia of moderate to severe levels (32%).
Mental health problems were prevalent among hospital staff working at COVID-19 isolation and management centers. Enhancing practices and policies of mental health support for hospital staff during crisis management including e-mental health interventions, conducting regular interviews and screening tools, support networks, offering psychological assistance especially to high-risk employees, and designing tailored prevention and supporting strategies are recommended.
Introduction
Coronavirus disease 2019 (COVID-19) was declared an outbreak by the World Health Organization (WHO) on December 31st, 2019, and was considered a pandemic on March 2020.1 -3 By the end of May 2023, more than 760 million confirmed cases of COVID-19 were registered. 1 The incubation period ranged from 0 to 24 days. Most patients have asymptomatic disease or mild to moderate illness, while approximately 20% of COVID-19 patients experience serious respiratory disease with a cumulative case fatality rate of about 2.3%.1,4 Multiple vaccines have been approved for COVID-19 and vaccination campaigns delivered more than 13 billion doses. 1
The first case of COVID-19 in Jordan was reported on March 2nd, 2020.2,4 After that, on March 17th, 2020, the government called for social distancing, and all airports were shut down with the activation of the Defence Law. 5 Jordan was classified as having a virus transmission “cluster of cases” by mid-April 2020.1,5 A complete curfew was activated by 21 March 2020 and continued for 6 weeks.2,4 During the period from March to the end of August 2020, Jordan registered a low number of COVID-19 cases due to preventive measures applied by the government including reduced working hours and working from home, distant learning, prohibition of gatherings, and cessation of international flights. 5 However, despite all preventive measures, the first wave of viral spread was recorded between September 2020 and January 2021 with 170 000 cumulative cases and 2000 deaths. This was mostly due to the opening of land boundaries, schools and universities resuming regular class teaching, and poor application of social distancing and face masks. 5 COVID-19 vaccination started in late 2020 in Jordan and priority was given to hospital staff. The vaccination program for the general population was launched in January 2021, with about 50 000 fully vaccinated by mid-March 2021. 5
Stress is a physiological human response that occurs when the body is exposed to harmful stimuli. The body responds to stressful events via interactions between several pathways, including the nervous system and the hypothalamic-pituitary-adrenal (HPA) axis.6,7 Anxiety is a psychological condition marked by discomfort or worry and is one of the most common health problems. Insomnia is a complaint about sleeping problems or difficulties in maintaining sleep. Work-related stress is the reaction that people may have when faced with job demands and conditions incompatible with their skills and abilities resulting in challenging their ability to cope. Hospital staff are known to be at higher risk.8,9
A link between mental illnesses and outbreaks of acute respiratory infections was previously documented for HIN1 influenza, and Severe acute respiratory syndrome (SARS). 10 The outbreak of COVID-19 triggered public fear, mental health stress, and public concern at unexpected levels. COVID-19 has resulted in a spike in the risk factors for mental health issues in the general population, infected individuals, and hospital staff.11 -15 Healthcare workers (HCWs) are generally exposed to many challenges that may impact their mental health well-being, especially during the COVID-19 era. They are exposed to extraordinary difficulties, such as extended workdays, heavy workloads, poor sleep and exhaustion, limited resources, trauma exposure, moral challenges, increased demands to make critical decisions, and infection risk. It is highly important to promote the mental health of HCWs via several proactive steps to mitigate the negative psychological consequences of the COVID-19 pandemic.8,12,16,17 Poor mental and psychological support leads to the progression of their mental state. 13
Studies have shown that hospital staff dealing with COVID-19 are exposed to a greater risk of mental health problems, such as anxiety, depression, insomnia, and stress.11,12 A review of 44 meta-analysis studies concluded the increased overall prevalence of stress (44.3%) and psychological distress (34.59%), insomnia or sleep problems (39.45%), anxiety symptoms (29.9%), and depressive symptoms (28.44%), of hospital staff due to the COVID-19 pandemic. 11 The lowest prevalence of other psychological symptoms was found for suicidal thoughts (6.17%) while the highest prevalence was for fear-related symptoms (67.0%) among hospital staff during the COVID-19 pandemic, however, the quality of evidence for these symptoms was low to very low. 11
The impact of COVID-19 on the mental health of hospital staff differs according to the time during the pandemic, geographic location, health system capacity, epidemiology of COVID-19, preventive measures applied, occupation of hospital staff, and other factors.9 -17 Limited data on the same topic are available from the Middle East area and none are available from Jordan. Understanding the impact of the COVID-19 pandemic on hospital staff mental health and its associated factors is critical for designing preventive and supportive strategies.11,13,16 The inclusion of all hospital staff and multiple COVID-19 centers after the first wave of the COVID-19 pandemic would enhance the significance of the study. This study aimed to investigate the effects of COVID-19 on mental health including anxiety, stress, and insomnia (the 3 most common and/or most evidence-supported mental health issues) 11 among hospital staff working at 10 COVID-19 isolation and management hospitals/centers after the first COVID-19 wave across Jordan.
Methods and Materials
Study Population
This was a cross-sectional study assessing the mental health effects of COVID-19 on hospital staff in Jordan, particularly the prevalence of anxiety, stress, and insomnia. A self-administered questionnaire was delivered to staff working at different COVID-19 isolation and treatment centers between March 31, 2021 and June 8, 2021. The inclusion criteria included any hospital staff working in governmental, military, or private hospitals or centers across Jordan assigned for isolation and treatment of COVID-19 patients, age older than 18 years, who could read the questionnaire, and who agreed to participate in the survey. The Raosoft online sample size calculator was used to calculate the sample size for the present study. A 50% response distribution, a 5% margin of error, and a 95% confidence interval served as the foundation for the computation. The computed sample size was 278 participants, out of an anticipated total of about 1000 hospital staff working at different COVID-19 isolation and treatment centers. However, the current study included 183 participants due to the specific and challenging nature of the research context. In studying health staff at COVID-19 isolation and treatment centers, it is expected to have a small group of participants. This is because few health workers exclusively handle COVID-19 patients in these special centers, and the job’s demands make it difficult to find many participants. Additionally, some health workers may have been infected themselves and are in isolation, making it difficult for us to access them for the study.
The study was approved by the institutional review board (IRB) of the Hashemite University and the targeted hospitals.
Instruments
A self-administered questionnaire in English and Arabic (native) languages was administered using Google forms to the targeted hospital staff using social media, friends, and other media. The current study employed validation questionnaires, including the Hospital Anxiety and Depression Scale (HAD), the Perceived Stress Scale 10 (PSS-10), and the Insomnia Severity Index (ISI). The questionnaire’s validity and reliability have been tested previously.14,15 Cronbach’s alpha was used for testing reliability with good results corresponding to a value of 0.86. The questionnaire was divided into 4 sections after providing informed consent. The first section included 26 self-designed questions covering demographic and exposure factors including age, gender, marital and fertility status, health conditions, occupation (physician, nurse, pharmacist, administrative staff, others), working years, total monthly income, deduction from salary during lockdown, residency location and status, transport type, emotional support, and direct contact with COVID-19 patients.
The second section was designed to assess anxiety using the HAD. 15 This scale includes 14 questions assessing anxiety and depression. Only questions covering anxiety were used (7 questions). Each question included 4 items and responses were scored on a numeric scale (range 0-3) for each item. The total score (range 0-21) was categorized as follows: (0-7) normal (no anxiety), (8-10) borderline abnormal (borderline case), and (11-21) abnormal (anxiety case). The third section is designed to evaluate stress using PSS-10. 15 The PSS-10 includes 10 questions used for assessing stress, each question includes 5 items scored as 0 (never), 1 (rarely), 2 (sometimes), 3 (fairly often), and 4 (very often). PSS-10 total score can range from 0 to 40. Scores of 0-13 were considered low stress. A score between 14 and 26 was considered moderate stress, and a score between 27 and 40 was considered high perceived stress. The fourth section is designed to assess insomnia using the ISI. 14 This scale includes 7 questions, each question has 5 items scored numerically from 0 to 4, and the total score ranged from 0 to 28 was categorized as follows: (0-7) no clinically significant insomnia, (8-14) subthreshold insomnia, (15-21) clinical insomnia (moderate severity), (22-28) clinical insomnia (sever). The study survey questions are available as a supplementary file (Supplemental File 1).
Statistical Analysis
The data were exported to the Statistical Package for the Social Sciences (SPSS, version 24.0 Chicago, IL, USA). The normality of the distribution of dependent variables (anxiety, insomnia, and stress) was assessed using the Shapiro-Wilk test. The descriptive statistics are presented as the frequency and percentage or mean and standard deviation (SD). Univariate statistical analysis was performed to compare the frequencies of different levels of anxiety, insomnia, and stress using the Chi-square test or Fisher’s exact test and strength of association was tested using Cramer’s test. The mean total anxiety, insomnia, and stress scores were compared across different categories by Student’s t-test or one-way ANOVA followed by LSD post-hoc test. Correlations between continuous variables were analyzed using the Pearson bivariate correlation test with correlation coefficient values (R). Multivariate regression model was used for analysis of factors associated with abnormal anxiety, high stress, and clinical insomnia while multivariate linear model was used for analysis of significant factors that affect anxiety, insomnia, and stress scores. A P value ≤.05 was considered to indicate statistical significance.
Results
Characteristics and Work-related Details of the Study Participants
A total of 183 participants were included in this study from 10 COVID-19 treatment and isolation centers across different cities and sectors in Jordan. Among the participants, 152 (83%) were from governmental hospitals, and 31 (17%) were from private hospitals. A total of 139 (76%) of the participants worked during the complete lockdown. Most participants’ ages (78%) ranged from 20 to 39 years and were equally distributed between genders (50% males and 50% females). Among the participants, 57% were married, and 55% had 3 or less children. Regarding occupation, 48.6% of participants were physicians, 27.3% were nurses, 10.4% were pharmacists, 7.1% were administrative staff, and 5.5% were radiotherapists. The percentage of time with direct contact with COVID-19 patients ranged from 0% to 20% for 56 participants (30.6%) to 81% to 100% for 29 participants (16%). The majority of the study participants spent less than 60 working hours per week (72.1%). Thirty-six percent of the study population strongly disagreed/disagreed that they had sufficient protective equipment in the hospital. Seventy percent of participants in this study strongly disagreed/disagreed about the availability of a sufficient workforce. Seventeen percent of participants strongly agreed that people treat the staff who worked in a hospital treating COVID-19 patients differently (Table 1). Further details of the study participants’ characteristics are described in Table 1.
Demographic and Work-Related Details of the Study Participants (n = 183).

Clinical, Social, and Financial Characteristics of the Study Participants
Approximately half of the participants (47.5%) were diagnosed with COVID-19, 51% received the COVID-19 vaccine, of them 72.3% received 2 doses. Among the participants, 37.5% reported that the vaccine did not affect their stress level, while 32.5% reported a decreased stress level. The most common chronic diseases reported by participants were migraine (10.4%) and asthma (10%), and approximately 30% of participants were smokers. The majority of the working force had more than 500 JD (equivalent to approximately 700 USD) of monthly income (n = 108, 59%), and most of participants (80%) had cut off from their salaries during the lockdown in the range from 0 to 100 JD. Most participants found difficulty in getting to work during the lockdown using public transport; of these, 56% found it very hard. The experience of sufficient food at the hospital during lockdown varied, with 24% of the study population strongly disagreeing that the food was sufficient. Participants reported that physical isolation from family and people made them feel lonely and sad (33% of participants strongly agreed and 39% agreed; Table 2).
Clinical, Social, and Financial History of the Study Participants.

The presented data are from multiple-choice rather than single-choice questions.
Emotional Support for Study Participants
Emotional support from family members was provided to most participants. Hence, 25.1% and 49.7% of the participants strongly agreed and agreed that they received emotional support from their families, respectively. A total of 27.3% and 23.5% of the participants agreed and strongly agreed, respectively, that they received emotional support from their spouses. A total of 39.3% of the participants agreed that they received support from colleagues, 4.9% strongly agreed, 29% were neutral, 21.3% disagreed, and 5.5% strongly disagreed about having any colleagues support (Table 3).
Emotional Support for the Study Participants.

Anxiety, Stress, and Insomnia of the Study Participants
Forty-five percent of the participants reported high levels of abnormal anxiety, 23% reported borderline high anxiety, and 32% reported normal levels. Approximately 81% of participants had moderate stress during the pandemic, 16.3% had high perceived stress, and 2.7% had low stress levels. Regarding insomnia levels, 31% of the study population had subthreshold insomnia, 27% had moderate severity clinical insomnia, and 5% had severe clinical insomnia (Table 4). The mean anxiety total score was 9.8 ± 4.8, the mean stress total score was 22.7 ± 4.5, and the mean insomnia total score was 11.0 ± 7.1 (Table 4).
Scores and Frequency of Different Categories of Anxiety, Stress, and Insomnia in the Study Participants.

Factors Associated With a Significant Increase in Anxiety, Stress, or Insomnia Levels/Scores
Compared with male participants, female participants reported a significantly higher frequency of abnormal anxiety levels (P = .010). Participants with asthma and migraine had a significantly higher frequency of abnormal anxiety (P = .018 and P = .011, respectively). Participants with less than 6 years of experience had a higher frequency of abnormal anxiety than people working for 6 years or more (P = .029). Participants with sadness due to isolation had a significantly greater frequency of abnormal anxiety levels than people who were not sad (P = .003). Increased time spent with COVID-19 patients, COVID-19 infection, and decreased workforce had significant effects on increased anxiety levels (P < .05). In contrast, participants who received the COVID-19 vaccine and who had lower stress and insomnia had significantly lower levels of anxiety (P < .05). The strength of association was generally weak for all factors that had significant association with anxiety levels. Increased vaccine related stress and clinical insomnia had the highest strength of association using Cramer’s test (closer to 1 indicate stronger association; Table 5).
Factors Associated With a Significant Increase in Anxiety, Stress, and Insomnia Levels.

Note. Frequencies of strongly agree and agree were combined as (agree) and frequencies of strongly disagree and disagree were combined as (disagree). Univariate statistical analysis was performed to compare frequencies of different categories of anxiety, insomnia, and stress using the Chi-square or Fisher exact test. The strength of association was calculated by Cramer’s test.
Significant ≤.05.
Factors associated with a significant increase in insomnia levels included working in the private sector (P = .004), working during lockdown (P = .046), single or divorced (P = .034), having more than 3 children (P = .01), having asthma, or heart disease (P = .002), having a migraine (P = .010), smoking (P = .000), having less work experience (P = .002), having more time spent with COVID-19 patients (P = .029) having less monthly income (P = .026), having a lower workforce (P = .000), and having more sadness and loneliness (P = .000). Participants with better emotional support from their spouses and colleagues had significantly lower insomnia levels (P = .002 and P = .019, respectively). Furthermore, receiving the COVID-19 vaccine and receiving 2 doses also had significantly lower insomnia levels (P = .019 and P = .001, respectively). Abnormal anxiety and high stress were associated with increased insomnia levels (P = .000). Among all factors that achieved significance, the strength of association was higher with vaccine doses and anxiety (Table 5).
The associations between stress and a cut in salary, emotional support from family, colleagues, and spouses, sufficient food provided by the hospital during the lockdown, and a decreased workforce size were significant (P < .05). Additionally, the associations between stress and feelings of sadness and loneliness due to isolation from family and friends were significant (P = .048). Moreover, the associations between stress and anxiety or insomnia levels were significant (P = .000) (Table 5).
The mean anxiety score was significantly higher with private sector, working during lockdown, lower age, female gender, asthma patients, less working years, more time spent with patients, lower salary deduction, lower workforce, changed people’s attitude, COVID-19 diagnosis, using hospital transport, sadness due to isolation, high stress levels, and clinical insomnia (P < .05; Table 6). To the contrary, participants receiving COVID-19 vaccination, having 2 doses, and having less vaccine-related stress had a significantly lower mean anxiety score (P < .05) (Table 6). Factors that had significant effect on insomnia mean score and stress mean score were described in detail in Table 6 and were generally similar to factors associated with increased insomnia and stress levels described above in Table 5.
The Mean of Total Scores of Anxiety, Insomnia, and Stress Were Compared Across Different Categories by Student t-Test or One-Way ANOVA.
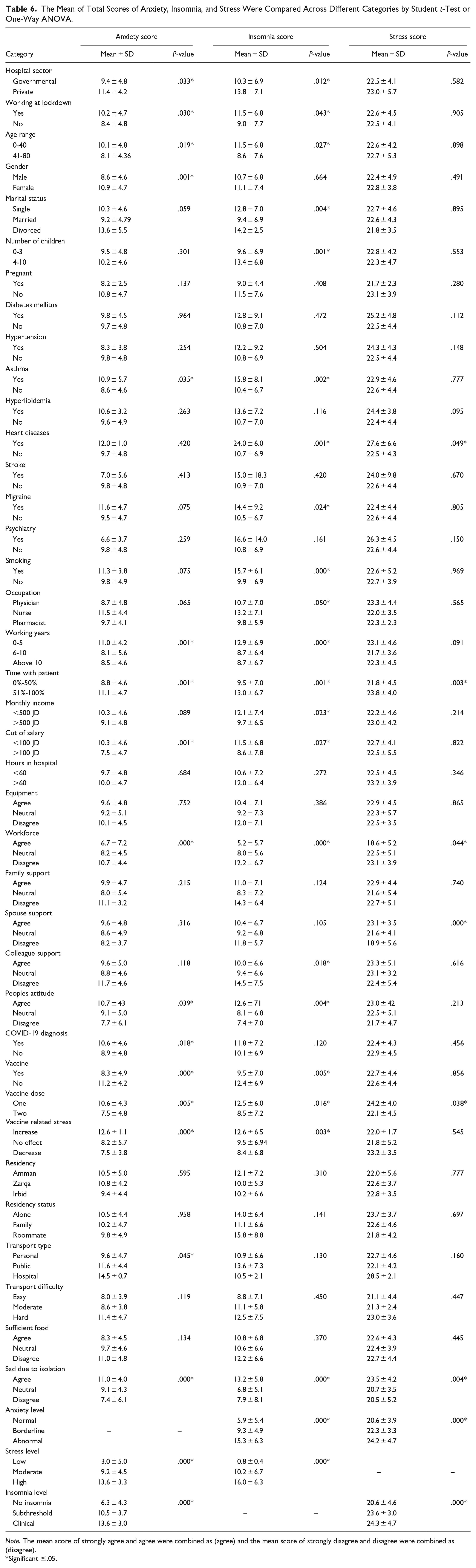
Note. The mean score of strongly agree and agree were combined as (agree) and the mean score of strongly disagree and disagree were combined as (disagree).
Significant ≤.05.
Positive correlations were noted between anxiety scores and insomnia scores (R = .618, P = .000), between anxiety scores and stress scores (R = .428, P = .000) and between stress scores and insomnia scores (R = .368, P = .000). As multiple factors were significantly associated with anxiety, insomnia, and stress, multivariate analysis was used to determine the most important factors. Both regression and linear models achieved high goodness of fit and were representative of data. Female gender, migraine, less working years, increased time spent with patients, lower work force, clinical insomnia and high stress were significant independent factors associated with anxiety using multivariate regression model. Similarly, female gender, clinical insomnia and high stress were significant independent factors associated with anxiety using multivariate linear model (Table 7). Younger age (≤ 40 years), single or divorced marital status, heart disease, smoking, occupation (nurses), lower workforce, vaccination dose, and anxiety were significant independent factors associated with insomnia (Table 7). Increased time spent with patients, lower workforce, lower spouse and colleagues support, sadness due to isolation and anxiety were significant independent factors associated with stress (P < .05) (Table 7).
Multivariate Analysis of the Independent Factors Associated With a Significant Effect on Anxiety, Stress, and Insomnia Levels (Multivariate Regression Model) or Significant Effect on Anxiety, Insomnia, and Stress Scores (Multivariate Linear Model).

Note. Normal anxiety levels, no insomnia, and normal stress levels were set as the reference value in the regression model.
Significant ≤.05.
Discussion
The current study evaluated the impact of the stressful COVID-19 pandemic on the mental health of hospital staff working at COVID-19 isolation and treatment hospitals/centers across Jordan. The study participants reported increased levels of stress, anxiety, and insomnia after the first wave of COVID-19 in Jordan (the first wave was recorded between September 2020 and January 2021 and the study was conducted between March 2021 and June 2021). Hospital staff are physically and mentally affected by the pandemic for being at the forefront of combating this crisis, being susceptible to infection, having a high workload with long working hours, limitation of resources, and experiencing the emotional challenges of patient suffering and loss.11,17
Salazar de Pablo et al. reported concerning rates of pandemic impacts on mental health of HCWs in a systematic review covering 115 studies. The review indicated high frequency of fear (43.7%), insomnia (37.9%), psychological distress (37.8%), anxiety features (29.0%), depressive symptoms (26.3%), post-traumatic stress disorder (20.7%), somatization (16.1%), and feelings of stigmatization (14.0%). 18 Similarly, a review of 44 meta-analysis studies reported an overall prevalence of stress at 44.3%, psychological distress at 34.59%, insomnia or sleep problems at 39.45%, anxiety symptoms at 29.9%, and depressive symptoms at 28.44%, of HCWs due to the COVID-19 pandemic. 11 The frequency of anxiety (68%) and stress (97.3%) among HCWs reported in this study were higher while levels of clinical insomnia (32%) were less than that reported by these systemic reviews and meta-analyses.11,18 Many factors could contribute to this difference, including the use of different instruments in different studies, factors related to the study population, and COVID-19 pandemic effects.11,18,19 The limited capacity of the Jordanian health system, low economic status and financial resources, governmental salary deductions, and the application of full curfew and physical isolation could contribute to increased anxiety and stress levels among Jordanian HCWs.2,4,5
A high percentage of the participants reported having abnormally high anxiety level/anxiety case (45%). Similar studies conducted during the peak of the COVID-19 pandemic reported increased severe anxiety levels of approximately 45% among HCWs.20,21 Severe anxiety levels/frequencies were lower in other studies.14,17,19 The physical condition of the staff, such as having asthma or migraine, was associated with increased anxiety levels. These findings were also observed during the 2003 SARS outbreak. 22 The emotional status of the staff, such as feeling sadness or loneliness due to isolation from family and loved ones, had a direct influence on their anxiety levels. Walton and colleagues reported staff feeling lonely, anxious, and sad due to being away from family while in quarantine and post-quarantine when required to return to work. 12 Female participants had higher anxiety rates, supporting previous findings explained by the general higher anxiety and stress levels of females. 4 Moreover, female HCWs in Brazil were anxious during the pandemic due to their low income combined with high workload, lack of personal protective equipment (PPE), and fear of transmitting the virus to their children. 23
Participants who spent more time treating COVID-19 patients and agreed on the limited workforce available, and COVID-19 infection were assocaited with higher anxiety levels. Similarly, a study conducted on frontline nurses during the SARS outbreak reported elevated stress and anxiety levels due to the high workload as a result of staff becoming infected and quarantined, resulting in a limited available workforce and continuous redeployment. 24 In Turkey, the exhaustion of healthcare staff due to a heavy workload leads to negative psychological effects, including an unwillingness to work, anxiety, insomnia, and stress. 19
The study participants’ who received COVID-19 vaccination with no vaccine doubts or fears had lower anxiety levels. A survey of 1205 nurses about COVID-19 vaccination hesitation showed less work stress and anxiety upon taking the vaccine. 25 In Saudi Arabia, a study of 1512 HCWs investigating COVID-19 vaccine acceptance reported 70% willingness to receive the vaccine among participants. Those willing participants had previously reported high anxiety scores regarding contacting the virus and transmitting it, suggesting that there are correlations between low anxiety levels and COVID-19 vaccination. 26 On the other hand, anxiety relief related to COVID-19 vaccine acceptance among HCWs varied among countries according to age, sex, and education level. In Ghana, fear, mistrust, and uncertainty were associated with vaccination and vaccine trial participation among HCWs, ultimately decreasing the hypothesized positive vaccination effect on anxiety levels. 27
The majority of participants (81%) in the present study had moderate levels of stress while 16.3% had sever levels of stress. Work-related factors such as increased time spent with patients, workforce availability, salary cut-off, and food availability were associated with increased stress levels. Likewise, a study comparing the psychological changes of HCWs during the MERS epidemic and the COVID-19 pandemic displayed higher stress rates from fears of community transmission and social limitations during the latter. 28 HCWs showed noticeable concerns about transmitting the virus to patients, friends, and family members. Additionally, they were worried about staff shortages and the unavailability of sufficient PPE, ultimately affecting their stress levels. 29 Low emotional support from family, spouse, and work colleagues and feeling lonely or isolated contributed to increased stress levels among participants, similar to other studies.29,30
Clinical Insomnia was reported by 32% of participants including 27% with moderate insomnia and 5% with severe insomnia. Factors related to the workplace, such as working experience, time spent with COVID-19 patients, salary cut-off, working during the lockdown, the available workforce, and working in the private sector, were found to negatively impact sleep quality. Similar results were displayed by 1153 Italian COVID-19 clinicians; 45% had symptoms of insomnia due to the heavy workload. 31 The physical and mental pressure faced by Chinese HCWs negatively affected their sleep quality, sleep duration, and habitual sleep efficiency and increase the use of sleep medication compared to the sleeping quality of the Chinese population. 15 Emotional support from the community and workplace leads to decrease stress levels and improves sleep quality.32,33 Participants with health conditions (asthma, heart disease, migraine) and smokers had greater insomnia levels than nonsmokers and healthy staff. On the other hand, vaccination had the opposite correlation with insomnia levels. Haddaden and his colleagues reported improved mood, social comfort, and sleep quality in HCWs upon COVID-19 vaccination. 34
A positive significant correlation between anxiety, stress, and insomnia levels was observed in the current study. Acute stress reactions are temporary and can last for days or weeks only. However, they could be shown in signs such as increased physical burn (such as having insomnia, headache, or chest pain) and emotional burn (such as numbness, anxiety, fear, and mood swings), supporting the positive correlation between the 3 studied outcomes.12,35 Moreover, Xiao et al. reported decreased sleep quality and increased levels of distress in China. 15
Similar studies on the effect of COVID-19 on the mental health of HCWs conducted in Arabic and Mediterranean regions during the same period reported comparable rates of stress, anxiety, and insomnia. HCWs from 9 Eastern Mediterranean countries reported stress and anxiety levels of 42.0% and 59.1%, respectively; 36 HCWs from 12 Arabic countries reported anxiety, stress, and insomnia levels of 48.9%, 41.4%, and 72.1%, respectively. 37 The prevalence of anxiety among HCWs in Jordan was only 11.3% at the start of the pandemic (March 2020), 38 whereas 45% was reported in this study conducted one year later (March 2021). Females and those with a history of chronic disease were at higher risk of developing anxiety,38,39 while the prevalence of mental health symptoms was greater among HCWs who worked more than 44 hours/week and those in contact with COVID-19 cases 37 similar to the findings reported in this study.
The mean scores for anxiety, stress, and insomnia observed in this study were greater than the scores observed in studies conducted using the same instruments on HCWs before COVID-19.40,41 Additionally, the scores were greater than the scores reported by the general population prior to COVID-19.42,43 Similarly, there was a significant worsening of mental health in the general population compared to the nonsignificant increase observed in pregnant women before and during COVID-19.42,43 The mean scores of anxiety, insomnia, and stress observed in this study were slightly higher than the scores observed in other studies in neighboring countries.36 -38
Multiple factors were associated with increased levels of anxiety, stress, and insomnia in this study, similar to other studies.13 -15,17,19,20,36 -38 Multivariate analysis was conducted to determine the most important independent risk factors. Deficiency in medical staff during the pandemic was independent risk factor for increased anxiety, insomnia and stress, similar to other studies.13 -15,17,19,20,36 -38 Female gender was an independent risk factor for anxiety, younger age was independent risk factor for insomnia, increased time spent with COVID-19 patients was an independent risk factor for increased levels of anxiety and stress, in agreement with other studies.15,17,20,36 -38 Isolation was an independent risk factor for stress in this study, in agreement with the findings of another study. 38 Profession type/title/position was an independent risk factor for mental health in many studies, similarly, nurses occupation was independent risk factor associated with insomnia in this study.11,17,20,36 -38 Social support including spouse support and colleague support have a significant effect in decreasing stress levels in multivariate analysis.
Among the significant factors that achieved larger effect in this study is the association of abnormal anxiety with clinical insomnia (association strength = 0.502 and correlation coefficient = 0.618). Abnormal anxiety group had 86% clinical insomnia compared to 16% with no insomnia and anxiety score mean was 13.6 for clinical insomnia compared to 6.3 for no insomnia. Beta coefficient in multivariate analysis after adjusting the effects of other factors was 9.6 indicating that clinical insomnia increased the odds of abnormal anxiety by about 10 times compared to no insomnia. Other studies indicated insomnia as a risk factor for anxiety and depression and insomnia was causally related to the experience of anxiety and other mental health problems.44 -46 Poor sleep quality could lead to increased anxiety levels which in turn would increase insomnia level getting into a viscous cycle. 45 Improving the sleep quality of medical staff is important in preventing increased anxiety levels. 46 Furthermore, early detection and management of mental health issues among medical staff would prevent further exaggeration of the condition and prevent development of other related physical and mental issues.44 -46
Maintaining the mental health of HCWs and reducing levels of anxiety, stress, and insomnia are important for preserving their quality of life and capacity to perform their duties effectively, increasing productivity, and avoiding medical mistakes and negligence. Attention to staff at higher risk during crises management like COVID-19 pandemic (female gender, young age, junior staff, nurses, poor social support, and staff with medical conditions), increase the number of staff and decrease workload and provision of proper support, protective measures and full vaccination are recommended. To protect the mental health well-being of HCWs, several solutions can be implemented, including e-mental health interventions, regular interviews, and screening tools, keeping a close eye on absenteeism, supportive networks, offering psychological assistance, especially to high-risk employees, and designing tailored prevention and support strategies.11,16,39 limitation of this study includes low number of participants with small groups in some categories due to difficulties related to recruitment of participants during the peak of the pandemic. Proper statistical tests to account for low numbers and multiple statistical testing were conducted to decrease this effect.
Conclusions and recommendations
This study highlighted increased levels of anxiety, stress, and insomnia among hospital staff working at COVID-19 centers after COVID-19 first wave in Jordan. The mean total scores for anxiety, stress, and insomnia were above the normal thresholds and were assessed using well-validated and relevant instruments (Hospital Anxiety and Depression Scale, Insomnia Severity Index, and Perceived Stress Scale 10). Furthermore, increased frequencies of abnormally high levels of anxiety, stress, and insomnia among hospital staff could indicate significant effects on mental health well-being. Multiple factors affect the increased levels of anxiety, stress, and insomnia among the study population. Early detection and preventive measures to support the mental well-being of HCWs during crises and stressful situations are recommended with special attention to high-risk groups.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580241248124 – Supplemental material for The Impact of COVID-19 on Mental Health and Sleep Function of Hospital Staff Working With COVID-19 Patients: A Cross-Sectional Nationwide Study
Supplemental material, sj-pdf-1-inq-10.1177_00469580241248124 for The Impact of COVID-19 on Mental Health and Sleep Function of Hospital Staff Working With COVID-19 Patients: A Cross-Sectional Nationwide Study by Mohammad Al-Tamimi, Iman Aolymat, Rahaf Alkhateeb, Saba Alshurman, Esra’a Dauod and Farah Rawabde in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We would like to thank all participants who agreed to be part of this study.
Author Contributions
M.A and I.A: conceptualization, supervision, research design, and writing manuscript. M.A: analysis of results. R. A, S.A, E.D, and F.R: design of survey, data collection and analysis, writing initial draft. M.A, I.A, R.A, S.A, E.D, F.R: review and approval of manuscript.
Data Availability
Data is available upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Mohammad Al-Tamimi is funded by Al-Quds Academy for Scientific Research (QASR), ARIF 2019. Amman, Jordan.
Ethical approval
The study protocol was approved by the Institutional Review Board (IRB) committee at the Hashemite University (Approval No 10/2/2020/2021 dated 25/10/2020) and the Jordanian Ministry of Health. All participants in the study have provided informed consent.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.